
Abstract
The availability of direct oral anticoagulants has caused a paradigm shift in the management of thrombosis. Rivaroxaban and apixaban are 2 direct oral anticoagulants whose target specificity is activated factor X (FXa). However, it is still not fully understood if and how xabans impact platelet function. This observational study aimed to assess the in vitro platelet function in patients with atrial fibrillation receiving xabans. This was a single-center study quantifying platelet aggregation in 41 patients treated with apixaban or rivaroxaban by light transmission aggregometry. The thrombin receptor activating peptide (TRAP)-induced platelet aggregation was significantly lower 2 hours after taking rivaroxaban or apixaban compared to baseline value (56.15% [8.53%] vs 29.51% [12.9%]; P = .000). Moreover, concomitant use of angiotensin-converting enzyme blockers, proton pump inhibitors, and statins reduces the efficiency of xabans. The TRAP-induced platelet aggregation was reduced in patients with cardiovascular disease 2 hours after receiving xabans.
Keywords
Introduction
Atrial fibrillation (AF) increases the risk of ischemic stroke by 5-fold and is associated with 15% of strokes in all age-groups and 30% in persons older than 80 years. 1 Patients with AF-related stroke have higher recurrent risk, morbidity, and mortality when compared to patients with other stroke types. 2 Current guidelines emphasize stroke prevention in patients with AF, in the presence of stroke risk factors. 3 Effective stroke prevention essentially refers to oral anticoagulation. The use of vitamin K antagonists (VKAs) reduces stroke/systemic embolism by 64% and all-cause mortality by 26%, compared to control or placebo. 4 However, the use of VKAs has many limitations, including the need to ensure proper anticoagulation control by regular monitoring, given VKAs’ many interactions with drugs and diet. 5 As a result, 30% to 50% of patients with AF were undertreated. 6 To overcome the limitations of VKAs, the direct oral anticoagulants (DOACs) have been introduced and offer relative efficacy, safety, and convenience compared to VKA therapy. 7 The available DOACs, dabigatran, rivaroxaban, apixaban, and edoxaban, were approved by the US Food and Drug Administration in October 2010, November 2011, December 2013, and January 2015, respectively.
Rivaroxaban and apixaban are 2 DOACs whose target specificity is activated factor X (FXa), which is why they are referred to here as xabans. 8 –10 The mechanism of action of rivaroxaban and apixaban is the inhibition of prothrombinase complex-bound and clot-associated FXa, resulting in a reduction of the thrombin burst during the propagation phase of the coagulation cascade. Thrombin is an essential enzyme in the coagulation system and it is also the strongest endogenous platelet agonist. 11 Effect of thrombin on platelets is mainly mediated by 2 G-protein-coupled receptors, protease-activated receptor 1 (PAR1) and PAR4. 12 Mechanistically, thrombin proteolytically cleaves a part of the extracellular loop of these receptors. It mediates platelet aggregation, calcium mobilization, and platelet shape change, ultimately resulting in activation of the platelet glycoprotein (GP)IIb/IIIa receptor. 13 –15 xabans do not directly affect platelet aggregation induced by collagen or adenosine diphosphate, but by inhibiting FXa, they indirectly decrease clot formation induced by thrombin. 16,17 Therefore, the aim of the present study was to assess the effects of xabans on in vitro platelet aggregation in patients with nonvalvular AF.
Materials and Methods
The local ethical committee of the Jessenius Faculty of Medicine in Martin approved this study (EK 1702/2015). All study participants agreed to participate in the project and signed a written informed consent in accordance with the Declaration of Helsinki.
Rivaroxaban was administered at fixed 15 mg once-daily dose (at 7:00
Light transmission aggregometry (LTA) was performed using the international protocol for the laboratory investigation of platelet function. 18 We wanted to emphasize that testing was performed on patients without any antiplatelet or nonsteroidal anti-inflammatory drugs (10-14 days before measurement) and with normal platelet count (≥150 × 109/L). The antecubital venous blood was collected into tubes containing 3.2% buffered sodium citrate (anticoagulant–blood ratio 1:9) to assess platelet aggregation. Platelet aggregability was tested with platelet-rich plasma using platelet aggregometry (PACKS-4 aggregometer; Helena Laboratories, Beaumont, USA). Blood samples were stimulated with thrombin receptor activating peptide (TRAP; 10 μmoL).
