
Abstract
Background:
The stage 1 Norwood procedure and its variants represent the first step of palliation for hypoplastic left heart syndrome. Although appropriate postoperative thromboprophylaxis is integral, significant variance remains across institutional practices. The purpose of this systematic review is to estimate the incidence of thrombosis and thromboembolism following the Norwood or modified Blalock-Taussig shunt procedure and examine current thromboprophylaxis regimens.
Methods:
Ovid MEDLINE and Embase were searched from January 2000 to June 2016 for primary studies explicitly reporting incidence of thrombosis, thromboembolism (strokes and pulmonary embolisms), or shunt occlusion in neonates, infants, and children undergoing the Norwood procedure or any variant. All-cause mortality was a secondary outcome of interest.
Results:
Of 887 identified articles, 15 cohort studies were deemed eligible, the majority including modified Blalock-Taussig shunt patients. Reported incidence of thrombosis ranged from 0% to 40%; thromboembolic events were rarely reported. Overall mortality ranged from 4.5% to 31.3% across studies. Although most studies involved the long-term acetylsalicylic acid use, thromboprophylaxis strategies varied across studies. Due to substantial variability in event rates, no correlation was identified with thrombotic complications.
Discussion:
Clinical practice guidelines recommend that patients receive intraoperative unfractionated heparin therapy and either aspirin or no antithrombotic therapy postoperatively. Our findings suggest a substantial risk of thrombosis and thromboembolism and demonstrate substantial variation in thromboprophylaxis practices.
Conclusion:
Although postoperative thromboprophylaxis seems optimal, it remains controversial whether the long-term aspirin use is most effective. Our findings highlight the lack of a gold-standard thromboprophylaxis strategy and emphasize the need for more consistency.
Background
Hypoplastic left heart syndrome is a univentricular congenital heart anomaly resulting in 2 anatomical ventricles but only 1 functional ventricle. Such a physiology is corrected by an invasive 3-staged surgical procedure in which systemic and pulmonary circuits are altered in order to reestablish hemodynamic stability. The stage 1 Norwood procedure represents the first step of the palliative strategy for these patients and involves directing blood away from the hypoplastic left ventricle by creating an atrial septal fenestration and allowing the stronger ventricle to pump blood to the rest of the body. 1,2 The surgical procedure also typically involves major reconstruction of the aortic arch and surgical reestablishment of the pulmonary circulation, which is primarily conducted in 1 of the 3 ways—a classical Blalock-Taussig (BT) shunt, a modified BT shunt (mBTS), or a Sano conduit.
The classical BT shunt procedure consists of a direct anastomosis between the subclavian artery and the ipsilateral pulmonary artery (PA) and consequently, involves antegrade flow into the upper extremity. The procedure has been largely replaced by the mBTS, which involves anastomosing the subclavian artery to the ipsilateral PA using an artificial shunt. The mBTS preserves vasculature of the upper extremity but results in low diastolic pressures, which poses a greater risk of diastolic steal from the coronary circulation. Introduced as an alternative to the mBTS in 2003, the Sano procedure involves a connection from the right ventricle (RV) to the PA using an artificial conduit. 3 Although the Sano procedure addresses the drawbacks of the mBTS, and preliminary data suggest the Sano modification is associated with better outcomes, 4 –6 it has still not been widely adopted due to the potential long-term risks.
In addition to these considerations, the Norwood procedures have been associated with other postoperative complications and mortality. 7 Hemodynamic abnormalities, conduit stenosis, cardiac output changes, arrhythmias, liver dysfunction, protein-losing enteropathy, and thrombotic complications are often reported postoperatively.
Appropriate prophylactic management is integral to the management of Norwood patients. However, there remains significant incongruity across studies with regard to both the diagnostic tools used to identify such events and different institutional prophylactic practices to minimize them. The purpose of this systematic review is—(1) to estimate the risk of thrombosis and thromboembolism associated with the Norwood procedure and (2) to examine current thromboprophylaxis regimens utilized and their effectiveness in reducing thrombosis and thromboembolic risks.
Methods
Data Sources and Searches
We searched Ovid MEDLINE and Embase (to June 2016). We restricted the search to human participants and infants and children. A detailed search strategy for both MEDLINE and EMBASE, developed and conducted with the help of a librarian (P.L.), is provided in ;Appendix A.
