
Abstract
Recurrent spontaneous abortion (RSA) is defined as 3 or more consecutive pregnancy failures. Thrombin-activatable fibrinolysis inhibitor (TAFI) is a plasma zymogen that regulates both fibrinolysis and inflammation. The TAFI 1040C/T polymorphism could alter the circulating levels of TAFI with a reduced capacity to remove the fibrin clots from the circulation; therefore, it could be considered a molecular risk factor for RSA. The TAFI 1040C/T polymorphism was studied in 50 patients with RSA by polymerase chain reaction–restriction fragment length polymorphism technique and compared to 50 age- and gender-matched healthy volunteers as a control group to verify its possible association with RSA. In case group, the wild genotype (C/C) and heterozygous genotype (C/T) did not reduce the risk of RSA (odds ratio: 0.368 and 0.767, respectively), even when compared to the number of RSA (P = .71). A higher frequency of C allele in the control group and a higher frequency of T allele in the case group were observed but with no statistical significance. In conclusion, our study revealed that TAFI 1040C/T could not be considered a molecular predictive factor for RSA in Egyptians.
Introduction
Recurrent spontaneous abortion (RSA) is a common health problem affecting 1% to 2% with 3 or more losses and up to 5% with 2 or more losses in women at the reproductive age. 1 Polymorphisms in maternal hemostatic system can lead to several serious pregnancy complications including RSA. However, there is much less clear data on the possible relation with any of factors involved in the regulation of the fibrinolysis. 2
The role of factors involved in the regulation of the fibrinolysis, or some of these factors, is potentially important because it has been shown that the fibrinolytic system participates in the regulation of early human trophoblastic invasion. 3
Thrombin-activatable fibrinolysis inhibitor (TAFI), also known as procarboxypeptidase U, is a human plasma zymogen that defines a novel pathway linking coagulation to fibrinolysis. It is a single-chain plasma protein of 401 amino acids and is synthesized in the liver. Cleavage of TAFI by thrombin, thrombin–thrombomodulin complex, and plasmin at Arg 92 results in activated TAFI (TAFIa). The TAFIa, in turn, acts by removing carboxy-terminal lysine residues from partially degraded fibrin, therefore preventing the linkage of fibrin to both plasminogen and tissue plasminogen activator and reducing the production of plasmin leading finally to attenuation of fibrinolysis. 4
Regulation of circulating TAFI levels is complex, and it is still not elucidated how the changes in maternal TAFI levels influence pregnancy or vice versa. Maternal circulating levels of TAFI have been reported to progressively increase during pregnancy with peak in third trimester, especially in complicated pregnancy, and then return to normal level within 24 hours postpartum. 5 The TAFI antigen is an integral component of cord blood, as it has been detected at relatively high levels in cord blood at birth. 6
Several single-nucleotide polymorphisms (SNPs) of the TAFI gene have been identified. Plasma TAFI levels or function has been related to these polymorphisms. The genotype, 1040C/T SNP, which results in the conversion of threonine codon (ACU) to an isoleucine codon (AUU) at position 325 (Thr325Ile) is of particular interest since it is associated with increased antifibrinolytic activity. 7,8
Although the pathophysiological role of TAFI in downregulation of fibrinolysis 9 and its role in inflammation 10 point to its possible role in RSA, the published data about TAFI 1040 C/T polymorphism in complicated pregnancies, including RSA, are limited and inconsistent. Moreover, it did not confer its possible association with RAS. 4,11 Considering the different genetic backgrounds of each population, this study aimed to highlight the role of TAFI 1040 C/T genetic polymorphism as a molecular risk factor for early recurrent RSA in a cohort of Egyptian females.
Patients and Methods
Study Population
This case control study included 100 Egyptian women. The participants were stratified into 2 groups. Group I included 50 unrelated RSA cases. Their ages ranged between 18 and 40 years with a mean age of 28.86 ± 4.58 years. All of them had 3 or more recurrent abortions before 20th week of gestation with the same partner during their marital life. Group II included 50 age-matched Egyptian healthy women, with negative consanguinity to any of the patients; they had no history of spontaneous abortion or complicated pregnancy as a control group.
All candidates were referred from the outpatient clinic of the Department of Obstetrics and Gynecology, Kasr Al-Ainy Hospital, Cairo University. An informed consent was obtained from all participants and approvals from the scientific and ethical committees at the Department of Clinical and Chemical Pathology were obtained.
All patients underwent a standard diagnostic workup including—pedigree analysis with detailed medical, obstetric, and family history, serum progesterone, follicular stimulating hormone and luteinizing hormone, antibody level for Toxoplasma, rubella, cytomegalovirus, herpes simplex virus (TORCH), anticardiolipin (IgM and IgG), lupus anticoagulant, thrombophilia panel assays for protein C, protein S, antithrombin III, thrombophilic gene mutations—factor V [G1691A Leiden], factor II prothrombin [G20210 A], methylene tetrahydrofolate reductase [MTHFR C677T], paternal and maternal karyotyping, and abdominal and pelvic ultrasound. Any candidate with any abnormality in any of the above investigations was excluded from our study.
