
Abstract
Recently, decreased levels of apolipoprotein M (ApoM) were shown to be associated with higher risk of recurrent venous thromboembolism (VTE) in male patients. However, the role of ApoM in primary VTE is unknown. We aimed in our study to analyze the plasma levels of ApoM in patients with VTE in order to evaluate the diagnostic importance of ApoM in primary VTE. A total of 357 patients with suspected first episode of VTE were recruited prospectively in the SCORE study. Plasma samples from 307 patients were available for quantifying the plasma levels of ApoM in patients with VTE using sandwich enzyme-linked immunosorbent assay method. Among the whole population, plasma levels (mean [standard deviation]) of ApoM were not significantly different between patients with VTE (0.72 [0.20]) and non-VTE patients (0.72 [0.16]), P = .99. Similarly, in regression analyses, no significant association of ApoM plasma levels with the risk of VTE was found on univariate (odds ratio [OR] =1.0, 95% confidence interval [CI] 0.21-4.84, P = .99) and multivariate analysis (OR = 1.25, 95% CI = 0.19-8.34, P = .819) after adjusting for age, body mass index, and smoking. Moreover, results did not differ significantly after stratification of data according to sex (P > .05). In this study, our results do not suggest a diagnostic role for ApoM plasma levels in patients with primary VTE. Moreover, the current study suggests that role of ApoM as a risk factor may differ for primary VTE and recurrent VTE in male patients.
Introduction
Deep vein thrombosis (DVT) is blood clot formation in the deep veins of the legs. Blood clot can detach and move toward to the lungs causing blockage of pulmonary arteries called pulmonary embolism (PE). Collectively, DVT and PE are called venous thromboembolism (VTE), which is the third most common type of cardiovascular disease after coronary artery disease and stroke.
1,2
Annual incidence rate of VTE is 1 to 2 cases per 1000 persons-years. Usually, DVT arises in lower extremities of the body including tibial, femoral, and iliac veins but can also occur at unusual locations including cerebral sinuses and visceral veins. Tibial vein thrombosis (distal DVT) is associated with low risk of PE, while femoral and iliac vein thromboses (proximal DVT) often lead to PE and postthrombotic syndrome.
3
Previous studies reported that about 79% of patients diagnosed with PE have evidence of DVT in their legs
3,4
; if DVT is not properly diagnosed in these patients, it is likely that the whole thrombus will detach and embolize to pulmonary arteries, which can lead to PE with a mortality of 10% to 25%.
5,6
Most common VTE symptoms include tenderness or pain and swelling in the leg, but these signs and symptoms are nonspecific, and the majority of patients presenting these symptoms do not have VTE.
7,8
Therefore, it is important to develop new diagnostic strategies that could precisely diagnose VTE patients in the clinics. Due to the nonspecific signs and symptoms of VTE, one way of proper diagnosis would be performing an objective imaging in all patients with suspected VTE. However, diagnosis by objective imaging would be inefficient, expensive, and can cause number of complications.
