
Abstract
Coronary artery disease (CAD) is one of the chief causes of death in the world. Several hypotheses have been promoted as for the origin of the disease, among which are genetic predispositions and/or environmental factors. The aim of this study was to determine the effect of factor V (FV) gene polymorphisms (Leiden, G1691A [FVL] and HR2 A4070G) and to analyze their association with traditional risk factors in assessing the risk of CAD. Our study population included 200 Tunisian patients with symptomatic CAD and a control group of 300 participants matched for age and sex. All participants were genotyped for the FVL and HR2 polymorphisms. Multivariate logistic regression was applied to analyze independent factors associated with the risk of CAD. Our analysis showed that the FVL A allele frequency (P < 10–3, odds ratio [OR] = 2.81, 95% confidence interval [CI] = 1.6-4.9) and GA genotype (P < 10–3, OR = 4.03, 95% CI = 2.1-7.6) are significantly more prevalent among patients with CAD compared to those controls and may be predisposing to CAD. We further found that the FVL mutation is an independent risk factor whose effect is not modified by other factors (smoking, diabetes, hypertension, dyslipidemia, and a family history of CAD) in increasing the risk of the disease. However, analysis of FV HR2 variation does not show any statistically significant association with CAD. The FVL polymorphism may be an independent risk factor for CAD. However, further investigations on these polymorphisms and their possible synergisms with traditional risk factors for CAD could help to ascertain better predictability for CAD susceptibility.
Keywords
Introduction
Coronary artery disease (CAD) is the major cause of death in most of the developing and developed countries. 1 It is caused by atherosclerosis of the coronary arteries, which leads to restriction of blood flow to the heart. This disease has a long asymptomatic developmental phase. It is a chronic process that begins during adolescence and slowly progresses throughout life. 2 Coronary artery disease has a complex etiology and pathophysiology generated by the combined effects of genes and the environment. 2,3
The association between CAD and environmental factors has been thoroughly investigated. Epidemiologic studies provide strong evidence of a causal relationship between CAD and dyslipidemia, hypertension, type 2 diabetes mellitus (T2DM), smoking, and family history of CAD. 4,5
Moreover, multiple biochemical processes can cause this disease, including the metabolism of lipids and apolipoproteins, inflammatory responses, endothelial function, platelet function, fibrinolysis, homocysteine metabolism, insulin sensitivity, the regulation of blood pressure, and thrombosis. 1,2 The role of genetic influences, however, is still poorly understood. 6,7
Factor V (FV) is a 330-kD protein playing a key role in blood coagulation, transforming prothrombin into thrombin, and it is inactivated by protein C (PC), thus modulating the amount of thrombin generated. 8 –10 Factor V is encoded by a gene spanning more than 80 kb, comprising 25 exons and located on chromosome 1 (1 q21-25). 11 Single nucleotide polymorphisms (SNPs) in the FV gene are considered as the most frequently inherited abnormalities in blood coagulation that leads to thrombophilia. 1,2,12
A widely studied abnormality in the FV gene is the G1691A mutation known as the FV Leiden (FVL; rs6025). 13 –15 This mutation is caused by a transition of guanine (G) to adenine (A) at position 1691 in the gene resulting in the substitution of glutamine for arginine at amino acid 506. The A4070G variant (also known as the FV HR2 or rs1800595 variant) is another common missense mutation of the FV gene that occurs at position 4070 where A replaces G, causing the substitution of histidine for arginine at position 1299. The FVL mutation results in an activated protein C (APC) resistance phenotype, which is associated with an increased risk of venous thromboembolism (VTE). Due to the loss of the APC cleavage site at R506, FVL is less susceptible to inactivation by APC and expresses reduced APC cofactor activity in factor VIIIa inactivation. This mutation is considered to be one of the most important risk factors leading to a predisposition for CAD. 3,12,16,17 Similarly, the FV HR2 variant alone or in coinheritance with FVL appears to be associated with a severe APC resistance phenotype. 12,18,19
The results from association studies between FV gene polymorphisms and CAD have been inconsistent, and several hypotheses have been suggested to explain possible mechanisms. The results from recent Tunisian studies have provided conflicting results, and few studies have considered the relationship between the FV gene and traditional risk factors for CAD.
