
Abstract
Objective:
To estimate the prevalence of thrombophilia in women with recurrent miscarriages and to assess the effect of antithrombotic therapy.
Design:
A retrospective cohort study between the years 2004 and 2010.
Setting:
A hypercoagulation community clinic in northern Israel.
Patients:
Four hundred ninety pregnant women referred for thrombophilia screening.
Main Outcome Measures:
Screening results for thrombophilia and antithrombotic treatment with enoxaparin, aspirin, or both and pregnancy outcomes.
Results:
The most common thrombophilia in our study group was factor V Leiden mutation with a prevalence of 20.9% followed by protein S deficiency with a prevalence of 19%. Live birth rate was higher in the group of women who received enoxaparin regardless of whether a specific thrombophilia could be found. This finding was more pronounced in women who had ≥4 miscarriages.
Conclusion:
The prevalence of thrombophilia was higher in our study group than in the general population. Furthermore, treatment with enoxaparin might improve the rate of live births in women with or without evidence of thrombophilia, especially in women with ≥4 miscarriages.
Introduction
Recurrent miscarriages is defined as 3 early miscarriages or 2 late miscarriages and its prevalence is between 1% and 3% in reproductive-age women. 1 –3 The incidence of miscarriages in healthy women is about 15% of the pregnancies. The prevalence of recurrent miscarriages is approximately 1% to 2%. 4 The etiology can be embryonic, anatomic, or chromosomal causes or maternal disorders creating a hostile environment for the fetus as in endocrine disorders, congenital, or acquired thrombophilia. One possible cause for idiopathic recurrent pregnancy loss is that couples are producing more aneuploidy embryos. Marquard et al found that chromosome analysis could explain 80% of unexplained recurrent miscarriages in women >35 years old. 5 A large number of miscarriages remain unexplained despite comprehensive investigation. The overall prevalence of thrombophilia is 1 in 10 in the general population. 6 Recurrent miscarriages are a predictable complication in conditions of hypercoagulation. The first reports were in women with antiphospholipid syndrome (APS), of which recurrent miscarriages are a characteristic. 7 Other studies described the association between other congenital or acquired thrombophilia and recurrent miscarriages. 8 –10 Recent study showed that women with obstetric APS, who have continuing pregnancies, are at increased risk of placenta-mediated pregnancy complications. 11
Heterozygote or homozygote mutation in factor V Leiden, protein S deficiency, protein C deficiency, or anti-thrombin III were described as causes for a higher incidence of recurrent miscarriages. In a meta-analysis of 31 studies, the presence of factor V Leiden was associated with early (before gestational week 12) and late (after week 12) recurrent miscarriages. Similar results were found in women with prothrombin mutation and protein S deficiency. 12
In a study that examined the prevalence of thrombophilia in women who had recurrent miscarriages, after exclusion of other causes, the prevalence of thrombophilia was found to reach 78%. 13 A number of studies found an association between thrombophilia and other obstetric complications, that is, preeclampsia, fetal growth retardation, placental abruption and still birth, 14,15 and early or severe preeclampsia. 16
Several studies have illustrated the efficacy and improved obstetric outcomes of anticoagulants in women with recurrent miscarriages and thrombophilia. 16 –19 Women with APS were found to benefit from treatment with aspirin and heparin. Rai et al demonstrate a rise in the rate of live births from 41% with aspirin alone to 71% when combined with low-dose heparin. 8 The current common treatment for women with recurrent miscarriages and thrombophilia is low-molecular-weight heparin (LMWH; enoxaparin) at a dosage of 40 mg once daily. However, this finding cannot prove the efficacy of heparin treatment due to the lack of studies with a control group. 6
Conversely, others argue the evidence is inconclusive regarding the efficacy of anticoagulant treatment in recurrent miscarriages. They claim the chance for live births without treatment in these women reaches over 50%, while additional randomized controlled trial (RCT) studies are warranted. 20
Previously, the common approach during the retrospective cohort period was to perform thrombophilia testing in every woman with a medical history of recurrent miscarriages or 1 miscarriage after gestational week 10. If testing reveals evidence for thrombophilia, anticoagulation treatment during pregnancy should be considered.