Genotyping of the Candidate Gene
From each patient and control, 3 to 5 mL of venous blood was collected on EDTA and stored at −20°C until DNA extraction using Gene JET Genomic DNA purification kit (Fermentas-Lithuania). For TAFI 1040C/T gene polymorphism study, the following primers were used 11 :
Forward primer: 5′-GCT TTG TTC AGC ATT GTC ATA G-3′. Reverse primer: 5′-CAA TTG TGA TTG CCA TAA AGT G-3′ (Fermentas-Lithuania).
Polymerase chain reaction (PCR) thermal cycling conditions included 4 minutes of denaturation at 94°C, then 35 cycles of the following: 94°C for 30 seconds, annealing at 63°C for 30 seconds, extension at 72°C for 1 minute. Then, the reaction was kept at 72°C for 10 minutes for final extension. The PCR product was subjected to digestion with SpeI (Fermentas-Lithuania). The PCR product and the digested product were separated by electrophoresis on 2% agarose gel and stained with ethidium bromide. The wild-type allele (C-allele) was identified by the presence of 2 fragments of 236 bp and 217 bp fragments, whereas the polymorphic allele (T-allele) contains no restriction site leading to a preserved 453 bp fragment. Genotyping of 25 randomly chosen samples was repeated to ensure quality control. Samples were interpreted blindly by 2 different observers, and the results were 100% concordant.
Statistical Methods
Statistical analyses were carried out using SPSS software version 13.0 for Windows (SPSS Inc, Chicago, Illinois). Deviations of genotype distributions from Hardy–Weinberg equilibrium were assessed by χ2 test for each cohort. Data were displayed as mean with standard deviation. Kruskal-Wallis test was used in comparison with number miscarriages within each genotype. The prevalence of 1040C/T polymorphism in patient and controls was compared by the use of Fisher exact test. χ2 test was used for comparison of genotype and allelic frequencies. Odds ratio (OR) and 95% confidence interval (CI) were calculated. P < .05 was considered statistically significant.
Results
The main characteristics of the studied group were summarized in Table 1. In this study, we found that genotypes of TAFI 1040C/T polymorphism showed no statistically significant differences between the study and the control group with P > .05 (Table 2). In order to assess whether the 1040C/T polymorphism could contribute to RSA, we calculated ORs as indicators of risk. T/T genotype was used as a reference, considering that expression of protein resulting from T/T genotype has extended the half-life and increased antifibrinolytic activity.
Main Characteristics of the Studied Patients.
Abbreviation: SD, standard deviation.
Genotype and Allelic Frequencies of TAFI 1040C/T Polymorphism Among Studied Patients.
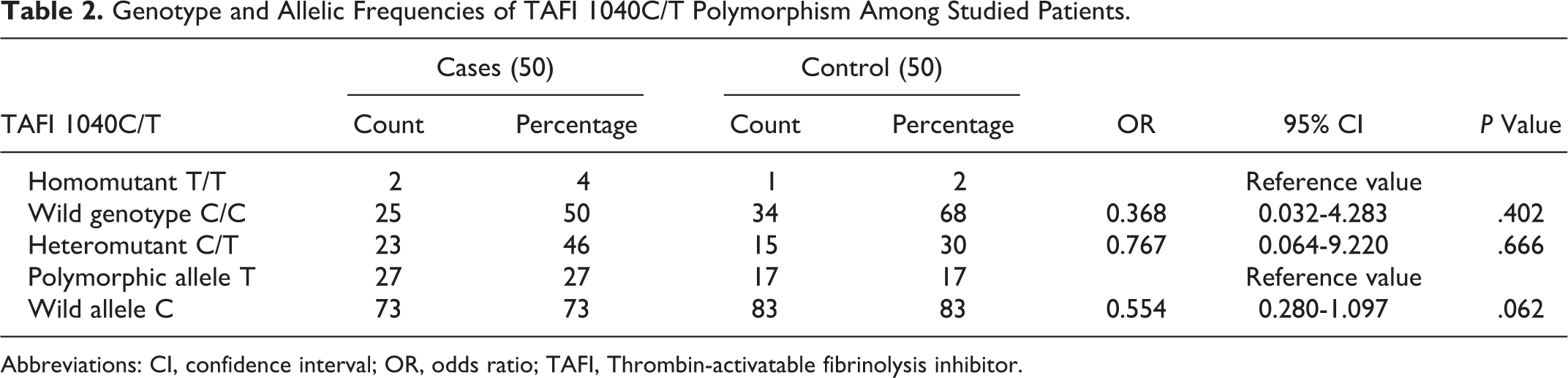
Abbreviations: CI, confidence interval; OR, odds ratio; TAFI, Thrombin-activatable fibrinolysis inhibitor.
