
Abstract
Time in therapeutic range (TTR) of international normalized ratio is crucial for the safety and efficacy of anticoagulation with warfarin and it is influenced by many factors. There are limited data about the quality of warfarin therapy and its effects on clinical outcomes in Turkey. The aim of this study is to demonstrate the quality of anticoagulant therapy with warfarin and evaluate the parameters that affect the quality of warfarin therapy. A total of 170 patients with atrial fibrillation (AF; mean age: 62.2 ± 13.3; 69.2% female) treated with warfarin were included in this study. The mean follow-up period was 20 ± 8.4 months. The mean TTR levels of all patients were found to be 54.2% ± 21.4%. The TTR levels were similar in patients with valvular AF (VAF) and nonvalvular AF (NVAF). Logistic regression analysis revealed that elderly, heart failure (HF), and renal dysfunction were independent predictors of lower TTR. There were no significant differences between the VAF and NVAF subgroups regarding the incidence of mortality, stroke, and myocardial infarction. Cox regression analysis revealed that HF, coronary artery disease, and renal dysfunction were independent predictors of clinical outcomes in addition to lower TTR. Our results provide data regarding the quality of anticoagulation with warfarin from a single tertiary center in Istanbul, Turkey. The questions remain in seeking quality improvement in anticoagulation.
Introduction
Atrial fibrillation (AF) is the most common arrhythmia in clinical practice with an increased prevalence in older adults. 1 The vitamin K antagonist warfarin greatly reduces the risk of stroke and is the most commonly used therapy to prevent stroke and stroke recurrence in patients with AF. 2 Because of its variable dose–response relationship and narrow therapeutic window, warfarin requires frequent monitoring of its anticoagulant effect, as reflected by the international normalized ratio (INR). A lower percentage of the time in therapeutic range (TTR) has been shown to correlate with stroke, major hemorrhage, and mortality. 3 The TTR, which is a measure used to describe the quality of INR control in clinical practice, associates with improved patient outcomes. 3 –6 Several observational studies and registries conducted on AF populations report that approximately half of the time, patients with AF are not within the therapeutic range of warfarin. 6 Lower TTR values have been displayed consistently throughout different countries in real-life patients compared to those participating in randomized controlled trials. 7
To date, only a few studies have examined patients’ TTR in clinical practices in Turkey. 8 –10 Most tertiary hospitals in Turkey do not have anticoagulation clinics and trained personal which hinder the adequate follow-up of patients on chronic anticoagulation. The aims of this study are to observe the clinical characteristics of patients with AF, to demonstrate the quality of anticoagulant therapy with warfarin in a tertiary care university hospital in an urban setting, and to evaluate the parameters that affect the quality of warfarin therapy and clinical outcomes.
Materials and Methods
Study Population and Design
The investigation conforms with the principles outlined in the Declaration of Helsinki. The study was approved by the local ethics committee. All participants gave written informed consent.
A total of 198 eligible consecutive patients with AF who had been under continuous warfarin therapy (n = 164 [82.8%]) and who were scheduled to receive continuous warfarin therapy (n = 34 [17.2%]) in the time interval between January 2014 and July 2016 constituted our study population. We restricted exclusion criteria to achieve a cohort close to real life. Only patients who did not give their informed consent and those with malignancy were excluded from the study. Patients with cancer are followed by the oncology clinic for vitamin K antagonist adjustment in our institution, and warfarin treatment was frequently interrupted due to chemotherapy. Routine biochemical tests and complete blood count were studied, and transthoracic echocardiography was performed in all participants at the time of enrollment into the study. Follow-up was performed by a cardiologist from research team during visits for INR monitoring. Time in therapeutic range values of all patients were calculated according to the method proposed by Rosendaal et al. 11 Rosendaal linear interpolation method adds each patient’s time within the therapeutic range and divides by the total time of observation. The estimation of the TTR was based on the INR ranges that have been defined for individual patient’s needs and clinical rationales (ie, an INR 2-3 for patients with nonvalvular AF [NVAF] with an aortic prosthetic valve and an INR 2.5-3.5 for patients with valvular AF [VAF] with a mitral prosthetic valve). The INR values below or above the mentioned intervals were accepted to be outside the therapeutic range.