Another unresolved issue is the therapeutic approach to women with recurrent miscarriages without evidence for thrombophilia from laboratory tests. Currently, laboratory tests can ascertain 50% of the causes for thrombophilia, whereas in the remaining 50% of patients, a measurable cause cannot be established. In light of the aforementioned controversy, in recent years, some specialists are still in favor of anticoagulant treatment in chosen cases of women without evidence of thrombophilia. A number of recently published control studies have failed to establish the benefits of anticoagulants in this group of women. 21,22
Objectives
To estimate the prevalence of thrombophilia in women referred for laboratory screening for thrombophilia as a cause for recurrent miscarriages, intrauterine growth restriction (IUGR), and intrauterine fetal death (IUFD).
To assess the success rates of pregnancies with enoxaparin treatment, aspirin, or both in women with thrombophilia.
To assess the success rates of pregnancies with enoxaparin treatment, aspirin, or both in women without thrombophilia.
Materials and Methods
The study was approved by the ethics committee of the Haemek Medical Center, Afula.
Study Population
The data regarding the study population were gathered retrospectively from the computerized data system in the Hypercoagulation Community Clinic in northern Israel between the years 2004 and 2010. Women are referred to the clinic if there is suspicion for thrombophilia as the cause for recurrent miscarriages, IUGR, and IUFD.
Data Collected
The demographic data include religion, date of birth, number of children, number of miscarriages, IUGR, and IUFD.
Test results for thrombophilia: Levels of protein S, protein C, antithrombin III, protein C resistance, lupus anticoagulant (LAC) presence, immunoglobulin G and immunoglobulin M antibodies to cardiolipin, in the women’s serum, homocysteine level, genetic testing for factor V Leiden gene mutation and prothrombin G20210A mutation.
Pregnancies following investigation.
Type of treatment each woman received.
Pregnancy outcomes: Miscarriage refers to either early or late pregnancy loss.
Inclusion/Exclusion Criteria
All women with 1 or more miscarriages, IUFD, or IUGR with a suspicion for thrombophilia as its possible cause were included in the study. Women without an investigation of the pregnancy were excluded.
Statistical Analysis
The categorical variables are presented by percentages. Comparison of categorical variables among groups was done with a χ2 test or a precise Fisher test as needed.
Two-tailed test with a P value < .05 was considered statistically significant. SPSS version 17 (Chicago, Illinois) was used for conducting the statistical analysis.
Results
The study included 490 women treated in the clinic between the years 2004 and 2010 who had thrombophilia as a possible cause for recurrent miscarriages, IUFD, or IUGR. The average age at first referral was 28.6 ± 5.4 (17-45). The distribution according to religion, the large majority were Muslim (414) followed by Christian (50) and Jewish.(26)
Thrombophilia Prevalence
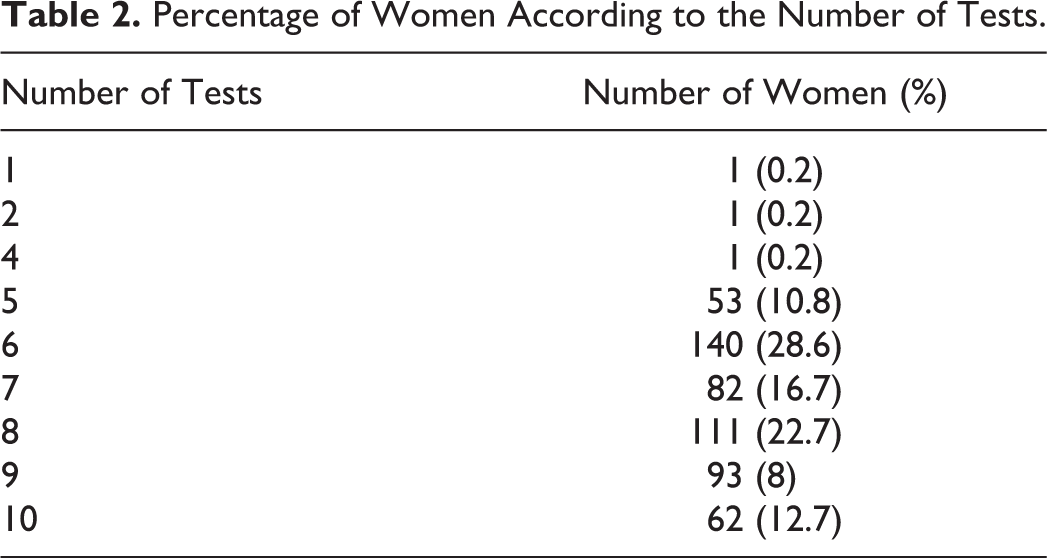
Among 490 women, 488 underwent a thrombophilia profile. All women were referred for additional tests requiring payment (not all went for testing)—PCR for factor V Leiden, prothrombin G20210A mutation, and homocysteine level. As presented in Table 1, only 181 patients went for factor V Leiden testing. Women with normal APCR ratio were not referred for this test as described below. Two hundred eleven women were tested for prothrombin G20210A mutation. Homocysteine levels were tested in 236 women. There are 2 main factors explaining the data presented in Table 1: the payment required for these tests is not included in the Ministry of Health subsidized services and they are performed in the hospital laboratory (not the clinic), requiring extra traveling. Table 2 depicts the percentage of women according to the number of tests that were performed.
