
Abstract
The objective of this literature review was to estimate the incidence of thrombosis and thromboembolism associated with the superior cavopulmonary anastomosis (SCPA) procedure and its variants and to examine current thromboprophylaxis regimens utilized. MEDLINE and EMBASE were searched from inception to August 2017 for all prospective and retrospective cohort studies explicitly reporting incidence of thrombosis, thromboembolism, or shunt occlusion in neonates, infants, and children undergoing 1 or more variants of the SCPA procedure. End points included thrombotic events and thromboembolic events (strokes and pulmonary embolisms) as primary outcomes, and overall mortality as a secondary outcome, at the last available follow-up time point. Of 1303 unique references identified, 13 cohort studies were deemed eligible. Reported incidence of thrombosis and thromboembolic events ranged from 0% to 28.0% and from 0% to 12.5%, respectively. Reported incidence of major bleeding events ranged from 0% to 2.9%. Reported overall mortality ranged from 2.5% to 50.5% across studies. Thromboprophylaxis protocols varied across institutions and studies, most commonly involving unfractionated heparin (UFH), warfarin, enoxaparin, acetylsalicylic acid (ASA), or combinations of ASA and warfarin, ASA and low-molecular-weight heparin (LMWH), UFH and LMWH, and UFH and ASA; several studies did not specify a protocol. Due to substantial variability in reported event rates, no clear correlation was identified between prophylaxis protocols and postoperative thrombotic complications. Despite guidance recommending postoperative UFH as standard practice, thromboprophylaxis protocols varied across institutions and studies. More robust trials evaluating different thromboprophylaxis regimens for the management of these patients are warranted.
Keywords
Background
The superior cavopulmonary anastomosis (SCPA) procedure represents the second step of the 3-staged palliative strategy for patients with single-ventricle physiology and involves redirecting deoxygenated blood directly from the superior vena cava (SVC) to the pulmonary artery (PA), bypassing the heart and effectively limiting ventricular workload exclusively to systemic circulation output. 1
Superior cavopulmonary anastomosis is typically achieved with 1 of 2 approaches: the bidirectional Glenn (BDG) and the hemi-Fontan. The classical BDG procedure consists of division of the SVC from the right atrium (RA), an incision made on the PA, and suturing of the SVC to the RA incision, creating an end-to-side SVC-PA anastomosis. 2 In contrast, the hemi-Fontan procedure preserves the SVC-RA confluence, creating an anastomosis between the SVC-RA confluence and the central and branch PAs in an end-to-end fashion. 3
Thrombotic and thromboembolic complications represent important considerations in the postoperative management of these patients. While thrombotic complications have been noted to be infrequent postoperatively, many patients proceed to the Fontan procedure, suggesting there may be a role for thromboprophylaxis in the routine management of these patients to increase the likelihood of successful conversion. 4 Recommendations from the American College of Chest Physicians Evidence-Based Clinical Practice Guidelines for Antithrombotic Therapy and the Prevention of Thrombosis (9th ed) encourage the use of postoperative unfractionated heparin (UFH) for neonates and children (grade 2C). 4 Summarized recent data regarding postoperative thromboprophylaxis protocols and risks of thrombosis, thromboembolism, and mortality remain limited. To the best of our knowledge, no randomized controlled trials comparing thromboprophylaxis strategies have been published.
The purpose of this literature review is (1) to estimate the risk of thrombosis and thromboembolism associated with the SCPA procedure and (b) to examine current thromboprophylaxis regimens utilized and their effectiveness in reducing thrombosis and thromboembolic risks. This is the third in a series of 3 literature reviews evaluating risk of thrombosis and thromboembolism and postoperative thromboprophylactic protocols in use with each stage of the 3-stage palliative procedure for hypoplastic left heart syndrome patients. 5,6
Methods
Data Sources and Searches
We searched the central MEDLINE and EMBASE (to August 2017). We restricted the search to humans and infants and children. A detailed search strategy for both MEDLINE and EMBASE, developed and conducted with the help of a librarian (P.L.), is provided in Appendix A.
