
Abstract
The common peroneal nerve stimulator (CPNS) is a UK–approved device for reducing venous thromboembolism risk. It resembles a wrist watch and is placed over the common peroneal nerve to fire at 1 electrical impulse/sec. The aim was to quantify the claim that it drives the venous muscle pump and imitates walking. Twelve healthy volunteers performed 10 tip-toe maneuvers and 10 ankle dorsiflexions to imitate walking movements. The reductions in calf volume were recorded using air plethysmography (APG). The common peroneal nerve was stimulated for over 10 seconds at each of the 7 increasing electrical impulse settings, and the volume reductions were measured for comparison. The results are expressed as median (interquartile range) absolute (mL), and percentage reduction in calf volume. Tip-toe and dorsiflexion pumping maneuvers were not significantly different: 59 (33.6-96.1), 81.9% vs 51.4 (34-68.5), 59.7%, respectively (P = .53). However, they both outperformed the CPNS: 10.8 (7.3-18), 13.2% at P = .002 and P = .002, respectively. Qualitatively, the CPNS registered on the tracings as a small spike (muscle twitch) at low settings, with larger amplitudes (ankle jerk) at higher settings. The CPNS activity spikes were discrete, lasting a median (range) of 0.24 (0.16- .3) seconds. The claim that the CPNS empties veins by pumping is supported statistically. However, the amount is small versus the tip-toe and dorsiflexion maneuvers. Furthermore, the CPNS has a short activity profile on the APG trace. Innovations that produce sustained contraction and involve the posterior calf compartments may improve pumping.
Keywords
Introduction
It is well known that venous thromboembolism (VTE) is a major contributor to morbidity and death worldwide. This can be prevented by the administration of anticoagulants. Venous thromboprophylaxis can be achieved also by nonpharmacological methods. These include intermittent pneumatic foot and/or calf compression, 1 medical compression stockings, 2 and electrical stimulation directly over the calf muscles 3 or indirectly via the common peroneal nerve. 4 Their aim is to facilitate the venous return in order to reduce the risk of VTE. Active or passive pumping is believed to be their prime mechanism of action.
The common peroneal nerve stimulator (CPNS) is a National Institute for Health and Care Excellence (NICE)–approved device in the United Kingdom. Its value is that it does not have the pharmacological side effect of bleeding, and its discrete nature means that it can be applied in situations where intermittent pneumatic calf compression is not applicable. For example, with plaster casts and orthopedic external fixation devices. The NICE document claims that it “drives the venous muscle pump, facilitating the emptying of veins to imitate the process normally achieved by walking” (NICE medical technology guidance 19). 5
The aim of this study was to investigate the performance of the CPNS device (geko™, Firstkind Ltd, Hawk House, Peregrine Business Park, High Wycombe, Bucks, UK) at calf pumping in comparison to the tip-toe and dorsiflexion movements that form part of walking.
Since 1964, air plethysmography (APG) has been used as a device that records a change in calf volume. 6 The volume of the calf decreases as venous blood is pumped out. This can be measured numerically with APG. 7 The APG sensor cuff is wrapped around the calf while the CPNS is strapped over the common peroneal nerve. In this way, pumping can be quantified as an absolute (mL) or percentage reduction in calf volume. This is the first time the CPNS has been evaluated as a pumping device by measuring volume change.
Method
Study Design
This was a single-center prospective study performed in Ealing Hospital on the right legs of 12 healthy volunteers. This side was selected because it was closest to the APG apparatus and the investigator. All volunteers received an information leaflet and had the opportunity to see the device in action and to test it on themselves prior to signing a consent form. Inclusion criteria were the absence of significant leg problems or symptoms and the willingness to take part in the study. Volunteers with overt venous skin changes, dermatitis, poor mobility, or significant leg edema were excluded.
The maximum calf circumference was measured while supine with the heel elevated on a foam support. The largest area was assessed by eyeballing the calf. Several readings were taken, and the greatest value was used for the record.
Pumping Tests
All 3 pumping tests were carried out during a single session in our laboratory from a position of stationary standing. The APG sensor cuff was wrapped around the calf of the test leg throughout the study (Figure 1). The participants were dressed in nonrestrictive clothing using shorts or loose fitting theater garments to ensure that there was no impediment to venous return.