Data are presented as numbers with frequencies for categorical variables and means with standard deviations (SD) for continuous variables. For comparison of the different groups, the closed test principle was used. An overall comparison was performed, followed by pairwise comparison if the results were significant. All tests were 2-tailed, and P values <.05 were considered statistically significant. Data were analyzed with SPSS 21.0.0.0 (SPSS Inc, Chicago, Illinois).
Results
Table 1 presents full clinical baseline characteristics of the patients. Forty-one patients with nonvalvular AF were enrolled. The mean age was 74.85 (9.32) years (range: 55-94 years), 22 patients were women, and the mean CHA2DS2VASc score was 3.83 (1.24). All patients began treatment with apixaban or rivaroxaban as initial anticoagulant treatment. The minimum term use of xabans was 18 days. Apixaban doses were 5 mg (65%) or 2.5 mg (35%) twice daily. The mean apixaban concentration was 66.48 (34.22) ng/mL in sample 1 and 151.56 (41.54) ng/mL in sample 2. Concentrations of rivaroxaban in serum (sample 1) were 45.92 (36.86) ng/mL and 195.53 (96.18) ng/mL 2 hours after administration (sample 2). The TRAP-induced platelet aggregation did not correlate significantly with apixaban or rivaroxaban levels (see Table 2). Through subgroup analysis, we found that apixaban significantly reduced the TRAP-induced platelet aggregation more than rivaroxaban. Subgroup analysis showed a significant reduction in TRAP-induced platelet aggregation after administration of angiotensin-converting enzyme blockers, proton pump inhibitors, and statins (see Table 3).
Clinical Baseline Characteristics of the Patients.
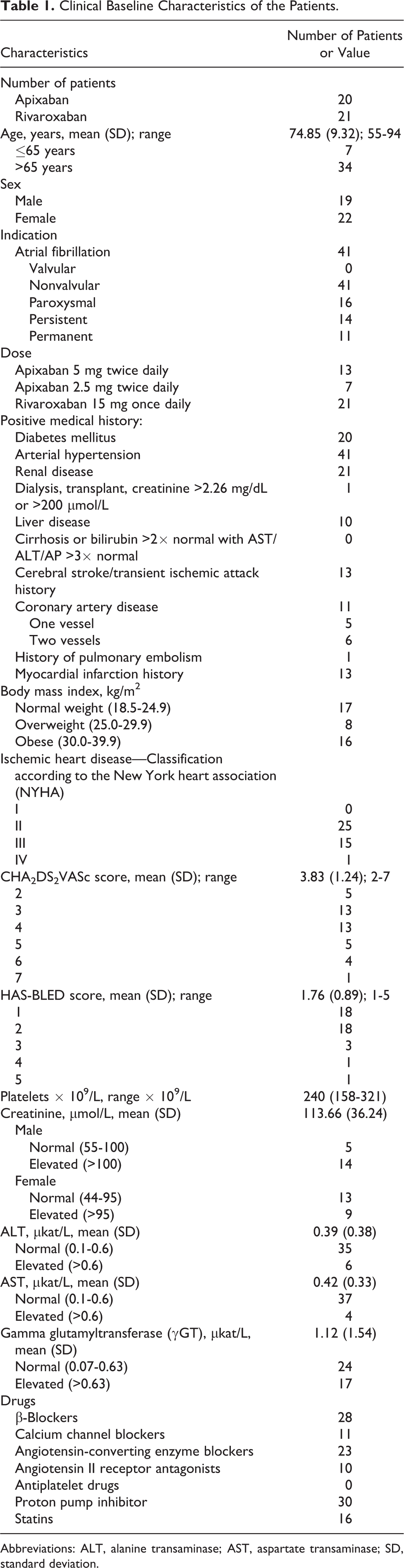
Abbreviations: ALT, alanine transaminase; AST, aspartate transaminase; SD, standard deviation.
