
Abstract
Bleeding is the most common complication of all anticoagulants. Any bleeding patient on an anticoagulant should be risk-stratified based on hemodynamic instability, source of bleeding, and degree of blood loss. Although minor bleed may be managed with discontinuation of anticoagulant, major bleed may require transfusion of blood products and use of specific antidote. The residual effects of each anticoagulant may be monitored with distinct coagulation assay. Intravenous or oral vitamin K can reverse the effect of warfarin within 24 to 48 hours and is indicated for any bleeding, international normalized ratio of >10 or 4.5 to 10 in patients with other risk factors for bleeding. Fresh frozen plasma or prothrombin complex concentrate (PCC) may be necessary in major bleeding related to warfarin. Protamine sulfate reverses the effect of unfractionated heparin completely and of low-molecular-weight heparin (LMWH) partially. Idarucizumab has recently been approved in United States for dabigatran reversal, whereas andexanet alfa is expected to get approved in the near future for reversal of oral factor Xa inhibitors. The PCC may reverse the effect of rivaroxaban to some extent, but no data are available regarding reversal of apixaban and edoxaban. Aripazine has shown promising results to reverse the effects of LMWH, fondaparinux, and direct oral anticoagulants but is still in the developmental phase.
Introduction
Bleeding is the most common complication of all anticoagulants. Although the rate of major bleeding among long-term users of vitamin K antagonists (VKAs) is 1.5% to 5.2% per year, 1 direct oral anticoagulants (including dabigatran, rivaroxaban, and apixaban) are associated with 2% to 3% of major bleeding complications. Various trials have demonstrated that direct oral anticoagulants are actually associated with lower risks of major bleeding (relative risk [RR]: 0.72; 95% confidence interval [CI]: 0.62-0.85), fatal bleeding (RR: 0.53; 95% CI: 0.43-0.64), and intracranial bleeding (RR: 0.43; 95% CI: 0.37-0.50) than VKAs. 2 –5 Similarly, bleeding complications range from about 2% with low-molecular-weight heparin (LMWH) to 5.5% with intravenous unfractionated heparin (UFH). 6
In major and life-threatening bleeding, timely and appropriate management can reduce morbidity and potentially mortality. With an increasing number of available anticoagulants, understanding the reversal strategy of different anticoagulants in an acute setting can be challenging. Additionally, reversal agents may not be available for all anticoagulants, and the onset of action may vary considerably. Here, we provide a focused approach to anticoagulant reversal and management of patients bleeding on various anticoagulants.
