
Abstract
In this study, all-cause, stroke/systemic embolism (SE)-related, and major bleeding (MB)-related health-care costs among elderly patients with nonvalvular atrial fibrillation (NVAF) initiating treatment with different oral anticoagulants (OACs) were compared. Patients ≥65 years of age initiating OACs, including apixaban, rivaroxaban, dabigatran, and warfarin, were identified from the Humana Research Database between January 1, 2013, and September 30, 2015. Propensity score matching was used to separately match the different OAC cohorts with the apixaban cohort. All-cause health-care costs and stroke/SE-related and MB-related medical costs per patient per month (PPPM) were compared using generalized linear or 2-part regression models. Compared to apixaban, rivaroxaban was associated with significantly higher all-cause health-care costs (US$2234 vs US$1846 PPPM, P < .001) and MB-related medical costs (US$106 vs US$47 PPPM, P < .001), dabigatran was associated with significantly higher all-cause health-care costs (US$1980 vs US$1801 PPPM, P = .007), and warfarin was associated with significantly higher all-cause health-care costs (US$2386 vs US$1929 PPPM, P < .001), stroke/SE-related medical costs (US$42 vs US$18 PPPM, P < .001), and MB-related medical costs (US$132 vs US$51 PPPM, P < .001). Among elderly patients with NVAF, other OACs were associated with higher all-cause health-care costs than apixaban.
Keywords
Introduction
Atrial fibrillation (AF) is a common cardiac dysrhythmic condition and is mostly not related to valvular heart disease (nonvalvular AF, or NVAF). 1 Patients with NVAF are at an increased risk of stroke and systemic embolism (SE). 2 A community cohort study in the United States indicated that the incidence of stroke among patients with AF remained unchanged in the last decade (2000-2010), suggesting more comprehensive measures need to be implemented to reduce stroke risk among patients with NVAF. 2 In 2010, it was estimated that AF affected over 5 million individuals in the United States. 3 Due to an increasing number of elderly people in the US population, AF is projected to affect over 12 million individuals by 2030. 3 The economic burden associated with AF is likely to be substantial, as the annual direct medical cost was estimated at US$6 billion (in 2008 USD) for AF-related costs and US$26 billion when including other concomitant cardiovascular and noncardiovascular costs. 4
Vitamin K antagonists, mainly warfarin, have been the predominant anticoagulation medications used for stroke/SE prevention for patients with NVAF for decades. 5 However, warfarin has several disadvantages, including a limited therapeutic index and a risk of bleeding. 5 Moreover, many patients with NVAF in the United States, especially those who are elderly, do not receive warfarin therapy as recommended. 6 Direct oral anticoagulants (DOACs), including dabigatran, rivaroxaban, and apixaban, have been introduced to the US market within the past several years and are alternatives to warfarin for stroke/SE prevention among patients with NVAF. In large randomized clinical trials, the DOACs were shown to be either noninferior or superior to warfarin for reducing stroke and bleeding risks. 7 –9
Economic modeling studies based on clinical event rates reported in the randomized clinical trials have predicted DOAC versus warfarin usage among patients with NVAF to be associated with cost savings to health-care systems in the United States, with apixaban usage having the greatest cost savings. 10 –13 However, patient characteristics and clinical outcomes may differ in the real-world setting from that in clinical trials. Additionally, elderly patients are at a higher risk of stroke/SE and bleeding 14 and are likely to incur increased health-care costs related to stroke/SE and bleeding. It is important to better understand the economic burdens associated with different OAC treatments among elderly patients with NVAF. We previously conducted a real-world study that compared the risks of stroke/SE and major bleeding (MB) among OAC treatment-naive elderly patients with NVAF who initiated treatment with apixaban versus rivaroxaban, versus dabigatran, and versus warfarin identified from the Humana Research Database. 15 As there is a lack of comparative data on health-care costs among elderly patients with NVAF, in this new study, we further compared all-cause, stroke/SE-related and MB-related health-care costs among the elderly and Medicare-insured NVAF study population that initiated treatment with different OACs identified from the Humana Database.
Methods
Study Population
This study was a longitudinal retrospective cohort analysis. Oral anticoagulant treatment-naive patients with NVAF with Medicare Advantage insurance coverage and an age of ≥65 years who had ≥1 pharmacy claim for apixaban, rivaroxaban, dabigatran, or warfarin were identified from the Humana Research Database, between January 1, 2013, and September 30, 2015. This study period was chosen in order to be subsequent to Food and Drug Administration (FDA) approval of all 3 DOACs in the United States and to have the most recent data at the time of the study. Edoxaban was not included in this analysis as its FDA approval was not long before the end of the study period and the patient count was too low for this study. The Humana Research Database includes medical claims or encounter data collected from all available health-care sites (inpatient hospital, outpatient hospital, emergency department [ED], physician’s office, surgery center, etc) for virtually all types of provided services, including specialty, preventive, and office-based treatments. The Humana Research Database is comprised of claim records for more than 500 000 members. The overall study period was from January 1, 2012, to September 30, 2015, which included a 12-month baseline period prior to the index identification period.
The date of the earliest OAC pharmacy claim to occur (index event) between January 1, 2013, and September 30, 2015, was defined as the index date. Patients were required to have 12 months of continuous health plan enrollment with medical and pharmacy benefits prior to OAC drug initiation (baseline period). Patients were also required to have at least 1 inpatient or outpatient AF diagnosis (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] diagnosis code 427.31) during the baseline period or on the date of drug initiation. Patients were excluded if they had evidence of the following during the 12-month baseline period: rheumatic mitral valvular heart disease, mitral valve stenosis, heart valve replacement/transplant, diagnosis of venous thromboembolism or pulmonary embolism, and transient AF as identified by diagnosis or procedure code. To ensure patients were OAC treatment naive, patients were excluded if they had a pharmacy claim for warfarin, apixaban, rivaroxaban, dabigatran, or edoxaban during the baseline period. Furthermore, patients were excluded if they had claims for >1 type of OAC on the index date. Eligible patients were assigned to the apixaban, rivaroxaban, dabigatran, or warfarin cohorts based on their newly initiated OAC. Patients were followed for a variable length of time until the earliest of the following dates: 90 days after the index OAC treatment discontinuation, the date that the patient switched from the index OAC treatment to another OAC, health plan disenrollment date, or the end of the study period (September 30, 2015). Index OAC treatment discontinuation was defined as the first day of a period of at least 30 consecutive days (grace period) in which 0 days of supply for the index OAC was detected. The date of discontinuation was defined as the end date of the last filled prescription before the treatment gap. A switch to a different OAC was defined as a prescription filled for nonindex anticoagulants within 30 days after the date of discontinuation.