Thus, the purpose of this study was to evaluate the association of FVL and FV HR2 SNPs in the occurrence of CAD, and further, to study the association and possible synergisms with traditional risk factors in predicting the risk of CAD.
Materials and Methods
Study Populations
Our study consisted of 200 Tunisian patients with symptomatic CAD (123 males and 77 females, with a mean age of 62.71 [12.57] years). Patients with significant coronary obstruction as determined by coronary angiography were selected consecutively from the Department of Cardiology.
In this study, only patients with evidence of myocardial infarction (MI), angina, a past history of prior angioplasty, CAD bypass grafting, or patients with more than 30% stenosis in 1 or more coronary arteries were included. However, patients with cardiomyopathy, valvular heart disease, congenital heart disease, or stroke were excluded from the study. Additionally, the control group consisted of 300 participants (186 males and 114 females, with a mean age of 62.50 [10.55] years) with no history of cardiovascular disease. Age- and gender-matched participants were recruited from the Military Hospital of Tunis. These participants can be military personnel or civilians. Despite the small number, this sample was a good representative of our population as patients and controls are referred to this hospital from all regions of Tunisia.
The risk factors considered were hypertension, T2DM, dyslipidemia, cigarette smoking, and a family history of CAD. Information about the conventional risk factors for CAD was obtained from all participants using a standard questionnaire, and the data were validated with reference to hospital case records. Hypertension was defined as a blood pressure of 160/95 mm Hg or greater on repeated measurements and/or the current use of antihypertensive drugs due to a previous history of arterial hypertension. 20 Diabetes mellitus was defined as hyperglycemia requiring antidiabetic drugs or a fasting blood sugar level exceeding 7.0 mmol/L (126 mg/dL). 21
Dyslipidemia was defined on the basis of the European guidelines on cardiovascular disease prevention in clinical practice that uses total cholesterol (TC) and low-density lipoprotein cholesterol (LDL-C) levels to guide treatment. In general, TC < 190 mg/dL and LDL-C < 115 mg/dL were regarded as normal (non-dyslipidemic). In patients with established cardiovascular disease (MI, acute coronary syndrome, and stroke) or T2DM, thresholds of TC < 175 and LDL-C < 100 mg/dL were applied. Patients exceeding either threshold were considered dyslipidemic. High-density lipoprotein and triglycerides were not used to define dyslipidemia. 22 Cigarette smoking was assessed by asking participants about prior and current history of smoking habits. A family history of CAD was defined as having a first degree relative with established CAD before 55 years of age in men and 65 years in women. 23
All participants in the study gave informed consent for giving a blood sample for genetic analysis. The study protocol was approved by the Ethics Committee of the Military Hospital of Tunis and has, therefore, been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Genotyping
Genomic DNA was extracted from peripheral blood leukocytes with DNA extraction kit (QIAmp blood kit; Qiagen GmbH, Hilden, Germany) according to the manufacturer’s protocol. The amplification with primers was used to amplify the genomic DNA. Factor V gene polymorphisms were analyzed by polymerase chain reaction (PCR)-restriction fragment length polymorphism (RFLP) using MnlI for FVL 24 and RsaI for FV HR2. 25 Digested PCR products were electrophoresed on agarose gels.
The quality control for genotyping accuracy for both SNPs was established by duplicating 10% of DNA samples. No discrepancies were observed. Further, the results were verified independently with reverse hybridization strip assay, a method recommended for ease of use and for obtaining results as equally reproducible as RFLP. 26 Genotypes were confirmed by random molecular hybridization of 10% of the samples using CVD StripAssay (ViennaLab, Vienna, Austria) which showed 100% agreement with.