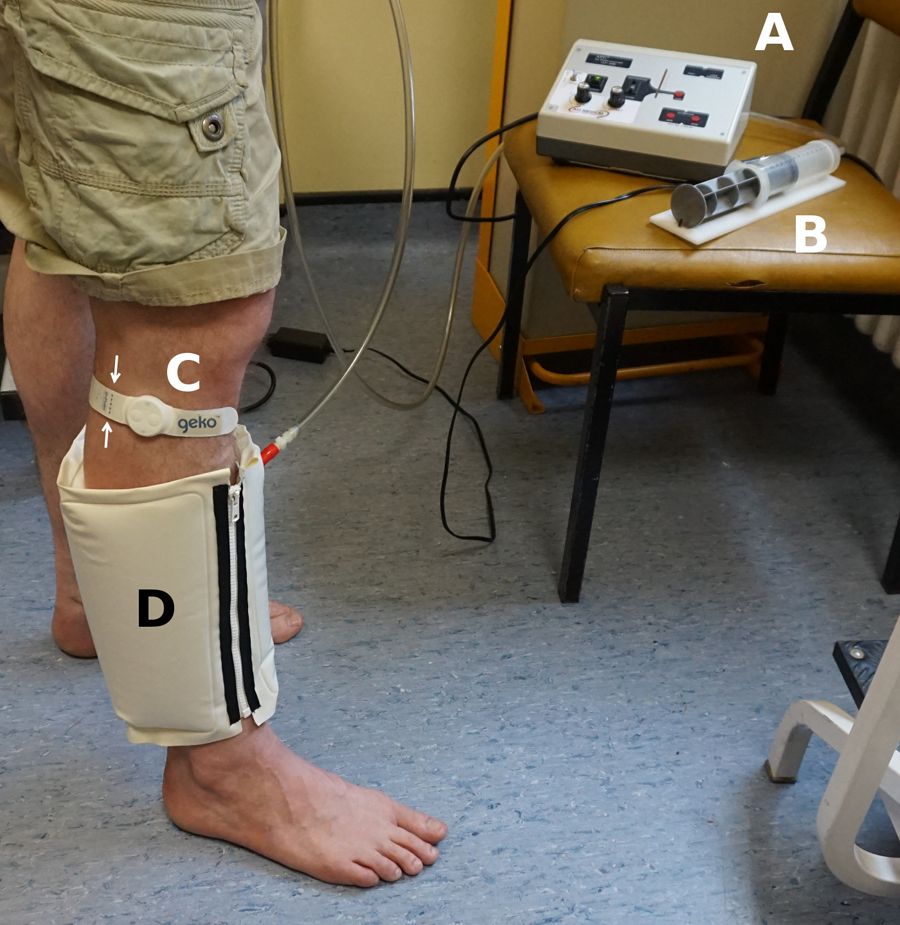
Experimental setup. (A) APG pump and transducer unit, (B) Calibration syringe, (C) CPNS device in situ across the common peroneal nerve (arrows), (D) air sensor cuff wrapped around a dependent non-weight-bearing leg measuring the decrease in calf volume in response to CPNS activity at each of the intensity settings from 1 to 7. APG indicates air plethysmography; CPNS, common peroneal nerve stimulator.
The tip-toe maneuver (TTM) was performed on equal weight bearing, with the legs slightly apart to make room for the calf cuff. The subjects were instructed to lift their body weight up onto their toes, with their heels off the ground, and down again, 10 times, at an approximate frequency of 1 TTM per second. An aluminum support frame was provided in front of the subject should a loss of balance occur.
The dorsiflexion maneuver (DFM) was performed on the leading leg, positioned a foot’s distance in front, making sure that both feet were flat on the ground. Nearly all their body weight was supported on the rear leg. The leading foot was dorsiflexed, 10 times, at a rate of 1 DFM per second, with the APG cuff recording the reduction in calf volume.
The CPNS device (geko version T-1) delivers pulse widths of 70, 100, 140, 200, 280, 400, and 560 μs to reflect the 7 intensity settings. The pulse current is 27 mA (±15%) with a repetition rate of 1 Hz (±5%). The CPNS was activated with the subject's body weight on the contralateral leg. The hips were supported at the edge of an examination couch, adjusted to a suitable height, so that the subject could lean back slightly. This ensured stability and offset some of the fatigue, inevitable while standing on 1 leg for the duration of the test. First, the CPNS was activated at intensity setting no. 1 for at least 10 seconds (10 electrical impulse cycles) and then through each intensity setting until the final setting at no. 7. The final setting was repeated twice to ensure that the maximum amount of volume reduction was achieved prior to switching the device off. Each increment intensity was recorded on the APG tracing as an event. This was depicted as a straight vertical line, with the number of vertical lines corresponding to the intensity setting number.
The device was positioned as recommended by the manufacturer across the common peroneal nerve. Stimulation activates the muscles of the anterior and peroneal compartments of the calf (Figure 2). At low intensity, these muscles can be seen to twitch with each impulse. At the higher settings, the foot starts to jerk upward and outward reflecting the action of the extensor (anterior compartment) and peroneal (peroneal compartment) muscles. The setting at which the foot first started to move was documented.