After the removal of identifiable duplicate hits, pairs of 2 investigators (N.B. and A.Y.) independently screened each title and abstract retrieved from the search. Consensus was reached on decisions to include or exclude potentially eligible studies, with discrepancies resolved by discussion between the 2 reviewers and adjudication by a third reviewer (A.A.) to make the final decision on study eligibility for full-text review as necessary. For all eligible titles and abstracts, full-text articles were retrieved for detailed review and were independently screened in duplicate (N.B. and A.Y.), with discrepancies resolved by discussion and adjudication by a third reviewer (A.A.) as necessary. Relevant data were then extracted from eligible studies as per a predetermined data extraction form (Appendix B). Reference lists of eligible systematic reviews were screened by a reviewer to identify potentially eligible studies.
Study Eligibility
We included all prospective or retrospective cohort studies that included neonates, infants, or children undergoing 1 or more variants of the SCPA procedure. Articles were considered eligible if they met the following criteria: (1) prospective or retrospective cohort study design or a systematic review of such studies, (2) involved a pediatric population undergoing either (or both) of the BDG or hemi-Fontan procedures, and (c) explicit reporting of outcomes related to thrombotic or thromboembolic events. We excluded clinical trials, case reports and case series, narrative reviews, and other secondary study designs and studies that did not make explicit mention of the primary outcomes of interest in the abstract. Studies exclusively including cases with thrombotic events and thromboembolic events were excluded. Studies reporting outcomes for interventions subsequent to SCPA operation with no explicit reporting of outcomes related to SCPA were excluded.
Data Abstraction
We abstracted the following information from each eligible study: sample size; period of data collection; description of procedure; patient age, sex, weight, relevant comorbidities, or complications; prophylaxis type, dose, frequency and duration, and proportion of patients receiving prophylaxis; duration of follow-up (days); thrombotic events (primary outcome) reported or not reported, definition of outcome, number of patients with events, and number of patients evaluated; thromboembolic events (primary outcome) reported or not reported, definition of outcome, number of patients with events, and number of patients evaluated; and mortality (secondary outcome) incidence, number of deaths, and number of patients evaluated.
