
Abstract
Our aim was to measure the venous blood flow velocity (VBFV) in case of hemiparetic patients, after passive and active thromboembolic methods, as well as the consensual effect in the hemiparetic limb following the active venous exercises in the healthy limb. We examined 215 patients, with the median age of 58.0 (55.0-63.0) years. The VBFV was measured with a HADECO BIDOP ES-100 V II type Doppler ultrasound device, using an 8 MHz head, on the femoral vein at the level of the hip joint. For statistical analysis, SPSS version 22 was used. After passive movement, on the hemiparetic side, compared to the value in resting state, the VBFV significantly (12.6; 11.6-13.5 cm/s; P < .001) increased. Following active venous exercises performed on the healthy side, the VBFV significantly (18.0; 15.6-19.6 cm/s; P < .001) increased compared to the value in resting state. Following the active venous exercises performed on the healthy side, the VBFV measured on the hemiparetic side (consensual effect) was significantly (15.1 [14.1-16.5] cm/s; P < .001) higher than the value on the hemiparetic side in resting state. Active and passive mechanical thromboprophylaxis methods can be effective. Movements of the healthy limb significantly increase the VBFV in the inactive limb, and patients can perform it themselves several times a day.
Introduction
The estimated worldwide incidence of stroke is 16.9 million cases. Hospitalized patients suffering from acute ischemic stroke have shown a high prevalence of total venous thromboembolism (20%-40%) in the absence of venous thromboembolism prophylaxis. The venous thromboembolic conditions pose serious health care, social, and economic problems in developed countries. 1,2 The hemiparetic patients are considered to be a highly endangered patient group concerning thromboembolism due to the prolonged immobility and inactivity and the deterioration of the muscle pump function resulting from muscle weakness causing increased venous stagnation. 3 –5
The prophylactic effect of mechanical methods is realized through the termination or alleviation of stasis and through increasing venous blood flow velocity (VBFV; the distance traveled by a given amount of liquid over time). The alleviation of venous stasis can be achieved by the constriction of the vein, by enhancing lymphokinesis, and by regulating the skin–muscle–fascia tone. 6 –8
The components of mechanical prophylaxis are passive techniques: positioning, elevation of the limbs, 9 massage, compression treatments (continuous elastic compression treatment, intermittent pneumatic compression stocking), 10 –12 electric nerve stimulation, transcutaneous electrical nerve stimulation, 10,13 electrical foot stimulation, 7 electric muscle stimulation, 9 passive movement, and active methods. 14,15
The active mechanical methods include breathing exercises, 16,17 leg pedal exercises, novel leg exercise apparatus, 18 and venous exercise with the lower limbs. 14,15 Consensual effect can also be added as an increase in the flow of the hemiparetic limb following the active movement of the healthy limb. 15 Treating the healthy side (massage, thermotherapy) has a good benefit on the contralateral side, in this case among hemiparetic patients on the hemiparetic side.
Several authors have examined the passive and active thromboprophylaxis methods among healthy volunteers and hospitalized patients, but relatively few objective examinations are available concerning the efficiency of these methods in case of hemiparetic patients, focusing on venous blood flow changes. From passive mechanical thromboprophylactic methods, passive movement is less examined and we did not find any study that scanned the change of venous blood flow in the lower limbs following passive movement.
Authors have found significantly higher VBFV compared to the resting value due to active thromboprophylaxis. It can be an interesting question, that in the hemiparetic side, how much the rest venous blood flow rate decreased compared to the healthy side, as well as it would be interesting to measure the consensual effect: After the active exercise of the healthy limb, how much the venous blood flow increases in the hemiparetic lower limb.
In this study, we are seeking answers to the questions how the VBFV in case of hemiparetic patients change on the healthy and hemiparetic side after thromboembolic treatments. We also observed the extent to which the movement of the healthy limb can improve the venal circulation of the hemiparetic side (consensual effect). 19 We explored whether the improvement in venal circulation resulting from the active exercise of the healthy side is sufficient for mechanical thromboprophylaxis.