The following measurements were not included in the calculation of TTR—the first 7 days after treatment had started or restarted, after permanent discontinuation of warfarin, and >5 days after temporary discontinuation. Similarly, periprocedural (anticoagulation bridging) INR and/or daily INR values during hospitalization were also excluded from TTR analysis. Patient compliance was verified by regular INR tests. Seventeen (8.5%) patients who had longer than 60-day interval between 2 consecutive INR measurements were accepted to be noncompliant patients and their data were excluded from analysis. 8,12 Data of 11 (5.5%) patients could not be used due to inadequate follow-up data regarding clinical outcome. In the end, data of 170 patients were used in the final analysis. Any history of recent serious event as major and minor bleeding, stroke and systemic embolism, myocardial infarction (MI), hospitalization, and death was recorded on case control form in each visit for INR monitoring. The combined clinical outcome of the study was defined as all-cause mortality, stroke, MI, and major bleeding. The data for long-term mortality were obtained from the hospital records, telephone contact with relatives of the patients, and a social health organization.
Definitions
Valvular AF was defined as a patient who had mitral stenosis or a history of prosthetic valve replacement, and the other forms of AF were classified as NVAF. Stroke was defined as a sudden onset of a focal neurologic deficit in a location consistent with the territory of a major cerebral artery. An event matching this definition but lasting less than 24 hours was considered a transient ischemic attack. Intracranial hemorrhage consisted of a hemorrhagic stroke and a subdural or subarachnoid hemorrhage. Systemic embolism was defined as an abrupt vascular insufficiency associated with clinical or radiological evidence of arterial occlusion in the absence of another likely mechanism. Major bleeding was defined as a reduction in the hemoglobin level of at least 2 g/dL, a transfusion of at least 2 units of blood, or symptomatic bleeding in a critical area or organ. All other bleeding were considered minor. A TTR of <55% was defined as lower TTR. 12,13 Renal dysfunction was defined as glomerular filtration rate, which was calculated with the method of Modification of Diet in Renal Disease Study equation <60 mL/dk. Elderly patients were defined as patients older than 75 years.
Statistical Analysis
All statistical tests were performed with a commercially available statistical analysis program (SPSS version 20.0 for Windows; IBM Corporation Software Group, New York). Continuous variables were expressed as mean (standard deviation) if they were normally distributed or as median (quartiles) if they were not normally distributed. Categorical variables were expressed in ratio. The distribution of data was assessed using a 1-sample Kolmogorov-Smirnov test. A Mann-Whitney U test was used to compare continuous variables, whereas a χ2 test was used for the comparison of categorical variables. Logistic regression analyses were used to assess comorbidities and those clinical characteristics that affect lower TTR. Cox proportional hazards modeling was used to evaluate the relationships for clinical outcomes. A receiver-operating characteristic (ROC) curve analysis was performed to determine the cutoff value of TTR to predict switching warfarin therapy with a novel oral anticoagulant (NOAC) drug. P values <.05 were interpreted as statistically significant.
Results
Data of 170 patients with AF were used in the analysis. The mean follow-up period was 20 ± 8.4 months. The mean age of study participants was 63.5 ± 14 years, and 109 (64.1%) of the patients were female. Seventy-six (43.6%) patients presented with VAF, whereas 94 (56.4%) patients presented with NVAF. The clinical characteristics of the study population based on the VAF and NVAF subgroups are shown in Table 1. The mean TTR levels of all patients were found to be 54.2 ± 21.4 (median, 57%). The TTR levels were similar in patients with VAF and NVAF. Warfarin of 25 patients with NVAF was exchanged for NOAC during the follow-up period. These patients had a significantly lower TTR compared to patients who continued warfarin therapy (TTR: 45.8% vs 56.8%; P = .02). The ROC analysis revealed that a 56.3% or lower TTR predicted the need to switch warfarin with NOAC; this analysis had a sensitivity of 55% and specificity of 72% (Figure 1). There were no significant differences between the VAF and NVAF subgroups according to all-cause mortality, stroke, and MI incidence, whereas major and minor bleeding incidence were higher in the VAF subgroup although difference failed to reach statistical significance at a border value (Table 2). Heart failure (HF) and renal dysfunction were significantly more prevalent in patients with a lower TTR, and these patients were more likely to be elderly when compared to patients with a high TTR. A logistic regression analysis was performed to explore the predictors of lower TTR in our cohort. Elderly, HF, and renal dysfunction were independent predictors of lower TTR in our study (Table 3).