The Newcastle-Ottawa Scale (NOS) for cohort studies was considered for evaluation of risk of bias. However, given studies generally included a single cohort where SCPA was the exposure and baseline assessments for thrombosis and embolisms were not conducted, the NOS’ criteria related to nonexposed cohort selection, ascertainment of exposure, demonstration of outcomes of interest not being present at baseline, and cohort comparability were deemed not applicable. As such, formal judgments regarding risk of bias were not conducted.
Data Synthesis
Studies were stratified by type of prophylaxis provided and further by type of procedure. Data were presented as proportions for the outcomes of interest for each study independently and were synthesized qualitatively without a meta-analysis.
Results
Of all, 1303 unique references were identified between Ovid MEDLINE and EMBASE searches using our search strategy (Appendix A). Of these, 34 were considered potentially eligible following title and abstract review, and 13 fulfilled eligibility criteria and were included in our literature review following full-text review. 7 –19 No additional eligible studies were identified with a review of the reference lists of included studies from the search (Figure 1).
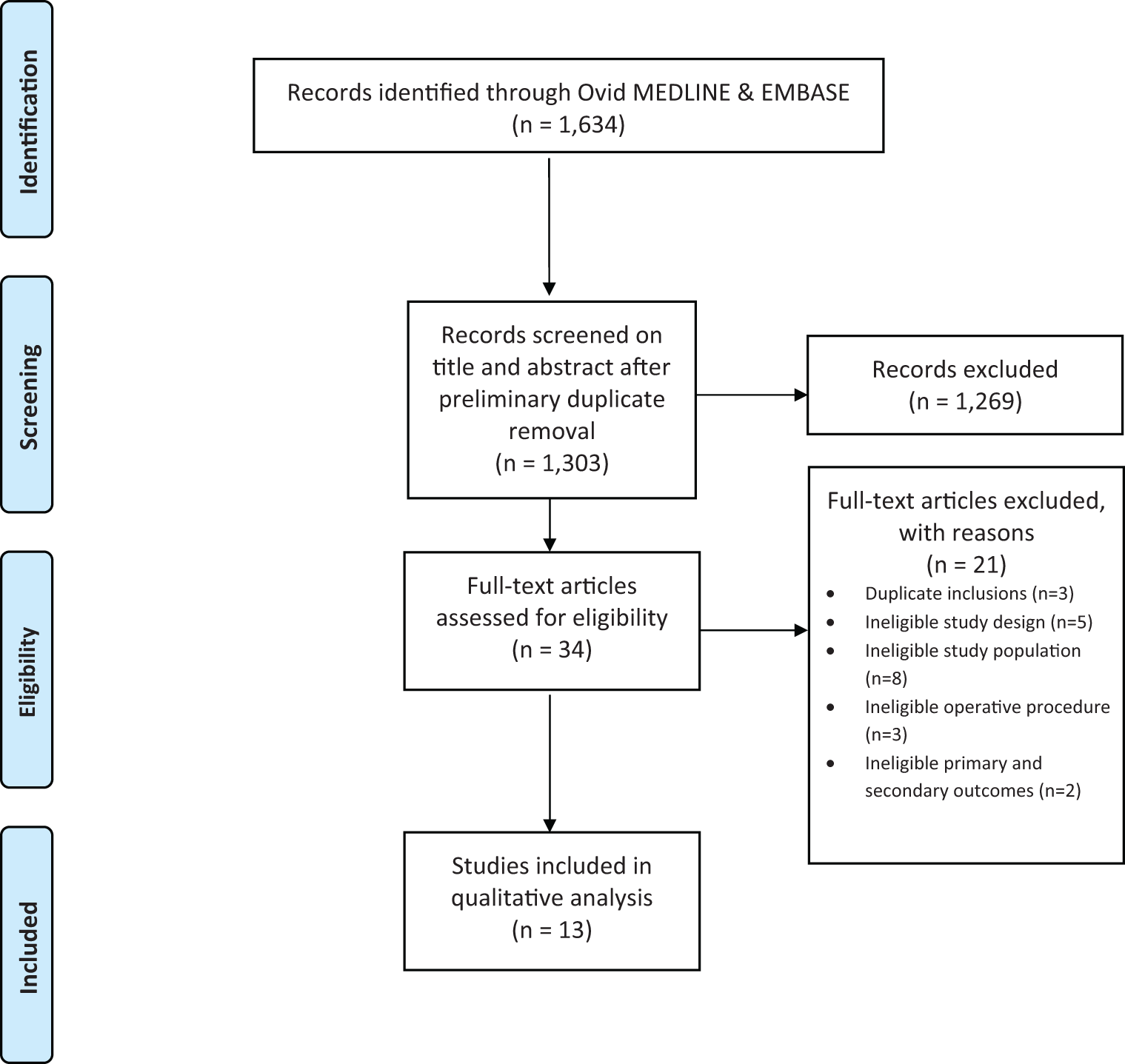
Study flowchart.
Study Characteristics
A total of 1136 patients (375 males, 237 females, 524 not reported) were included across the 13 eligible studies, 4 (30.8%) of which included over 100 patients. Eight (61.5%) studies included patients who underwent the BDG procedure; 9 (69.2%) studies included patients who underwent the hemi-Fontan procedure. The primary indication for operation for the majority of included patients was hypoplastic left heart syndrome. Six (46.2%) studies were conducted in the United States, 2 (15.4%) studies were conducted in each of Canada and Germany, and 1 (7.7%) study was conducted in each of Poland, Japan, and China (Table 1).
Characteristics of Included Studies.