We also observed a higher frequency of C allele in the control group and a higher frequency of T allele in the case group, but results were not statistically significant (OR: 0.554; 95% CI: 0.280-1097; P = .062). There was no statistically significant difference between mean number of miscarriages and TAFI 1040CT polymorphic types in studied patients with P = .710.
Discussion
High level of TAFI antigen, observed during hypofibrinolysis, might be advantageous during pregnancy, especially during the first few weeks. 12,13 Hypofibrinolysis can also be advantageous because it might be associated with lower levels of fibrin degradation products that have shown to induce apoptosis of placental trophoblast cells. 14
Due to the variability in the level of TAFI Ag during the course of pregnancy, 5 in our current study, a permanent and precise gene polymorphism TAFI 1040 C/T polymorphism was investigated, which is considered a molecular risk factor for RSA among Egyptian females.
The observed frequencies of genotypes resulting from TAFI 1040 C/T gene polymorphism showed slight increase in the wild and heteromutant genotypes (C/C and C/T) in addition to the C allele among the control group than in patient group who had a slight increase in the homomutant genotype (T/T) and T allele. However, this distribution was statistically insignificant with a P > .05.
Up to our knowledge, Masini et al 4 and Pruner et al 11 were the only ones who investigated the possible association of TAFI 1040C/T with RSA; however, there was no statistical association found. Pruner et al 11 concluded that carriers of T/T genotype have an increased risk of fetal loss by 1.23-fold, compared with carriers of C/C and 1.34-fold compared with carriers of C/T genotype. Their results assumed that 1040C allele acts protectively against fetal loss and that the women who are carriers of C/C and C/T genotype had a reduced risk of recurrent fetal loss, thus suggesting a possible association between TAFI 1040C/T polymorphism and RSA.
However, in the current study, we could not conclude such a verbal conclusion even after trying to stratify the number of RSA with the 1040C/T polymorphic types. It is worth mentioning that the study design of Masini et al, 4 differed from this study, as they defined recurrent pregnancy loss as 2 or more consecutive abortions while this study included patients with 3 or more consecutive abortions. In addition, their study population of women with RSA was heterogeneous since it included women with definite, possible, or doubtful causes of RSA together with women with unexplained RSA while our exclusion criteria were stricter, where infections, karyotype abnormalities, thrombophilias, gynecological, and endocrinological disorders were ruled out.
Our results, of insignificant TAFI polymorphism among RSA, could be explained by the fact that the Ile-325(T/T) variant is associated with lower TAFI Ag levels, which is compensated by extending the half-life of the activated form (TAFIa) and increasing its antifibrinolytic activity by 60%, trying to reach the same function done by normal TAFI Ag level of the wild type, with a net result of equilibrium between the different polymorphisms. 12
As pregnancy is a well-known state of hypercoagulability, it can be put under the umbrella of increased risk of venous thrombosis. 15 Two recent meta-analysis 16,17 concluded that T/T genotype of TAFI 1040 C/T polymorphism was associated with a decreased risk of venous thrombosis, and 1 C allele carrier (CC and CT) of 1040C/T gave rise to the development of venous thrombotic diseases. 16 It is possible that if the antifibrinolytic ability of TAFI was increased by suppressing plasminogen activation which is secondary to the genetic polymorphism, the dynamic balance between clot intension and lysis could be shifted toward intension and therefore thrombosis.
Furthermore, the role of the TAFI Ag level in RSA rather than TAFI polymorphism is uncertain, as Legnani et al 18 and Folkeringa et al 19 reported that the risk of RSA was significantly lower in women with high TAFI Ag levels. In a subsequent analysis of the same population, Knol et al 20 suggested that high TAFI levels may even protect against early RSA. More recently, Eser et al 12 did not indicate any change in the level of TAFI in women with recurrent miscarriage and did not support the role for altered TAFI levels in such women.
Moreover, TAFI inhibits inflammation in vivo by inactivating the inflammatory mediators; bradykinin and the anaphylatoxins C3a and C5a. 21 As the inflammatory processes play an important role in the development of RSA, it is possible that the high TAFI levels decrease the risk of RSA by decreasing the inflammatory response. 22 Indeed, there are studies that have shown that high TAFI levels are associated with a lower risk of myocardial infarction, ascribed to the anti-inflammatory properties of TAFI. 23
It is necessary to clarify that the role of TAFI, whether on antigen or molecular levels, in normal as well as in complicated pregnancy can be no more than uncertain. In fact, current knowledge on TAFI in pregnancy is still too scant to allow firm associations.
Footnotes
Authors’ Note
Informed consent was obtained from all individual participants included in the study. All procedures performed in studies involving human participants were in accordance with the ethical standards of the ethical committee of Department of Clinical Pathology, Faculty of Medicine, Cairo University and with the Declaration of Helsinki 1964 and its later amendments or comparable ethical standards.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Department of Clinical Pathology, Faculty of Medicine, Cairo University.