Prevalence of Thrombophilia According to Type in Women Referred to the Hypercoagulation Clinic.
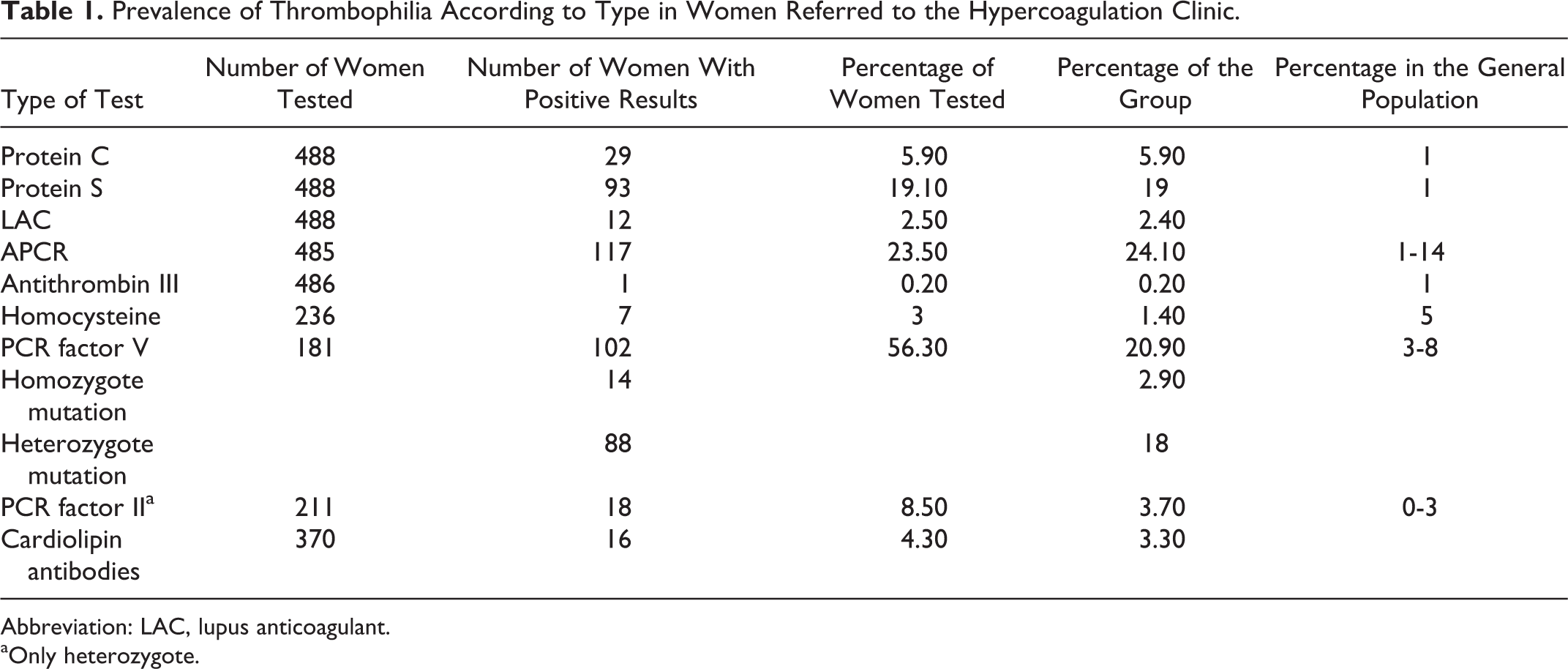
Abbreviation: LAC, lupus anticoagulant.
aOnly heterozygote.