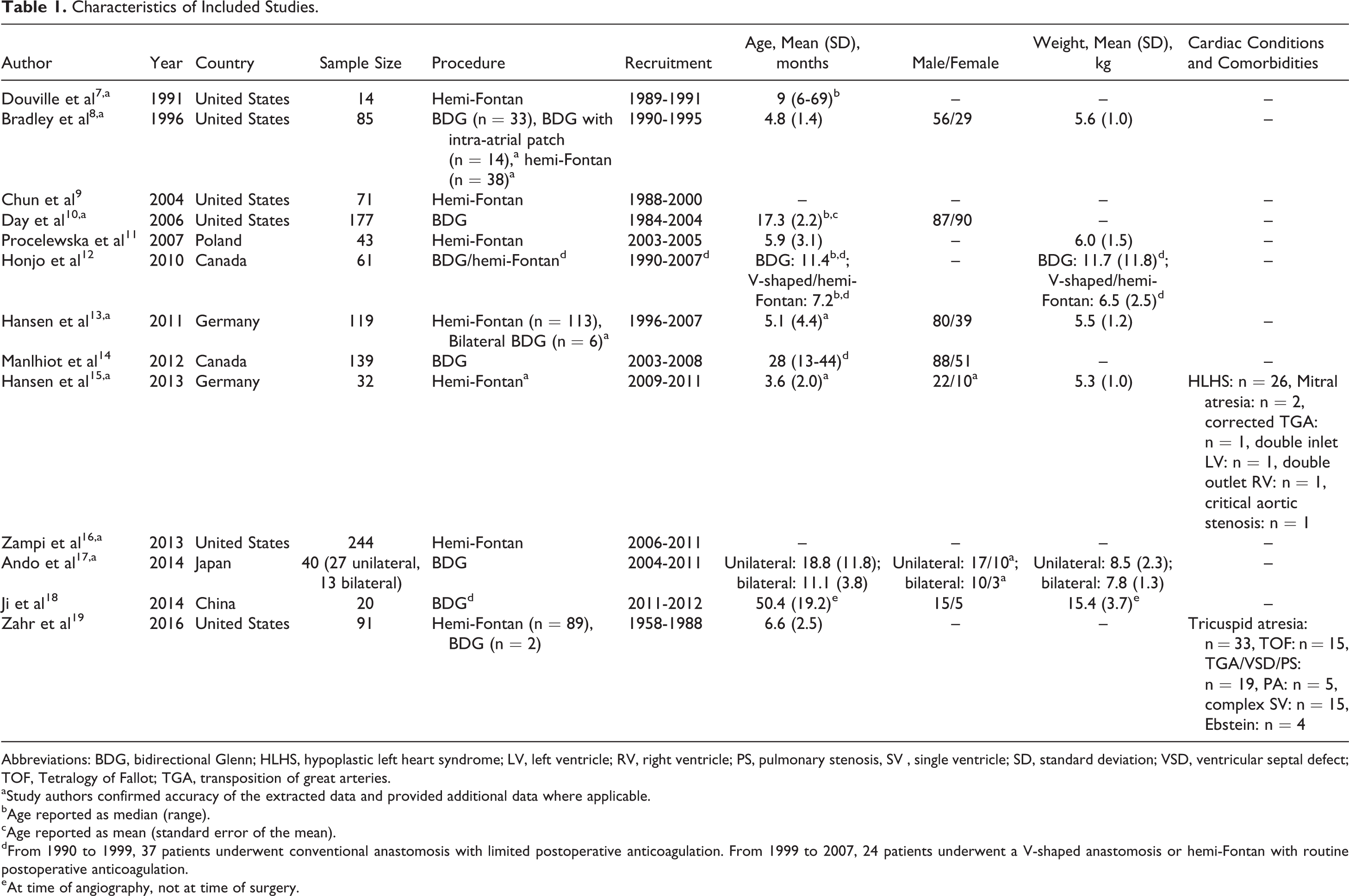
Abbreviations: BDG, bidirectional Glenn; HLHS, hypoplastic left heart syndrome; LV, left ventricle; RV, right ventricle; PS, pulmonary stenosis, SV , single ventricle; SD, standard deviation; VSD, ventricular septal defect; TOF, Tetralogy of Fallot; TGA, transposition of great arteries.
aStudy authors confirmed accuracy of the extracted data and provided additional data where applicable.
bAge reported as median (range).
cAge reported as mean (standard error of the mean).
dFrom 1990 to 1999, 37 patients underwent conventional anastomosis with limited postoperative anticoagulation. From 1999 to 2007, 24 patients underwent a V-shaped anastomosis or hemi-Fontan with routine postoperative anticoagulation.
eAt time of angiography, not at time of surgery.
Among the 13 eligible studies, 5 (38.5%) studies 10,11,14,16,17 reported on postoperative UFH, warfarin, low-molecular-weight heparin (LMWH), or acetylsalicylic acid (ASA) use alone; 4 (30.8%) studies 8,12,13,15 reported on combination UFH and ASA; 1 (7.7%) study 9 reported on combination ASA and warfarin; 1 (7.7%) study 14 reported on combination ASA and LMWH; 2 (15.4%) studies 12,16 reported on combination UFH and LMWH; and 4 (30.8%) studies 8,12,14,19 reported on a no-thromboprophylaxis protocol postoperatively.