Correlation Between TRAP-Induced Platelet Aggregation and Antifactor Xa (Rivaroxaban) and Antifactor Xa (Apixaban) in Samples 1 and 2.a
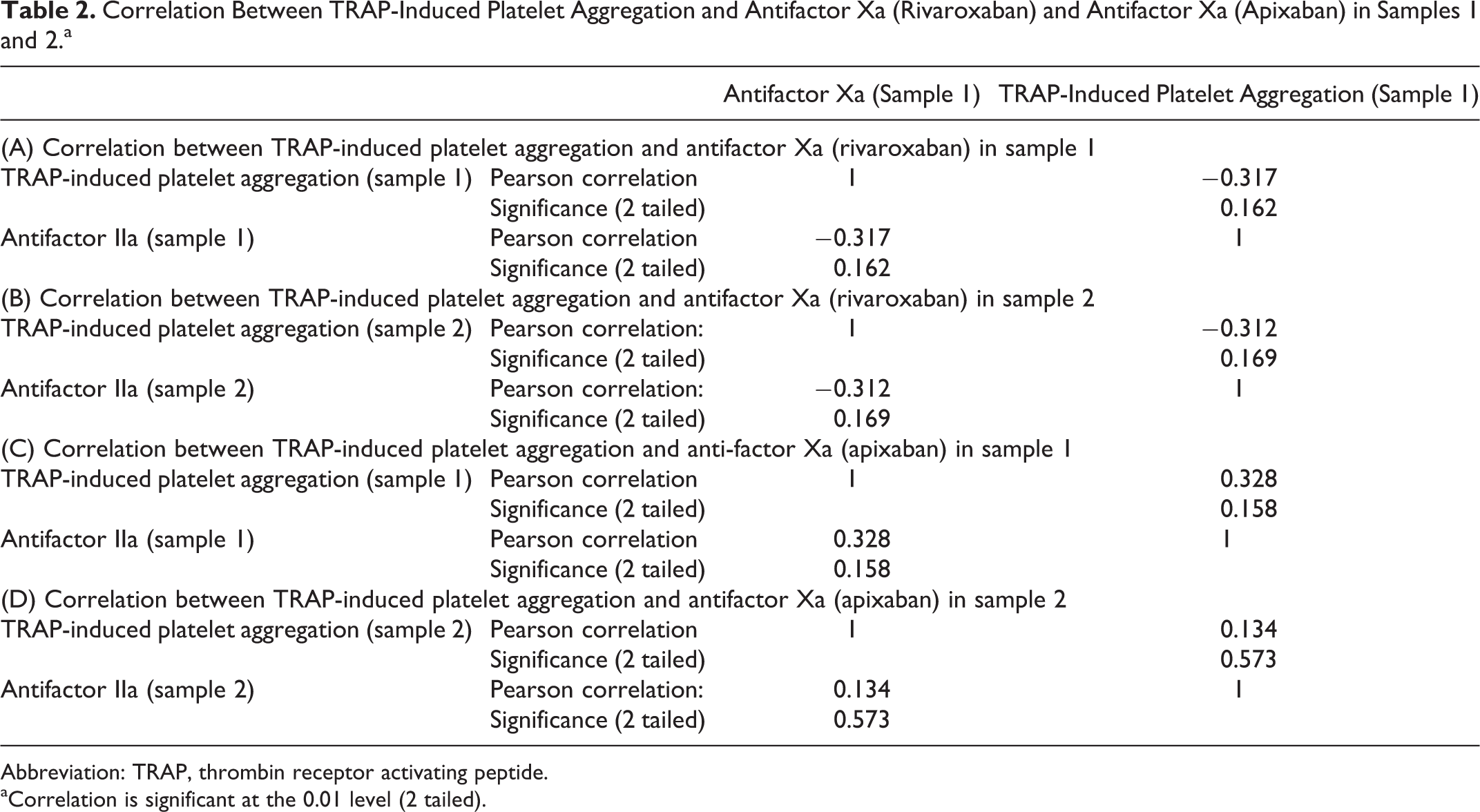
Abbreviation: TRAP, thrombin receptor activating peptide.
aCorrelation is significant at the 0.01 level (2 tailed).
Subgroup Analysis.
