
Abstract
The purpose was to determine whether young women in the emergency department who received computed tomographic (CT) pulmonary angiograms were evaluated to receive lower dose imaging or no imaging, recognizing that the risks of radiation are particularly high in young women. This was a retrospective cohort investigation of women aged 18 to 29 years seen for suspected acute pulmonary embolism in emergency departments of 5 regional hospitals from May 1, 2015 to April 30, 2016. Computed tomographic (CT) pulmonary angiograms were obtained in 379 young women. Pulmonary embolism was diagnosed by CT angiography in 2.1%. A Wells probability score could be calculated in 11.9%. D-dimer was obtained in 46.2% and a chest radiograph was obtained in 41.7%. Among patients with a normal chest radiograph, 3.9% had a lung scan. Venous ultrasound of the lower extremities was obtained in 1.8%. Each had an elevated D-dimer. Among the young women who received CT angiograms, 53 were pregnant. In 17.0% of pregnant women, a Wells clinical probability score could be calculated from the medical record. D-dimer in pregnant women was obtained in 30.2%, chest radiograph in 22.6%, lung scan in 11.3%, and venous ultrasound of the lower extremities in none. In conclusion, young women and pregnant women often received CT pulmonary angiograms for suspected acute pulmonary embolism without an objective clinical assessment, measurement of D-dimer, lung scintiscan, or venous ultrasound, which may have eliminated the need for CT pulmonary angiography in many instances.
Young women are a group of patients at particularly high risk of radiation-induced cancer. 1 –3 Recommendations have been made to reduce exposure to radiation from diagnostic imaging, 3 –8 but the constraints of practice in emergency departments have limited application of such recommendations. 9 Presuming that there are risks from radiation with computed tomographic (CT) pulmonary angiography, particularly in young women, the purpose of this investigation is to determine whether young women in emergency departments who received CT pulmonary angiograms were evaluated to receive lower dose imaging or no imaging.
Methods
This was a retrospective cohort investigation of women aged 18 to 29 years seen in the emergency departments of 5 regional hospitals from May 1, 2015 to April 30, 2016 for suspected acute pulmonary embolism. Collaborating hospitals were Sparrow Hospital, Lansing, Michigan; McLaren Greater Lansing Hospital, Lansing, Michigan; St. Lawrence Hospital, Lansing, Michigan; Ionia Hospital, Ionia, Michigan; and Clinton Memorial Hospital, St. Johns, Michigan. The hospitals are all university-affiliated teaching hospitals with annual emergency department volumes between 25 000 and 100 000 visits. We searched radiology department records of consecutive imaging tests for pulmonary embolism obtained in the emergency department at each of the collaborating hospitals.
Among women aged 18 to 29 years, pregnant and nonpregnant, we determined if sufficient information was on the chart to calculate a Wells clinical probability score. We determined if a plain chest radiograph, D-dimer, ventilation-perfusion lung scan, or venous ultrasound examination of the lower extremities was obtained prior to imaging and their results. We determined from the report of the CT angiogram if pulmonary embolism was diagnosed. A Wells Clinical Score was calculated from data on the medical records according to findings on Table 1. 10 An unlikely probability of pulmonary embolism was score 0 to 4 and a likely probability was >4.