Demographics and Clinical Characteristics
Demographics and clinical characteristics during the 12-month baseline period were determined for each patient in the study cohorts prior to and after propensity score matching (PSM).
Propensity Score Matching
The PSM technique was used to balance identified patient characteristics when comparing the different OAC cohorts to apixaban cohorts. Propensity scores were generated using logistic regression analyses, which included the following as covariates: age, gender, race, US geographic region, Charlson comorbidity index (CCI) score, CHA2DS2-VASc score, HAS-BLED score, follow-up period duration, baseline total health-care cost, baseline stroke/SE-related medical cost, baseline bleeding-related medical cost, baseline comorbidities (thrombocytopenia, congestive heart failure, diabetes, hypertension, renal disease, myocardial infarction, dyspepsia/stomach discomfort, peripheral vascular disease, transient ischemic attack, coronary artery disease), and baseline medication usage (angiotensin-converting enzyme inhibitors, amiodarone, angiotensin receptor blockers, β-blockers, H2-receptor antagonists, proton pump inhibitors, statins, antiplatelet drugs). These covariates were included based on their relevance to disease state and were based on inputs from clinical experts and previous studies. 15 In the PSM matching process, the matching caliper of the propensity scores was set at 0.001. Matching was conducted 1:1 by using the nearest neighbor algorithm. Matched patient cohorts (rivaroxaban vs apixaban, dabigatran vs apixaban, and warfarin vs apixaban) were inspected to ensure cohorts were well balanced with key patient characteristics statistically similar (P > .05).
Health-Care Economic Outcomes
The health-care economic outcomes assessed during the follow-up among each of the matched cohorts included monthly total all-cause health-care costs, all-cause medical costs, all-cause pharmacy costs, all-cause hospitalization (inpatient) costs, all-cause ED and outpatient medical costs, stroke/SE-related medical costs, and MB-related medical costs. Medical costs were defined to include the inpatient and outpatient medical service costs, but not the outpatient pharmacy cost. Stroke/SE and MB events were identified using hospital claims that had the corresponding diagnosis code as the first listed ICD-9-CM diagnosis code (online Appendix). Stroke/SE-related and MB-related medical costs were defined as hospitalization costs and outpatient medical service costs associated with all stroke/SE or MB diagnosis codes reported as the primary or secondary diagnosis. Costs were inflation-adjusted to 2015 cost levels using the Consumer Price Index: Medical Care. 16 Costs were calculated and reported as per patient per month (PPPM) costs within each propensity score matched cohort. Per patient per month cost was calculated as the total cost in the follow-up for the patient divided by the number of months in the follow-up periods for the patient.
Statistical Analyses
Generalized linear models (GLMs) with log transformation and gamma distribution and with only the OAC drugs as independent variables were used to evaluate the impact of the different OAC treatments relative to apixaban treatment on total all-cause health-care costs (inpatient, outpatient medical costs, and outpatient pharmacy costs), all-cause medical costs (inpatient and outpatient medical costs), outpatient medical costs, and outpatient pharmacy costs. Log transformation and gamma distribution were applied to the cost regression analysis so that the most appropriate cost data distribution would be incorporated in the GLMs as is commonly done in such data analyses. Least-squares means were estimated by analysis of covariance in the GLMs.
Two-part regression analyses were used to evaluate the impact of the different OAC treatments relative to apixaban on stroke/SE-related, MB-related medical costs, and all-cause inpatient costs. The 2-part regression analyses were used to avoid the analytical issues associated with the large number of data, with 0 cost values for stroke/SE-related, MB-related medical costs, and all-cause inpatient costs. In the 2-part regression analyses for stroke/SE-, MB-related costs, or all-cause inpatient costs, the first part was multivariable Cox regression with only the OAC drugs as independent variables, which was used to evaluate the impact of OAC treatment on the risks of stroke/SE, MB events, or all-cause hospital admissions. We previously conducted a study that compared the risks of stroke/SE and MB among OAC treatment-naive elderly patients with NVAF who initiated treatment with apixaban, versus rivaroxaban, versus dabigatran, and versus warfarin in the same study population identified for this comparison of health-care costs. 15 However, hazard ratios (HRs) describing the impact of the different OAC drugs on stroke/SE and MB events were for apixaban versus the different OACs. 15 Since the current comparison of health-care costs used apixaban as the reference group, HRs for stroke/SE events, MB events, and all-cause hospitalizations were generated again from Cox proportional hazards regression models and expressed as each OAC versus apixaban (online Appendix Table 1). Apixaban was used as the reference cohort in the regression analyses since it was the most recently FDA-approved drug in the analysis and is the current market leader of the new prescription of DOACs among patients with NVAF. 17
The second part involved the use of a multivariable GLM with log transformation and gamma distribution to evaluate the stroke/SE-, MB-related cost, or all-cause inpatient cost data among patients with such corresponding events (nonzero costs). Hazard ratios estimated from the first part of the analyses were combined with the costs generated from the second part to estimate the corresponding incremental stroke/SE- and MB-related cost or incremental all-cause inpatient costs of treatment with other OACs versus apixaban among all patients with NVAF receiving the treatments. The 2-part calculations were further carried out in 1000 cycles of random bootstrapping resampling to generate 1000 such estimates. Univariate statistics of the 1000 incremental stroke/SE-related, MB-related, and all-cause inpatient admission costs among all patients were used to evaluate the corresponding stroke/SE-related, MB-related costs, and all-cause inpatient admission costs. The 2.5 and 97.5 percentiles of the incremental stroke/SE-, MB-related costs, and all-cause inpatient admission costs estimated from the 1000 cycles of bootstrapping were used to represent the lower and upper 95% confidence levels, respectively. In all regression analyses, a P value of <.05 was used to define statistical significance. All data analyses were executed using statistical software SAS version 9.4.