We had 4 hypotheses: (1) It is assumed that the resting VBFV in the hemiparetic lower limb is significantly lower than the resting VBFV in the healthy lower limb. (2) It is assumed that after fast-paced passive movement, the VBFV significantly increases in the limb on the hemiparetic side. (3) Following venous exercise performed on the healthy side, the VBFV in the healthy lower limb significantly increases compared to the resting VBFV measured in resting position. (4) Following venous exercise performed on the healthy side, the VBFV in the hemiparetic lower limb significantly increases compared to the resting VBFV measured in the hemiparetic lower limb, thus the consensual effect can be detected.
Methods
Study Design
The study was a prospective cohort study. The survey and examination of the patients was carried out at the Rehabilitation Ward for Patients with Severe Brain Injury of the Neurosurgery Department of the Clinical Centre of University of Pécs and at the University of Pécs, Faculty of Health Sciences, Institute of Physiotherapy and Sport Science, in Hungary. The examinations were performed between January 10, 2016, and September 15, 2017.
Patients
In this study, we examined 215 persons (117 males, 98 females) with hemiparetic stroke diagnoses (42.79% ischemic, 57.21% hemorrhagic). Patients could participate in the research, with a 2 or lower limb muscle strength value on the hemiparetic side in the Research Medical Council 0-5 system (the patient is capable of active movement perpendicularly to the line of gravity, but not against gravity). 20
In the healthy limb, there were minimum 3 muscle strength values according to Research Medical Council 0-5 system, which means who are capable of active movement against to gravity, but not against to resistance.
The exclusion criteria included deep venous thrombosis, any thromboembolic event, pulmonary embolism, arteriosus circulatory disturbance, neuropathy, vascular complications, arteriosclerosis obliterans, malignant tumors, swelling, necrosis, epidermization, heart failure, systolic blood pressure above 180 mm Hg, a history of diastolic blood pressure above 110 mm Hg, serious internal-musculoskeletal-psychiatric diseases, repeated stroke, and other neurologic disease besides stroke, and bigger than 35 kg/m2 body mass index. 15 –17
Patient selection was according to neurologist and rehabilitation specialists by taking into account both the inclusion and exclusion criteria. Patients received oral and written informative about the process and the aim of the study. They participated voluntarily and signed informed consent.
Ethical Consideration
The research ethics approval was granted by the University of Pécs Clinical Centre Regional and Institutional Research Ethics Committee; its record number is 6129/2016.
Data Collection
We carried out a questionnaire and also through measuring the VBFV. We used a self-prepared questionnaire in the study. The items of the questionnaire included questions concerning the diagnosis, companion diagnosis (deep venous thrombosis, arteriosus circulatory disturbance, type II diabetes mellitus), cardiovascular diseases, previous operations, taking medication, the length of immobility, the scale of mobility, and the use of medical aids.
Determining VBFV in Resting State
The VBFV was measured with a HADECO BIDOP ES-100 V II type Doppler ultrasound device, using an 8 MHz head, in “peak velocity” mode (Kawasaki, Japan). The VBFV was measured in the femoral vein, at the level of the hip joint. Before measuring, patients were rested in bed for 30 minutes.
During the examination, the participants were wearing comfortable, loose clothing, and only underwear on their lower body. They were positioned in supine, in horizontal position, the head of the bed was not raised, and there was a 4-cm pillow under the head. The examination room was equipped with an air conditioner; for this reason, we could set the temperature to the optimal level between 22°C and 24°C.
Passive Movement in the Hemiparetic Lower Limb
Fast-paced passive movement was performed in a large articular range of motion, with a high repetition number. 20 During the movement, the patient was in a relaxed state; we moved the joints without any contributing muscular activity by the patient. In the course of the passive movement, the base joint of the big toe was moved in flexion and extension direction; the ankle joint was moved in plantar, dorsal flexion, and pronation and supination directions and circumduction; the knee joint was moved in flexion and extension directions; and the hip joint was moved in flexion, extension, abduction, and adduction directions and inward and outward rotation and circumduction with a repetition of 16 in every joint, in every direction.
At each examination, we determined the effect of passive movement on VBFV at the first 10 minutes and at the 15th minute, after doing all the passive movements in all the lower limb’s joints from proximal to distal, in every direction.
Venous Exercise Program for the Healthy Lower Limb
The participants performed the venous exercise program in supine position. The patients were not wearing any medical aids facilitating venous flow, such as compression stockings or elastic bandage.