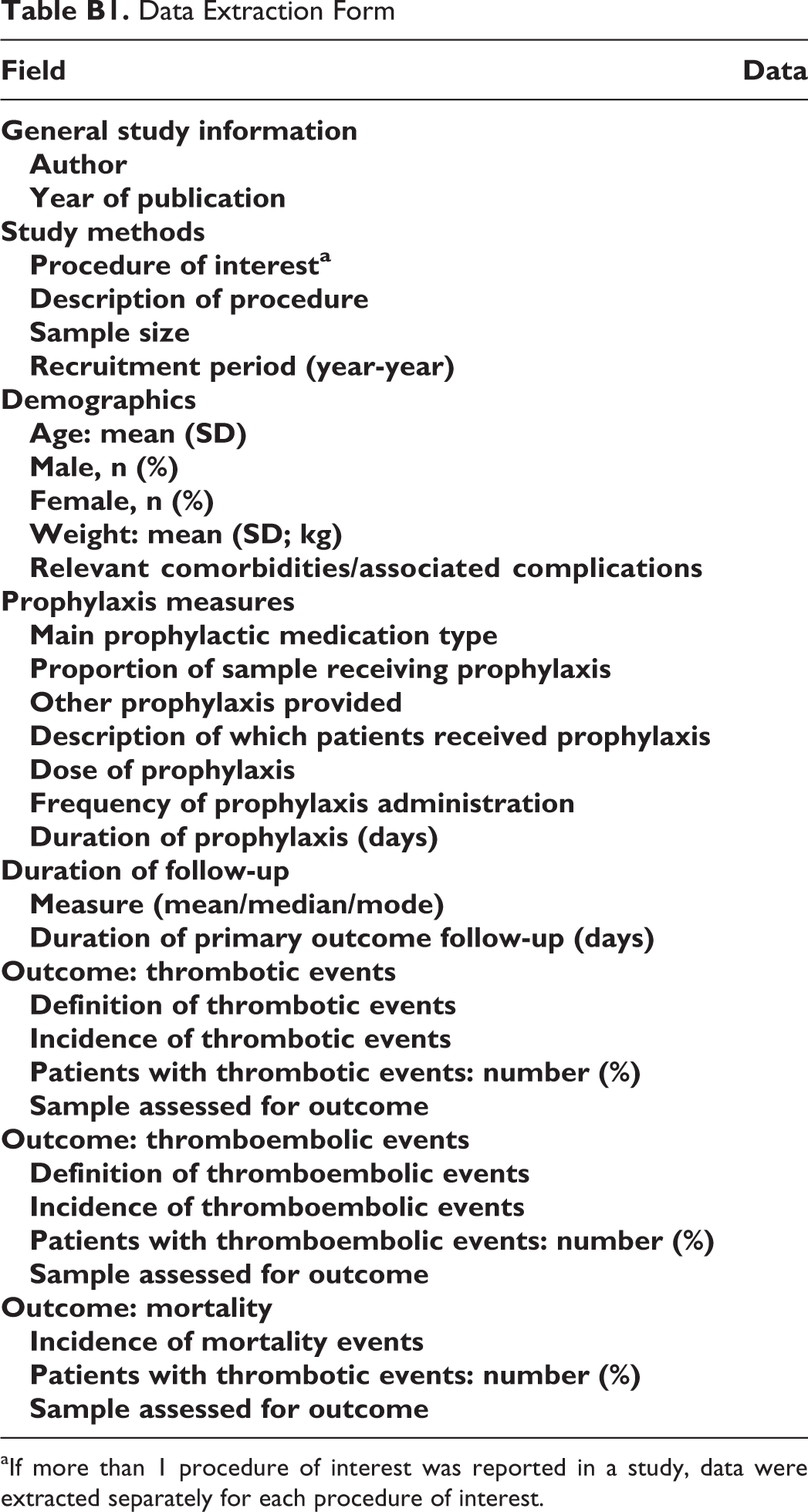
After the removal of identifiable duplicate hits, pairs of 2 investigators (N.B. and A.Y.) independently screened each title and abstract retrieved from the search. Consensus was reached on decisions to include or exclude potentially eligible studies, with discrepancies resolved by discussion between the 2 reviewers and adjudication by a third reviewer (A.A.) to make the final decision on study eligibility for full-text review as necessary. For all eligible titles and abstracts, full-text articles were retrieved for detailed review and were independently screened in duplicate (N.B. and A.Y.), with discrepancies resolved by discussion and adjudication by a third reviewer (A.A.) as necessary. Relevant data were then extracted from eligible studies as per a predetermined data extraction form (Appendix B). For every eligible systematic review identified, 1 reviewer examined the reference list to identify included citations to potentially eligible studies.
Study Eligibility
We included all prospective or retrospective cohort studies that included neonates, infants, or children undergoing the Norwood procedure or a similar variant procedure. Articles were considered eligible if they met the following criteria: (1) published in the year 2000 or after; (2) prospective or retrospective cohort study design or a systematic review of such studies; (3) involved a pediatric population undergoing 1 or more of the BT shunt, systemic-to-pulmonary connection, Norwood, mBTS, Sano, or RV-PA shunt procedure); and (4) explicit reporting of outcomes related to thrombosis, thromboembolism, and/or shunt occlusions. Given patients with a number of critical congenital heart disease lesions involving BT shunt and mBTS placement are at high risk of thrombosis and thromboembolism, all studies explicitly reporting on these adverse events in these patients were considered eligible. We excluded case reports and case series, narrative reviews and other secondary study designs, and studies that did not make explicit mention of the primary outcomes of interest in the abstract.
Data Abstraction
We abstracted the following information from each eligible study—sample size and period of data collection; description of procedure; patient age, sex, weight, relevant comorbidities, or complications; prophylaxis type, dose, frequency and duration, and proportion of patients receiving prophylaxis; duration of follow-up (days); thrombotic events (primary outcome) reported or not reported, definition of outcome, number of patients with events, and number of patients evaluated; thromboembolic events (primary outcome) reported or not reported, definition of outcome, number of patients with events, and number of patients evaluated; mortality (secondary outcome) incidence, number of deaths, and number of patients evaluated. Risk of bias was not formally evaluated, given that cohort representativeness, control group characteristics and comparability, and attrition as per the Newcastle-Ottawa Scale for cohort studies were not very applicable to our synthesis.