Wells Clinical Scoring System (Simplified Model). 10
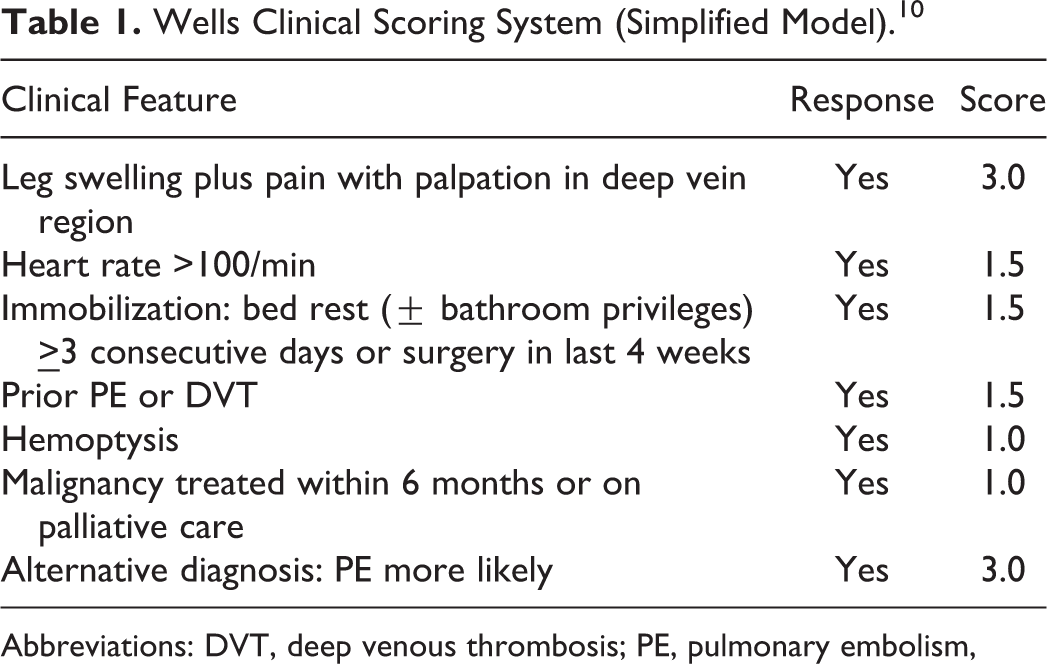
Abbreviations: DVT, deep venous thrombosis; PE, pulmonary embolism,
Among young women who received CT pulmonary angiograms, the effective dose of radiation was estimated as the product of the dose-length product and the normalized effective dose conversion factor. The dose-length product was recorded directly from the console display at the time of the scan. The normalized effective dose conversion factor of 0.017 mSv·mGy−1·cm−1 was used to determine the effective dose. 11
All data were deidentified. The investigation was approved by the institutional review boards of all participating centers.
Statistical Methods
Descriptive statistics were used. Continuous variables were expressed as means and 95% confidence intervals (CI) and were calculated using Graphpad Quickcalcs (Graphpad, San Diego, California).
Results
Computed tomographic pulmonary angiograms were obtained in 379 young women. Pulmonary embolism was diagnosed by CT angiography in 8 (2.1%) of 379 (Figure 1). The CT pulmonary angiograms were negative for pulmonary embolism in 365 patients and inadequate for interpretation in 6.
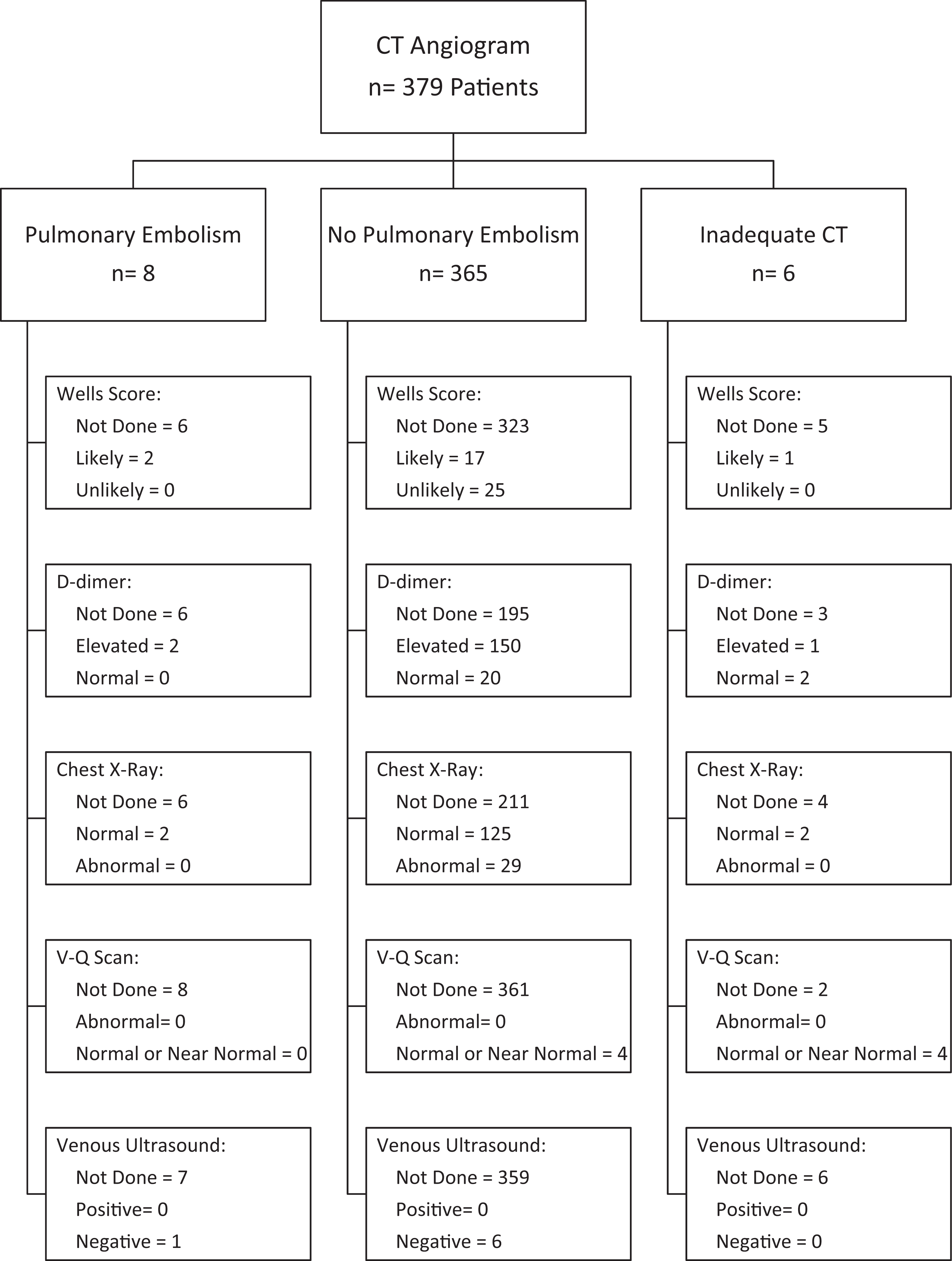
Flow diagram showing clinical evaluation and tests in all young women who underwent computed tomographic (CT) pulmonary angiography. V-Q, ventilation-perfusion.