9
–11
Among the currently used strategies for VTE diagnosis, a well-known marker is the
Apolipoprotein M (ApoM) gene is located on chromosome 6, adjacent to the major histocompatibility complex class III region. Genes in this region are related to the immune and inflammatory responses. 15 It was first identified in 1999 by Xu et al. The ApoM protein has molecular weight of ∼26 kD and accounts for ∼5% of high-density lipoprotein (HDL) and less than 2% of low-density lipoprotein (LDL). 15,16 Expression array analysis revealed that expression of ApoM is tissue specific in human, mainly expressed in liver and kidneys. 17 Although the ApoM is mainly associated with HDL, its biological functions and mechanisms in HDL and disease development are not elucidated yet. Apolipoprotein M is a newly identified protein with potential antioxidant and antiatherogenic properties through reverse cholesterol transport (RCT). 16 Moreover, ApoM carries a biological lipid called “sphingosine-1-phosphate” (S1P), which is responsible for several physiological and pathological pathways including lymphocyte trafficking, cell growth, and vascular stability. 18 Previous studies showed that S1P performs these functions through different ways, for example, by activation of the nuclear factor κB pathway resulting in improved endothelial adhesion, enhancing the production of nitrogen oxide via endothelial nitric oxide synthase, and vasoprotective effects on the endothelium by HDL-ApoM-S1P complex. 19,20
Preclinical animal studies reported that in mice lacking LDL receptor, overexpression of ApoM abates the plaque area within the aortic root. They also found that levels of cholesterol are not largely affected by the ApoM modulation in the mice models in question, showing that ApoM may be involved in abatement and prevention of atherosclerosis development in these models by its effect on pre-β HDL formation. 19 –21 Pre-β HDL has a critical role in RCT and its use as a risk factor for several cardiovascular diseases. 22 Apolipoprotein M has also been thoroughly studied for its role in metabolic and arterial diseases. 19 Increased plasma levels of ApoM were significantly associated with lower risk of abdominal aortic aneurysms and critical limb ischemia. 23,24 Studies have shown that genetic aberrations in ApoM that affect the expression levels are associated with higher risk of coronary artery disease and diabetes mellitus. 25 –27 Recently, genetic aberrations in ApoM have been shown to be associated with high risk of VTE recurrence in males. 28 Similarly, in a study by Memon et al, lower plasma levels of ApoM were associated with an increased risk of VTE recurrence in male patients. They also showed that ApoM plasma levels are better predictors of VTE recurrence than previously well-known predictive marker, that is, thrombophilia. 29 However, the role of ApoM plasma levels in primary VTE is unknown yet. We aimed our study to analyze the plasma levels of ApoM in patients with VTE to evaluate the diagnostic importance of ApoM in primary VTE. To our knowledge, this is the first study in which ApoM levels have been analyzed in patients with primary VTE, and role of ApoM in diagnosis of VTE has been elucidated.
Material and Methods
Study Participants
SCORE study was performed from December 2003 to December 2005 including adult patients with suspected first episode of VTE at 7 different centers in southern Sweden as reported previously. 12 Briefly, a total of 491 outpatients were evaluated consecutively for the recruitment period of 2 years. These patients were enrolled directly at their arrival to emergency department, and the enrollment was possible 24 hours a day for 7 days a week. Inclusion criteria were adult patients with suspected VTE, referred from primary care physicians, self-referral, or in some cases from other clinics. Of the 491 patients, 107 (22%) patients were excluded due to one of the following reasons: duration of symptoms more than 10 days (n = 37), previous VTE (n = 54), pregnancy (n = 1), getting anticoagulation therapy (n = 1), suspicious symptoms for PE (n = 3), unwillingness or inability to provide informed consent (n = 9), comorbid conditions (n = 1), and contraindication to contrast media (n = 1). Furthermore, 27 cases were excluded because of inadequate or missing reports forms, blood samples, or written informed consent. Remaining 357 patients were considered eligible to include in this study. Among these patients, 9% were immobilized in bed or had a major reduction in mobility.
All the enrolled patients were evaluated for Wells score
30
by the emergency physician available on duty at that time. Pretest probability according to Wells score was determined for patients with VTE. All the patients were categorized according to pretest probability as low, medium, and high. Low probability patients underwent
Only confirmed VTE diagnoses (by contrast venography and/or CUS of the leg and computed tomography and/or ventilation/perfusion scintigraphy of the lungs) were treated with anticoagulant according to anticoagulant regime, that is, initial treatment with low-molecular-weight heparin or unfractionated heparin and then with warfarin as an oral anticoagulant. According to hospital treatment protocol, therapy was recommended for 3 to 6 months for first-time VTE, with consideration of extended treatment in case of recurrent VTE. Ongoing anticoagulant treatment was an exclusion criterion for this study.
For
Apolipoprotein M Plasma Level Analysis
Aliquoted plasma stored at −70°C was obtained for ApoM plasma level analysis. Sandwich enzyme-linked immunosorbent assay method was used to measure ApoM levels as described previously. 32 In summary, 96-well Costar plates (Corning, Inc, Lowell, Massachusetts) were coated and blocked with catching monoclonal ApoM antibody (100 μL of monoclonal M58) and quenching buffer (200 μL), respectively. Plasma samples and standards were diluted and incubated overnight at room temperature. After washing steps, bound ApoM was detected by using 100 µL of biotinylated secondary M42, diluted to a final concentration of 0.5 μg/mL in combination with streptavidin–avidin horseradish peroxidase and 1,2-phenylenediamine dihydrochloride (Dako, Glostrup, Denmark). The reaction was terminated and 490-nm absorbance was measured and compared with a plasma standard curve having known amounts of ApoM.