Data Synthesis
Studies were stratified by type of prophylaxis provided and further by type of procedure. Data were presented as proportions for the outcomes of interest for each study independently and was synthesized qualitatively without a meta-analysis.
Results
Eight hundred and eighty-seven references were identified between Ovid MEDLINE and Embase searches using our search strategy (Appendix A). Of these, 54 were considered potentially eligible following title and abstract review and 15 fulfilled eligibility criteria and were included in our systematic review following full-text review. 8 –22 No additional eligible studies were identified with a review of the reference lists of included studies from the search (Figure 1).
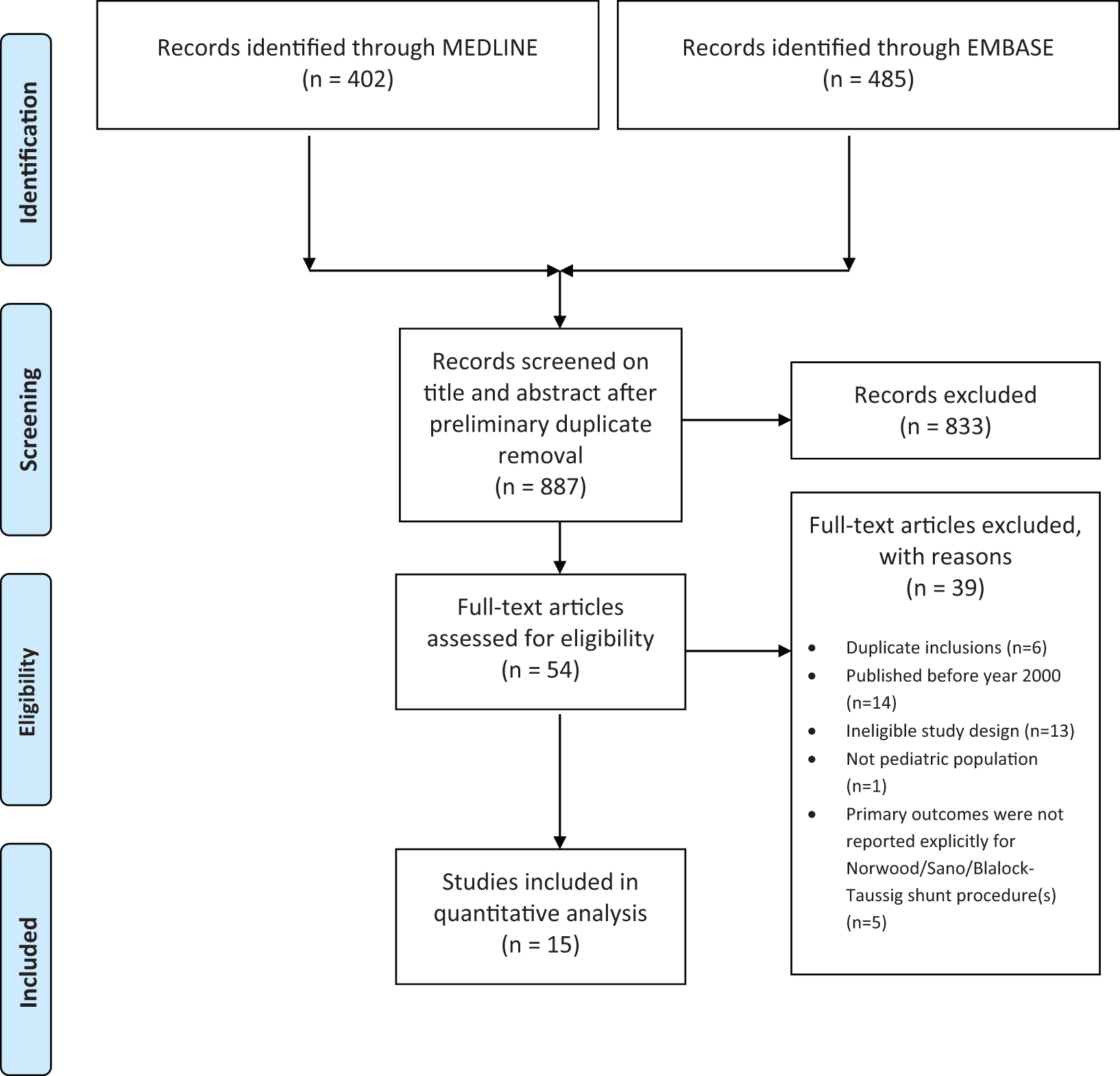
Study flowchart.