Statistical Analysis
Genotype distribution and allele frequencies were represented as absolute numbers and percentages. Differences between cases and controls were evaluated by using the χ2 test or Fisher exact test for qualitative variables and the Student t test for quantitative variables. The associations between conventional risk factors and genotypes with CAD were reported using odds ratio (OR) with a 95% confidence interval (CI). Conditional multivariate logistic regression was applied to analyze factors associated with the risk of CAD. Conditional logistic regression analysis is the most common and conventional method applied for analyzing data of a matched case–control study. In this study, the matching criteria applied were gender and age at the time of study. 27,28
Probability values (P < .05) were considered statistically significant. Genotype distributions were in Hardy-Weinberg equilibrium as assessed by the χ2 test. All association analyses were carried out using SPSS software, version 21 (IBM, Armonk, New York).
Results
Demographic data are shown in Table 1. The case and control groups did not differ significantly in terms of age, sex, and smoking. The prevalences of diabetes, hypertension, dyslipidemia, and family history of CAD were significantly higher in the CAD group as compared to controls.
Clinical Characteristics of Study Participants.a
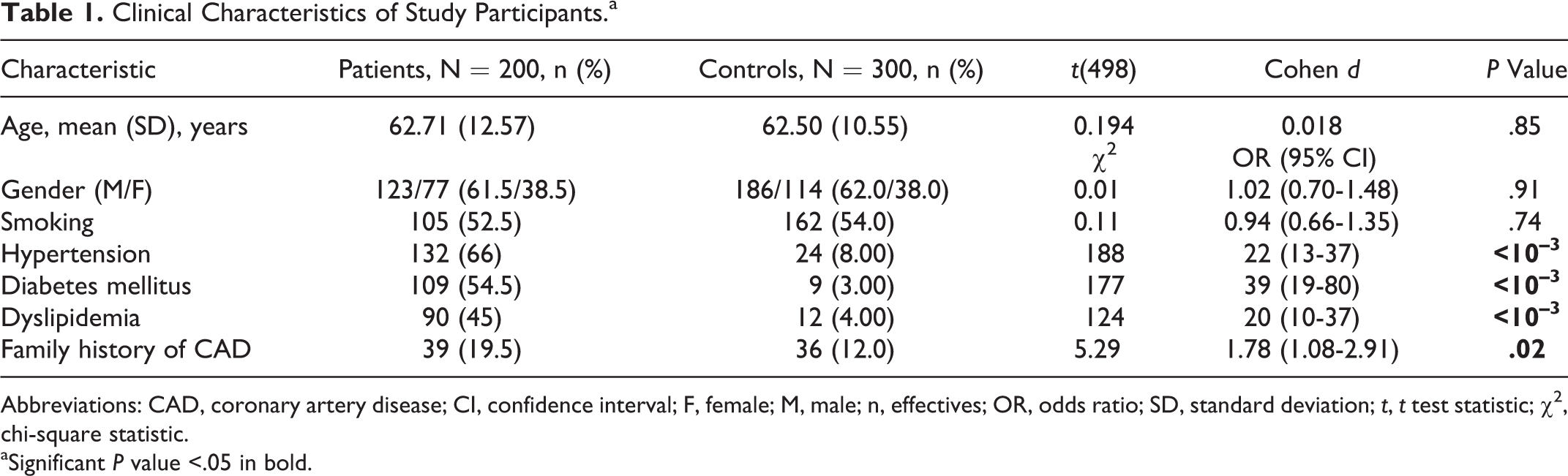
Abbreviations: CAD, coronary artery disease; CI, confidence interval; F, female; M, male; n, effectives; OR, odds ratio; SD, standard deviation; t, t test statistic; χ2, chi-square statistic.
aSignificant P value <.05 in bold.
The frequencies of the FV (G1691A and A4070G) genotypes in our study (Table 2) were in Hardy-Weinberg equilibrium for both patient and control populations. The distribution of the FVL heterozygote genotypes and mutant allele (A) was significantly different between the study and control groups (P < 10–3, OR = 4.03, 95% CI = 2.1-7.6; P < 10–3, OR = 2.81, 95% CI = 1.6-4.9), respectively (Table 2). However, the distribution of FV HR2 genotypes was not significantly different between the study group and control (P = .89; Table 2).