General Measures
The optimal approach to management should be risk-adapted based on hemodynamic instability, source of bleeding, and degree of blood loss (Figure 1). Although a minor bleed may be managed by stopping the anticoagulant, reversal of anticoagulant and transfusion of blood products may be required in the presence of a major bleed. Transfusion of platelets and cryoprecipitate may be required to achieve platelet counts >50 000 to 100 000/µL and fibrinogen level >100 to 150 mg/dL depending on the severity and site of bleeding. In select cases, activated charcoal may be utilized if the ingestion is within 2 to 6 hours for dabigatran, apixaban, and rivaroxaban. 7,8 It is available as an oral suspension with a single dose of 50 to 100 g administered via oral or nasogastric route. Dialysis may be useful in dabigatran-associated bleed in patients with renal impairment as dabigatran binds to plasma proteins. 9
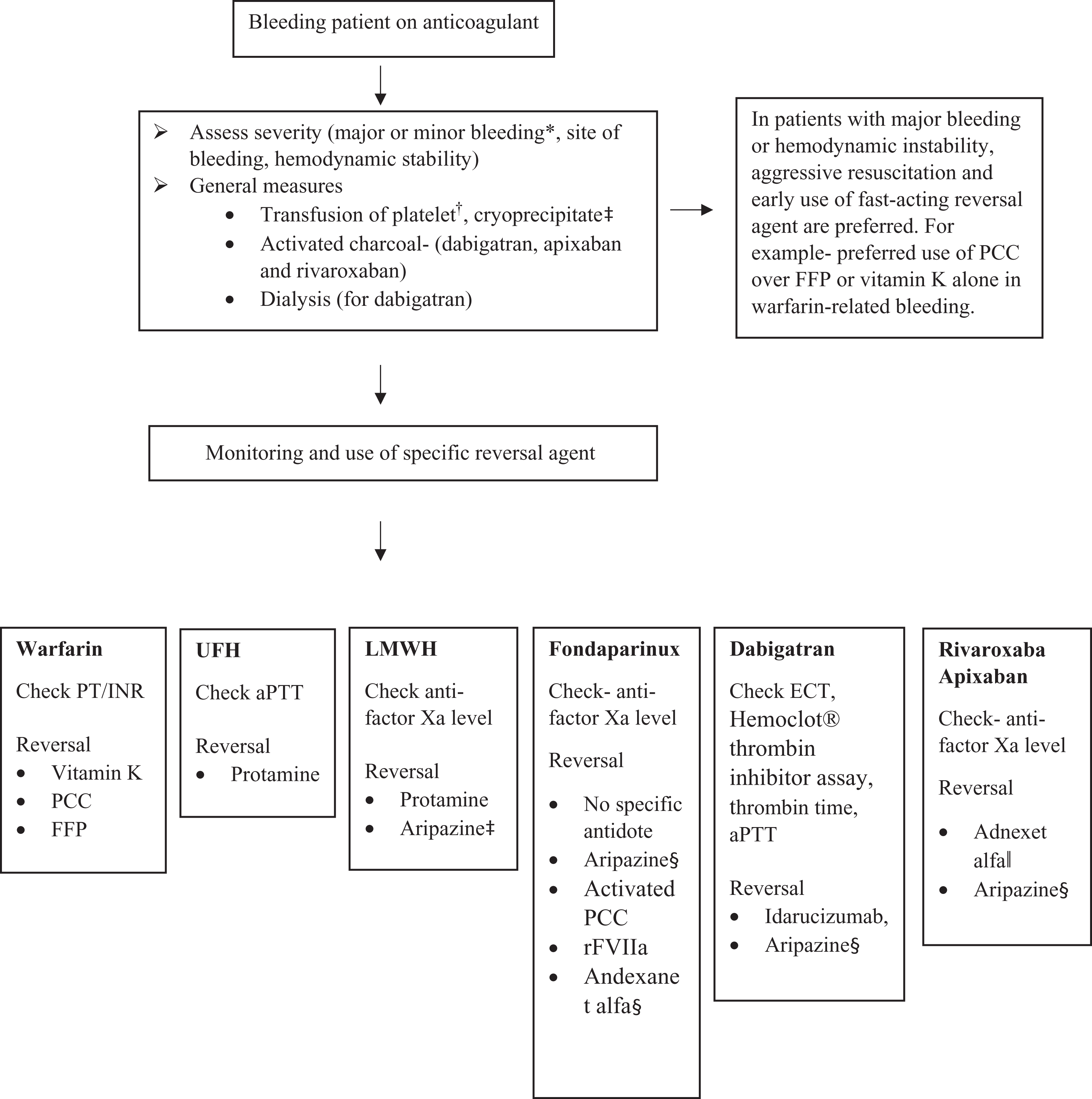
An algorithm on management of bleeding patient on anticoagulant. aPTT indicates activated partial thromboplastin time; ECT, ecarin clotting time; FFP, fresh frozen plasma; INR, international normalized ratio; LMWH, low-molecular-weight heparin; PCC, prothrombin complex concentrate; PT, prothrombin time; rFVIIa, recombinant-activated factor VIIa; UFH, unfractionated heparin. *Major bleeding is defined as fatal bleeding or symptomatic bleeding in a critical area or organ, such as intracranial, intraspinal, intraocular, retroperitoneal, intraarticular or pericardial, or intramuscular with compartment syndrome, and/or bleeding causing a fall in hemoglobin level of 20 g/L or more, or leading to transfusion of 2 units of packed red blood cells. †Etiology of bleeding and clinical manifestations guide platelet transfusion. Although actively bleeding patients are transfused to keep platelet count >50 000/μL, patients with no acute bleeding are transfused only when platelet count is <10 000/μL. Patients on anticoagulants, or those with coagulopathy or an anatomical lesion at risk of bleeding may require platelet transfusion to keep platelet count above 20 000/μL. ‡In patients with hypofibrinogenemia, cryoprecipitate may be used to keep fibrinogen level above 100 to 150 mg/dL depending on the severity of bleeding. §Aripazine is still in clinical trials. ||Andexanet alfa is not Food and Drug Administration (FDA)-approved yet.