Study Characteristics and Risk of Bias
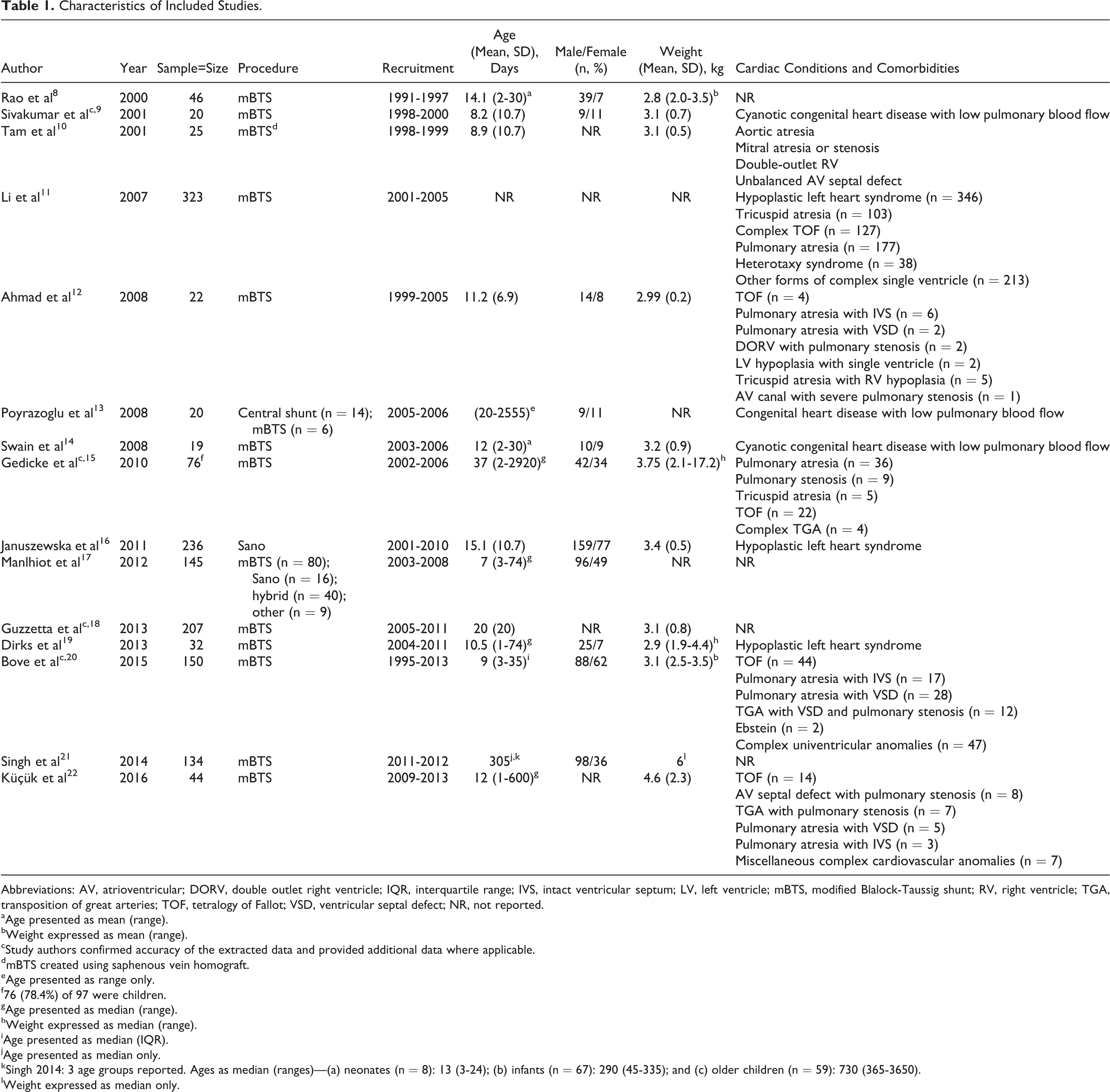
General study characteristics of the included studies are described in Table 1. A total of 1499 patients (589 males, 311 females, 599 not reported) were included across the 15 eligible studies 8 –22 ; 6 (42.9%) of these studies had sample sizes over 100 patients. 11,16 –18,20,21 Thirteen (92.9%) studies included patients who underwent the mBTS procedure 8 –15,17 –22 ; one of these studies also included patients who underwent a central shunt procedure, 13 and a second also included patients who underwent the Sano procedure, a hybrid procedure between the mBTS and Sano procedure, or an alternate related procedure. 17 The remaining study included only patients who underwent the Sano procedure. 16
Characteristics of Included Studies.
Abbreviations: AV, atrioventricular; DORV, double outlet right ventricle; IQR, interquartile range; IVS, intact ventricular septum; LV, left ventricle; mBTS, modified Blalock-Taussig shunt; RV, right ventricle; TGA, transposition of great arteries; TOF, tetralogy of Fallot; VSD, ventricular septal defect; NR, not reported.
aAge presented as mean (range).
bWeight expressed as mean (range).
cStudy authors confirmed accuracy of the extracted data and provided additional data where applicable.
dmBTS created using saphenous vein homograft.
eAge presented as range only.
f76 (78.4%) of 97 were children.
gAge presented as median (range).
hWeight expressed as median (range).
iAge presented as median (IQR).
jAge presented as median only.
kSingh 2014: 3 age groups reported. Ages as median (ranges)—(a) neonates (n = 8): 13 (3-24); (b) infants (n = 67): 290 (45-335); and (c) older children (n = 59): 730 (365-3650).
lWeight expressed as median only.