Results
Rivaroxaban Versus Apixaban
Table 1 shows the PSM baseline demographics, clinical characteristics, and health-care costs of study cohorts treated with rivaroxaban and apixaban. After implementing PSM, 13 620 patients were matched with 6810 patients in each of the rivaroxaban (mean age: 77.0 years) and apixaban (mean age: 77.1 years) cohorts. Stroke and bleeding risks, according to CHADS2 score (2.6 vs 2.6, P = .97), CHA2DS2-VASc score (4.4 vs 4.4, P = .86), and HAS-BLED score (2.9 vs 2.9, P = .90), were similar and not significantly different between cohorts, as was general comorbidity measured by CCI (2.7 vs 2.8, P = .97). Total all-cause health-care costs (US$1054 vs US$1057 PPPM, P = .85), all-cause medical costs (US$850 vs US$849 PPPM, P = .97), stroke-related medical costs (US$39 vs US$42 PPPM, P = .42), and bleeding-related medical costs (US$46 vs US$40 PPPM, P = .15) during the baseline period were not significantly different for patients with NVAF treated with rivaroxaban and apixaban. Also, the mean durations of follow-up for the rivaroxaban and apixaban cohorts were similar (6.4 vs 6.5 months, P = .54).
Baseline Demographics, Clinical Characteristics, and Health-Care Costs of Study Cohorts After Propensity Score Matching.a
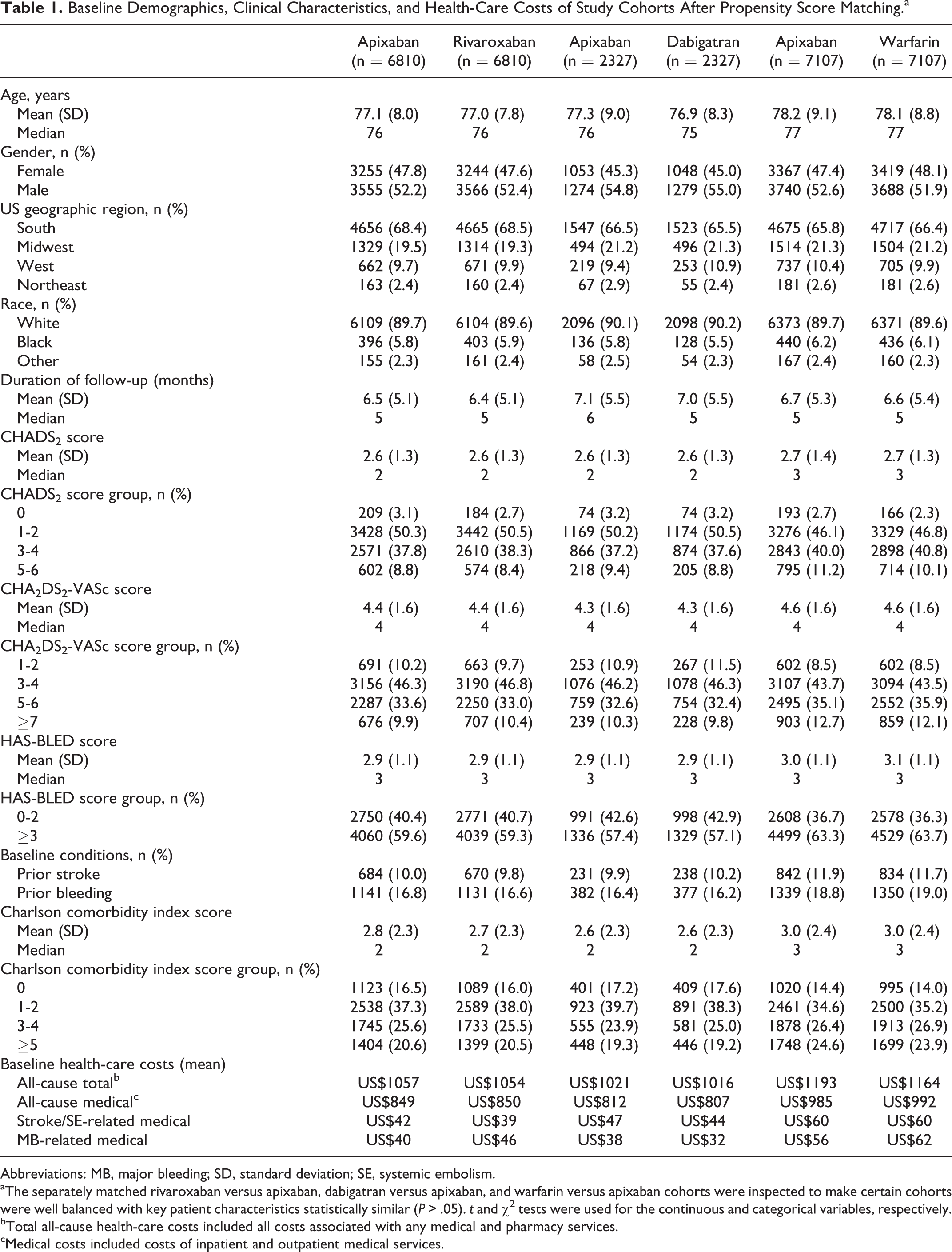
Abbreviations: MB, major bleeding; SD, standard deviation; SE, systemic embolism.
aThe separately matched rivaroxaban versus apixaban, dabigatran versus apixaban, and warfarin versus apixaban cohorts were inspected to make certain cohorts were well balanced with key patient characteristics statistically similar (P > .05). t and χ2 tests were used for the continuous and categorical variables, respectively.
bTotal all-cause health-care costs included all costs associated with any medical and pharmacy services.
cMedical costs included costs of inpatient and outpatient medical services.