Statistical Analysis
Statistical software SPSS (IBM, Armonk, New York) was used for analysis. Characteristics of the studied population were presented as mean (standard deviation; SD) for the continuous variables, while for the categorical variable, numbers and percentages of the patients were shown. Due to skewed distribution,
Results
In total, 357 patients were included in this study comprising 83 (27%) confirmed patients with VTE. Baseline characteristics of the patients with VTE are presented in Table 1. The APC-PCI complex levels were significantly higher in patients with VTE when compared to non-VTE patients (P < .0001). Similarly, Wells score and
Baseline Characteristics of Studied Population.a
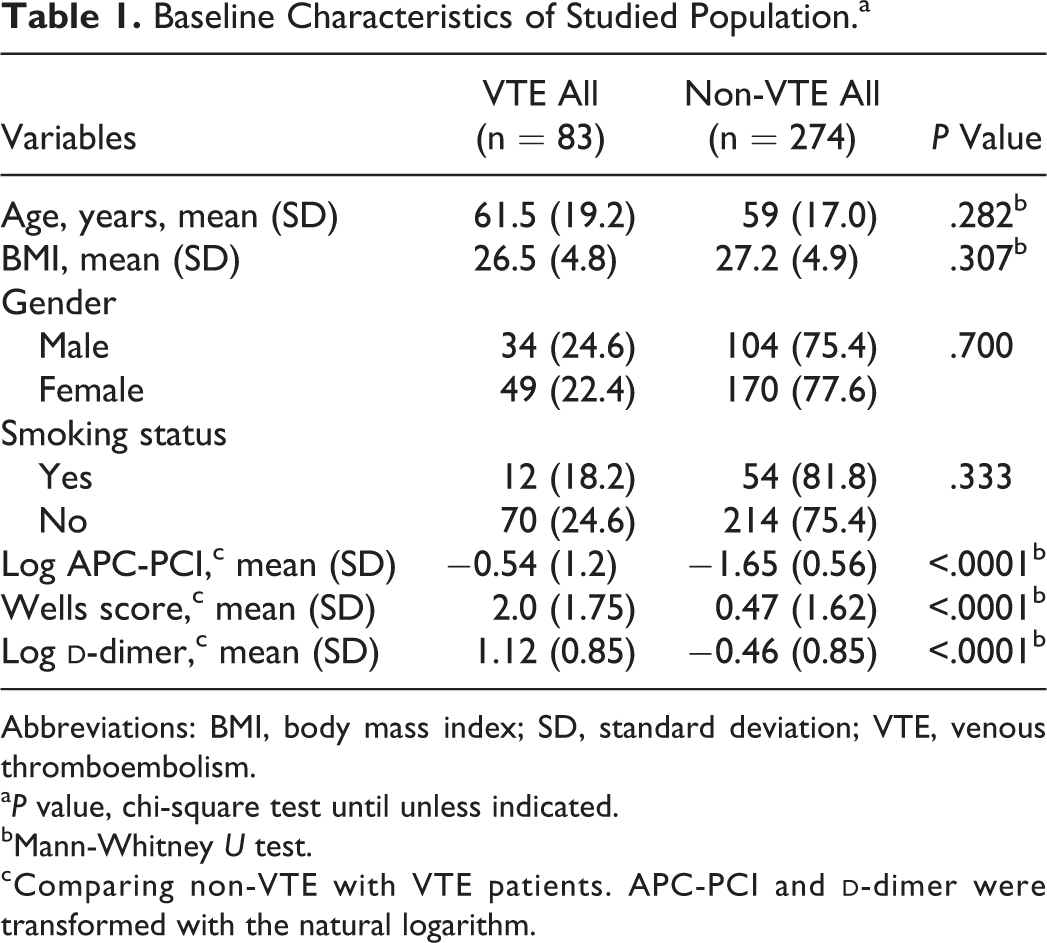
Abbreviations: BMI, body mass index; SD, standard deviation; VTE, venous thromboembolism.