The majority of studies included patients between 0 and 1 months of age. The majority of studies included children weighing between 2.8 and 3.1 kg. Relevant cardiac conditions and other comorbidities present among the patient samples included hypoplastic left heart syndrome, cyanotic congenital heart disease with low pulmonary blood flow, pulmonary atresia or stenosis with or without ventricular septal defect, aortic atresia, tricuspid atresia with right ventricular hypoplasia, mitral atresia or stenosis, double outlet right ventricle, unbalanced atrioventricular septal defect, complex tetralogy of Fallot, complex transposition of the great arteries, heterotaxy syndrome, Ebstein anomaly, and other related complex single-ventricle anomalies (Table 1).
Thromboprophylaxis Strategies and Postoperative Outcomes
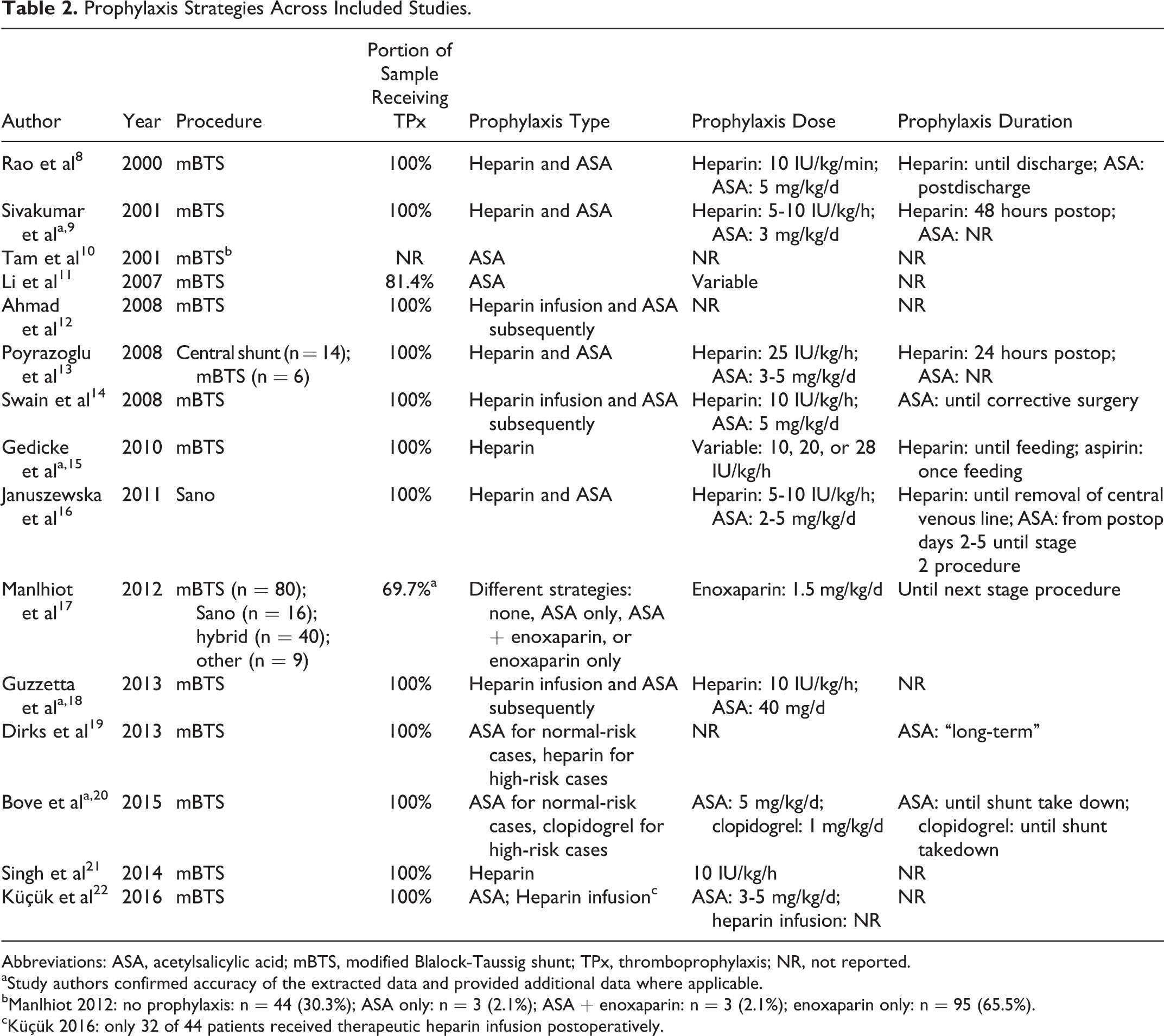
Among the 15 eligible studies, 2 studies reported postoperative acetylsalicylic acid (ASA) use alone, 10,11 8 studies reported a strategy involving initial heparin infusion and subsequent long-term ASA use, 8,9,12 –14,16,18,22 and 2 studies reported initial unfractionated heparin (UFH) infusion alone. 15,21 One study reported ASA use for normal-risk cases and heparin use for high-risk cases. 19 Another study reported ASA use for normal-risk cases and clopidogrel use for high-risk cases. 20 The remaining study included patients on a number of different thromboprophylactic strategies—30.3% of patients were maintained on no prophylaxis, 2.1% were maintained on ASA alone, 2.1% were maintained on ASA and enoxaparin, and 65.5% were maintained on enoxaparin alone (Table 2). 17
Prophylaxis Strategies Across Included Studies.