Of note, Bradley et al initially followed a no-thromboprophylaxis protocol, subsequently introducing an UFH-ASA protocol. 8 Manlhiot et al followed different prophylactic protocols based on patient-related and operative characteristics; individual thrombotic and thromboembolic event data were not reported for each prophylactic protocol; as such, study findings were summarized separately from other included studies. 14 Two (15.4%) studies 7,18 did not explicitly report a thromboprophylaxis regimen (Table 2).
Prophylaxis Strategies Across Included Studies.
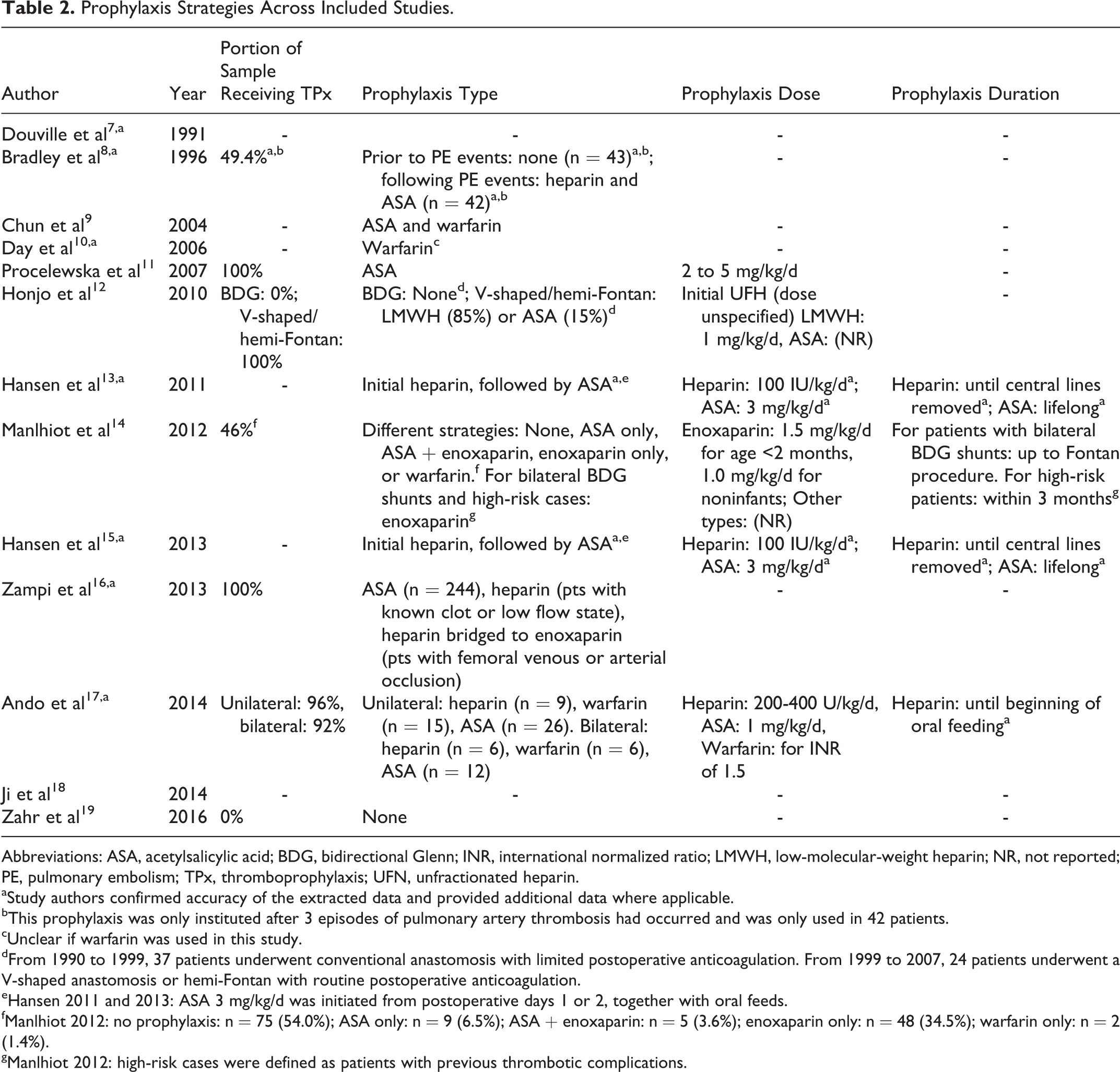
Abbreviations: ASA, acetylsalicylic acid; BDG, bidirectional Glenn; INR, international normalized ratio; LMWH, low-molecular-weight heparin; NR, not reported; PE, pulmonary embolism; TPx, thromboprophylaxis; UFN, unfractionated heparin.