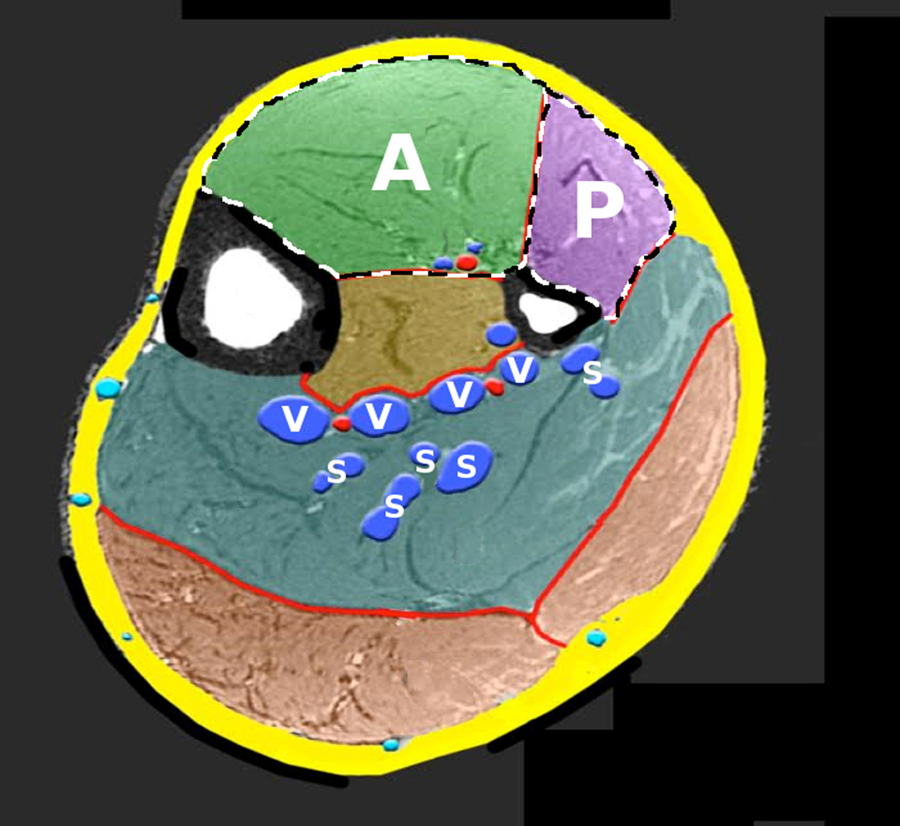
Modified magnetic resonance image of the mid-calf standing demonstrating the anterior (A) and peroneal (P) compartments that together occupy 25.9% of the cross-sectional muscle mass (ImageJ™). Deep veins (V); venous soleal sinuses (S). With kind permission, Jean-François Uhl, Descartes University, Faculty of Medicine, Paris.
Air Plethysmography
Calf volume change calibrated to milliliters formed the basis of the results. It was measured using APG (ACI Medical LLC, San Marcos, California). The volume versus time tracings were recorded in files with a .WDQ extension, so that they could be played back and analyzed using the noncommercial software (WINDAQ™ Waveform Browser; DATAQ Instruments, Akron, Ohio).
The first value measured was the range of change in volume from a position of high leg elevation in the supine position to standing dependency. This was recorded as the working venous volume (wVV). Subsequently, the ejection volume (EV) as a result of the pumping effect of the TTM and then the DFM were recorded. Finally, the decrease in volume (EV) in response to the CPNS set at the maximum intensity setting (no. 7) was recorded. Care was taken to ensure that the leg veins were “full” prior to each of the 3 tests. This was seen on the APG tracing as a horizontal plateau that represents the state when the arterial inflow into the leg equals the venous outflow. On dependency, with the leg hanging freely, normal calf veins fill usually within 2 to 3 minutes, and it was from this plateau that the tests were performed in order to register maximum possible ejection.
The ejection fraction (EF) is a derived APG parameter. It is the EV/wVV and expressed as a percentage of the wVV ejected. Both the EV (mL) and the EF (%) were used in the analysis of pumping performance. By definition, the EV and EF measure the effect of a single pumping maneuver. 8 However, in this article, it was taken as the total volume ejected after 10 maneuvers or 10 CPNS impulses. The reason is that it is very difficult to record the pumping effect of only 1 CPNS impulse and then switch the device off while it is attached to the calf, without creating movement artefacts. Ten pumping actions, 1 second apart, for each test provided comparability.