Distribution of FV Leiden and FV R2 (Genotypes and Alleles) in Coronary Artery Disease for Patients and Controls.a
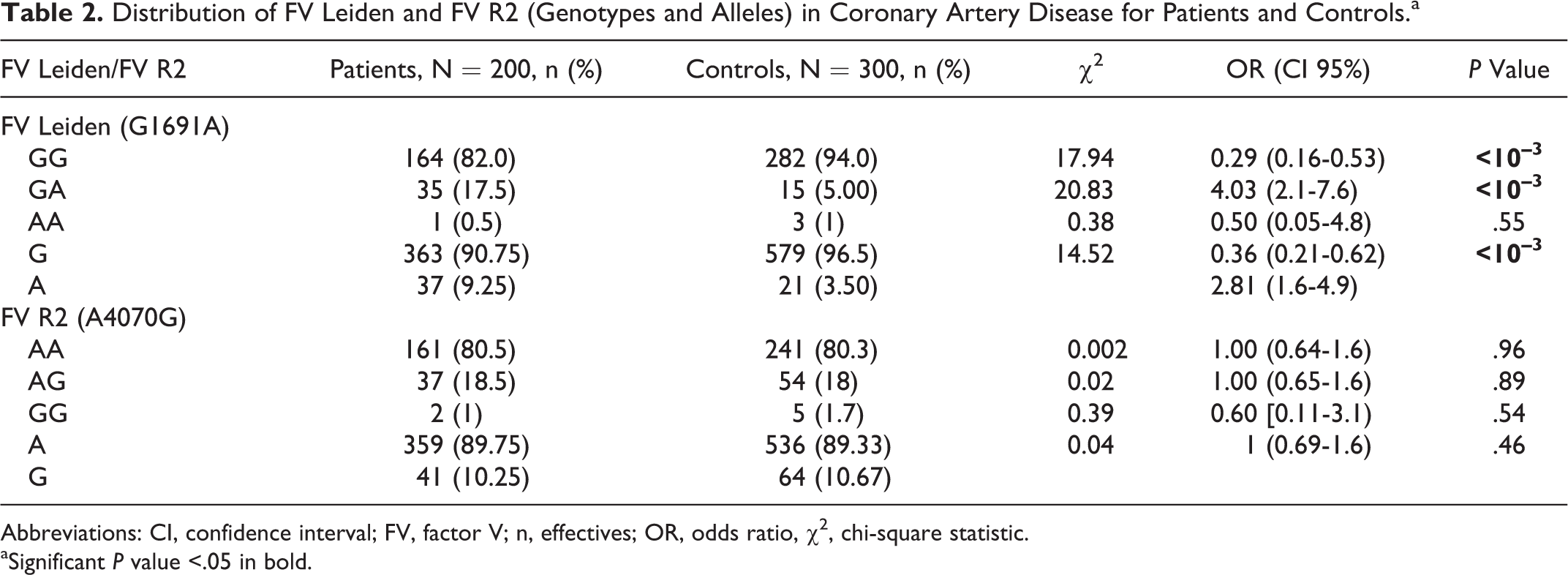
Abbreviations: CI, confidence interval; FV, factor V; n, effectives; OR, odds ratio, χ2, chi-square statistic.
aSignificant P value <.05 in bold.
The conditional multivariate logistic model indicates that the FVL genotype (GA + AA, OR = 5.05, 95% CI = 1.70-15.0), hypertension (OR = 6.05, 95% CI = 2.85-12.9), diabetes (OR = 31.9, 95% CI = 8.43-121), dyslipidemia (OR = 4.46, 95% CI = 1.81-11.0), and age (OR = 1.03, 95% CI = [1.00-1.06) are statistically significant independent risk factors for CAD. Family history of CAD was a significant variable in the univariate analysis; however, this parameter lost significance in multivariate analysis (Table 3). These results indicated that diabetes is the most significant risk factor. Dyslipidemia, hypertension, and FVL */A genotypes all carry commensurate risk. Age contributes a much smaller adjusted risk with a 3% increase in odds per year.