Abbreviations: ASA, acetylsalicylic acid; mBTS, modified Blalock-Taussig shunt; TPx, thromboprophylaxis; NR, not reported.
aStudy authors confirmed accuracy of the extracted data and provided additional data where applicable.
bManlhiot 2012: no prophylaxis: n = 44 (30.3%); ASA only: n = 3 (2.1%); ASA + enoxaparin: n = 3 (2.1%); enoxaparin only: n = 95 (65.5%).
cKüçük 2016: only 32 of 44 patients received therapeutic heparin infusion postoperatively.
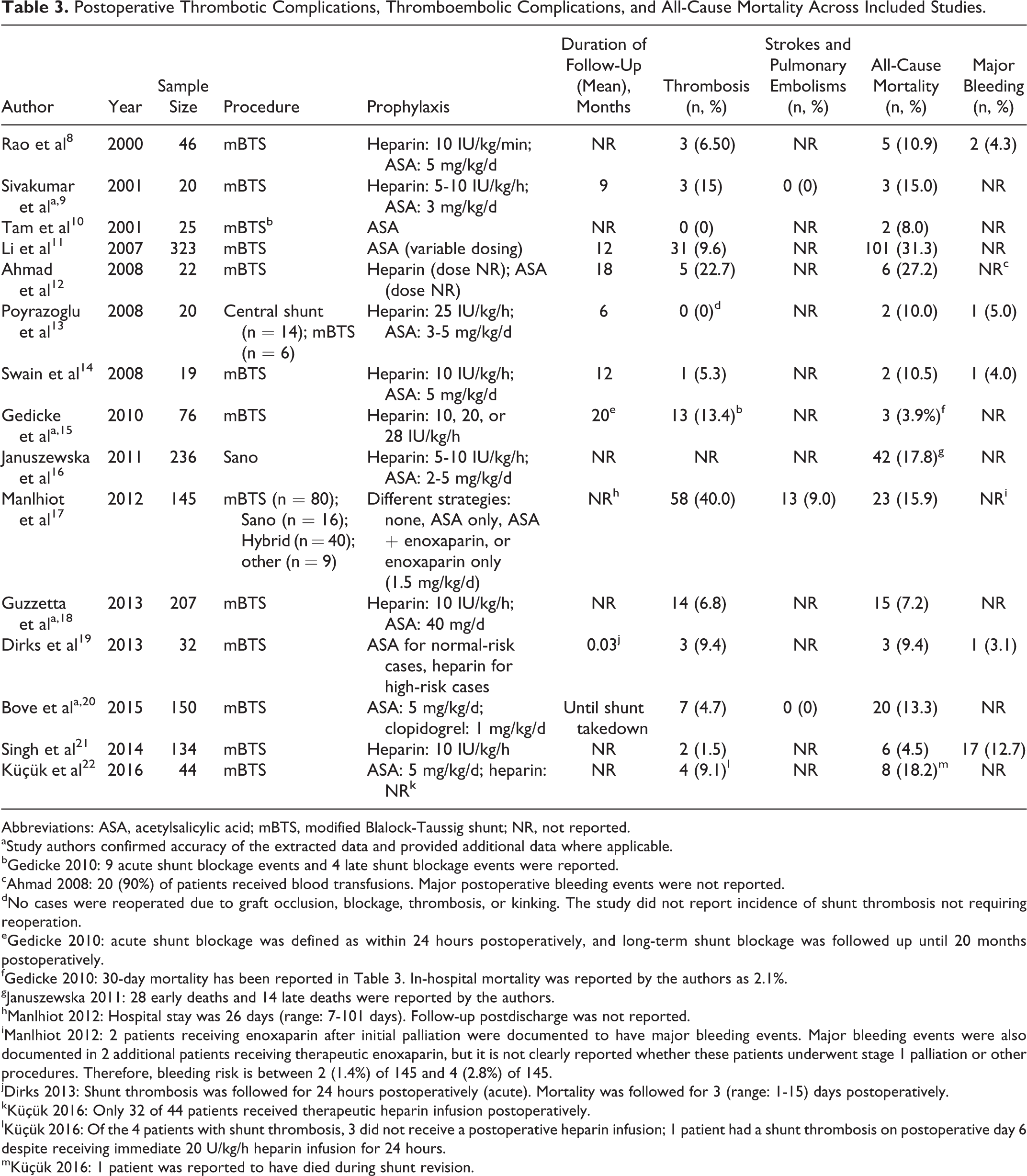
The 2 studies reporting postoperative ASA use reported widely variable rates of thrombotic events. 10,11 One study reported thrombotic events in 0% of children, 10 whereas the other reported events in 9.6%. 11 Similar variability was noted in the overall mortality, with 1 study reporting deaths in 8.0% of children 10 and the other reporting deaths in 31.3%. 11 Strokes pulmonary embolisms and major bleeding were not reported in either study (Table 3).
Postoperative Thrombotic Complications, Thromboembolic Complications, and All-Cause Mortality Across Included Studies.