In accordance with the physiological principles, the structure of the exercise program was the following: breathing exercises to facilitate return flow from the abdominal cavity to the heart, the isometric exercises of lower limbs from proximal to distal, due to discharge into the veins of the lower limb, isotonic exercises of the lower limbs using the pump function of the muscles from distal toward proximal, lifting the lower limb over the level of the heart to take advantage of gravity, ankle movements with leg lifting to use the combined effects of gravity and muscle pumps, pelvis lifts due to discharge from the lesser pelvis, finally, the exercise program was closed with breathing exercises to facilitate the return flow of venous blood from the abdomen toward the heart.
14
–16,21
The exercises of the applied training are dynamic. The repetition number of breathing exercises was 16, the repetition number of the isometric exercises of lower limbs (from proximal toward distal) was 16, holding for 3 seconds, the number of repetitions for the isotonic exercises of the lower limbs (from distal toward proximal, small movements, then vigorous large movements) was 16, the repetition number of lifting the lower limbs was 16, the repetition number of ankle movements with leg lifting was 16, the repetition of lifting the pelvis was 16, holding it for 3 seconds, and the repetition number of breathing exercises was also 16. 22
Consensual Effect in the Hemiparetic Lower Limb
After exercising the healthy limb, we examined the effect of the venous exercises on the healthy side and also the consensual effect and the VBFV on the hemiparetic limb, at the first 10 minutes and at the 15th minute. 15
Data Analysis
Baseline characteristics were summarized using descriptive statistics. Continuous variables were reported as median and interquartile ranges; categorical variables were reported as percentages and confidence interval. The distribution of the data was examined with boxplots and Q_Q plots, and non-normality was confirmed by Kolmogorov-Smirnov tests. In accordance with the results of the normality test (P < .05), we used nonparametric test during the statistical analysis: Within-group differences were tested using the Wilcoxon signed-rank test, group differences were tested using Mann-Whitney U test, and Friedman test was used to test the changes in time adjusted for multiple comparisons, using Bonferroni correction. The P value was considered significant if it was lower than .05. We used SPSS software version 22 for the statistical analysis.
Results
Characterization of the Sample
The study examined 215 persons and consort flow diagram shows the enrolment (Table 1 and Figure 1).
Characterization of the Sample.


Flow diagram of how the number of participants has changed during the study.
Venous blood flow velocity in resting state
In case of patients who suffered a brain infarction, a median VBFV value of 7.0 (6.2-7.8) cm/s was measured in the femoral vein of the healthy lower limb, in supine resting position. On the hemiparetic side, also in supine resting position, a median VBFV of 2.7 (2.4-4.4) cm/s was measured. The VBFV measured in resting state was 42.1% (35.6%-51.4%) lower on the hemiparetic side than on the healthy side. The VBFV measured in resting state on the hemiparetic side was significantly lower (Z = −4.8, P < .001, Wilcoxon signed rank test) than the VBFV measured in resting state on the healthy side (Table 2; Figures 2 and 3).
Changes of Venous Blood Flow Velocity (cm/s) Measured in the Femoral Vein as a Result of Passive Movement in the Hemiparetic Side.a

Abbreviations: HI, hemiparetic side; IQR, interquartile range; VBFV, venous blood flow velocity.
aN = 215.
bWilcoxon signed rank test.
cFriedman test using Bonferroni correction.