All Patients
Among all 379 young women who had a CT pulmonary angiogram, a Wells probability score could be calculated from the medical records in 45 (11.9%). In most of those in whom a Wells score could be calculated, 25 (55.6%) of 45, the probability score indicated pulmonary embolism was “unlikely.”
D-dimer was obtained in 175 (46.2%) women. In those in whom it was measured, D-dimer was elevated in 153 (87.4%) of 175. Both D-dimer and Wells score were obtained in 15 (4.0%). D-dimer was normal and Wells score “unlikely” in 2 (13.3%) of 15. A chest radiograph was obtained in 158 (41.7%). Among those who had a chest radiograph, it was normal in 129 (81.6%) of 158. Among patients with a normal chest radiograph, 5 (3.9%) of 129 had a lung scan. A ventilation-perfusion lung scan was obtained in 8 (2.1%), and it was normal or nearly normal in all. In 4 patients, a lung scan was obtained because the CT angiogram was inadequate for interpretation. Venous ultrasound of the lower extremities was obtained 7 (1.8%). Each had an elevated D-dimer. The ultrasound was negative in each.
Patients With No Pulmonary Embolism
Among 365 women whose CT angiogram showed no pulmonary embolism, a Wells score could be calculated from information on the medical records in 42 (11.5%; Figure 1). In those in whom it was measured, the Wells score indicated that pulmonary embolism was unlikely in 25 (59.5%) of 42.