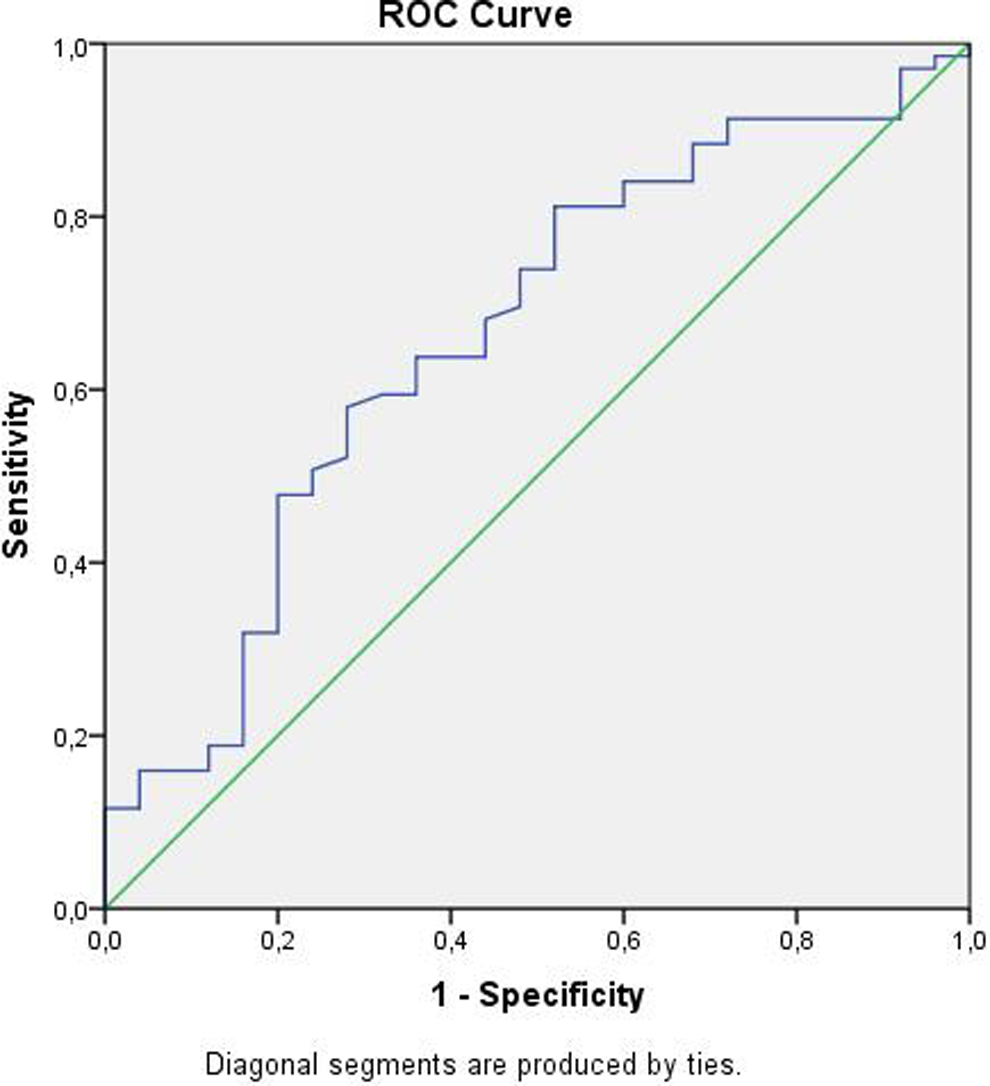
Receiver-operating characteristic (ROC) analysis revealed that a 56.3% or lower time in therapeutic range (TTR) predicted the need to switch warfarin with novel oral anticoagulant (NOAC); this analysis had a sensitivity of 55% and specificity of 72%.
Clinical and Demographical Features of Patients.