Statistical Analysis
The Microsoft® Office Excel 2003 spreadsheets and the IBM® SPSS® statistics package version 22 (IBM Corporation, USA) were used to record the data, perform the statistical analysis, and display the results. The data were expressed as median, interquartile range, and range. Pumping comparisons from the 3 tests were assessed using the nonparametric Wilcoxon signed rank test. The Spearman ρ test was used for correlations. Significance was set when P < .05.
Results
Participant Characteristics
Of the 12 participants who completed the study, 3 were females. A 4th female volunteer declined to take part because of excessive pain with the device. All volunteers exhibited muscle twitching and foot jerking, but the intensity settings required to deliver this response differed between individuals. The intensity settings (1-7) required to start a movement of the foot was 1 (n = 1); 2 (n = 3); 3 (n = 2); 4 (n = 2); 5 (n = 2); 6 (n = 2); and 7 (n = 0). The characteristics of the 12 participants are shown in Table 1.
Characteristics and APG Parameters Defining the Study Volunteers.
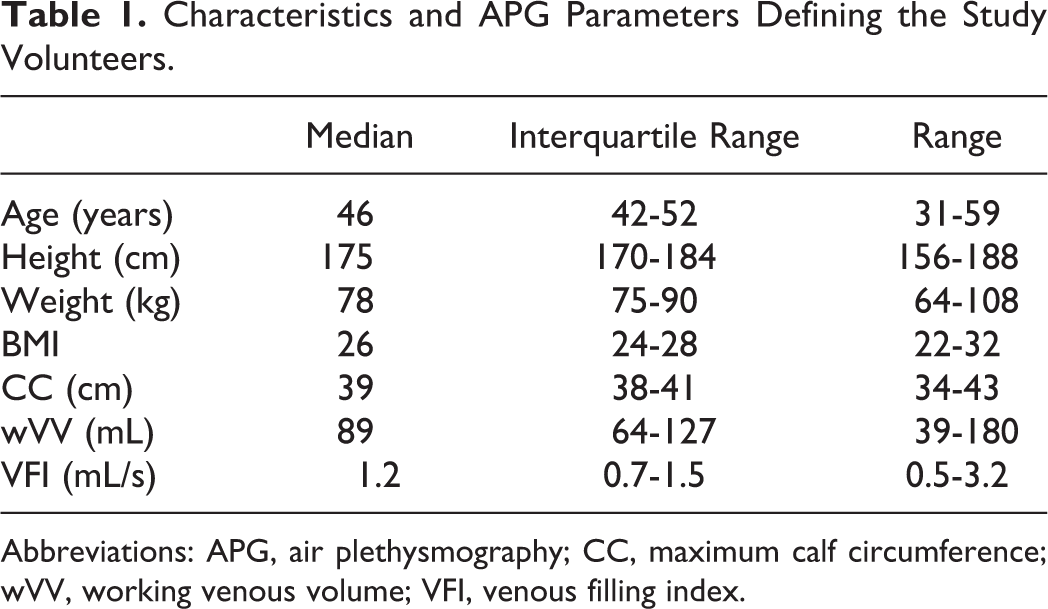
Abbreviations: APG, air plethysmography; CC, maximum calf circumference; wVV, working venous volume; VFI, venous filling index.
Significant correlations (Spearman) were not observed between the maximum calf circumference and any of the APG parameters indicating that static calf dimensions bear no relationship to dynamic pumping activities. The venous filling index (VFI) measures the rate of calf expansion on dependency and is a surrogate for global reflux. The VFI was 3.2 mL/s (normal: <2.9 mL/s) in 1 volunteer, indicating that there may be occult reflux present in that patient. 9
Pumping Comparisons
A typical tracing is shown in Figure 3. The impact of the 3 tests at reducing the volume of the calf appeared to be more with the maneuvers that are used in walking. In this tracing, the TTM had the greater effect in pumping compared to the DFM. Despite selecting the tracing of the volunteer with the maximum effect of the CPNS, the pumping volume was still small with the CPNS in comparison to the walking movements.