a P value, chi-square test until unless indicated.
bMann-Whitney U test.
cComparing non-VTE with VTE patients. APC-PCI and
Apolipoprotein M and VTE
Of 357 patients with VTE, 50 patients had inadequate amount of plasma or poor plasma quality (eg, hemolysis) and therefore were excluded in risk assessment analysis. In the whole studied population, levels of ApoM were not significantly different between patients with VTE (0.72 [0.20] μmol/L) and non-VTE patients (0.72 [0.16] μmol/L; Figure. 1A). Similarly, no difference in levels of ApoM was found between patients with VTE and non-VTE patients after stratification of data according to sex. Figure 1B shows distribution of ApoM levels between patients with VTE (0.70 [0.22] μmol/L) and non-VTE patients (0.68 [0.16] μmol/L) in males. Likewise, ApoM levels were not significantly different among patients with VTE (0.73 [0.17] μmol/L) and non-VTE patients (0.74 [0.16] μmol/L) in female patients.
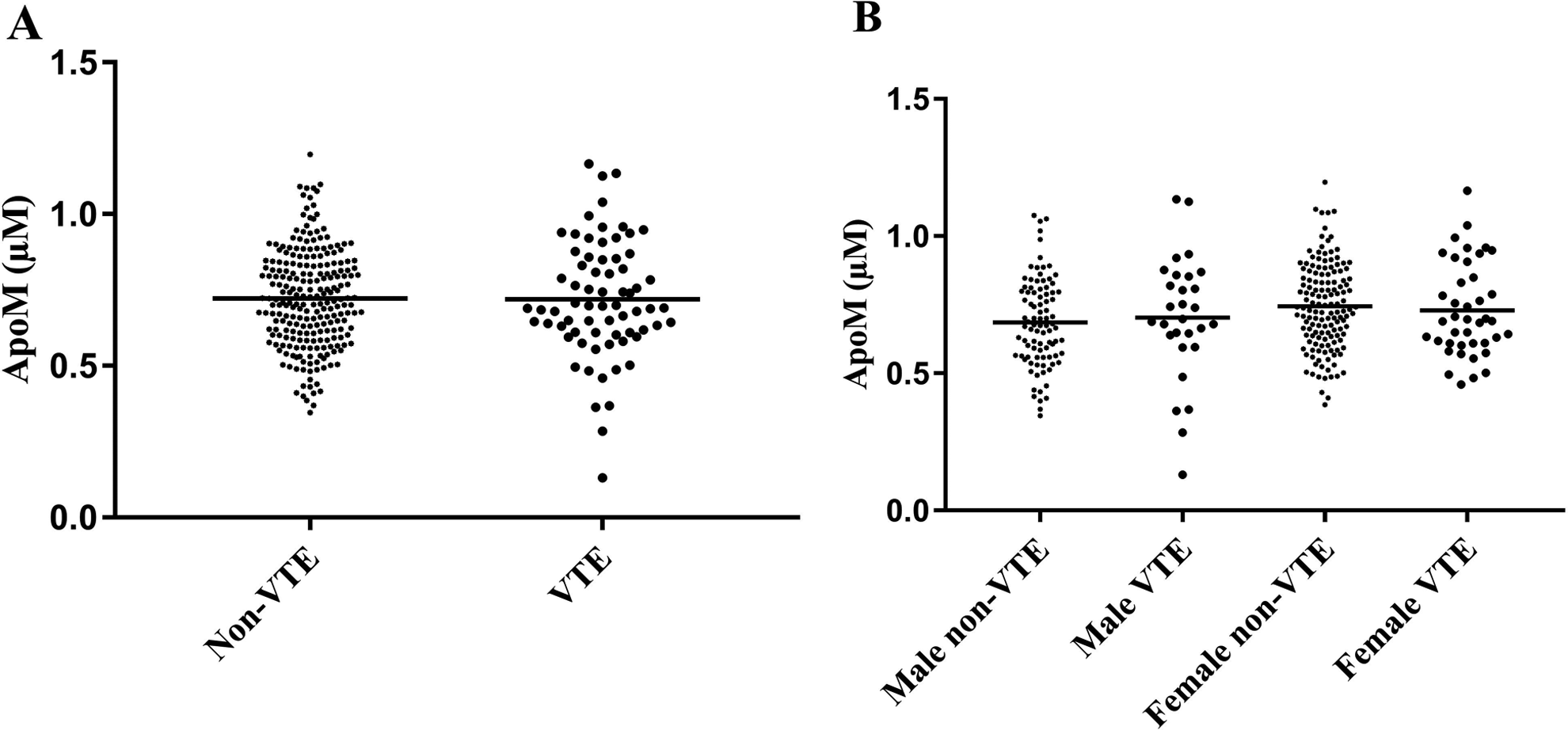