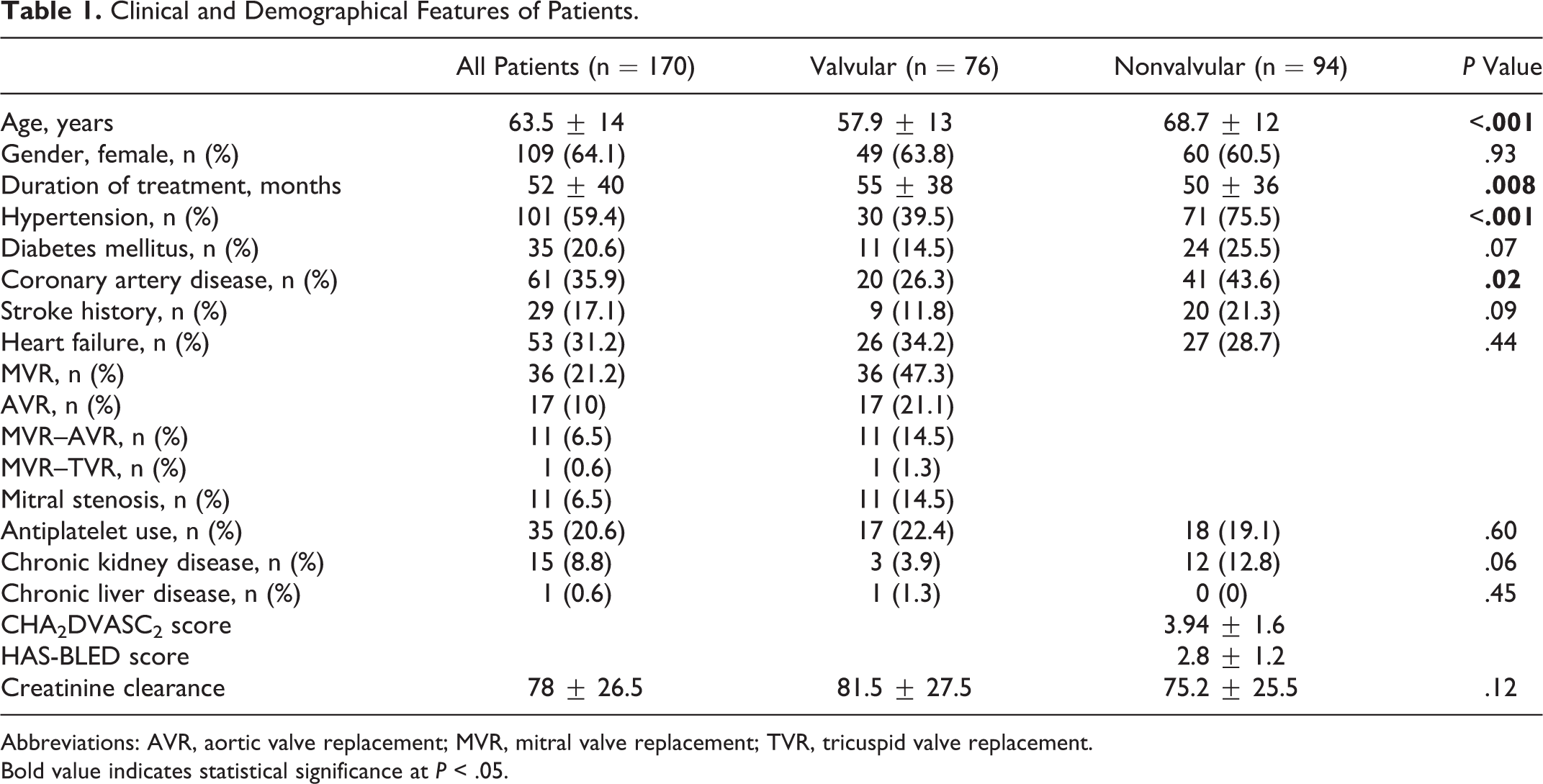
Abbreviations: AVR, aortic valve replacement; MVR, mitral valve replacement; TVR, tricuspid valve replacement. Bold value indicates statistical significance at P < .05.
Clinical Outcomes During Follow-Up.