Conditional Multivariate Logistic Regression Model Showing Significant Risk Factors Having Association With CAD.a,b
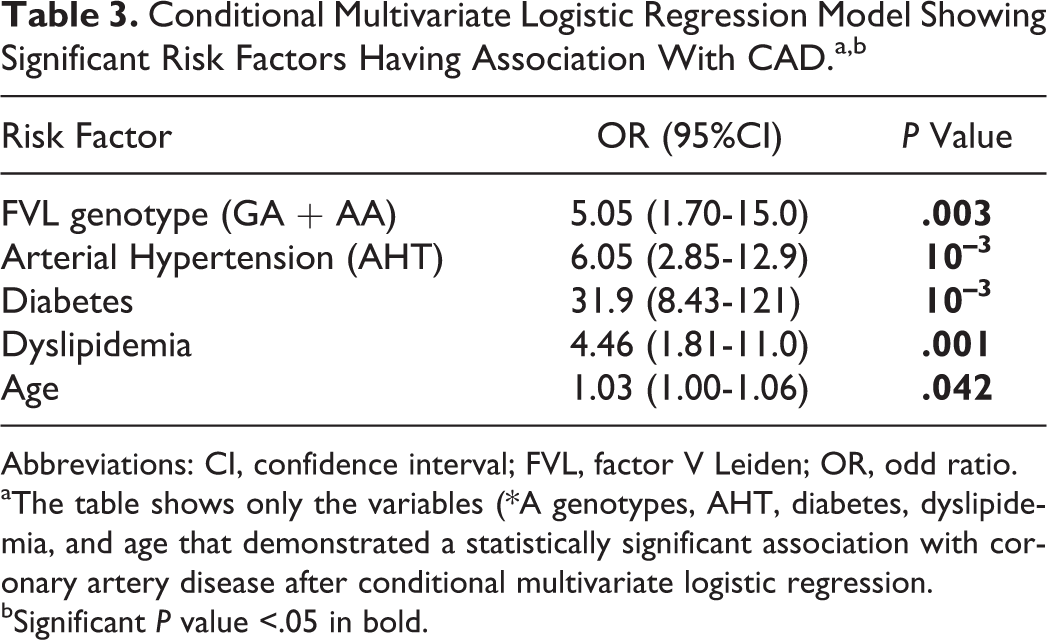
Abbreviations: CI, confidence interval; FVL, factor V Leiden; OR, odd ratio.
aThe table shows only the variables (*A genotypes, AHT, diabetes, dyslipidemia, and age that demonstrated a statistically significant association with coronary artery disease after conditional multivariate logistic regression.
bSignificant P value <.05 in bold.
The influence of the genotypes with or without consideration of cardiovascular risk factors was assessed in stratified groups of participants (Table 4). Carriers of the FVL (GA + AA) genotypes were found at commensurate across both genders. In contrast, FVL (GA + AA) carriers among nonsmokers (OR = 5.5; 95% CI= 2.1-14.4) were at a greater risk as compared to (GA + AA) among carrier smokers (OR = 2.4; 95% CI = 1.1-5.3). Moreover, we did not find any significant interaction of FVL and FV HR2 polymorphisms with hypertension, diabetes, dyslipidemia, and a family history of CAD.