aStudy authors confirmed accuracy of the extracted data and provided additional data where applicable.
bThis prophylaxis was only instituted after 3 episodes of pulmonary artery thrombosis had occurred and was only used in 42 patients.
cUnclear if warfarin was used in this study.
dFrom 1990 to 1999, 37 patients underwent conventional anastomosis with limited postoperative anticoagulation. From 1999 to 2007, 24 patients underwent a V-shaped anastomosis or hemi-Fontan with routine postoperative anticoagulation.
eHansen 2011 and 2013: ASA 3 mg/kg/d was initiated from postoperative days 1 or 2, together with oral feeds.
fManlhiot 2012: no prophylaxis: n = 75 (54.0%); ASA only: n = 9 (6.5%); ASA + enoxaparin: n = 5 (3.6%); enoxaparin only: n = 48 (34.5%); warfarin only: n = 2 (1.4%).
gManlhiot 2012: high-risk cases were defined as patients with previous thrombotic complications.
Thromboprophylaxis Protocols and Postoperative Outcomes
Overall, incidence of thrombotic and thromboembolic events ranged from 0% to 28.0% and 0% to 12.5%, respectively. Three studies reported rates of major bleeding or bleeding requiring reintervention, ranging from 0% to 2.9%. 10,17,20 Mortality rates ranged from 2.5% to 50.5%.
Incidence of thrombotic events ranged from 0% to 1.2% for single-agent prophylaxis (2 studies), 16,17 4.2% for UFH-ASA (1 study), 13 0% for warfarin-ASA (1 study), 9 1.2% for UFH-LMWH (1 study), 16 0% for no prophylaxis (1 study), 19 and 5.0% to 7.1% for no explicitly-reported thromboprophylaxis protocol (2 studies). 7,18
Incidence of thromboembolic events ranged from 0% to 2.9% for single-agent prophylaxis (4 studies), 10,11,14,17 0% to 12.5% for UFH-ASA (4 studies), 8,12,13,15 5.6% for warfarin-ASA (1 study), 9 4.2% for UFH-LMWH (1 study), 12 2.2% to 8.1% for no prophylaxis (3 studies), 8,12,19 and 7.1% for no explicitly-reported thromboprophylaxis protocol (1 study). 7
Reported mortality rates ranged from 2.5% to 7.9% for single-agent prophylaxis (3 studies), 10,14,17 3.1% to 12.5% for UFH-ASA (4 studies), 8,12,13,15 12.5% for UFH-LMWH (1 study), 12 7.9% to 50.5% for no prophylaxis (3 studies), 8,12,19 and 7.1% for no explicitly-reported thromboprophylaxis protocol (1 study). 7
Manlhiot et al applied a protocol involving several thromboprophylaxis protocols: no prophylaxis (54.0%), ASA only (6.5%), ASA + enoxaparin (3.6%), enoxaparin only (34.5%), and warfarin only (1.4%). Overall rates of thrombotic, thromboembolic, and mortality events across prophylactic regimens following SCPA were 28.0%, 2.9%, and 9.0%, respectively (Table 3). 14 The study reported a decreased risk of thrombotic complications postoperatively with enoxaparin compared to no prophylaxis (hazard ratio [HR] = 0.2; P = .04). The study found that use of prophylaxis after postoperative day 7 was associated with a lower risk of thrombotic complications and that premature birth (HR = 2.6; 1.1-6.0; P = .03) and postoperative extracorporeal membrane oxygenation (HR = 12.5; 3.0-21.7; P < .001) were most associated with increased risk of thrombotic complications postoperatively. 14
Postoperative Thrombotic Complications, Thromboembolic Complications, and Mortality Across Included Studies.