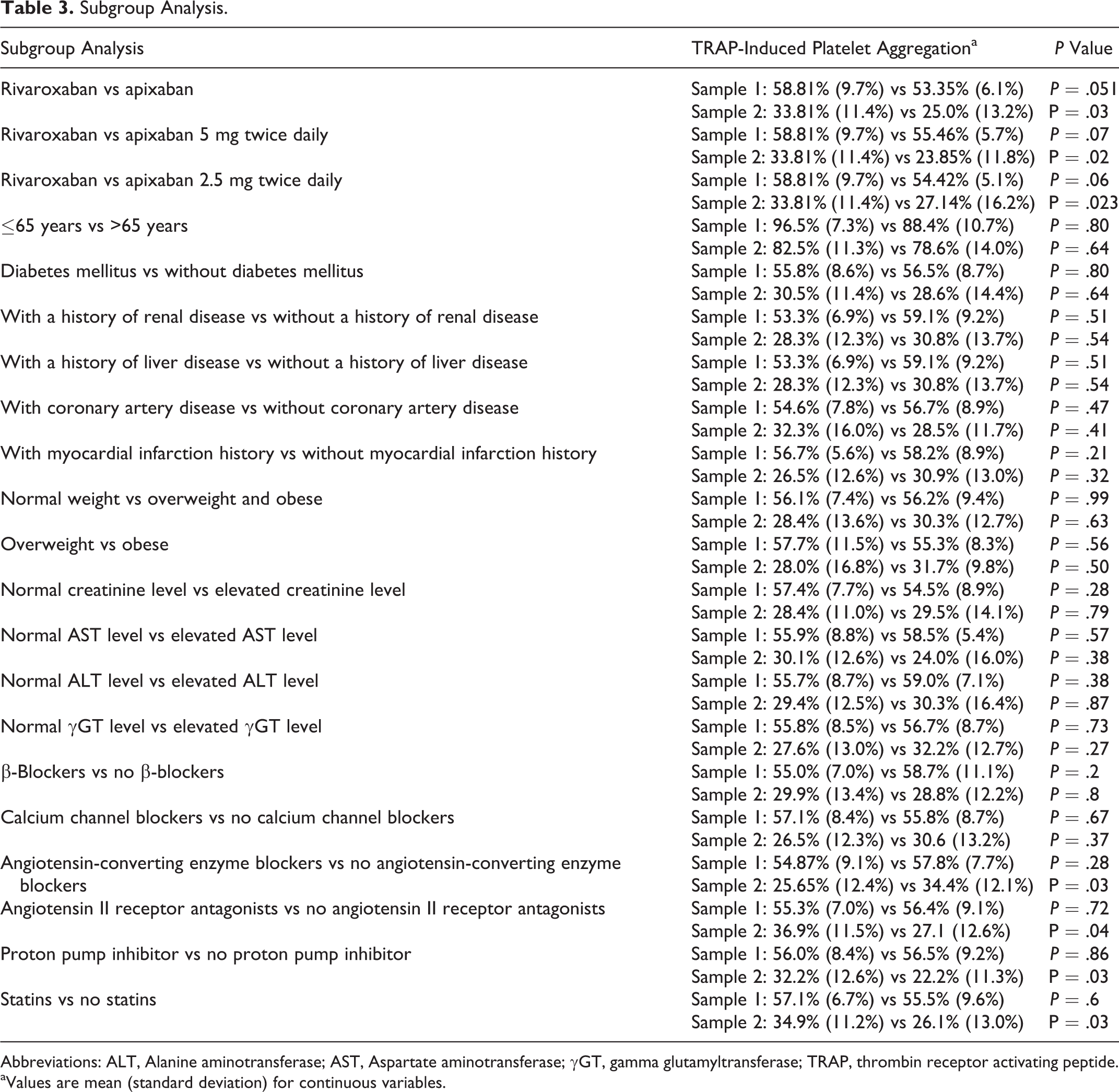
Abbreviations: ALT, Alanine aminotransferase; AST, Aspartate aminotransferase; γGT, gamma glutamyltransferase; TRAP, thrombin receptor activating peptide.
aValues are mean (standard deviation) for continuous variables.
As shown in Figure 1, the TRAP-induced platelet aggregation by LTA was significantly reduced in sample 2 compared to sample 1 (56.15% [8.53%] vs 29.51% [12.9%]; P = .000). Aggregation results for each patient are shown in Figure 2.