Monitoring of Anticoagulant’s Effects
The effects of anticoagulants vary based on the time elapsed since the last dose; hence, monitoring may be valuable to assess the residual effect of anticoagulants (Table 1). Warfarin, UFH, and LMWH are accurately measured using international normalized ratio (INR), partial thromboplastin time (PTT), and anti-factor Xa level, respectively. If calibrated properly, anti-factor Xa level may be useful for monitoring the effects of other factor Xa inhibitors such as fondaparinux, rivaroxaban, and apixaban. Although Hemoclot thrombin inhibitor assay and ecarin clotting time are preferred monitoring tests for dabigatran, these tests lack exact reference values and may not be available in all centers. 10,11 Thus, in cases of emergency, thrombin time and PTT may be of some use to qualitatively monitor the effects of dabigatran. 12
Management of Bleeding Episodes Associated With Common Anticoagulants.
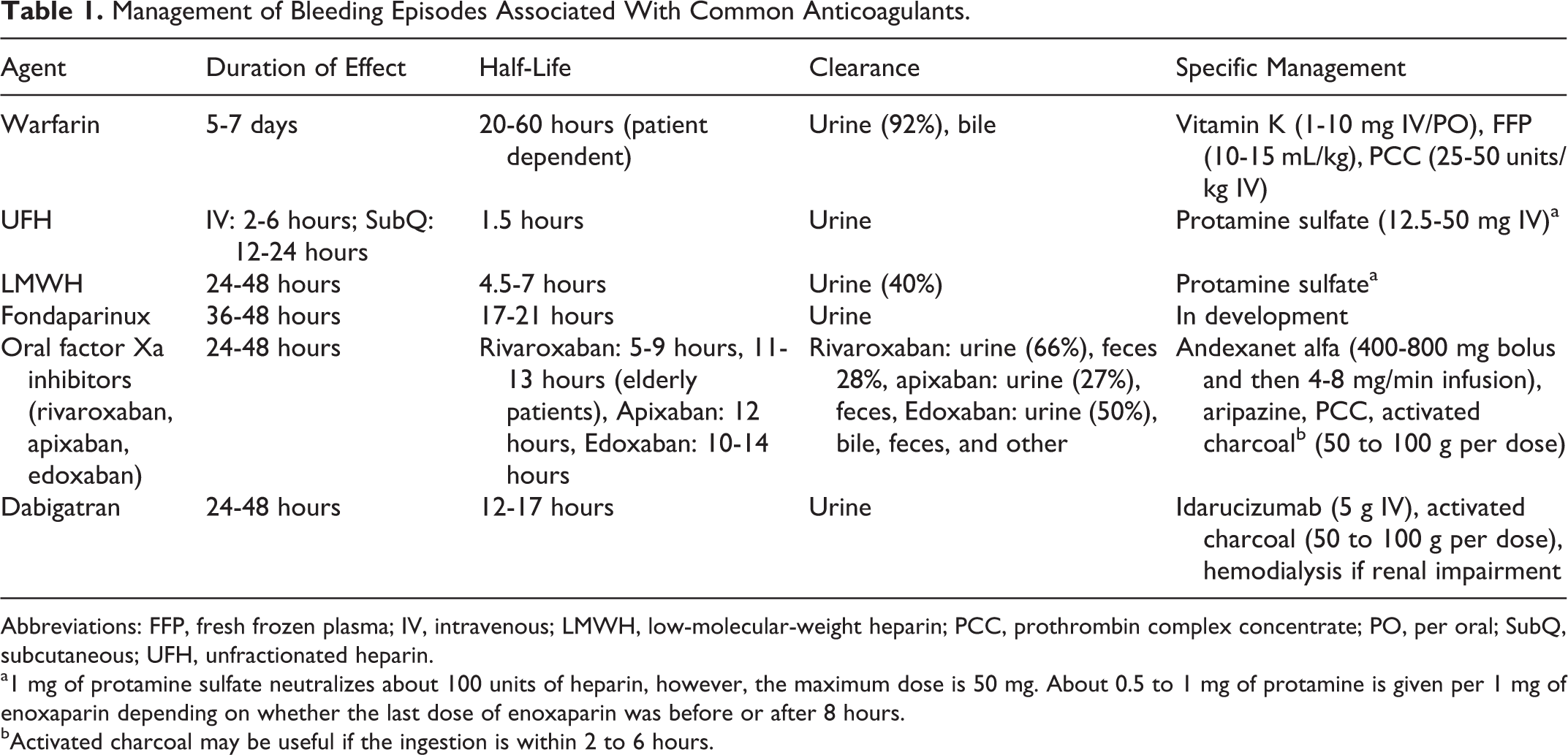
Abbreviations: FFP, fresh frozen plasma; IV, intravenous; LMWH, low-molecular-weight heparin; PCC, prothrombin complex concentrate; PO, per oral; SubQ, subcutaneous; UFH, unfractionated heparin.