Results of Interactions FVL (GA + AA) Versus GG and FV R2 (AG + GG) Versus AA by Stratum for Patients Versus Controls.a
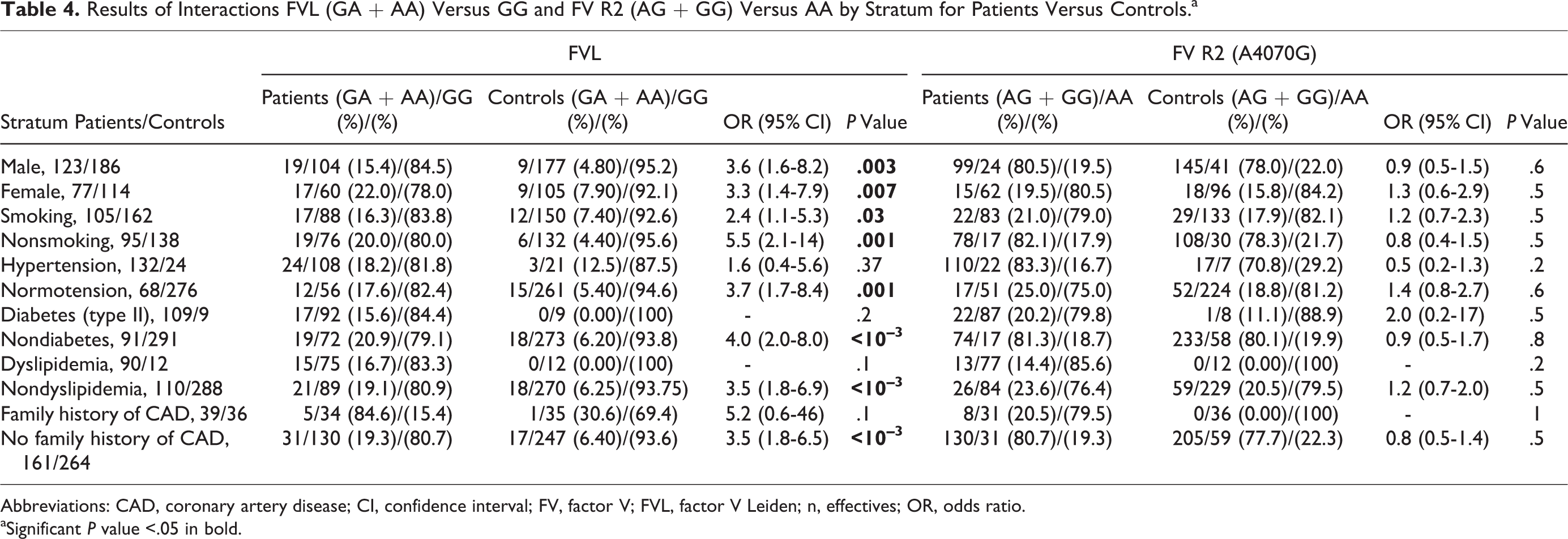
Abbreviations: CAD, coronary artery disease; CI, confidence interval; FV, factor V; FVL, factor V Leiden; n, effectives; OR, odds ratio.
aSignificant P value <.05 in bold.
We further analyzed the association of the FVL */A genotype with the risk of MI adjusted by sex, age, smoking, hypertension, diabetes, dyslipidemia, and family history of CAD. Patients with CAD were divided into 2 subgroups (Table 5) according to MI status. The analysis does not show a significant association for the FVL GA + AA genotype between the positive MI and negative MI groups.
The Prevalence of FVL (GA + AA) Polymorphism in Patients With CAD Having MI and Without MI and in Controls.a,b
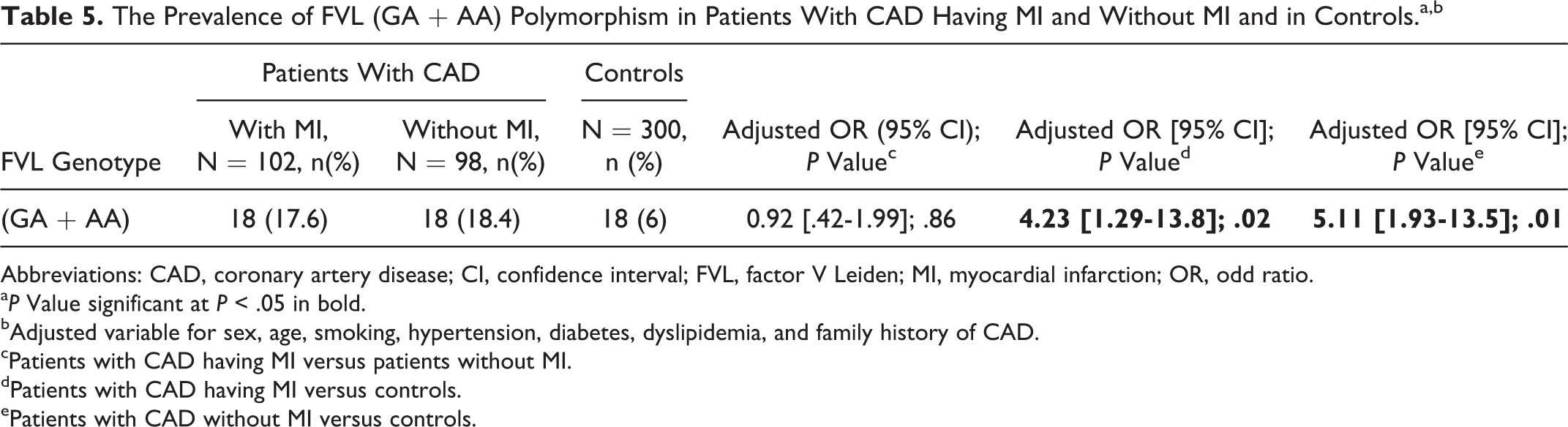
Abbreviations: CAD, coronary artery disease; CI, confidence interval; FVL, factor V Leiden; MI, myocardial infarction; OR, odd ratio.