Generalized linear model regression analyses showed that during the follow-up, rivaroxaban versus apixaban treatment was associated with significantly higher monthly total all-cause health-care costs (US$2234 vs US$1846 PPPM, P < .001; Figure 1). While patients treated with rivaroxaban had lower monthly all-cause pharmacy costs than those treated with apixaban (US$388 vs US$427 PPPM, P < .001; Figure 2), monthly medical costs (inpatient + outpatient) for all causes were US$427 PPPM higher for patients treated with rivaroxaban versus apixaban (US$1846 vs US$1419 PPPM, P < .001; Figure 2). Additionally, all-cause hospitalization costs (US$1184 vs US$704 PPPM, P < .001; Figure 3A) and ED/outpatient medical costs (US$845 vs US$761 PPPM, P < .001; Figure 3B) were also significantly higher for patients treated with rivaroxaban compared to those treated with apixaban. Stroke/SE-related medical costs (US$23 vs US$18 PPPM, P = .41; Figure 4) were not significantly different between cohorts; however, MB-related medical costs were significantly higher for patients treated with rivaroxaban compared to those treated with apixaban during the follow-up period (US$106 vs US$47 PPPM, P < .001; Figure 5).
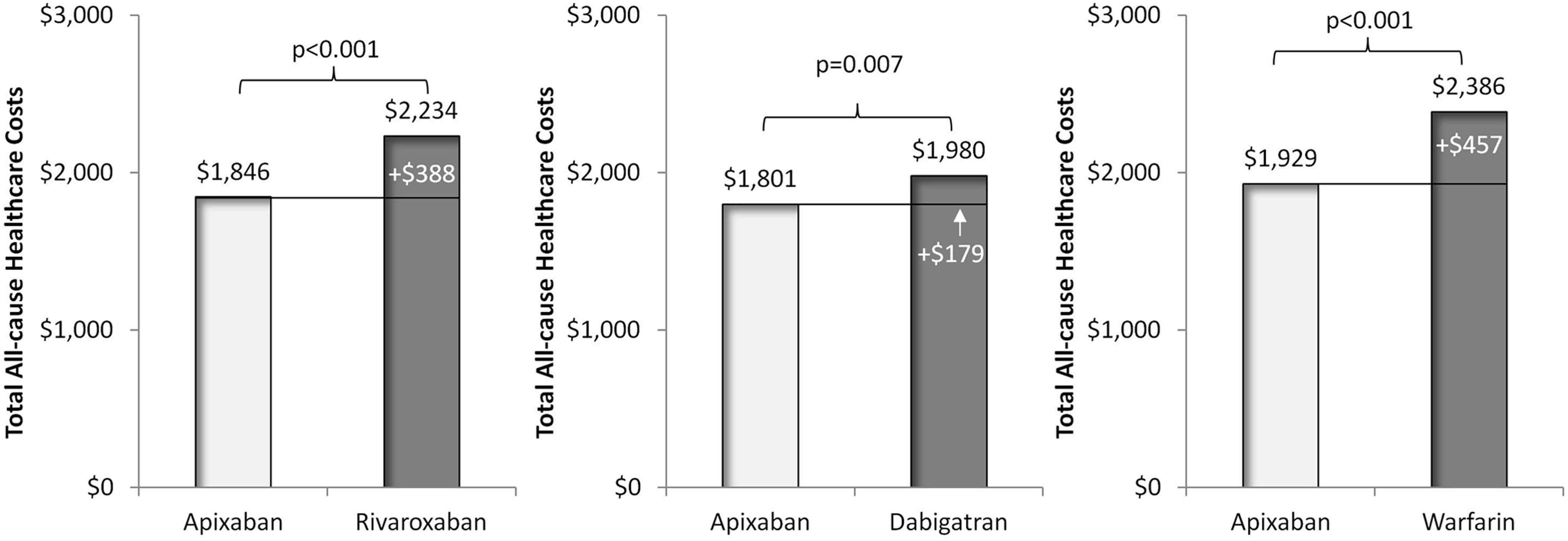
Comparison of total all-cause health-care costs per patient per month during follow-up for postmatched cohorts treated with other oral anticoagulants versus apixaban. Total all-cause health-care costs included all costs associated with any medical and pharmacy services.
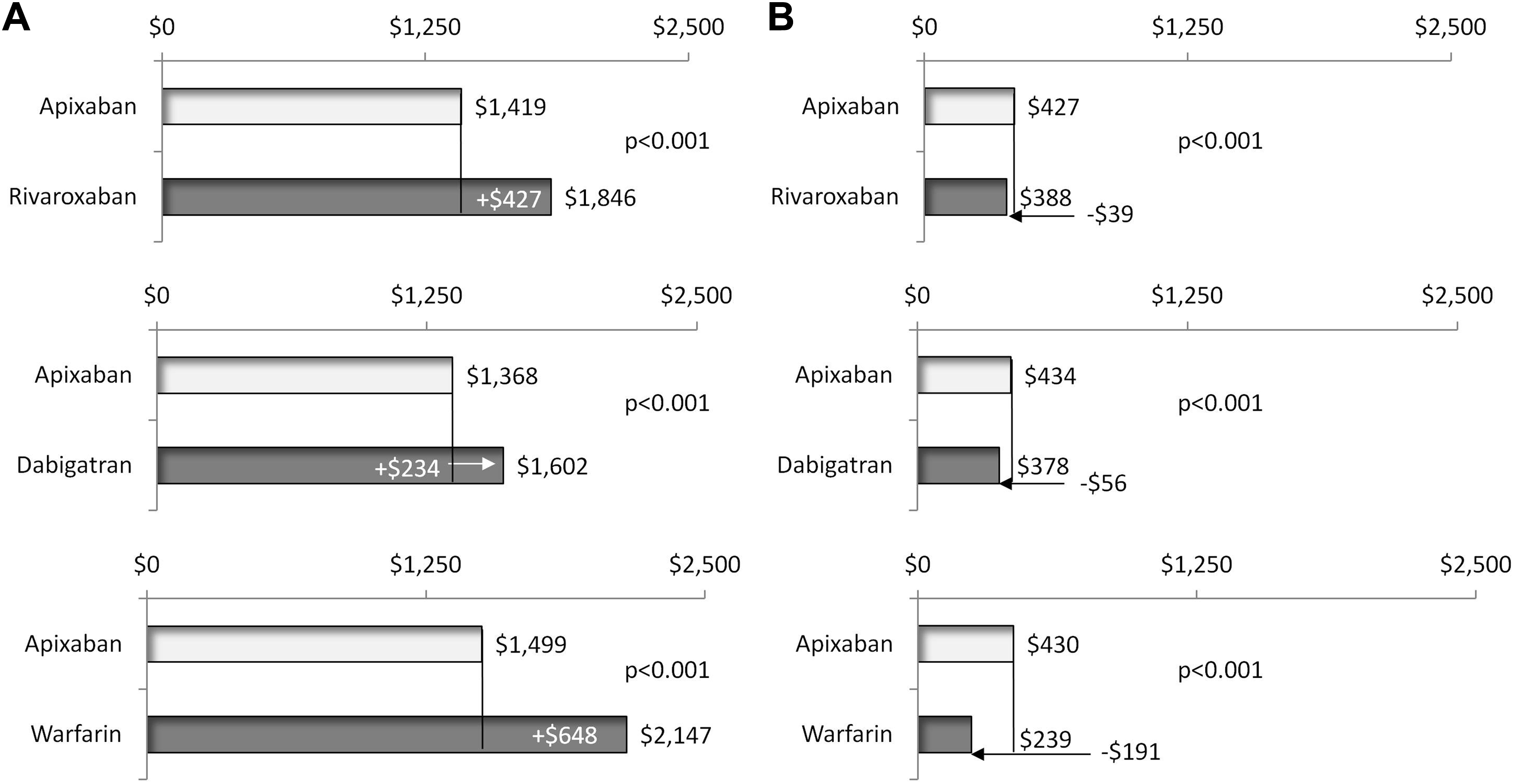
Comparison of all-cause medical costs (A) and pharmacy costs (B) per patient per month during follow-up for postmatched cohorts treated with other oral anticoagulants versus apixaban. Medical costs included costs of inpatient and outpatient medical services.
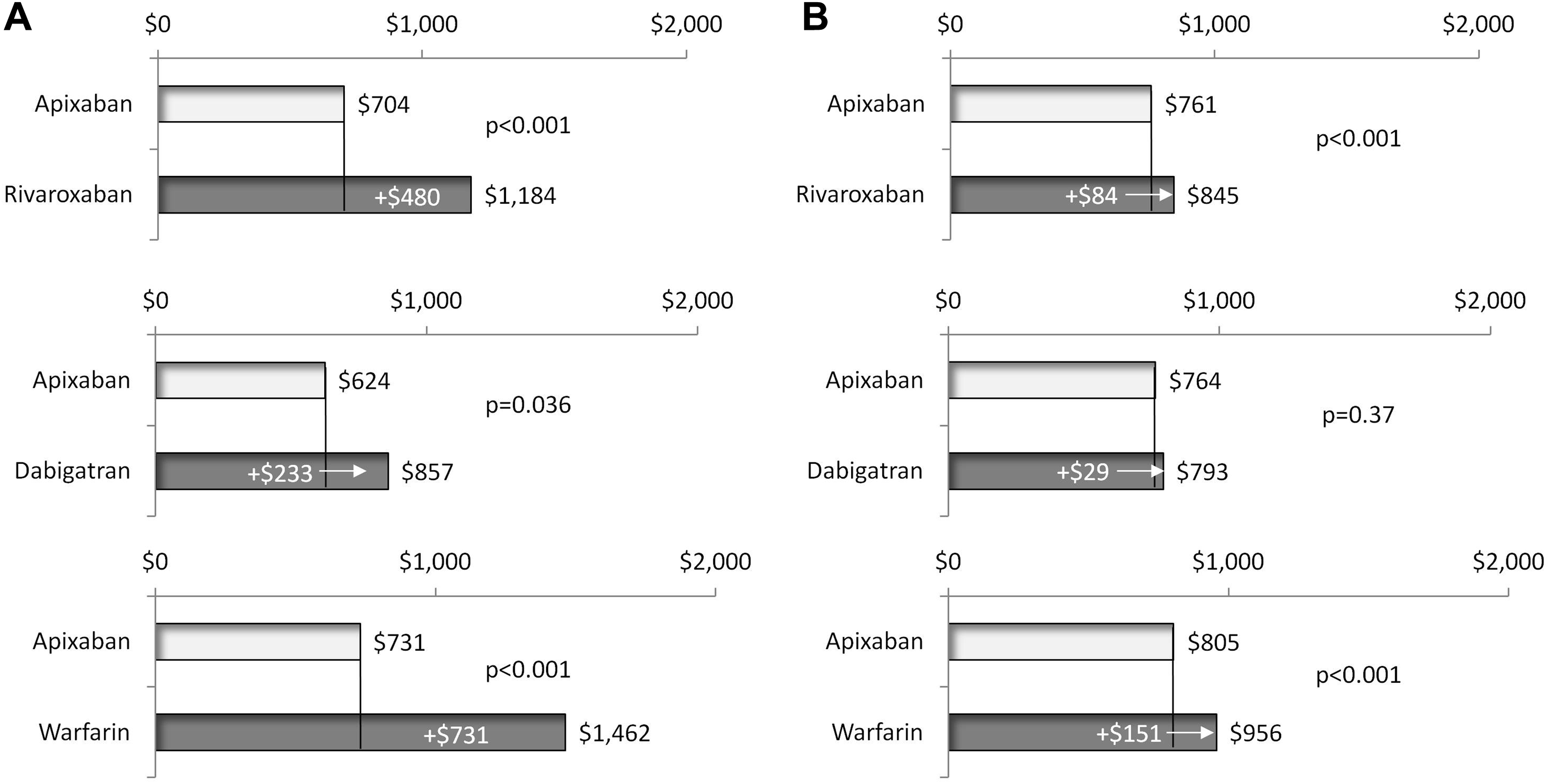
Comparison of all-cause hospitalization costs (A) and emergency department/outpatient medical costs (B) per patient per month during follow-up for postmatched cohorts treated with other oral anticoagulants versus apixaban.