a1 mg of protamine sulfate neutralizes about 100 units of heparin, however, the maximum dose is 50 mg. About 0.5 to 1 mg of protamine is given per 1 mg of enoxaparin depending on whether the last dose of enoxaparin was before or after 8 hours.
bActivated charcoal may be useful if the ingestion is within 2 to 6 hours.
Warfarin
Intravenous or oral vitamin K can reverse warfarin within 24 to 48 hours in most patients with supratherapeutic INR (Table 2). Vitamin K is indicated for warfarin reversal if a patient is bleeding or has INR of >10 or 4.5 to 10 in the presence of other risk factors for bleeding. Vitamin K alone is administered when INR is >10, and the patient does not have active bleeding or has minor bleeding. 13,14 Although 10 mg of intravenous vitamin K should be given by slow intravenous infusion in individuals with major bleeding, individuals without emergent indication may receive lower doses of oral vitamin K. Additionally, fresh frozen plasma (FFP) or prothrombin complex concentrate (PCC) may be necessary in bleeding patients. In cases of major bleeding, although PCC or FFP are given to reverse the immediate action of warfarin, vitamin K is given to maintain the reversal effect against warfarin as the half-life for warfarin is 72 hours. Vitamin K helps prevent the late bleeding complication of warfarin after the effects of PCC and FFP wear off. Patients who receive FFP for warfarin reversal should undergo repeat coagulation profile to ensure sustained warfarin reversal. Approximately, 3 to 5 units of FFP (10-15 mL/kg IV) may be required in most adults to increase plasma coagulation factors by ∼15% to 25%. 15 If required, additional doses may be used based on repeat INR testing. Although rare, transfusion of FFP is associated with a risk of HIV (1:2 million), hepatitis C virus (1:1.5 million), hepatitis B virus (1:300 000), and other infections. 16 The PCC acts by providing high levels of 3 or 4 coagulation factors, depending on the preparation, along with protein C and S, and is preferred to FFP in cases of major bleeding. 17 It is associated with smaller volume, faster infusion, and less immunologic reactions but is more expensive and less widely available than FFP. In a clinical trial that randomly assigned 216 patients with warfarin-associated bleeding to receive PCC or FFP with intravenous vitamin K, PCC was found to be at least as effective as FFP with similar hemostasis (72% vs 65%) and similar length of hospital stay (median 4.5 vs 4.2 days). 18 Mortality related to therapy was 0% in both arms, and adverse events related to study drugs were low; fluid overload was more common in patients receiving FFP. The dose of PCC ranges from 25 to 50 units/kg, depending on INR, and may be as high as 5000 units. Recombinant-activated factor VIIa (rFVIIa), used off-label for warfarin reversal, may not restore hemostasis as effectively as it corrects INR. 19
Common Agents Used for Reversal of Anticoagulants.