a P Value significant at P < .05 in bold.
bAdjusted variable for sex, age, smoking, hypertension, diabetes, dyslipidemia, and family history of CAD.
cPatients with CAD having MI versus patients without MI.
dPatients with CAD having MI versus controls.
ePatients with CAD without MI versus controls.
Furthermore, comparing patients with CAD with and without MI to the controls, the frequency of the GA + AA genotype is significantly higher in patients with CAD for either MI status (P = .02, OR = 4.23, 95% CI = 1.29-13.8; P = .01, OR = 5.11, 95% CI = 1.93-13.5), respectively.
Discussion
There is ample evidence that, in addition to environmental risk factors, genetic factors and the interactions among them can contribute to the pathogenesis of CAD. Among these factors, genes involved in homeostasis and coagulation are excellent candidate risk factors for CAD and its thrombotic complications. 3,29 The aim of this study was to investigate the associations of FVL and FV HR2 gene polymorphisms alone and with traditional risk factors with the onset of CAD.
Our data indicate that hypertension, diabetes, dyslipidemia, and smoking (only in males) are independent risk factors associated with CAD. In several studies, these factors are consistently and independently related to CAD. 30 –32 The evidence is based on numerous prospective epidemiological studies and clinical observations in the general population. 33,34 Our previous study explains the pathophysiology mechanisms of diabetes, hypertension, and dyslipidemia in the contribution of CAD. 35
The role of the FV G1691A and A4070G gene polymorphisms in the development of CAD is controversial. 36 From our data, we concluded that the frequency of the FVL GA genotype was significantly different between the study groups. This result is consistent with numerous studies. 3,16,37,38 In contrast, other findings do not support an association between the presence of this genotypic variant and the incidence of CAD. 39 –42 Furthermore, our multivariate logistic regression revealed that the association of FVL (GA + AA) variants is independent of other confounding variables. Further, the study found that the distribution of the FV HR2 gene polymorphism was not significantly different between the patient and control groups and this result is similar to other studies on CAD. 2,3,37,39,40,43 In contrast, however, in the study by Fekih-Mrissa et al, the heterozygous variant of FVL (G1691A) and the heterozygous variant of FV A4070 gene polymorphism were both significantly associated with vascular access thrombosis in hemodialysis patients, respectively, but in the study by Aleksova et al, FV HR2 was significantly associated with an increased risk of VTE while FVL was not. 44,45
The contribution of thrombogenic risk factors in the development of atherosclerosis has been less well characterized. Several studies have examined the relationship between the development of atherosclerosis and prothrombotic genetic markers such as G1691A and A4070G polymorphisms. They demonstrated that the FVL and FV HR2 variants are associated with APC resistance and, further, that the anticoagulant activity of FV plays a pivotal role in the regulation of thrombin formation. 12,46,47 Moreover, an alteration in the FV protein function leads to an increased thrombin generation, 48 and the chronic influence of higher levels of thrombin can cause the development and/or progression of atherosclerosis. 46,49,50 A recent meta-analysis of 191 studies, investigating 7 common hemostatic gene polymorphisms in cardiovascular disease, indicated that both 1691A variant of the FV gene and 20210A variant of the prothrombin gene, promoting thrombin generation in blood, might be associated with the risk of CAD. 51