A D-dimer in women with no pulmonary embolism was measured in 170 (46.6%). The D-dimer in those in whom it was measured was normal in 20 (11.8%) of 170. Both D-dimer and Wells score were obtainable in 15 (4.0%). D-dimer was normal and Wells score probability “unlikely” in 2 (13.3%) of 15. A chest radiograph was obtained in 154 (42.2%). It was normal in 125 (81.2%) of 154. A ventilation-perfusion lung scan was obtained in 4 (1.1%). All were normal or nearly normal. A venous ultrasound was obtained in 6 (16.4%). It was normal in all. In those who had an elevated D-dimer, a venous ultrasound was obtained in 6 (4.0%) of 150. Each was normal.
Patients With Pulmonary Embolism
Pulmonary embolism was shown on the CT angiogram in 8 patients. Results of the Wells score, D-dimer, chest radiograph, lung scan, and venous ultrasound are shown in Figure 1.
Multiple CT Angiograms
More than 1 CT pulmonary angiogram was obtained in 19 (5.0%) of 379 patients during the year of analysis. Among 8 patients in whom the index CT angiogram was positive, 1 patient had 2 follow-up CT angiograms and both remained positive. Among 365 patients with a negative index CT angiogram, 14 patients had 1 follow-up CT angiogram, 1 patient had 2 follow-up angiograms, 1 had 3 follow-up angiograms, and 1 had 4 follow-up angiograms. Among 6 patients with an inadequate CT angiogram, 1 had a follow-up CT angiogram.
Pregnant Women
Among the young women who received CT angiograms, 53 were pregnant (Figure 2). None showed pulmonary embolism. In 49, the CT angiogram was negative for pulmonary embolism, and in 4 the CT angiogram was inadequate for interpretation.
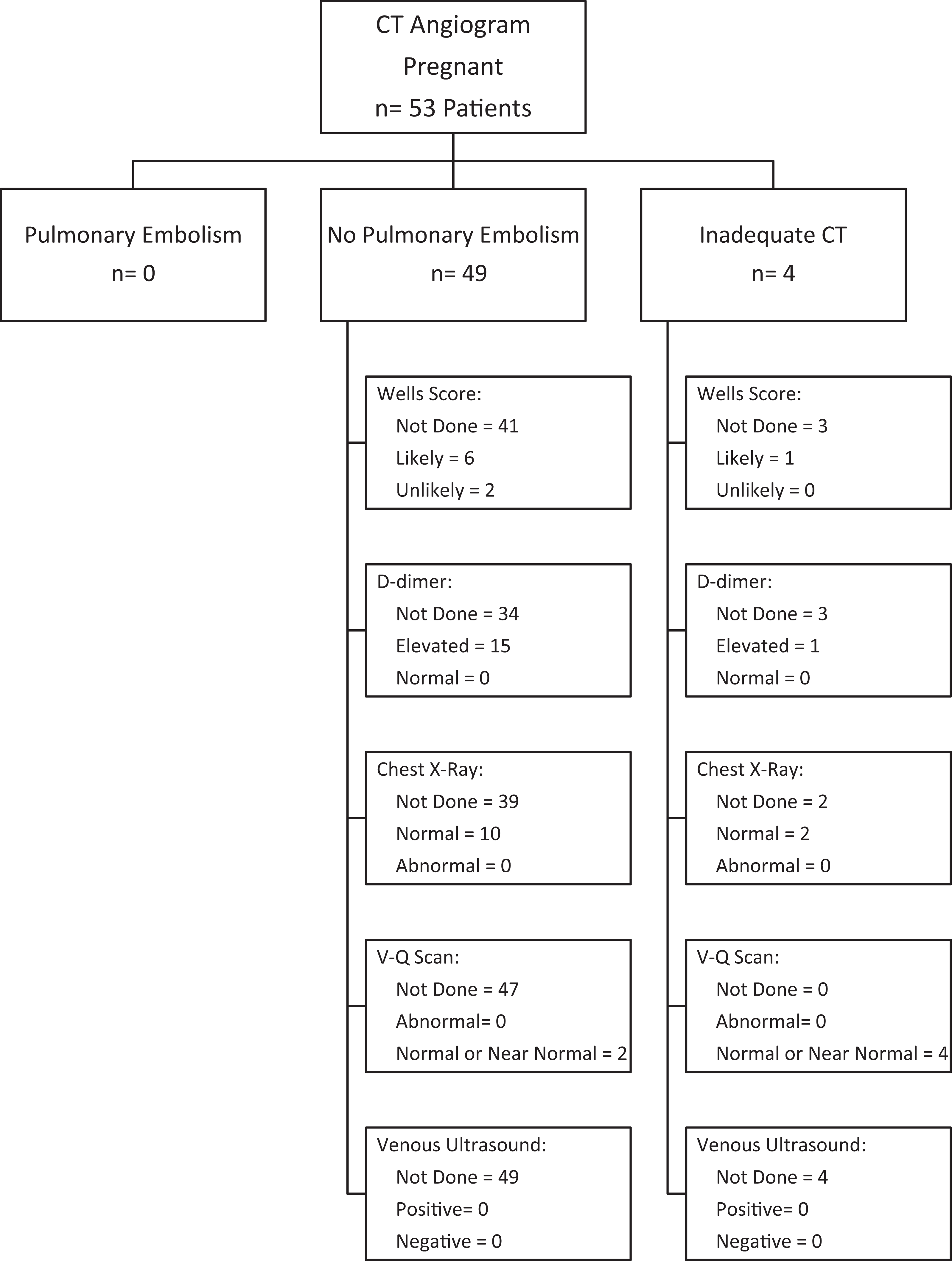
Flow diagram showing clinical evaluation and tests in pregnant women who underwent computed tomographic (CT) pulmonary angiography. V-Q, ventilation-perfusion.