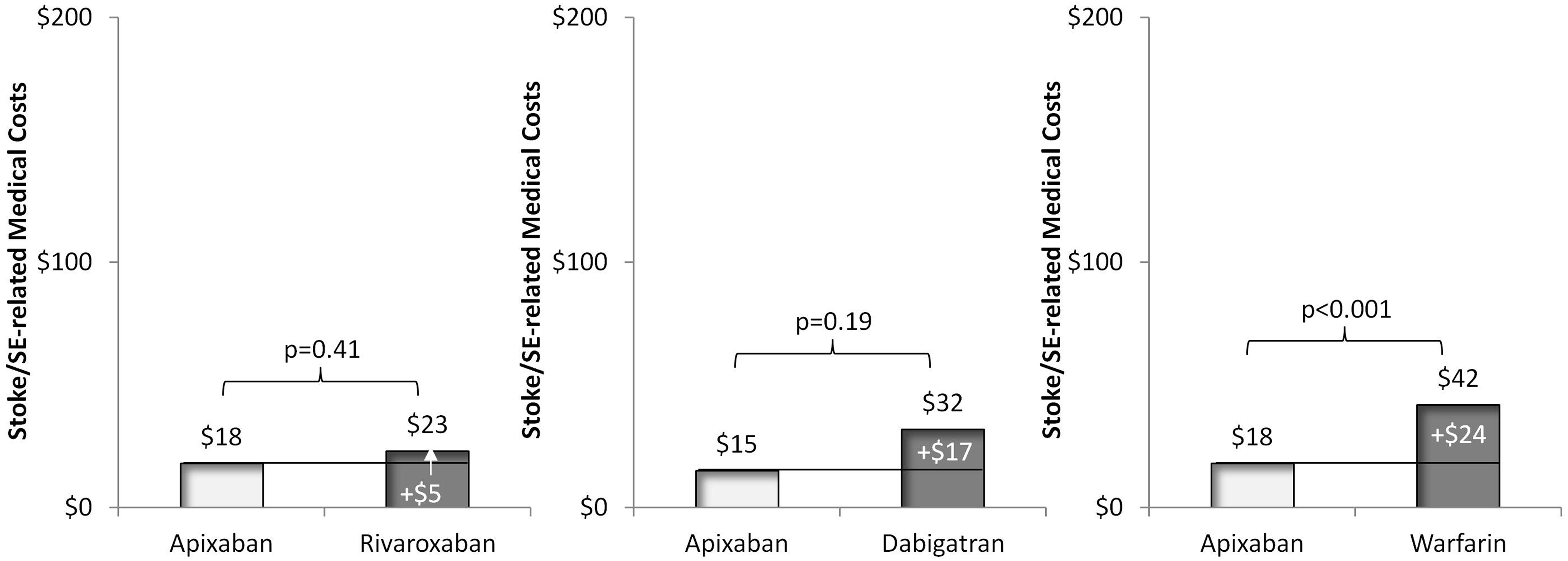
Comparison of stroke/systemic embolism (SE)-related medical costs per patient per month during the follow-up for postmatched cohorts treated with other oral anticoagulants versus apixaban. Medical costs included costs of inpatient and outpatient medical services.
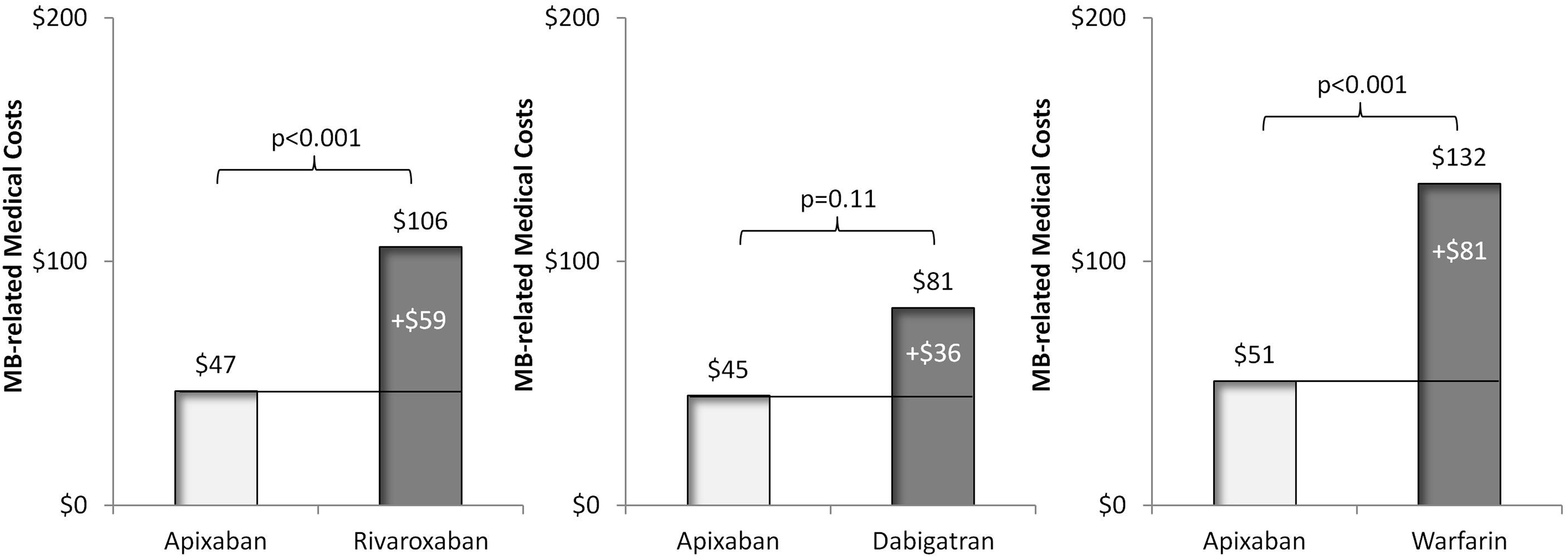
Comparison of major bleeding (MB)-related medical costs per patient per month during the follow-up for postmatched cohorts treated with other oral anticoagulants versus apixaban. Medical costs included costs of inpatient and outpatient medical services.