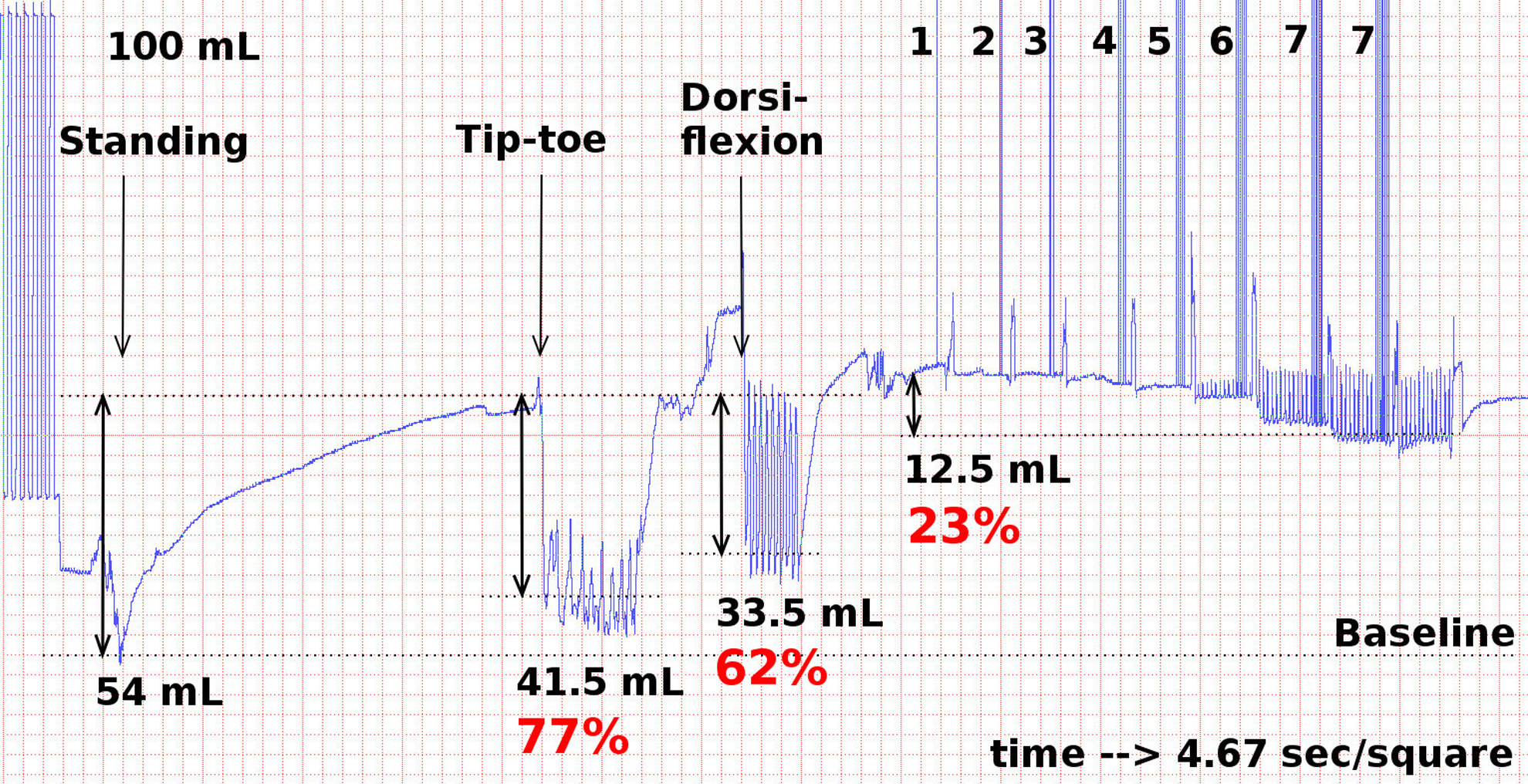
Volume versus time APG tracing comparing the reductions in calf volume in the volunteer who had the maximum pumping effect with the CPNS. The 100 mL calibration is on the left, with the working venous volume (wVV) from leg elevation to dependency of 54 mL. The absolute and percentage reduction on the wVV of the tip toe and dorsiflexion maneuvers, and the CPNS at the highest intensity setting (no. 7) are shown. APG indicates air plethysmography; CPNS, common peroneal nerve stimulator.
The collective results are illustrated in Figure 4 with numerical values displayed in Table 2. Surprisingly, the performance of the TTM was not significantly different to the DFM, irrespective of whether the EV or EF was used as the measurement (Table 2). All the tests had a statistically significant impact in pumping in comparison to no pumping, but the effect of the CPNS was very small.