Percentage of Women According to the Number of Tests.
Among the 488 women tested, 102 (20.9%) were found positive for factor V Leiden. Eighty-eight (18%) were heterozygote. The highest prevalence of thrombophilia was found in this mutation among the group of women tested. Table 1 demonstrates that 56.3% of the women tested for factor V Leiden gene mutation were found positive.
A low level of protein S was found in 93 (19%) of the women tested. As previously stated, all women referred and tested were included in the statistical analysis as depicted in Table 1.
Protein C deficiency was found in 29 (5.9%) women. Eighteen (3.7%) were found positive for prothrombin G20210A mutation, and 8.5% of the women screened for thrombophilia. Sixteen (3.3%) were found positive for cardiolipin antibodies, and 12 (2.5%) were found positive for anticoagulant lupus.
Of the women screened for thrombophilia, 135 (27.6%) had 1 positive test, 96 (19.6%) had 2 positive tests, and 26 (5.3%) had 3 positive tests. Cumulatively, 261 (56.3%) women were found to have thrombophilia.
Clinical Indication and Treatment
Among all women tested in the clinic, 431 were treated with anticoagulants during pregnancy, of whom 320 pregnancies presented with thrombophilia and 111 without. In 88.4% of the pregnancies, the women were treated with enoxaparin, 5.1% were treated with aspirin, and 6.5% were treated with both.
Among the pregnancies with thrombophilia, 94.1% (301 pregnancies) were treated with enoxaparin, 5.3% (17 pregnancies) were treated with enoxaparin and aspirin, and only 2 pregnancies were treated with aspirin alone. While among the pregnancies without thrombophilia, 72% (80 pregnancies) received enoxaparin, 9.9% (11 pregnancies) received combination treatment, and 18% (20 pregnancies) were treated with aspirin alone (P < .001).
Table 3 summarizes the thrombophilia distribution in all the pregnancies. Four pregnancies were without follow-up, so we were unable to determine pregnancy outcome.
Prevalence of Thrombophilia According to Type in Pregnant Women.
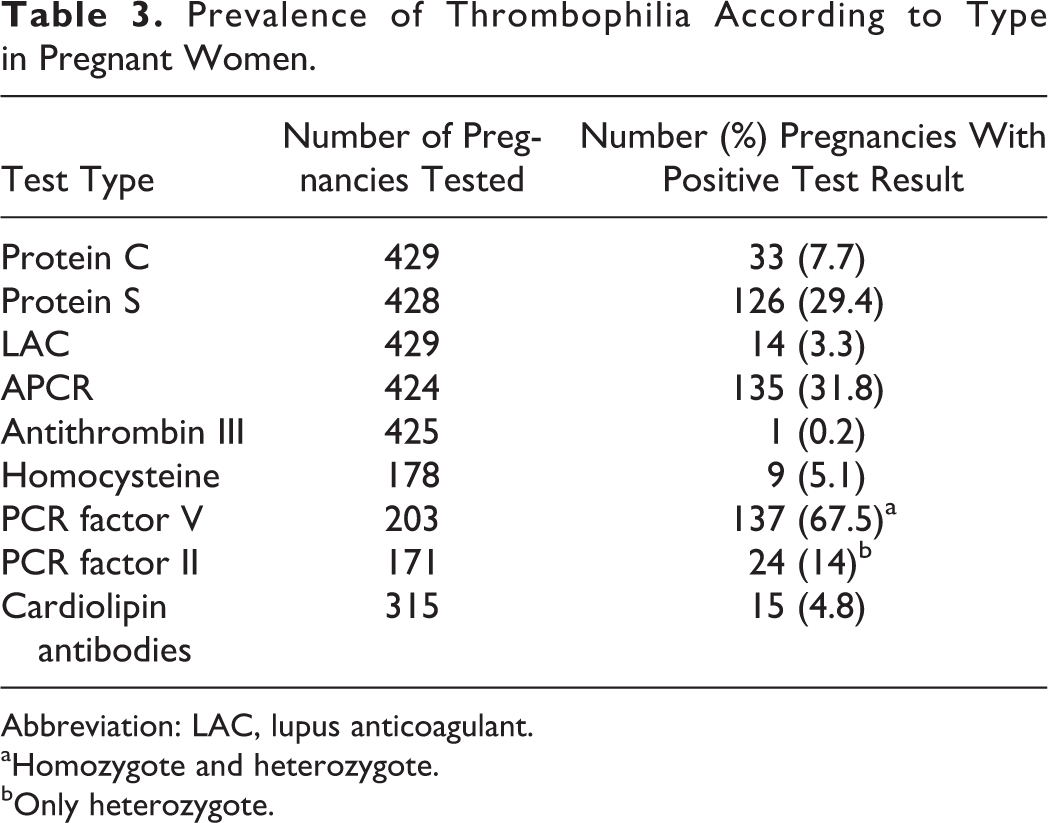
Abbreviation: LAC, lupus anticoagulant.
aHomozygote and heterozygote.
bOnly heterozygote.
Pregnancies Outcomes