Apolipoprotein M (ApoM) plasma levels in the overall studied population (A) and in male and female patients (B) in primary venous thromboembolism (VTE) and non-VTE patients. Levels of ApoM were not significantly different between VTE and non-VTE in the overall population (P = .99). Similarly, there was no significant difference in distribution of ApoM levels in patients with VTE and non-VTE patients after stratification of patients according to sex (P > .05). Solid line represents mean.
Furthermore, we analyzed the ApoM plasma levels according to the location of VTE. In patients with proximal DVT, ApoM plasma levels were 0.69 (2.0), while 0.77 (16) were found in patients with distal DVT. The plasma levels of ApoM were not significantly different in both groups (P > .05, results not shown).
To evaluate the diagnostic value of ApoM for VTE, we performed ROC curve analysis in the whole cohort. The AUC for ApoM plasma levels was 0.503, with a P value and 95% confidence interval (95% CI) as .93 and 0.42 to 0.58, respectively. The AUC for ApoM was not significantly different from a reference of AUC (0.50). The ROC curve results are shown in Figure 2.
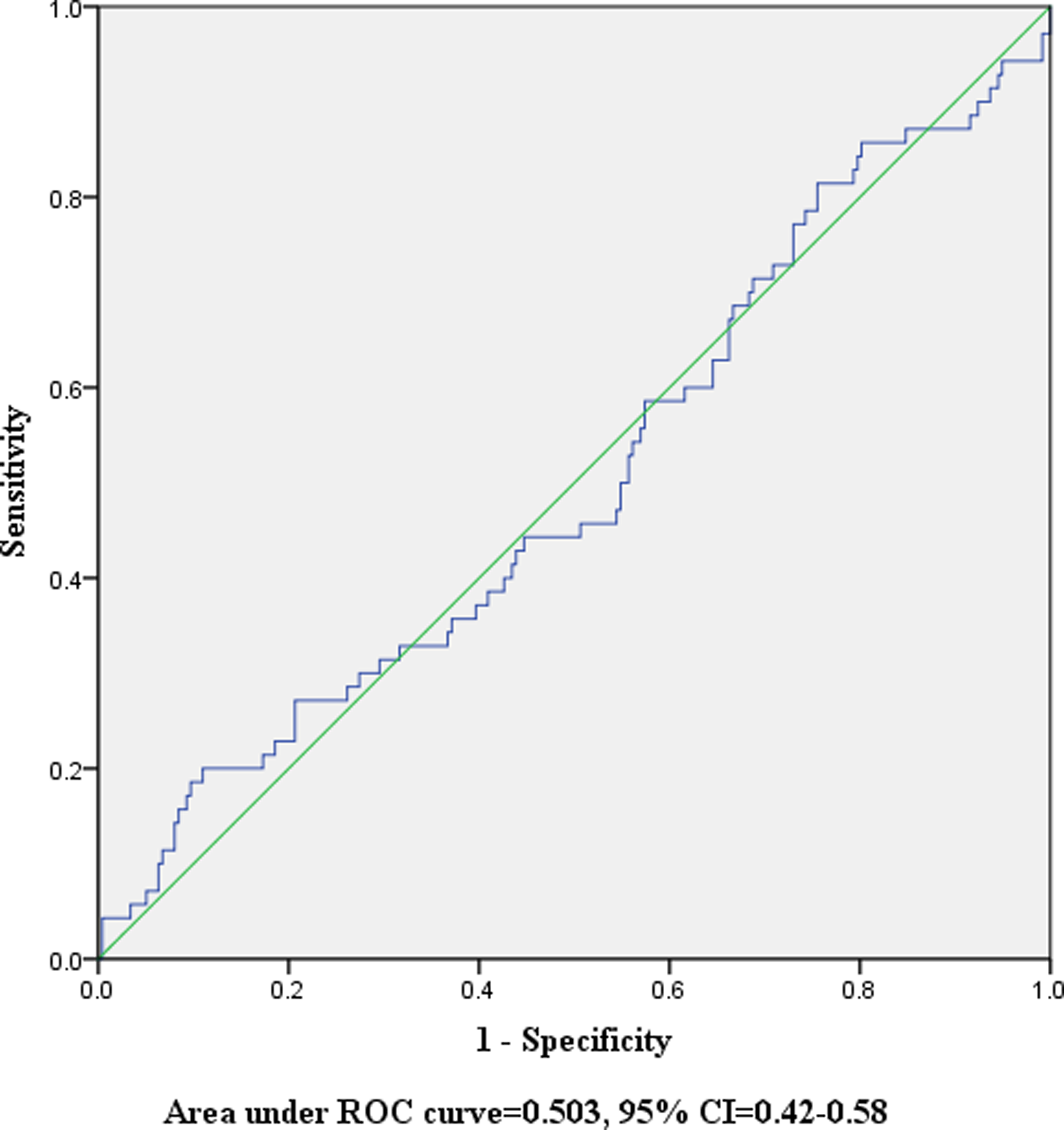
Receiver operating characteristic (ROC) curves showing area under the curve (AUC) for apolipoprotein M (ApoM) plasma levels in patients with primary venous thromboembolism (VTE).
Apolipoprotein M and VTE Risk
Apolipoprotein M was analyzed for its role in diagnosis of primary VTE. To calculate OR and 95% CI, binary logistic regression analyses were performed in 307 patients including 70 (23%) patients with confirmed VTE. No significant association between ApoM plasma levels and risk of VTE was found in all patients as whole on univariate analysis (OR = 1.0, 95% CI = 0.21-4.84) and on multivariate regression analysis (OR = 1.25, 95% CI = 0.19-8.34) after adjusting for age, BMI, and smoking status. The
Association of ApoM Plasma Levels With the Risk of Primary VTE in All Patients and Different Gender Groups.

Abbreviations: ApoM, apolipoprotein M; BMI, body mass index; CI, confidence interval; OR, odds ratio; VTE, venous thromboembolism.
aAdjusted for BMI, age, and smoking.
We also analyzed the correlation between ApoM plasma levels,
Previous study indicated that role of ApoM plasma levels was sex-specific, and decreased levels of ApoM were significantly associated with increased risk of VTE recurrence in male patients.