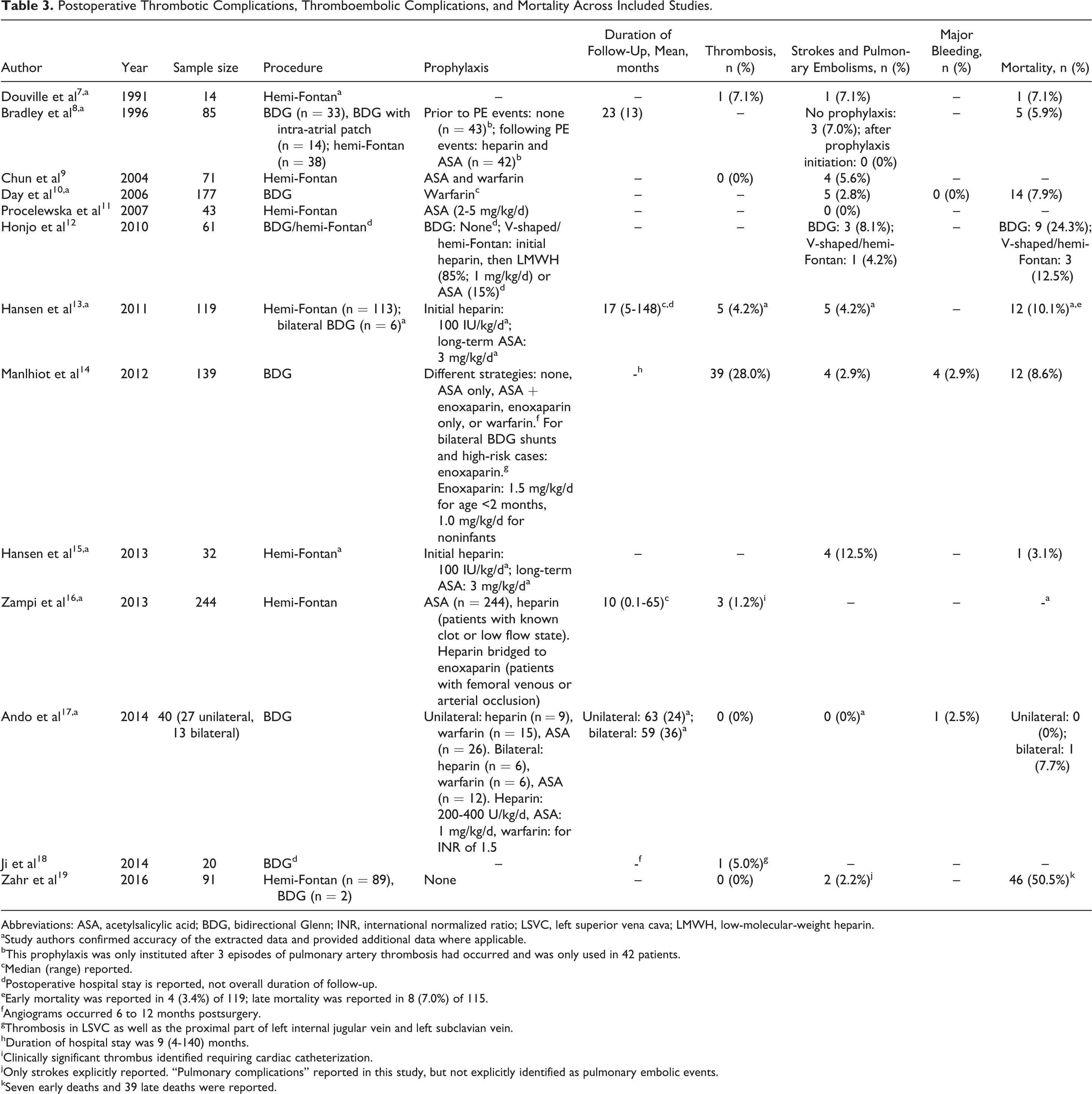
Abbreviations: ASA, acetylsalicylic acid; BDG, bidirectional Glenn; INR, international normalized ratio; LSVC, left superior vena cava; LMWH, low-molecular-weight heparin.
aStudy authors confirmed accuracy of the extracted data and provided additional data where applicable.
bThis prophylaxis was only instituted after 3 episodes of pulmonary artery thrombosis had occurred and was only used in 42 patients.
cMedian (range) reported.
dPostoperative hospital stay is reported, not overall duration of follow-up.
eEarly mortality was reported in 4 (3.4%) of 119; late mortality was reported in 8 (7.0%) of 115.
fAngiograms occurred 6 to 12 months postsurgery.
gThrombosis in LSVC as well as the proximal part of left internal jugular vein and left subclavian vein.
hDuration of hospital stay was 9 (4-140) months.
iClinically significant thrombus identified requiring cardiac catheterization.
jOnly strokes explicitly reported. “Pulmonary complications” reported in this study, but not explicitly identified as pulmonary embolic events.
kSeven early deaths and 39 late deaths were reported.