Dabigatran Versus Apixaban
Table 1 shows the PSM baseline demographics, clinical characteristics, and health-care costs of study cohorts treated with dabigatran and apixaban. After implementing PSM, 4654 patients were matched with 2327 patients in each of the dabigatran (mean age: 76.9 years) and apixaban (mean age: 77.3 years) cohorts. Stroke and bleeding risks, according to CHADS2 score (2.6 vs 2.6, P = .61), CHA2DS2-VASc score (4.3 vs 4.3, P = .58), and HAS-BLED score (2.9 vs 2.9, P = .77), were similar and not significantly different between cohorts, as was general comorbidity measured by CCI (2.6 vs 2.6, P = .86). Total all-cause health-care costs (US$1016 vs US$1021 PPPM, P = .89), all-cause medical costs (US$807 vs US$812 PPPM, P = .84), stroke-related medical costs (US$44 vs US$47 PPPM, P = .70), and bleeding-related medical costs (US$32 vs US$38 PPPM, P = .32) during the baseline period were not significantly different for patients with NVAF treated with dabigatran and apixaban. The mean durations of follow-up for the dabigatran and apixaban cohorts were also similar (7.0 vs 7.1 months, P = .71).
Generalized linear model regression analyses showed that during the follow-up, dabigatran versus apixaban treatment was associated with significantly higher monthly total all-cause health-care costs (US$1980 vs US$1801 PPPM, P = .007; Figure 1). While patients treated with dabigatran had lower monthly all-cause pharmacy costs (US$378 vs US$434 PPPM, P < .001; Figure 2), monthly medical costs (inpatient + outpatient) for all causes were US$234 higher for patients treated with dabigatran versus apixaban (US$1602 vs US$1368 PPPM, P < .001; Figure 2). All-cause hospitalization costs were also significantly higher for patients treated with dabigatran compared to those treated with apixaban (US$857 vs US$624 PPPM, P = .036; Figure 3A), but ED/outpatient medical costs were not significantly different (US$793 vs US$764 PPPM, P = .37; Figure 3B). Stroke/SE-related medical costs (US$32 vs US$15 PPPM, P = .19; Figure 4) and MB-related medical costs (US$81 vs US$45 PPPM, P = .11; Figure 5) were numerically higher for patients treated with dabigatran compared to those treated with apixaban, but the differences did not reach statistical significance.
Warfarin Versus Apixaban
Table 1 shows the PSM baseline demographics, clinical characteristics, and health-care costs of study cohorts treated with warfarin and apixaban. After implementing PSM, 14 214 patients were matched with 7107 patients in each of the warfarin (mean age: 78.1 years) and apixaban (mean age: 78.2 years) cohorts. Stroke and bleeding risks, according to CHADS2 score (2.7 vs 2.7, P = .37), CHA2DS2-VASc score (4.6 vs 4.6, P = .66), and HAS-BLED score (3.1 vs 3.0, P = .22), were similar and not significantly different between cohorts, as was general comorbidity measured by CCI (3.0 vs 3.0, P = .97). Total all-cause health-care costs (US$1164 vs US$1193 PPPM, P= .15), all-cause medical costs (US$992 vs US$985 PPPM, P = .72), stroke-related medical costs (US$60 vs US$60 PPPM, P = .99), and bleeding-related medical costs (US$62 vs US$56 PPPM, P = .24) during the baseline period were not significantly different for patients with NVAF treated with warfarin and apixaban. The mean durations of follow-up for the warfarin and apixaban cohorts were also similar (6.6 vs 6.7 months, P = .67).
Generalized linear model regression analyses showed that during the follow-up, warfarin versus apixaban treatment was associated with significantly higher monthly total all-cause health-care costs (US$2386 vs US$1929 PPPM, P < .001; Figure 1). While patients treated with warfarin had lower monthly all-cause pharmacy costs than those treated with apixaban (US$239 vs US$430 PPPM, P < .001; Figure 2), monthly medical costs (inpatient + outpatient) for all causes were US$648 higher for patients treated with warfarin versus apixaban (US$2147 vs US$1499 PPPM, P < .001; Figure 2). All-cause hospitalization costs (US$1462 vs US$731 PPPM, P < .001; Figure 3A) and ED/outpatient medical costs (US$956 vs US$805 PPPM, P < .001; Figure 3B) were also significantly higher for patients treated with warfarin compared to those treated with apixaban, as were stroke/SE-related medical costs (US$42 vs US$18 PPPM, P < .001; Figure 4) and MB-related medical costs (US$132 vs US$51 PPPM, P < .001; Figure 5).
For all comparisons of health-care costs between the different OACs and apixaban, the regression results were obtained from separate regression analyses, and therefore, the resulting inpatient and outpatient medical costs may not add up to the total medical costs.