29
Thus, we stratified our data according to sex to explore the sex-specific effects of ApoM in primary VTE. Our results, however, indicated that ApoM plasma levels were not risk factor for VTE in any of the sex group. The ORs and 95% CI were as follows: for male (OR = 1.78, 95% CI = 0.17-19.15 and OR = 4.18, 95% CI = 0.23-75.23) and female patients (OR = 0.68, 95% CI = 0.08-5.90 and OR = 0.39, 95% CI = 0.02-6.09) on uni- and multivariate analysis, respectively. The
Discussion
In the present study, we have analyzed the distribution of ApoM plasma levels among patients with VTE and non-VTE patients. Our results show that ApoM levels are not significantly different among patients with VTE and non-VTE patients, while
During the recent years, efforts have been made to identify the diagnostic markers and diagnostic models for primary VTE, such as the Wells score. Despite a number of well-known diagnostic markers, that is, D-dimers, APC-PCI complex, it remains a challenge to precisely diagnose the primary VTE. 2,12,13
Apolipoprotein M is preferentially associated with HDL and plays important role in lipid metabolism as well as protection against atherosclerosis. 19,21 However, our results show that ApoM may not be a marker for primary VTE. We could not find any study showing the role of ApoM in primary VTE. Nevertheless, role of ApoM has been reported in recurrent VTE by 2 studies previously; one reported that decreased ApoM plasma levels are associated with higher risk of VTE recurrence in male patients. In the second study, genetic aberrations in ApoM were associated with increased risk of VTE recurrence in male patients. 28,29 Apolipoprotein M has also been studied for its role in other cardiovascular diseases including coronary artery disease, where low levels of ApoM were associated with high risk of disease development. 27,33 One possible explanation for the difference between our results and other’s findings could be the difference in nature of the diseases under investigation. Now it is well established that primary and recurrent VTE are 2 different diseases and their risk markers are not similar. 34,35 Contrary to intuition, studies have shown that the risk factors for the first event do not simply show the same results as for VTE recurrence. In some cases, even the results of recurrence were opposite of what was found in primary event as reported by Dahabreh and Kent and they named it “paradoxes of recurrence”. 36 Another situation that has been seen many times is that a risk factor that was strong in first event is found much weaker in the second event (recurrence). For example, thrombophilia, which is a strong risk factor for a primary VTE, increases the risk of VTE recurrence only about 1.5-fold. 34,37 Similarly, age, the strongest risk factor for primary VTE, even has no effect on the risk of VTE recurrence whatsoever. 38,39
Previous studies in VTE recurrence have shown that effects of ApoM are sex-specific 28,29 ; thus, we stratified our data according to sex. Results, however, showed that ApoM plasma levels are not different among males or females in patients with primary VTE. This discrepancy can be explained as follows: sex is a risk factor for VTE recurrence but not in primary VTE, and this sex-dependent risk of disease may explain the difference in our results from previous findings. 40
Apolipoprotein M is mainly associated with HDL having antiatherogenic properties. Several studies confirmed the association between ApoM and cholesterol metabolism. 19 Wolfrum et al reported that silencing of ApoM gene leads to 25% decrease HDL cholesterol (HDL-C) levels, while others have shown a pivotal role of ApoM in the formation of pre-β HDL. 21,41 However, inconsistent data are available on the role of HDL-C in development of primary venous thrombosis. Elevated HDL-C levels have been reported to be associated with a decreased risk of venous thrombosis in few but not in all studies, while most studies reported no association between HDL-C levels and risk of primary VTE. 42 –45 Chamberlain et al and Everett et al found no association between HDL-C and risk of primary venous thrombosis. 46,47 One may conclude from these studies that if HDL-C is not a risk factor for primary VTE, it is very rare that ApoM, that is, a part of HDL, may have a role in the diagnosis of primary VTE.
The present study has several strengths including relatively large size of samples and use of empirical clinical judgment as well as objective confirmation of VTE; we also acknowledge the possible limitation in our experimental design, which was the absence of patients with PE in our cohort which should be considered when interpreting the results. Moreover, there was a nonsignificant trend in increased risk of primary VTE in men compared to women. However, it was difficult to conclude based on our results, but it will be interesting to investigate this point in future studies. Nevertheless, it was a hypothesis-generating study in which ApoM was analyzed for its diagnostic role in primary VTE.
In conclusion, this was the first study in which we have analyzed the plasma levels of ApoM in patients with primary VTE. Our results show that ApoM may not be a diagnostic marker for primary VTE and also endorse the previous studies that risk markers for primary and recurrent VTE are different. Further studies on the role of ApoM in primary VTE, however, are required to confirm these findings in other cohorts with large number of samples.
Footnotes
Authors’ Note
The funders had no role in in study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the grants from NIH awarded to Dr. Kristina Sundquist, grants awarded to Dr Bengt Zöller by the Swedish Heart-Lung Foundation, ALF funding from Region Skåne awarded to Dr Bengt Zöller and Dr Kristina Sundquist, grants awarded to Dr Kristina Sundquist by the Swedish Research Council, and grants awarded to Dr Jan Sundquist by King Gustaf V and Queen Victoria’s Foundation of Freemasons.