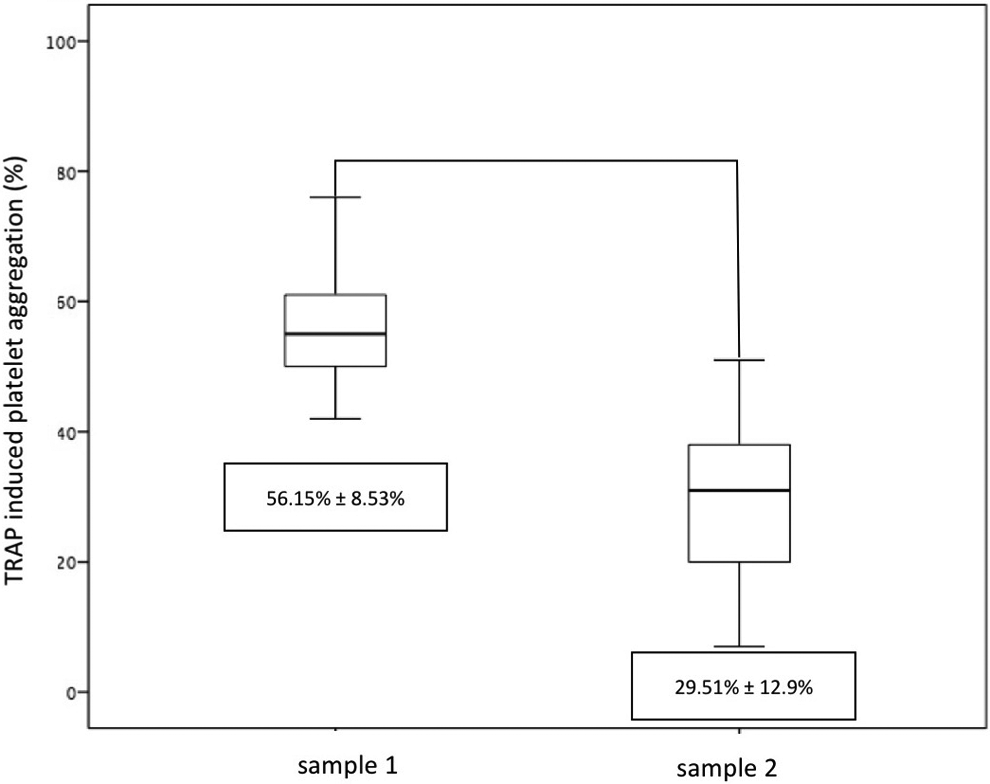
Results of thrombin receptor activating peptide (TRAP)-induced platelet aggregation.
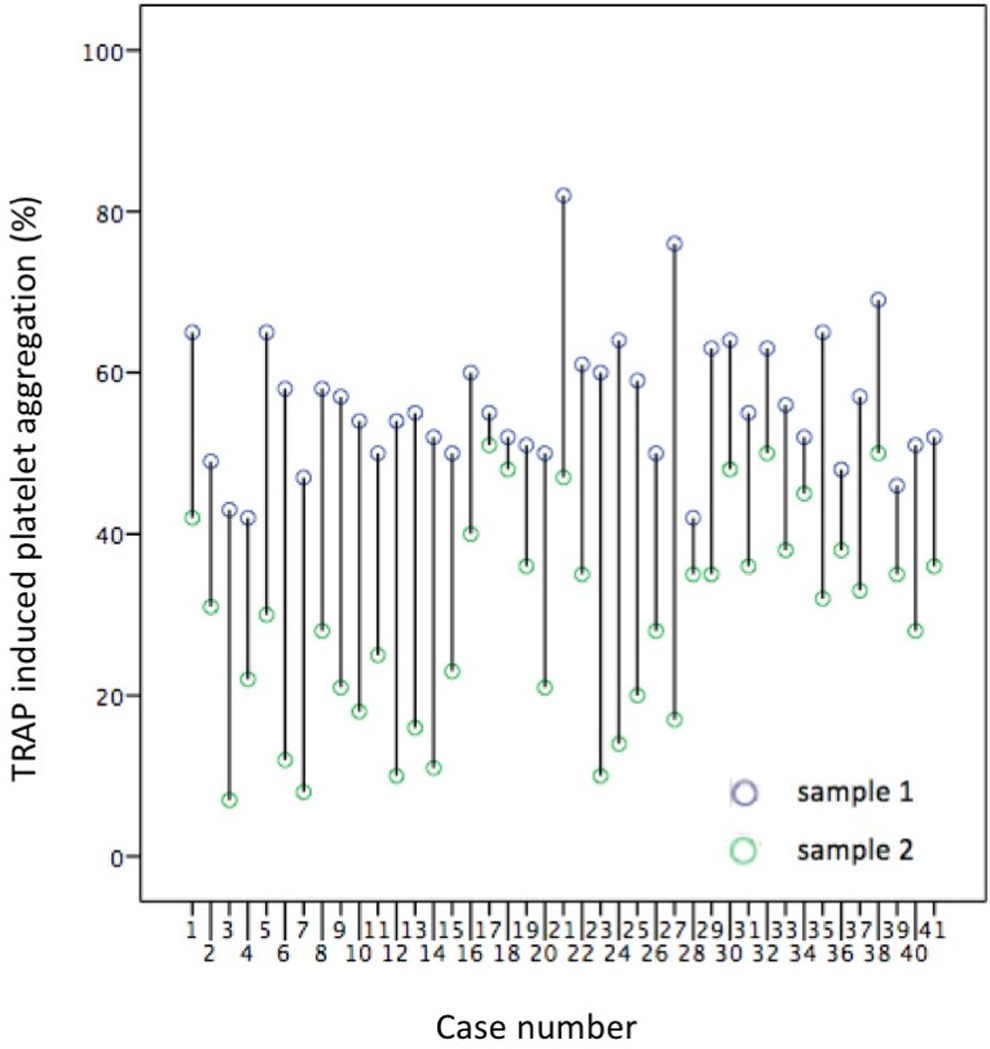
Aggregation results for each patient.