Abbreviations: ASA, acetylsalicylic acid; mBTS, modified Blalock-Taussig shunt; NR, not reported.
aStudy authors confirmed accuracy of the extracted data and provided additional data where applicable.
bGedicke 2010: 9 acute shunt blockage events and 4 late shunt blockage events were reported.
cAhmad 2008: 20 (90%) of patients received blood transfusions. Major postoperative bleeding events were not reported.
dNo cases were reoperated due to graft occlusion, blockage, thrombosis, or kinking. The study did not report incidence of shunt thrombosis not requiring reoperation.
eGedicke 2010: acute shunt blockage was defined as within 24 hours postoperatively, and long-term shunt blockage was followed up until 20 months postoperatively.
fGedicke 2010: 30-day mortality has been reported in Table 3. In-hospital mortality was reported by the authors as 2.1%.
gJanuszewska 2011: 28 early deaths and 14 late deaths were reported by the authors.
hManlhiot 2012: Hospital stay was 26 days (range: 7-101 days). Follow-up postdischarge was not reported.
iManlhiot 2012: 2 patients receiving enoxaparin after initial palliation were documented to have major bleeding events. Major bleeding events were also documented in 2 additional patients receiving therapeutic enoxaparin, but it is not clearly reported whether these patients underwent stage 1 palliation or other procedures. Therefore, bleeding risk is between 2 (1.4%) of 145 and 4 (2.8%) of 145.
jDirks 2013: Shunt thrombosis was followed for 24 hours postoperatively (acute). Mortality was followed for 3 (range: 1-15) days postoperatively.
kKüçük 2016: Only 32 of 44 patients received therapeutic heparin infusion postoperatively.
lKüçük 2016: Of the 4 patients with shunt thrombosis, 3 did not receive a postoperative heparin infusion; 1 patient had a shunt thrombosis on postoperative day 6 despite receiving immediate 20 U/kg/h heparin infusion for 24 hours.
mKüçük 2016: 1 patient was reported to have died during shunt revision.
The 8 studies reporting prophylaxis with an initial heparin infusion and subsequent long-term ASA use reported rates of shunt thrombosis and other thrombotic events between 0% and 22.7%, demonstrating substantial variability. 8,9,12 –14,16,18,22 Guzzetta and colleagues’ 2013 study with 207 children with mBTS was the largest and most recent of these studies and reported thrombotic events in 6.8% of patients. 18 Strokes and pulmonary embolisms were not reported in any of the 8 studies. Overall rates of mortality ranged from 7.2% to 27.2% across the studies. 8,9,12 –14,16,18,22 Major bleeding rates ranged from 4.0% to 5.0% but were largely unreported across studies (Table 3). 8,9,12 –14,16,18,22
The 2 studies reporting postoperative heparin use alone also reported widely variable rates of thrombotic events. 15,21 One study reported thrombotic events in 1.5% of children, 21 whereas the other reported events in 13.4%. 15 Neither study reported stroke or pulmonary embolism events. Overall mortality ranged from 3.9% to 4.5% across the 2 studies. 15,21 Major bleeding was not reported by Gedicke and colleagues 15 and was reported in 12.7% of patients by Singh and colleagues, the highest rate reported across all identified studies (Table 3). 21
Dirks and colleagues applied a protocol where normal-risk cases received ASA, whereas high-risk cases received heparin. 19 The study reported 24-hour shunt thrombosis in 9.4% of children with mBTS and an overall mortality rate of 9.4%. One (3.1%) patient was reported to have a major bleeding event. 19 Administering ASA to normal-risk patients and clopidogrel to high-risk patients, Bove and colleagues reported thrombosis in 4.7% of 150 mBTS patients and an overall mortality rate of 13.3%; major bleeding events were not reported (Table 3). 20
Manlhiot and colleagues applied a protocol involving several thromboprophylaxis strategies—ASA alone (2%), ASA and enoxaparin (2%), enoxaparin alone (66%), and no thromboprophylaxis (30%). 17 The study reported a decreased risk of thrombotic complications postoperatively with enoxaparin compared to no thromboprophylaxis (hazard ratio [HR]: 0.5; P = .05). The study found that patients undergoing the Norwood procedure were more likely to be prescribed thromboprophylaxis than those undergoing the Sano procedure, a hybrid stage 1 procedure, or other cardiac procedures (90% vs 46%; P < .001) and found that earlier year of surgery (HR: 1.3 [1.1-1.5]; P = .002), hypoplastic left heart syndrome (HR: 2.0 [1.0-3.7]; P = .04), and a dominant left ventricle (versus right; HR: 0.5 [0.3-1.0]; P = .04) were associated with increased risk of thrombotic complications after stage 1 palliative surgery. Comparing surgical strategies, the study reported a higher risk of thrombotic complications with the Sano shunt versus the mBTS (HR: 3.8 [1.9-7.6]; P = .01) and versus the hybrid procedure (HR: 2.1 [1.0-4.3]; P = .06); the mBTS procedure was associated with a lower risk of thrombotic complications relative to the hybrid procedure (HR: 0.6 [0.3-1.1]; P = .08). Major bleeding events were not reported. 17
Discussion
Although it is recognized that risk of postoperative thrombosis and thromboembolic complications in Norwood, Sano, and mBTS patients may be substantial, estimates of these risks and current thromboprophylaxis strategies have not been previously synthesized. The findings of our systematic review shows variability across institutional thromboprophylaxis strategies in the management of the postoperative stage I palliative patient and substantial variability in the incidence of thrombosis and thromboembolic events reported in the literature.