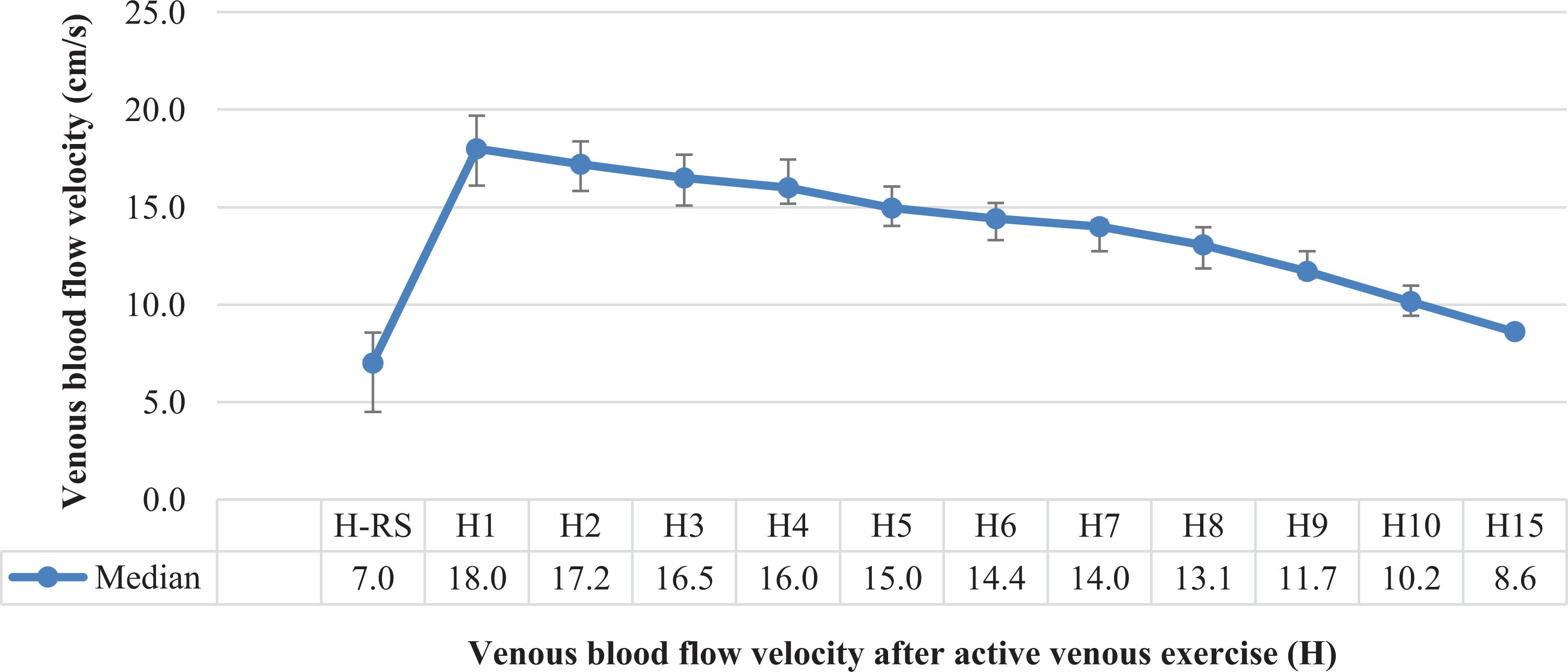
Venous blood flow velocity values after active exercises on the healthy side.

Venous blood flow velocity values of the consensual effect on the hemiparetic side after active venous exercise on the healthy limb.
Venous blood flow velocity following passive movement of the hemiparetic lower limb
Following the passive movement on the hemiparetic side, compared to the values received in resting state, the VBFV increased significantly (12.6; 11.6-13.5 cm/s; Z = −4.8, P < .001, Friedman test). The VBFV measured in the hemiparetic side in resting state increased by 4.5 (3.5-5.3) cm/s following the passive movement. The VBFV gradually decreased in the period after the treatment, but even the value measured 15 minutes later is significantly higher than the value of the hemiparetic side measured in resting state. The value measured on the hemiparetic side 15 minutes after the treatment is similar to the value of the healthy side of measured in resting state (Table 2).
Venous blood flow velocity in the healthy limb measured following venous exercise program
Following active venous exercises performed on the healthy side, the VBFV in the healthy lower limb significantly increased compared to the resting VBFV value measured in the healthy lower limb, from 7.0 to 18.0 cm/s (15.6-19.6 cm/s; Z = −4.8, P < .001, Wilcoxon signed rank test). In the minutes following the treatment, the scale of the change decreased, but even the value measured 15 minutes later (8.6; 7.9-9.4 cm/s) was significantly higher than the VBFV measured in resting state (χ2 = 299.5, P < .001; Figure 2).
Consensual effect. Following active venous exercise on the healthy limb, the results of the VBFV measured on the hemiparetic side
In this study, we examined the consensual effect. Following active venous exercise program on the healthy side, we measured VBFV on the hemiparetic side, which was 15.1 (14.1-16.5) cm/s, being significantly higher (Z = −4.8, P < .001, Wilcoxon signed rank test) than that in resting state, 2.7 (2.4-4.4) cm/s. Thus, the patients can increase the VBVF at an appropriate level on the nonmoving hemiparetic side with the help of the active, healthy limb, after learning the exercises, independently, several times a day (χ2 = 300.0, P < .001, Friedman test using Bonferroni correction; Figure 3). The VBFV of the consensual effect in the hemiparetic side was significantly higher (Z = −3.7, P < .001, Wilcoxon signed rank test) at the first minute, than the VBFV in the hemiparetic side, measured at the first minute following passive movement.