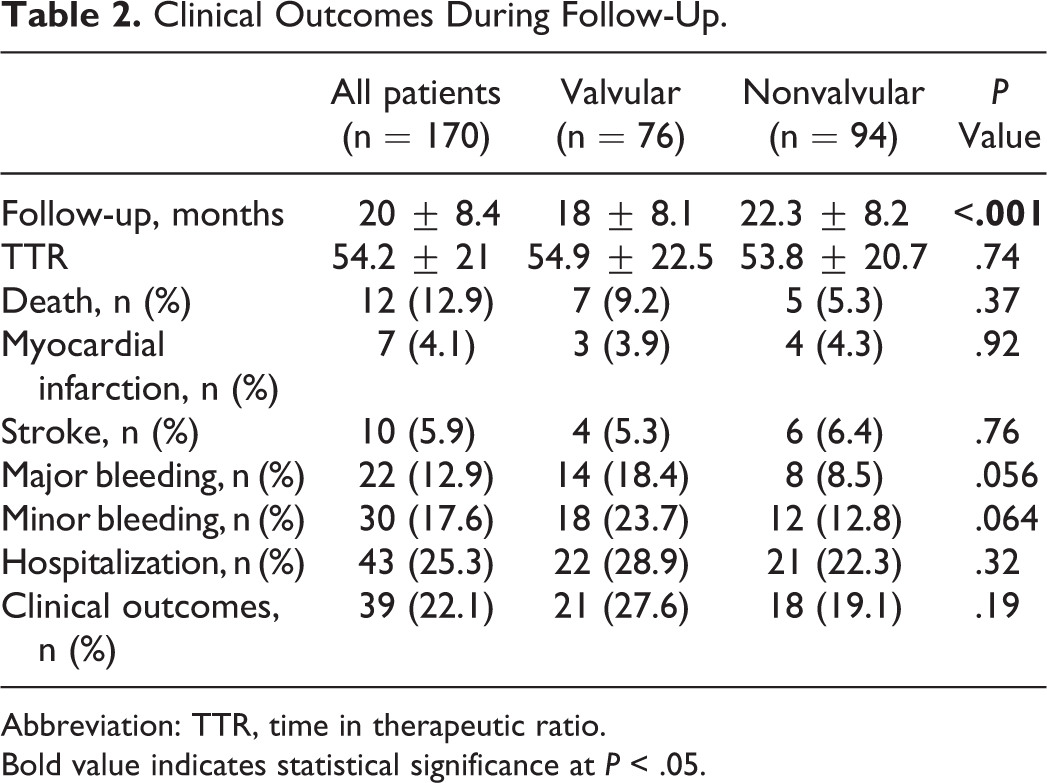
Abbreviation: TTR, time in therapeutic ratio.
Bold value indicates statistical significance at P < .05.
Logistic Regression Analysis Showing the Predictors of Lower TTR.
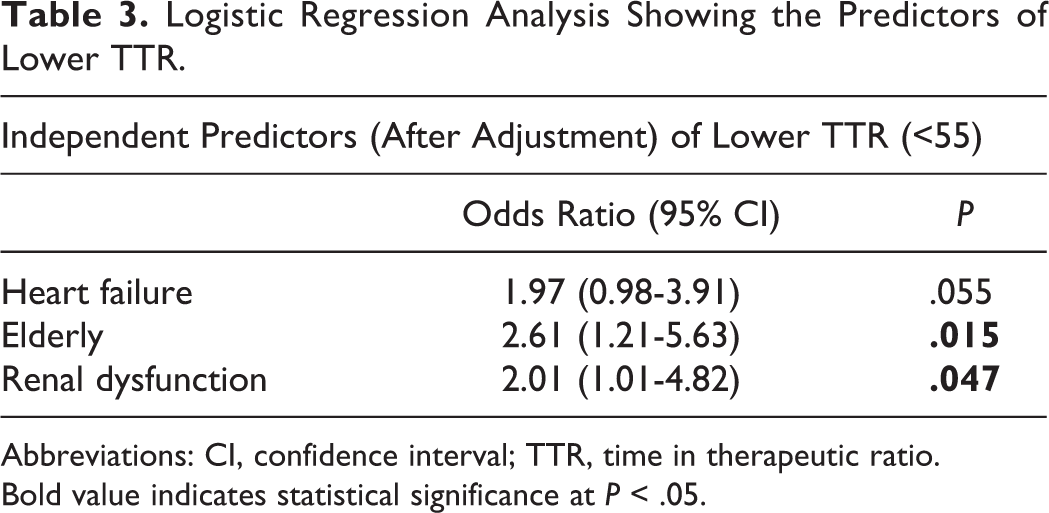
Abbreviations: CI, confidence interval; TTR, time in therapeutic ratio.
Bold value indicates statistical significance at P < .05.
When clinical outcomes were examined, 12 (7%) patients were deceased, and a combined clinical outcome occurred in 39 (22%) patients during follow-up. In addition to a lower TTR, HF, renal dysfunction, and coronary artery disease (CAD) were significantly more prevalent in patients in which a combined clinical outcome occurred. After the adjustment, a Cox regression analysis revealed that a lower TTR, HF, CAD, and renal dysfunction were independent predictors of a combined clinical outcome (Table 4).