A Wells clinical probability score could be calculated from the medical record in 9 (17.0%) of 53. The Wells score indicated an “unlikely” probability of pulmonary embolism in 2 (22.2%) of 9. D-dimer was obtained in 16 (30.2%) of 53. Both D-dimer and Wells score were obtained in 1. That patient did not have a negative D-dimer and Wells score indicating an unlikely probability. A chest radiograph was obtained in 12 (22.6%) of 53. All were normal. A lung scan was obtained in 6 (11.3%) of 53. In 4 of these patients, the lung scan was obtained because the CT scan was inadequate for interpretation. Venous ultrasound of the lower extremities was not obtained in any of the pregnant women.
Estimated Radiation
The mean dose-length product of CT pulmonary angiograms was 683.2 (95% CI: 633.0-733.4). Based on this, the estimated effective dose of radiation in those who received a CT pulmonary angiogram was 11.6 mSv (95% CI: 10.8-12.5 mSv).
Discussion
Among young women who received a CT pulmonary angiogram for suspected acute pulmonary embolism, the vast majority was negative. A Wells probability score could be calculated from the clinical information on the medical record in only a small proportion, and less than half received a D-dimer or chest radiograph. A lung scan was rarely obtained although the chest radiograph, when obtained, was usually normal. Among pregnant women, most did not receive a clinical probability assessment, D-dimer, chest radiograph, lung scan, or venous ultrasound.
In our investigation, the diagnostic yield was only 2.1%. The diagnostic yield of CT pulmonary angiograms is low in patients with a low or unlikely clinical probability of pulmonary embolism. 12,13 Most of our patients, however, did not have an objective assessment of clinical probability. Others showed a diagnostic yield of 4.2% among emergency department patients with an unlikely clinical probability. 13 Strikingly, we showed that even those at the highest risk of radiation-induced cancer, young women including pregnant women, had a low diagnostic yield.