Pregnancies in 70.5% of the treated women resulted in live births compared to 28.8% that ended in miscarriages. Pregnancies in 72.2% of the women treated with enoxaparin resulted in live births (regardless whether with or without thrombophilia). Pregnancies in 72.9% of women with thrombophilia treated with enoxaparin resulted in live births compared to 69.6% of the pregnancies without thrombophilia treated with enoxaparin (P = .079). Of note, 71.7% of the treated pregnancies with thrombophilia resulted in live births compared to 67.0% of the treated pregnancies without thrombophilia (P = .6).
Eighty percent of the pregnancies were treated with a dosage of 40 mg enoxaparin compared to 8.1% treated with a dosage of 60 mg enoxaparin and 6% treated with a dosage of 80 mg enoxaparin. Pregnancies of women with a history of ≤3 miscarriages resulted in live births in 74.8% versus 68.4% (P = .69) of women with and without thrombophilia, respectively.
Pregnancies of women with a history of 4 or more miscarriages resulted in live births in 55.8% versus 63.3% (P = .60) of women with and without thrombophilia, respectively. Table 4 depicts the percentages of thrombophilia in pregnancies in the study and the percentages of live births.
Percentage of Live Births in Pregnancies With Thrombophilia.
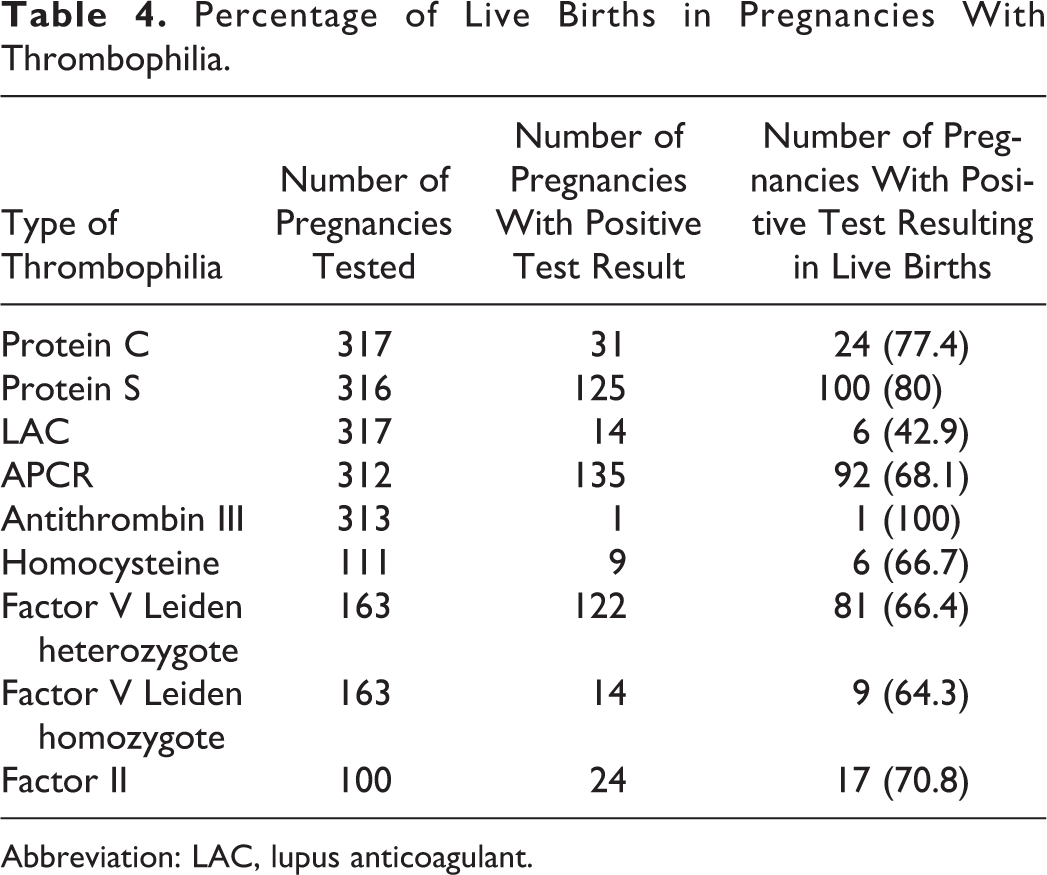
Abbreviation: LAC, lupus anticoagulant.
Discussion
According to the vast research, there are numerous causes for recurrent miscarriages. When metabolic, chromosomal, and anatomical reasons are excluded, a rise in the prevalence of thrombophilia is seen in these women concurrent with our study demonstrating an association between thrombophilia and recurrent miscarriages. In the present study, thrombophilia was found in 53.3% of the study population. The percentages vary between studies due to the differences in inclusion criteria and ethnic background. Although D’Uva et al in an Italian study found a prevalence of 78% in this group of women, 13 others found a prevalence between 49% and 65%. 10,15
The 5 basic tests included protein S, protein C, LAC, APCR, and antithrombin III, which were offered gratis to the general population. The test for antibodies to anticardiolipin was also included in the Ministry of Health subsidized services. Any additional test was paid for privately. Since the study population presented financial diversity, obviously not all women who came for testing could afford a full screening.