Discussion
Postoperative thrombotic and thromboembolic complications have been previously reported to be infrequent. 4 However, it is evident from the findings of our literature review that notable variability exists in both reported incidences of thrombosis and thromboembolic events and thromboprophylactic protocols used, with some studies reporting relatively high incidences of such complications despite prophylaxis.
The American College of Chest Physicians Evidence-Based Clinical Practice Guidelines for Antithrombotic Therapy and the Prevention of Thrombosis (9th ed.) recommends that neonates and children undergoing the BDG or bilateral cavopulmonary shunt procedure should receive postoperative UFH therapy (grade 2C). 4 Despite noting that thrombotic complications are infrequent, the guideline indicates that the completion of the Fontan procedure in many patients suggests a prophylaxis protocol may be beneficial to reduce subsequent risk of thromboembolic events. 4
Our findings suggest that thromboprophylaxis protocols vary across institutions and studies, among UFH and ASA, ASA and warfarin, ASA and LMWH, UFH and LMWH, single-agent UFH/warfarin/LMWH/ASA, or a no-thromboprophylaxis protocol postoperatively. While several studies reported on postoperative UFH use, they largely involved UFH as part of a protocol with other medications, and none reported outcome data specifically pertaining to UFH use alone.
In general, incidence of thrombotic and thromboembolic events ranged from 0% to 28.0% and 0% to 12.5% between studies, respectively. Mortality rates ranged from 2.5% to 50.5%. Due to the substantial variability in estimates with each postoperative thromboprophylaxis protocol and no robust studies supporting any single protocol, no clear relationship was identified between protocols and reduction in thrombosis and thromboembolic events.
It is important to recognize the potential risk of bleeding complications with thromboprophylaxis use. Several studies have demonstrated a relatively low overall incidence of these complications in pediatric patients. 20 –22 Only 3 included studies reported the incidence of major bleeding or bleeding requiring reintervention; all consistently reported low rates of such events. 10,17,20
It is also important to recognize that all included studies recruited patients prior to the release of the American College of Chest Physicians’ guideline recommendations. 4 As such, the penetration of these recommendations into clinical practice is challenging to assess based on our findings.
Our findings must be interpreted with several other limitations in mind. While the review is a comprehensive effort to evaluate the risk of thrombosis and thromboembolic complications and the postoperative thromboprophylaxis protocol used in this patient population, the lack of a meta-analysis limits the utility of our findings. Furthermore, while risk of bias wasn’t formally assessed, the retrospective nature, small sample sizes and poor reporting quality for outcomes of interest in the majority of studies limit the reliability of the review’s findings. The wide variability in study results further limits the generalizability of the findings. In addition, reported rates of thrombotic and thromboembolic complications may be underestimated, given that the majority of the studies included likely reported clinically relevant thrombotic complications. Lastly, several studies report pooled outcome data for patients with different thromboprophylactic protocols, preventing a clear assessment of which protocols were associated with the reported outcome events.
Conclusion
The incidence of thrombotic and thromboembolic complications following initial palliation for pediatric patients with single-ventricle physiology varies from 0% to 28.0% and 12.5%, respectively. They are accompanied by a relatively minor risk of bleeding events. While these thrombotic events have been reportedly infrequent and recent guidance suggests postoperative UFH as a standard prophylactic strategy, significant variance appears to exist in reported incidences of these complications as well as thromboprophylaxis protocols in use.
Our findings highlight the lack of a standardly used thromboprophylaxis protocol based on existing evidence despite existing guidelines. Randomized trials examining thromboprophylaxis protocols are warranted, alongside increased efforts to promote the adoption of a standard protocol for the postoperative management of these patients.
Footnotes
Appendix A
Appendix B
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.