Discussion
This retrospective cohort analysis, which used the Humana Research Database, compared all-cause, stroke/SE- and MB-related health-care costs among elderly patients with NVAF treated with other OACs versus apixaban. It was found that treatment with rivaroxaban, dabigatran, and warfarin were all associated with significantly higher all-cause health-care costs compared with apixaban treatment after controlling for key significant differences in patient characteristics with PSM. The higher all-cause health-care costs associated with other OACs versus apixaban were mainly attributed to higher all-cause hospitalization costs. All-cause hospitalization costs PPPM were US$480 higher for rivaroxaban, US$233 higher for dabigatran, and US$731 higher for warfarin when compared to apixaban. The higher hospitalization costs associated with the other OACs versus apixaban may be partly reflective of the significantly higher risks of stroke/SE and MB for patients treated with rivaroxaban versus apixaban (stroke/SE: 3.3% vs 2.4%; MB: 9.5% vs 4.7%) and those treated with warfarin versus apixaban (stroke/SE: 4.2% vs 2.8%; MB: 9.4% vs 5.1%) and the trend toward higher risks of stroke/SE (3.3% vs 2.6%) and MB (5.8% vs 4.7%) among patients treated with dabigatran versus apixaban as described previously. 15 Consistently, the current study showed that when compared to apixaban treatment, warfarin treatment was associated with significantly higher stroke/SE- and MB-related medical costs, rivaroxaban treatment was associated with significantly higher MB-related medical cost and numerically higher stroke/SE-related medical cost, and dabigatran treatment was associated with numerically higher stroke/SE- and MB-related medical costs. In this study, MB-related medical costs included all hospitalization and outpatient medical service costs associated with an MB diagnosis code. Drug costs for MB were not included since there is not a reliable method to identify specific drugs for the treatment of MB, and thus, the economic burden of MB may have been underestimated in this analysis. All-cause total health-care costs and medical costs may have also included the incremental costs associated with any potential complications associated with ineffective OAC treatment. For instance, when patients had ineffective DOAC treatment, they might have also experienced complications from treatment interruption, complications from MB and stroke events, and potentially exacerbation of underlying comorbidities. These additional costs were all included in the all-cause medical and total health-care costs. However, as this study was a real-world retrospective claims database analysis, a causal relationship between usage of any of the OACs and any such additional adverse outcomes cannot be discerned.
The findings of the current study are in general consistent with those of 2 other recent publications. 18,19 Amin et al compared the health-care and economic burdens of stroke/SE and MB among elderly patients with NVAF treated with DOACs relative to warfarin in the real-world setting. 18 Among 186 132 patients with NVAF initiating warfarin or DOACs identified from a Medicare database, the study also found that compared to warfarin, apixaban was associated with lower stroke/SE-related and MB-related medical costs. 18 The findings of the current study are directionally consistent with that of another recent study, in which a direct comparison of all-cause and MB-related costs associated with OAC treatment was conducted. 19 In this study by Lin et al, patients with NVAF (mean age: 62-64 years) newly initiating OACs were identified from the IMS PharMetrics database. 19 The findings were similar to the current study, such that compared to apixaban, total all-cause health-care costs were significantly higher for patients with NVAF treated with either rivaroxaban or warfarin. 19 Also, all-cause hospitalization costs were also found to be significantly higher for patients with NVAF treated with rivaroxaban, dabigatran, and warfarin versus apixaban, and MB-related medical costs were significantly higher for those treated with warfarin versus apixaban. 19
This study has some limitations and considerations. Firstly, each OAC cohort was independently propensity score matched against an apixaban cohort; thus, comparisons cannot be made across the 3 separate arms of the analysis. Edoxaban was not included in this analysis since the number of edoxaban-treated patients was too few for meaningful statistical analysis. This was not a cost-effectiveness analysis based on directly comparative randomized clinical trial data, since there are no head-to-head clinical trials comparing the efficacy and safety of any of the DOACs among patients with NVAF. This cost analysis does not imply comparable efficacy, safety, or product interchangeability. Furthermore, interpretation of stroke-related outcomes and associated costs should be carefully considered due to the low number of stroke events.
Administrative claims data are collected for purposes other than research and the analysis is constrained by available billing codes, which may contain coding errors and missing data. Also, potential confounders not captured in the database, such as taking over-the-counter medications (eg, aspirin) and adherence to anticoagulation therapy, exist. This database contains information from administrative claims covered by the Humana health plan and may not be generalizable to the entire US population of patients with NVAF. The follow-up period for patients was not uniform nor consistent with those in the clinical trials. On the other hand, in the matched populations, the durations of the follow-up periods between the comparison cohorts were relatively similar and thus may potentially reduce some of the potential bias from the differences in the follow-up durations. However, the follow-up periods for the study populations were relatively short (<7 months) and further study of long-term patient outcomes is warranted. Lastly, as this is an observational study, no causal relationship between treatment and outcome can be inferred, and only associations can be assessed.
In the real-world setting, after controlling for differences in patient characteristics with PSM, rivaroxaban, dabigatran, and warfarin were all associated with significantly higher all-cause health-care costs when compared with apixaban among elderly patients with NVAF. Warfarin was associated with significantly higher stroke/SE- and MB-related medical costs and rivaroxaban also had significantly higher MB-related medical costs than apixaban. The findings of this study provide potentially useful information for payers, providers, and patients for decision-making in the different treatment options for stroke prevention among elderly patients with NVAF.
Supplemental Material
Supplemental Material, Apix_vs_Riva_Dabi_Warf_HRU_CATH_manuscript_v9_Supp_Table - All-Cause, Stroke/Systemic Embolism–, and Major Bleeding-Related Health-Care Costs Among Elderly Patients With Nonvalvular Atrial Fibrillation Treated With Oral Anticoagulants
Supplemental Material, Apix_vs_Riva_Dabi_Warf_HRU_CATH_manuscript_v9_Supp_Table for All-Cause, Stroke/Systemic Embolism–, and Major Bleeding-Related Health-Care Costs Among Elderly Patients With Nonvalvular Atrial Fibrillation Treated With Oral Anticoagulants by Steve Deitelzweig, Xuemei Luo, Kiran Gupta, Jeffrey Trocio, Jack Mardekian, Tammy Curtice, Patrick Hlavacek, Melissa Lingohr-Smith, Brandy Menges, and Jay Lin in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Steve Deitelzweig is a consultant for Pfizer and Bristol-Myers Squibb. Xuemei Luo, Jeffrey Trocio, Jack Mardekian, and Patrick Hlavacek are employees of Pfizer and own stock in the company. Kiran Gupta and Tammy Curtice are employees of Bristol-Myers Squibb and own stock in the company. Melissa Lingohr-Smith, Brandy Menges, and Jay Lin are employees of Novosys Health, which has received research funds from Pfizer and Bristol-Myers Squibb in connection with conducting this study and development of this manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by Pfizer and Bristol-Myers Squibb.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.