The relationship between CAD and thrombin can be explained by several biological processes. Indeed, thrombin impairs endothelial barrier function. It induces endothelial cell contraction, leading to an increased permeability and resulting in plasma extravasations and edema. 52 Furthermore, several reports indicate the potentiating effect of thrombin on reactive oxygen species production in humans, leading to the formation of an atheromatous plaques. 53,54
Additionally, thrombin has been shown to augment levels of mRNA that encode monocyte chemoattractant protein 1, a well-characterized chemokine, abundant in human atherosclerotic plaques. 55 In fact, thrombin is a central coagulation protease. It is known to promote numerous pro-atherogenic actions in vitro such as activation of protease-activated receptor 1, endothelial permeability, migration and proliferation of vascular smooth muscle cells, platelet activation, leukocyte adhesion and recruitment, cytokine and chemokine production, vascular calcification, angiogenesis, and apoptosis. 53,56,57 In addition, a study by Borissoff et al provided substantial new evidence showing that control of coagulation via thrombin inhibition is a potential new therapeutic target for treating atherosclerosis. 58
The study population was subgrouped by risk factors such as smoking, diabetes, hypertension, dyslipidemia, and a family history of CAD. We did not find any significant interaction of FVL and FV HR2 mutations with hypertension, diabetes, dyslipidemia, and family history of CAD. We observed that FVL (GA + AA) carriers among nonsmokers were at a greater risk as compared to (GA + AA) carrier smokers. These results showed that the FVL mutation is an independent risk factor in the occurrence of CAD. Other studies have been noted that there was a concomitant risk with the presence of the FVL mutation and smoking, besides with FVL mutation and metabolic risk. 59 –61
Our work has several limitations. The results are preliminary given the small number of patients. The correlation of genotype with the level of thrombin generation would also be of interest in future studies.
Furthermore, in this study, only 2 widely studied missense SNPs located in the FV gene (R506Q [rs6025, G1691A] and H1299R [rs1800595, A4070G]) were assessed. However, there exists other FV gene missense SNPs that were not examined in this CAD study. These missense SNPs, R306G (rs118203905, A1090G), R306T (rs118203906,G1091C), I359T (rs118203911,T1250C), K830R (rs4524, A2663G), H837R (rs4525, A2684G), K897E (rs6032, A286,3G), L1257I (rs1046712, C3943A), and P1376S (rs9332608, C4300T), as described by Vos, 15 could have functional impacts and could be associated with CAD.
Moreover, other FV gene polymorphisms, in addition to FVL and H1299R, could be studied in concert using haplotype analysis. This is a more powerful tool for analysis than single SNP analysis. 62 Haplotype-based association analysis could be conducted, for example, by first applying either Haplotyper, 63 Haploview, 64 or Phase 65 software to construct multi-SNP haplotype phases followed by performing haplotype-specific association tests. This could reveal specific multi-SNP haplotype(s) that are associated with CAD.
Conclusion
Coronary artery disease is a complex disease and, pathophysiologically, is the result of multiple genetic factors, environmental factors, and often the conjunction of the 2. The results of the present study suggest that FVL may increase the risk of CAD. The FVL mutation is an independent risk factor whose effect is not modified by other traditional risk factors (smoking, diabetes, hypertension, dyslipidemia, and a family history of CAD) in increasing the risk of the disease. However, analysis of the FV HR2 variation does not show any statistically significant association with the disease. Future studies in a larger sample will be required to clarify the effect of FVL and FV HR2 mutations alone and with concomitant risk factors on CAD.
Footnotes
Acknowledgment
The authors would like to thank Dr Christian Winchell for his precious help in correcting this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.