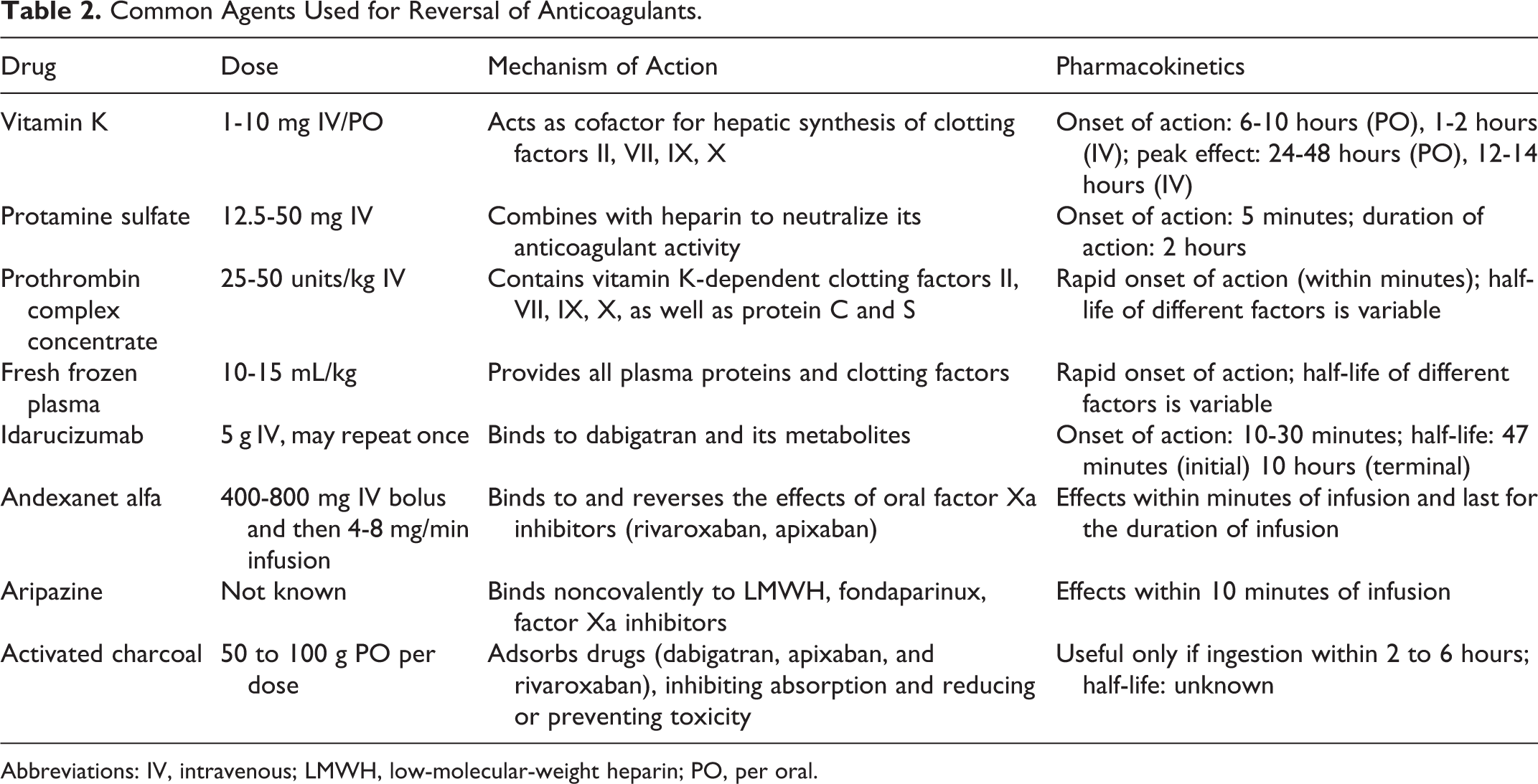
Abbreviations: IV, intravenous; LMWH, low-molecular-weight heparin; PO, per oral.
Unfractionated and LMWH
Protamine sulfate completely reverses the action of UFH but not of LMWH. Approximately, 1 mg of protamine sulfate neutralizes 100 units of heparin. Dosage varies depending on the duration since last dose and route of administration of heparin (subcutaneous or intravenous route); however, the dose is capped at a maximum of 50 mg. 20 In cases of LMWH, about 0.5 to 1 mg of protamine is given per 1 mg of enoxaparin depending on whether the last dose was after or before 8 hours, respectively. 21 A potential reversal agent for LMWH, aripazine (discussed in the following sections), is currently under development.