COX Regression Analysis Showing the Predictors of Clinical Outcomes During Follow-Up Periods in All Study Population.
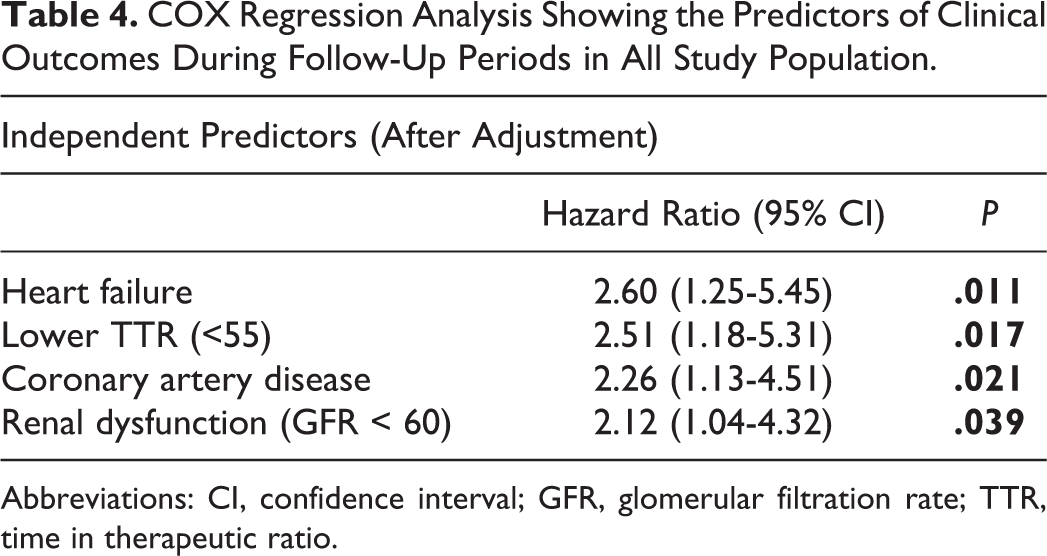
Abbreviations: CI, confidence interval; GFR, glomerular filtration rate; TTR, time in therapeutic ratio.
Discussion
In the present study from a large inner city university hospital, we found a median TTR value of 57% in patients with AF who received warfarin. Thus, the quality of anticoagulation appeared to be suboptimal. Approximately half of the patients in our population (43%) had VAF. There was no significant difference in TTR values between the VAF and NVAF groups. Comorbidities such as HF and renal dysfunction were associated with poor anticoagulation control and adverse clinical outcome.
Our study is not the first to report suboptimal TTR from Turkey. Turk et al 8 reported a median TTR value of 40% in their multicenter study conducted in Turkey, and patients with VAF had higher TTR values compared to the NVAF subgroup. The cause of higher median TTR value in our study might be related to progressively increased usage of NOACs in patients with NVAF and poor INR control. Moreover, the growing awareness of the risks of anticoagulant therapy in Turkey might also be a contributing factor for an increase in the quality of warfarin therapy. Although TTR is routinely suggested for assessment of anticoagulation quality in patients treated with warfarin, there is a lack of a consensus on an acceptable TTR level. For the purpose of our analysis, we use the cutoff point for TTR 55% as defined by Nelson et al 12 and Baker et al. 13
Patients with HF, renal dysfunction, and elderly were more likely to have a lower TTR. Previous studies have demonstrated that comorbidities and the patient characteristics that affect the quality of warfarin therapy may vary among countries. 14 –16 In a study from Unites States, Nelson et al 12 reported that HF, diabetes mellitus, and previous stroke were associated with a lower TTR in patients with NVAF, yet age did not associate with poor anticoagulation control. However, in the AF in Turkey: Epidemiologic registry, age was found to be the only independent factor of stroke in patients with NVAF 15 and VAF. 10 They also reported that only 37% of patients with NVAF and 36.1% of patients with VAF had a therapeutic INR in the Turkey. Melamed et al 16 found that HF and having a nonboard-certified physician to be independent predictors of poor anticoagulation control in Israel. Contrary to Nelson et al, the current study and Melamed et al also displayed that the old-age was associated with poor anticoagulation control. It remains uncertain whether poor social infrastructure or decline in cognitive function lead to deterioration in treatment compliance in elderly patients in developing countries. In developed countries, access to advanced health services can improve the quality of anticoagulation.