Discussion
In the course of the research, we measured the VBFV in the lower limbs of hemiparetic patients, in resting state, and following active and passive thromboprophylaxis methods. There were significant differences between the resting VBFV in the hemiparetic and healthy lower limbs. Following passive movement of the hemiparetic side, we found 474% increase in the venous blood flow of the hemiparetic lower limb; following active venous exercise, we found 257% increase in the venous blood flow of the healthy and 559% of the hemiparetic lower limb (consensual effect).
Several authors have examined the values of the VBFV in resting state and after different active and passive mechanical thromboprophylaxis. We summarized the results of major researches found in the literature (Table 3).
Values of the Venous Blood Flow Velocity Following the Treatment.
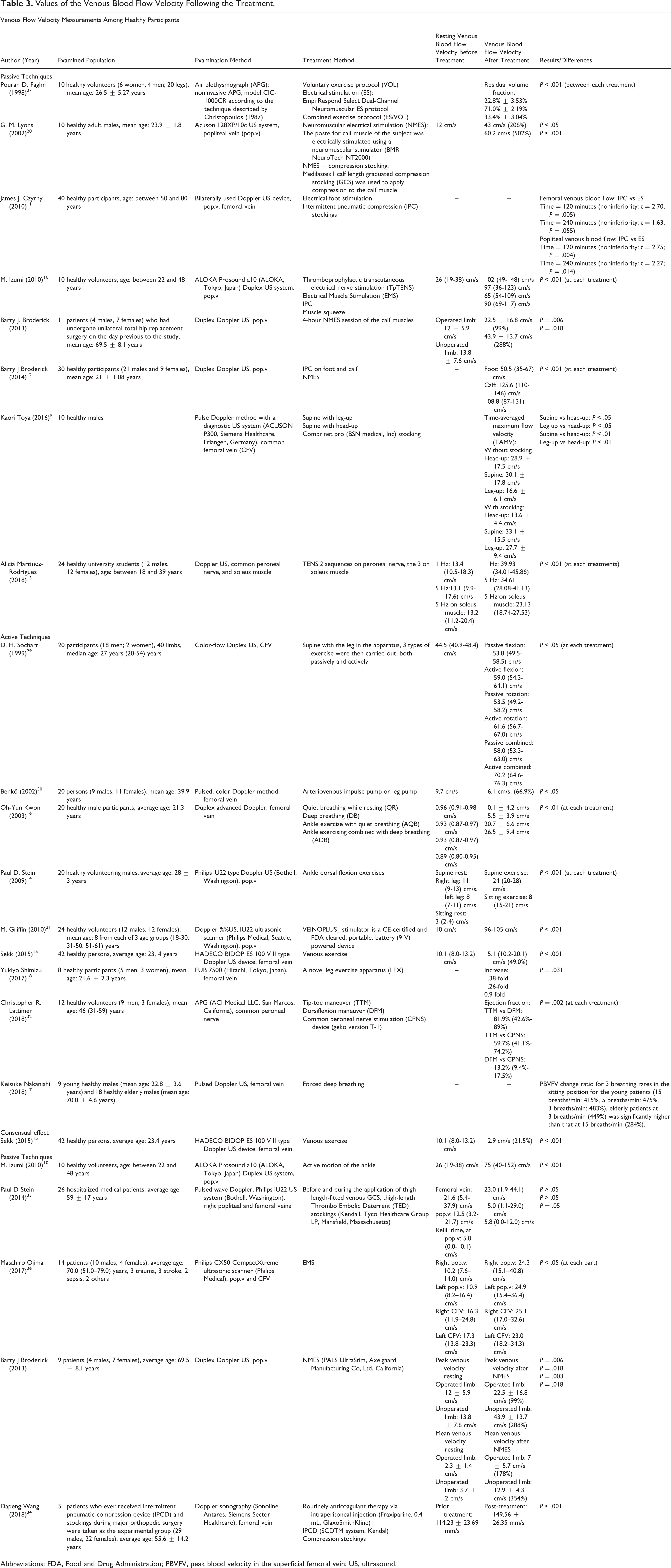
Abbreviations: FDA, Food and Drug Administration; PBVFV, peak blood velocity in the superficial femoral vein; US, ultrasound.