Fondaparinux
No specific antidote exists for fondaparinux reversal. Prohemostatic agents such as rFVIIa and activated PCC have been shown to reverse anticoagulant action of fondaparinux, although clinical data are largely limited to in vitro studies. 22 –24 In 1 study, in nonbleeding volunteers treated with fondaparinux, low doses of activated PCC was shown to be more effective than rFVIIa in normalization of thrombin generation time. 22 Andexanet alfa (described in detail in the following sections), currently being studied for reversal of oral factor Xa inhibitors, may perhaps be effective for reversing effects of fondaparinux. 25,26 Aripazine, still in clinical trial, may also be effective in reversal of fondaparinux. 20
Direct Oral Anticoagulants
Early results with reversal agents for direct oral anticoagulants are promising. Idarucizumab, a humanized monoclonal antibody fragment, binds to dabigatran and its metabolites and has been approved by Food and Drug Administration (FDA) to reverse the anticoagulant effect of dabigatran. A total of 5 g (2 separate 2.5 g doses no more than 15 minutes apart) of idarucizumab is used in emergent reversal of dabigatran. It is usually indicated in patients with life-threatening bleeding or for whom conservative measures have failed. The effectiveness of idarucizumab in dabigatran reversal was demonstrated in Reversal Effects of Idarucizumab on Active Dabigatran study, which included 90 patients with serious bleeding or the need for an urgent invasive procedure (<8 hours) while receiving dabigatran. Using dilute thrombin time and ecarin clotting time as the laboratory measures, idarucizumab was observed to completely reverse anticoagulation in over 90% of patients within the first 10 to 30 minutes of infusion. 27
Andexanet alfa is a recombinant-modified human factor Xa decoy protein, which binds to and reverses the effects of oral factor Xa inhibitors, and is expected to be FDA-approved in the near future. In ANNEXA studies (ANNEXA-A for apixaban and ANNEXA-R for rivaroxaban), 400 mg IV bolus of andexanet alfa with continuous infusion of 4 mg/min for 120 minutes was administered for apixaban, whereas 800 mg IV bolus with continuous infusion of 8 mg/min was administered for 120 minutes for rivaroxaban. The studies included 101 healthy volunteers aged 50 to 75 years. Andexanet alfa reversed the anticoagulant activity of both apixaban and rivaroxaban within minutes after its administration and for the duration of infusion, without any severe adverse events. 25 A study to evaluate the effect of andexanet alfa in bleeding patients receiving factor Xa inhibitors is ongoing (NCT02329327).
A small molecule aripazine (PER977) has been shown to bind noncovalently to anticoagulants, effectively reversing in vitro effects of LMWH, fondaparinux, factor Xa inhibitors, and dabigatran. The drug is currently undergoing a phase 2 clinical trial. 20 In a study of 80 healthy volunteers on edoxaban, aripazine normalized the whole blood clotting time within 10 minutes, compared to 12 to 15 hours with placebo. 28
The PCC, mainly used for reversal of VKA, have limited data regarding their efficacy in bleeding associated with direct oral anticoagulants. In a randomized double-blind study, PCC completely reversed the effects of rivaroxaban in 12 healthy subjects but had no influence on anticoagulant effects of dabigatran. 29 The PCC was, however, unable to stop rivaroxaban-induced bleeding in rabbits in another study. 30 Activated PCC was also shown to dramatically improve the thrombin generation effect of dabigatran in an ex vivo study, thus suggesting its effectiveness in correcting coagulopathy associated with dabigatran use. 31 There have been no reports on use of PCC for apixaban reversal.
Conclusion
Approach to a bleeding secondary to an anticoagulant use should be based on hemodynamic instability, source of bleeding, and degree of blood loss. Although a minor bleed may be managed with supportive measures and discontinuation of the drug, a major bleed may require transfusion of blood products and use of specific antidote, when feasible. Direct oral anticoagulants, compared to VKAs, are generally associated with a lower risk of bleeding. The availability of reversal agents such as idarucizumab for dabigatran and andexanet alfa for factor Xa inhibitors can further improve their safety and enhance their utilization. Vitamin K, and in emergency conditions, PCC, or FFP can be used for warfarin reversal, whereas protamine sulfate reverses the effects of heparin completely. Fondaparinux and LMWH do not have effective reversal agents; however, protamine (for LMWH) and rFVIIa or activated PCC (for fondaparinux) may have some value. Aripazine has shown promising results to reverse the effects of LMWH, fondaparinux, and direct oral anticoagulants. Confirmation of the value of this agent in future studies may provide additional option for anticoagulation reversal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Vijaya R. Bhatt is supported by the 2016-2017 Physician-Scientist Training Program Grant from the College of Medicine, University of Nebraska Medical Center.