Discussion
To our knowledge, this is the first prospective comprehensive study to test whether the xabans affect TRAP-induced platelet aggregation. This study aimed to analyze the influence of the DOACs apixaban and rivaroxaban on platelet function. Thrombin is a key protein in the cascade of fibrin clot formation and also a potent inducer of platelet aggregation. 18 –21 The FXa inhibitors potently and selectively inhibit thrombin formation. 22 Thrombin is capable of activating platelets, which is mediated primarily by the hydrolysis of a G-protein-coupled receptor on the platelet membrane, referred to as PAR-1 and a second receptor (PAR-4) that expresses a lower sensitivity to thrombin. 23 Probably, low concentration of thrombin (blocked FXa cannot activate thrombin) is unable to cleave and activate PAR-1. However, the effects of xabans on platelet aggregation are still not fully understood.
This single-center study quantifies platelet aggregation in 41 patients treated with xabans by LTA. The TRAP-induced platelet aggregation was significantly lower 2 hours after administration of xabans compared to baseline value (56.15% [8.53%] vs 29.51% [12.9%]). Thus, xabans reduce platelet aggregation by 53% at the time of maximum plasma concentration. However, patients with higher doses of apixaban showed higher TRAP-induced platelet aggregation (Table 3) with dose-dependent characteristics. Nevertheless, no direct association between the apixaban plasma level and TRAP-induced aggregation was found in this study (Table 2). This indicates that the enhanced TRAP-induced platelet aggregation is not necessarily an immediate effect of apixaban but may be explained by the duration of chronic apixaban therapy. In addition, TRAP-induced aggregation should bypass any indirect effect of xabans on thrombin generation. Thus, our data indicate that the TRAP-induced platelet aggregation is enhanced by a chronic, indirect inhibition of thrombin. This might be due to changes in the expression of PAR-1 receptor on the platelets. The same results were observed in study by Olivier et al and Renda et al. 24,25
No significant differences were found in the patients with a history of renal or liver disease, diabetes, coronary artery disease, myocardial infarction, and so on (see Table 3). It seems that the concomitant use of angiotensin-converting enzyme blockers, proton pump inhibitors, and statins reduces the efficiency of xabans. So far, these interactions have not been seen in any other study.
Our findings could have some important clinical implications because platelet aggregation and coagulation cascade are affected at the same time. The situation could be more worse during concomitant administration of antiplatelet or anticoagulant agents. Moreover, concomitant use of angiotensin-converting enzyme blockers, proton pump inhibitors, and statins reduces the efficiency of xabans. But on the other side, it reduces the impact of xabans on platelet aggregation.
There were several limitations in our study. The small number of participants may have limited the ability to detect small drug effects on platelet function. Second, this study was not powered for clinical outcome. Therefore, it cannot be concluded that, for example, combination of antiplatelet therapy and xabans is not safe. Third, platelet aggregability is greatly affected by preanalytical issues and therefore interpretation of platelet hyperaggregability is potentially accordingly adversely influenced.
Conclusion
In conclusion, our study showed significant effect of xabans on platelet aggregability. Moreover, concomitant use of angiotensin-converting enzyme blockers, proton pump inhibitors, and statins reduces the efficiency of xabans. Future, larger investigations are required to confirm our hypothesis-generating work and correlate them with thrombotic and bleeding clinical events.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by grants VEGA 1/0187/17.