The American College of Chest Physicians Evidence-Based Clinical Practice Guidelines for Antithrombotic Therapy and the Prevention of Thrombosis (9th ed.) recommends that neonates and children undergoing the mBTS procedure should receive intraoperative UFH therapy (grade 2C) and either aspirin or no antithrombotic therapy as compared to prolonged low-molecular-weight heparin (LMWH) or vitamin K antagonists postoperatively (grade 2C). 23 The guideline reports that smaller shunt size, smaller infant size, and increased perioperative hemoglobin level are risk factors for shunt thrombosis within the first 24 hours postoperatively. 12,15,23,24 Postdischarge shunt thrombosis-related mortality is reported to be substantial, and mortality in patients discharged on aspirin is reported to be almost identical to those discharged on no antithrombotic therapy. 12,23,25 The guideline also refers to findings of several studies pointing to no significant differences in early and late failure rates with or without heparin use, 23,26,27 while referring to others supporting a reduction in postoperative thrombotic events with aspirin use. 11,23,28 Finally, no supporting data for long-term anticoagulation with heparin, LMWH, or vitamin K antagonists are identified. 23
Given the small shunt size and the use of a similar shunt in the standard Norwood procedure, guideline recommendations support the same prophylactic strategy postoperatively for the Norwood procedure, 23,29,30 as for the mBTS procedure. The guideline acknowledges that modifications necessary with the Sano procedure are currently unknown. 23,31
The findings of our systematic review indicate that while long-term ASA use was reported in 87% of the studies, thromboprophylaxis protocols are generally inconsistent across institutions, with some using postoperative ASA alone, some others using postoperative heparin followed by ASA, some others using long-term heparin alone, and some others using alternate treatment strategies involving 1 or more of ASA, heparin, and clopidogrel based on risk stratification. The study of Manlhiot et al was the only study that involved a subset of the patient sample receiving no thromboprophylaxis 17 ; other studies, all reported some form of postoperative prophylaxis. Incidence of thrombosis ranged from 0% to 40.0%, and embolic events were largely unreported across the studies. Overall mortality ranged from 4.5% to 31.3%. It is important to note that mortality may be largely attributable to hemodynamic stability following the Norwood procedure, rather than thrombotic and thromboembolic events alone. Due to the substantial variability in estimates with each postoperative thromboprophylaxis strategy, no clear relationship was identified between prophylaxis strategies and reduction in thrombosis and thromboembolic events.
It is important to recognize the potential risk of bleeding complications with thromboprophylaxis use. Several studies have demonstrated a relatively low overall incidence of these complications in pediatric patients. 32 -34 Our findings suggest that while postoperative bleeding rates are a concern, 8,13,14,19,21 they are not likely to be attributed to thromboprophylaxis use alone. Keeping in mind these considerations and that the majority of the included studies did not report major bleeding rates, it may be fair to assume that the risk-benefit balance favors the use of thromboprophylaxis in these patients postoperatively.
Our findings must be interpreted with several limitations in mind. Although the review is a comprehensive effort to evaluate the risk of thrombosis and thromboembolic complications and the postoperative thromboprophylaxis strategies used in this patient population, the lack of a meta-analysis limits the findings. Furthermore, the high risk of bias of the individual studies included in the systematic review and the wide variability in their results and follow-up times limit the reliability and generalizability of the overall findings. The studies also include highly heterogeneous samples with a number of rare and complex comorbidities that are not accounted for in contextualizing the findings. Finally, reported rates of thrombotic and thromboembolic complications may be underestimated, given that the majority of the studies included likely reported clinically relevant thrombotic complications.
Conclusion
The incidence of thrombosis following initial palliation for pediatric patients with single-ventricle physiology varies from 0% to 40% in the literature, and thromboembolic complications are largely unreported. Alongside a number of other comorbidities often identified in this heterogeneous patient population, shunt thrombosis and shunt failure place these patients at a relatively high risk of morbid and fatal outcomes. Although it seems evident that some form of thromboprophylaxis is ideal following the stage I palliative procedure, it remains controversial whether prophylactic ASA reduces the risk of shunt occlusion and failure and improves survival. 23,35
Our findings highlight the lack of a gold standard in thromboprophylaxis strategies based on existing evidence despite existing guidelines and emphasize the need for more consistency in protocols across institutions. Randomized trials examining thromboprophylaxis strategies are warranted to identify this gold standard and encourage widespread adoption of a standard protocol for the postoperative management of these patients.
Footnotes
Appendix A
Appendix B
Data Extraction Form
|
|
|
|---|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
aIf more than 1 procedure of interest was reported in a study, data were extracted separately for each procedure of interest.
Acknowledgments
The authors would like to thank Thierry Bove, Robert Tulloh, Kothandam Sivakumar, and Nina A. Guzzetta for their assistance in confirming the accuracy of the extracted data and providing additional data not available in the published articles for their studies for the purposes of our review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.