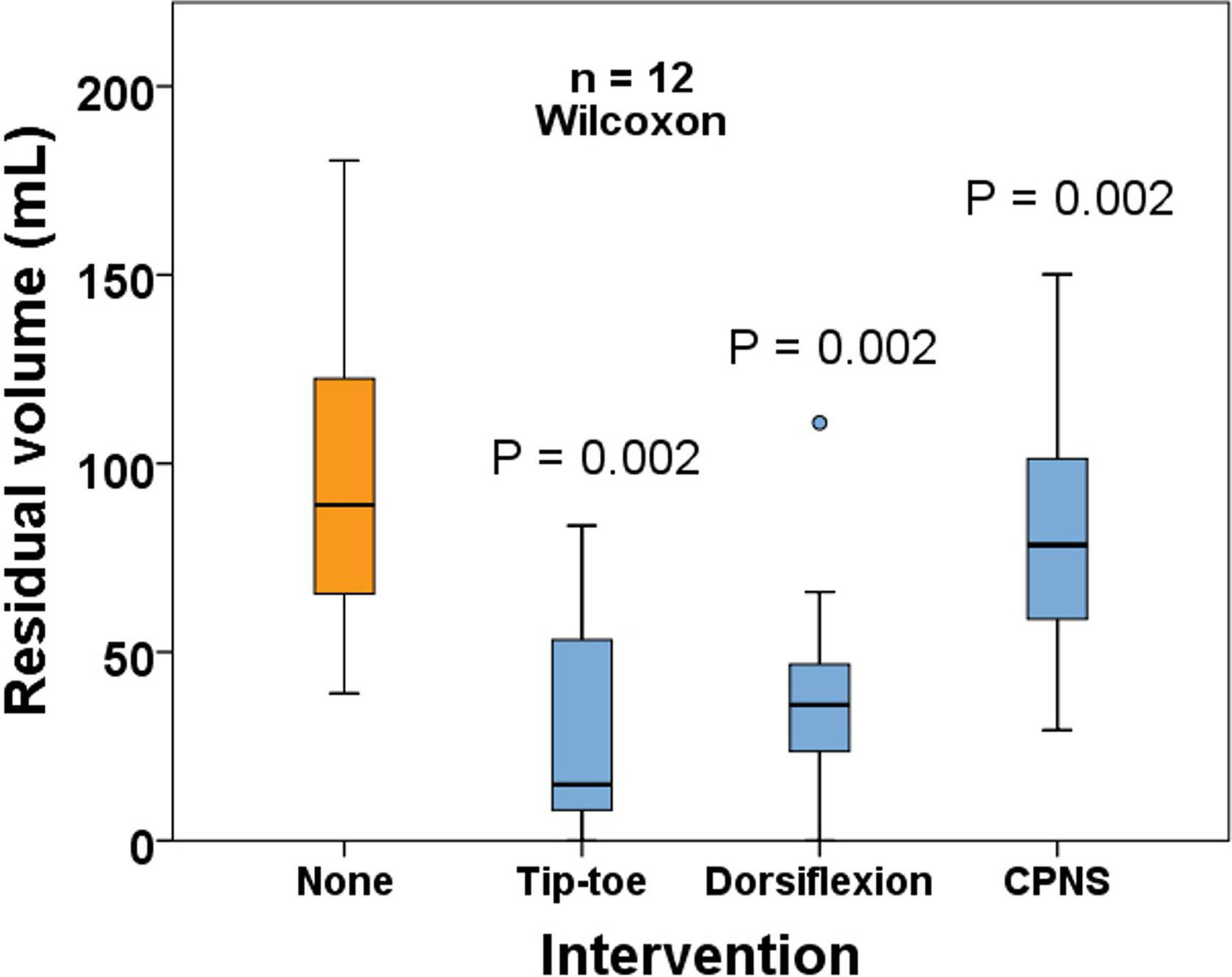
Box plots demonstrating the working venous volume (wVV) remaining in the calf after 10 tip-toe maneuvers, 10 dorsiflexion maneuvers, and the CPNS device set at the maximum intensity setting using APG. Without intervention, the volume illustrated (none) is the elevation to dependency volume change (wVV). The P values demonstrate the significance of the decrease in volume versus none. APG indicates air plethysmography.
Values and Comparative Performance of the 3 Pumping Tests.a
Abbreviations: TTM, tip-toe maneuver; DFM, dorsiflexion maneuver; CPNS, common peroneal nerve stimulation (maximum setting); EV, ejection volume; EF, ejection fraction.
aData are expressed as median (interquartile range).
bWilcoxon signed rank test.
cStatistically significant difference are given in boldface.