Heart failure was an important factor that affected the quality of warfarin therapy. It is known that chronic diseases such as HF and renal dysfunction come with polypharmacy and affect the pharmacodynamics of the warfarin and drug interactions lead to a reduced quality of warfarin therapy.
In addition to a suboptimal TTR, the prevalence of major bleeding in our study was higher than in previous studies. We believe that this might be due to the relatively high rate of mitral valve replacement in patients who need relatively higher target INR level compared to other patients. A high HAS-BLED score in our study population (the median HAS-BLED score was 3 for patients with NVAF) likely contributed to the increased frequency of bleeding. Heart failure, renal dysfunction, and CAD have been previously identified as important causes of mortality and cardiovascular morbidity in patients with AF. 17,18 In Rivaroxaban Once Daily Oral Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation (ROCKET AF) study, population, Pokorney et al 19 reported that the majority of classified deaths were cardiovascular, whereas only 6% were due to a nonhemorrhagic stroke or systemic embolism. They demonstrated that traditional cardiovascular risk factors such as HF, pulmonary and renal comorbidities, age greater than 75 years, male sex, and peripheral artery disease were associated with mortality in patients with NVAF. In our study, we confirmed that HF, CAD, and renal dysfunction were associated with all-cause mortality and combined clinical outcome. According to our findings, HF and renal dysfunction both impair the quality of warfarin therapy and increase the prevalence of the combined clinical outcome.
Several studies indicate that a large room exists for improvement in the practice of anticoagulation for the prevention of stroke in AF in general practice. 20 The questions remain in seeking quality improvement in anticoagulation. Quality improvement interventions to achieve satisfactory TTR at a cardiology clinic have a hierarchy for sustainability. Patient education and assessment of psychometric properties can help to improve TTR. 21 There is profusion of patient education materials to answer patient centeredness and readability. However, educational tools, such as online modules, conferences, pocket cards, and signs, tend to have a positive initial effect, but this effect is not lasting. Many patients with chronic diseases forget to keep their pocket cards.
We believe that employment of appropriately trained nurses in patient education might have an effect on improvement in TTR values. However, current nursing shortage problem is preventing nurses from taking an active part in patient care. We believe that in order to find effective and long-lasting solutions we need to overcome the low TTR, evidence-based recommendations should be used in nursing management. Strengthening primary health care is equally and critically important for efficient and responsive follow-up of patients with chronic complex disease such as those on chronic anticoagulation. 22,23 Although an institutional consensus or policy may improve adherence to the protocols, it is difficult to implement and develop consistent adherence. In case of low TTR in an institution, the order set may likely provide a sustained improvement. Such order sets along with patient-related variables (ie, HAS-BLED and CHA2DS2-VASc scores) can be integrated into a computerized order entry system. 24 –30
Study Limitations
Our study is a single tertiary care center study and comes with several limitations including small sample size and short follow-up period. We cannot claim that our study represents the global patient population in a chronic condition such as AF. A growing challenge concerns the interpretation of health system errors that can at least partially explain the observed differences in other studies. Anticoagulation provider continuity has profound effects on TTR for patients treated with warfarin. 31 Several center- and country-specific factors can affect the TTR. For instance, in Turkey, outpatient clinics have a tremendous patient load enabling the physician less than 5 minutes to conclude the examination. Our hospital did not have a protocol for warfarin follow-up. We also did not use any software for monitoring of anticoagulation. Lack of specialty clinics such as anticoagulation clinic, and lack of time and resources for patient education in major institutions can also affect the TTR outcome. This may be particularly detrimental for patients with coexistent comorbidities. Finally, because some of the data of our study was obtained from telephone contacts and hospital records, these data might not be precisely accurate.
Conclusion
In conclusion, low TTR was observed in a single tertiary care center experience from Istanbul, Turkey. Elderly, HF, and renal dysfunction are associated with low TTR levels. The questions remain in seeking quality improvement in anticoagulation.
Our findings are timely and crucial as NOACs are inevitable alternatives for these patients, but the high prevalence of VAF and high cost of NOACs in developing economies require extra scrutiny and limit their use. Subspecialty clinics (ie, anticoagulation), resources for patient education, and allowance of longer time for physicians to educate their patients may help developing countries to embrace cost-effective and time-proven therapeutics such as warfarin in a more effective manner.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.