Assessment of pretest probability has been recommended as an essential step before ordering a CT pulmonary angiogram.3-7,14 If clinical assessment is “unlikely” or low probability a D-dimer is recommended,3–7 unless the patient meets all Pulmonary Embolism Rule-out Criteria, 15 in which case imaging (and treatment) are unnecessary. 14 If clinical assessment indicates a low or unlikely probability and D-dimer is negative, no treatment is considered necessary. 3 –6 With a D-dimer rapid enzyme-linked immunosorbent assay (ELISA) in combination with an unlikely probability by the Wells criteria, 10 pulmonary embolism at 3-month follow-up occurred in 0.4%. 16
In women of reproductive age, if D-dimer measured by ELISA is positive, optional steps to avoid CT pulmonary angiography are venous ultrasound (treat if positive) and pulmonary scintigraphy. 3,4 Venous ultrasound detected deep venous thrombosis in 29% to 58% of patients with diagnosed pulmonary embolism. 17,18
In pregnant patients, D-dimer testing may be useful even though it may be positive due to pregnancy. 4,19
Some, however, recommend not to make use of D-dimer tests or clinical decision rules in pregnant women until this approach has been proven safe in this group. 20 Venous ultrasound in pregnant patients is recommended before imaging tests with ionizing radiation. 3,4
The American Thoracic Society/Society of Thoracic Radiology recommended chest radiography as the first radiation–associated procedure in pregnant patients, and use of lung scintigraphy as the preferred test in the setting of a normal chest radiograph. 8 In patients who do not have complex lung disease, which is the case with most young women, a perfusion lung scan alone may diagnose or exclude pulmonary embolism. 21 The dose of 99mTc-macro aggregated albumin for a perfusion lung scan in the Prospective Investigation of Pulmonary Embolism Diagnosis II (PIOPED II) was 4 mCi (148 MBq). 22 The effective dose of 99mTc-macro aggregated albumin is 0.011 mSv/MBq. 23,24 The effective dose of a perfusion lung scan after administration of 148 MBq of 99m-Tc macro aggregated albumin would, therefore, be 1.6 mSv. The effective dose that we estimate from the dose-length product in women with a CT angiogram was 11.6 mSv. A perfusion lung scan, therefore, would have resulted in about 13.8% of the radiation delivered by CT pulmonary angiography in these young women.
To bring the radiation exposure into perspective, the effective dose with a chest posterior–anterior in combination with a lateral radiograph is 0.07 mSv. 25 Therefore, the radiation dose these women received with CT pulmonary angiograms was comparable to 166 posterior–anterior and lateral chest radiographs.
The risk of inducing a fatal malignancy in a 30-year-old man by exposure to radiation is estimated to be 5 cases for each 100 000 individuals exposed to an effective dose of 1 mSv. 26 With an effective dose of 11.6 mSV, for example, the nominal cancer fatality risk in a 30-year-old man would be 5.8/10 000 patients. Estimates of the risk of radiation-induced cancer associated with 64-slice CT coronary angiography showed that a 20–year-old woman had approximately 4.7 times the risk of cancer with a single CT coronary angiogram than a 30-year-old man. 2 Assuming the relative risks are the same with CT pulmonary angiography as with CT coronary angiography, the risk of radiation-induced cancer in young women who underwent an 11.6 mSv CT scan would be 27.3/10 000 or approximately 0.3%. However, the linear no-threshold hypothesis, upon which an imaging-related low-dose (<100 mGy) risk of cancer is based, has been questioned. 27
A strength of this investigation is that it is the first of which we are aware that assesses diagnostic evaluations received and radiation from CT pulmonary angiography in young women and pregnant women. The investigation calls attention to the possibility that young women and pregnant women could undergo alternative diagnostic evaluations more frequently. A weakness, as with all retrospective investigations, is that some information may not be available.
In conclusion, young women and pregnant women, patients who have the highest risk of radiation-induced cancer, usually received CT pulmonary angiograms for suspected acute pulmonary embolism without an objective clinical assessment, measurement of D-dimer, lung scintiscan, or venous ultrasound, which may have eliminated the need for CT pulmonary angiography in many instances.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.