CPNS Pumping
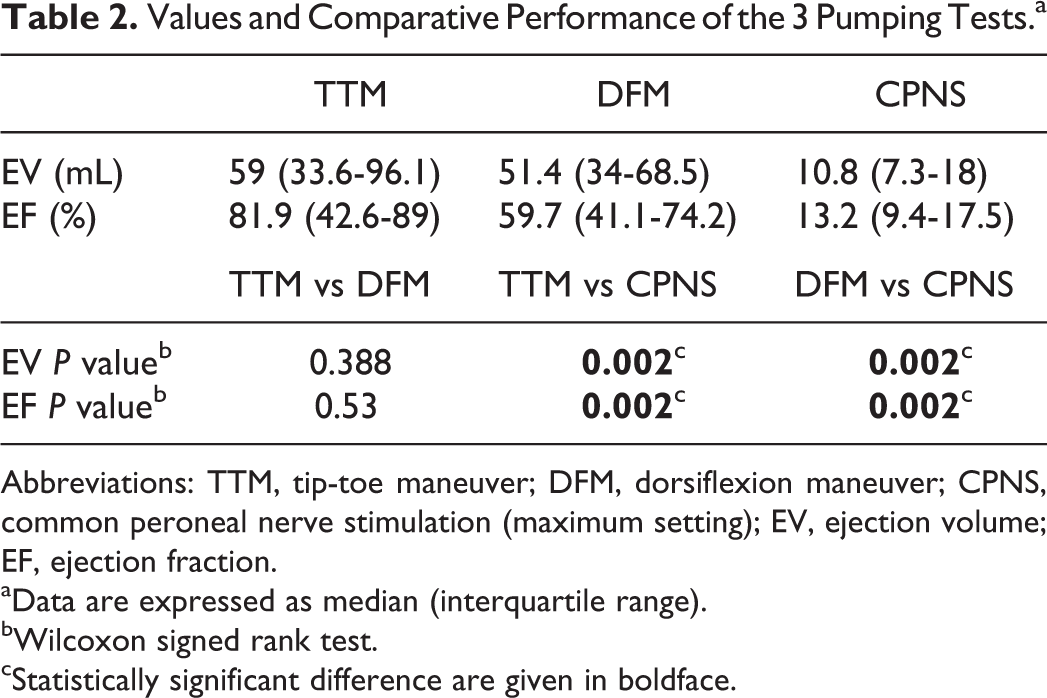
The detailed effects of CPNS on the APG tracing are shown in Figure 5A and B. As the muscles in the anterior and peroneal compartments commence twitching with increasing electrical intensity, this movement can be seen on the high-resolution tracing as a spike (Figure 5B). The duration of these spikes in the group lasted a median (range) of 0.24 (0.16-0.3) seconds. Since the impulse rate was set at a frequency of 1 per second, the median percentage of the cycle occupied by contraction was 24. The remainder of the cycle was without movement. During this time, there was a miniscule increase in the volume of the calf. The slight incline of the tracing between the spikes can be seen if observed carefully in Figure 5B. When the device was switched off at intensity setting no. 7, the calf returns to its original volume (Figure 5A).
Volume versus time APG tracing. A, Low resolution. The numbers alongside the vertical event markers indicate the CPNS intensity setting. The volume starts to decrease at setting no. 4 and returns to full volume (plateau) after the device is turned off (arrow). B, High resolution depicting the detail encircled in (A). Discreet spike impulses are recorded with the same frequency as the muscle twitches (1/s) with minimal activity during the remaining part of the pumping cycle. APG indicates air plethysmography; CPNS, common peroneal nerve stimulator.
The spikes represent a short temporary pressure increase and decrease in the sensor cuff of the APG apparatus. This is concordant with the muscle twitches and jerks observed during CPNS activation. They do not represent a sudden increase and decrease in calf volume.
Discussion
The pathophysiological cause of deep venous thrombosis (DVT) has not changed significantly since the original hypothesis of Virchow’s triad: endothelial injury, hypercoagulable state, and stasis. 10 Stasis is required for fibrin formation. 11
A recent systematic review detailed the effects of many different neuromuscular electrical stimulation devices on venous blood flow and its role in thromboprophylaxis. 12 Increased venous blood flow was reported in the 21 articles identified. However, in the 10 comparative studies identified, the reported incidence of DVT ranged from 2% to 50% with electrical stimulation versus 6% to 47.1% in the controls. The review concluded that current evidence does not support a role for neuromuscular electrical stimulation in thromboprophylaxis.
A randomized, prospective, multi-institutional study, with interval results (1, 3, and 6 months), assessing the device with VTE endpoints in high-risk patients versus low risk is required to confirm or refute the efficacy of the device. Such a study should involve orthopedic surgery or other operations with confirmed higher DVT risks.
Four recent studies, all sponsored by the manufacturer, have focused on increased ultrasound flow parameters as a conclusion in evaluating the performance of CPNS stimulation. 4,13 –15 One study assessed femoral vein flow supine and standing with a below-knee plaster cast on 10 healthy volunteers. 13 Another study compared CPNS to 1 intermittent pneumatic compression device on 10 healthy volunteers with ultrasound over the femoral vein and artery. 14 A similar study compared CPNS to 2 intermittent pneumatic compression devices on 10 healthy volunteers with ultrasound over the femoral vein and artery. 15 The most recent study on 18 healthy volunteers insonated the axial deep venous of the calf and demonstrated an improvement of flow parameters in all 3 veins with CPNS. 4 Interestingly, all these studies focused on the magnitude of effect of the device on increasing venous flow, implying that this gives better protection against DVT. However, there is no evidence to support a dose–response relationship with increasing flow providing more protection from DVT. Moreover, it has been argued that high-peak venous velocities may increase the risk of DVT. 16 All the veins in the above studies had measurable flow before the CPNS device was activated. There was no record of stasis within these veins. Contrary to the information stated in these studies, the stasis part of Virchow’s triad would not be a valid argument promoting the CPNS device for DVT prophylaxis.