Although wanted to compare the findings of the study with researches connected to stroke, mechanical thromboprophylaxis, and VBFV measurement, we found only reviews that examined the effect of pharmacological or mechanical thromboprophylaxis not on the change of VBFV or gave recommendations for thromboembolism in patients with stroke. 23,24
We did not find a research that measured in both lower limbs the resting VBFV among hemiparetic patients. Broderick et al examined 30 healthy patients (21 males and 9 females, mean age: 21 ± 1.08 years). There was no significant difference in the resting venous blood flow between the operated and unoperated limb (12 ± 5.9 to 13.8 ± 7.6 cm/s, P = .68; Table 3). 25 In our study, the VBFV measured in resting state was significantly lower (2.7 [2.4-4.4] to 7.0 [6.2-7.8], P < .001) on the hemiparetic side than on the healthy side.
We did not find a research that measured the effect of passive movement on the change of VBFV among hemiparetic patients. Masahiro et al examined 14 patients (10 males, 4 females, average age: 70.0 [51.0-79.0] years). In this study, 3 had traumatologic injury, 3 had stroke, 2 had sepsis, and 2 suffered from other diseases. They used electrical muscle stimulation to increase VBFV. At each leg and vein (popliteal vein, common femoral vein), they found a significant increase (P < .05) in the VBFV due to electrical muscle stimulation as passive mechanical thromboprophylaxis (Table 3). 26 In our research following passive movement on the hemiparetic side, the VBFV significantly increased (2.7 [2.4-4.4] to 12.6 [11.6-13.5] cm/s, P < .001) compared to the values received in resting state.
Kwon et al reported that as a result of active exercises (breathing exercises and active plantar–dorsal flexion ankle joint movements), a significant increase (P < .01) was experienced in the VBVF (0.89 [0.80-0.95] to 26.5 ± 9.4 cm/s) among 20 healthy adult men (mean age: 21.3 years; Table 3). 15 In our study, we did not examine the efficiency of various breathing exercises on the velocity of venous flow; however, breathing exercises are included in the venous exercise program, which we also applied. 16 Following active venous exercises performed on the healthy side, the VBFV in the healthy lower limb significantly increased (7.0 [6.2-7.8] to 18.0 [15.6-19.6] cm/s, P < .001) compared to the resting VBFV measured in the healthy lower limb.
Sekk et al determined the efficiency of venous exercise in relation to the VBFV. Forty-two healthy persons (13 males, 31 females, mean age: 23.4 [20-30] years) participated in the study. They concluded that the venous exercise performed by the lower limb significantly increased (10.1 [8.0-13.2] to 12.9 cm/s, P < .001) the VBFV on the opposite side compared to the resting VBFV (Table 3). 15 In accordance with our survey, following active venous exercise on the healthy side, the VBFV significantly increased (2.7 [2.4-4.4] to 15.1 [14.1-16.5], P < .001) compared to the values received in resting state.
Limitations of the Study
The limitations of our examinations include the low item number. We did not have the possibility to examine the cross section and saturation of the vein in addition to the examination of the VBFV. We did not differentiate subgroups according to muscle strength. We have examined VBFV in the first 15 minutes after the intervention, which have not been examined for longer.
Conclusions
Besides active venous exercise, the passive movement and the consensual effect increase significantly the VBFV. The consensual effect has significant increase in the VBFV in the paralyzed limb; thus, it can be an important element of the active mechanical thromboprophylaxis methods.
The use of active mechanical thromboprophylaxis methods can be emphasized in patient education, as the patient can apply it independently or use passive mechanical thromboprophylaxis methods with the help of the family members during the 24-hour care.
During patient education, it is important to place emphasis on the venous exercise program that is taught by professional, easy to learn, and can be performed without the lead of professional. The patient is advised to perform exercise on the healthy side several times a day, which has a VBFV increasing effect on the hemiparetic side through the consensual effect.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the GINOP 2.3.2-15-2016-00047 grant.