The current study on 12 healthy volunteers focused on the pumping abilities of the CPNS device to investigate the claim from the NICE document on how it works. 5 Pumping was measured using APG and defined as the ability of the calf to reduce its volume. Comparisons were made with 2 walking movements: tip toe and dorsiflexion. Unlike the above studies on ultrasound flow assessments, no claim is made that better pumping equates to better DVT prophylaxis. However, this study is unique because it has investigated pumping in comparison to walking movements.
An explanation as to why the CPNS behaves as a poor pump is shown in Figure 2. The muscles of the anterior and peroneal compartments which are activated form approximately 26% of the bulk of the calf. Furthermore, these compartments are separate from the major veins of the soleus and gastrocnemious muscles and the veins in the deep compartment. The CPNS isolates the contraction of the muscles in the anterior and peroneal compartments while preserving the powerhouse muscles that clad the veins of the calf muscle pump.
Interestingly, there was no significant difference in pumping between the TTM and the DFM. It would be anticipated that the TTM is better because of the involvement of the posterior and deep compartments of the calf. There are 2 explanations. The first is that it is difficult for a person to perform isolated muscle contractions of the anterior and peroneal compartments. It is likely that the posterior compartment contracts also with a dorsiflexion in order to stabilize and protect the ankle joint, preventing it from overextending or jerking. The second was described by Gardner and Fox 17 who performed lower limb venography with the aim of defining the movements involved in pumping. In particular, dorsiflexion causes the posterior compartment muscles to descend into rigid fibrous sheaths which force the venous blood out of the muscle sinuses and deep veins, just like a wet sponge is wringed out to release its water.
Similarities may exist between the spike impulses observed on the APG tracing (Figure 5B) and the spikes observed on the duplex ultrasound velocity profiles when the CPNS is activated. Both are short, lasting <1/4 second. They may not represent volume flow but pressure impulses which transmit much faster than flow waves. Ultrasound measurements on arterial inflow into the leg and venous outflow from the leg should be equal. However, this is not the case. 14,15,18 The difficulties in discriminating volume flow and the impulse velocities from pressure waves may be responsible for the inbuilt machine errors associated with interpreting the reflected sounds back into the ultrasound transducer.
The relationship between pumping, ultrasound measurements of flow and velocity, venous stasis, and prophylaxis against VTE is not clear. This is a grossly underresearched area in DVT prevention. Since stasis occupies one-third of Virchow’s triad, it may be appropriate for further research studies to quantify stasis rather than focus on the surrogate markers of antistasis like pumping, flow, and velocity. 19 Nevertheless, this study has clarified that the mechanism of action of CPNS in protecting against any thrombotic activity is unlikely to be achieved primarily by pumping.
Conclusion
In comparison to walking movements, the CPNS device is not efficient as a venous pump. However, statistical tests did demonstrate a significant but miniscule pumping effect versus stationary standing. Devices that cause a sustained coordinated muscle contraction in the posterior compartments of the calf may be more effective. The results of this study question the claim by NICE that the mechanism of action of geko in VTE prophylaxis is by pumping. In this regard, the study is likely to have a clinical impact by reducing the use of a device of borderline pumping effect. Furthermore, the muscle twitches, and ankle jerks observed with the CPNS device do not resemble walking in neurologically intact individuals. The NICE guideline on the mechanism of action of the CPNS device in venous thromboprophylaxis requires revision in keeping with the results of this study.
Footnotes
Authors’ Note
This work was presented as an oral abstract in 3 societies: (i) BRONZE PRIZE, 29th Annual Congress of the American College of Phlebology, 11-15 Nov 2015, Orlando, FL, USA; (ii) Vascular Society for Great Britain and Ireland, 11-13 Nov 2015, Bournemouth, Dorset, UK; (iii) XXVII World Congress of the International Union of Angiology, October 5-8, 2016, Lyon, France. The demographic details, pumping data and APG tracings of the study participants are held at the Josef Pflug Vascular Laboratory, 7th Floor Ealing Hospital, Middlesex, UB1 3HW, UK.
Acknowledgments
The authors wish to thank the nurses and doctors of the Anaesthetic, Intensive Care Unit, and Vascular departments who volunteered their legs for this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.