Two key points may have caused a bias in the results of the thrombophilia prevalence. The first was a higher prevalence due to referral of women with existing thrombophilia to the hypercoagulation clinic, while possibly women found negative for thrombophilia were not referred for continued screening. The second point, possibly a lower prevalence was found since not all women had a full screening for thrombophilia due to financial reasons or distance from the hypercoagulation clinic.
A significantly higher prevalence of thrombophilia was found in our study group in women with recurrent miscarriages compared to the general population, which is 3% to 8%. Table 1 compares the prevalence of thrombophilia according to the type in the study population as compared to the general population. Further analysis of the prevalence of each type of thrombophilia reveals interesting findings, for example, the prevalence of protein S in the study group is 19%, whereas in the general population, the prevalence is much lower (∼1%). 23 Notably, the guidelines were to perform this test when the woman was not pregnant or over 3 months since delivery or miscarriage had occurred. It appears a higher percentage in our study group of women with a low level of protein S since some of the women performed the test while pregnant or immediately following delivery or miscarriage. There were also cases the test was performed during pregnancy. In other studies, the prevalence of this type of thrombophilia was 13% (in the Italian group) 13 or between 5% and 8%. 17,25
The most prevalent thrombophilia was factor V Leiden gene mutation found in 21% of the study group, whereas the prevalence in the general population shows only between 3% and 8% and in the Arab population around 7%. Other studies have shown a prevalence of between 8% and 32%. 5 The prevalence in patients after first or second thrombotic embolism event rises to 15% and 50%, respectively. 26
The prevalence of protein C deficiency in the general population is 1% and in our study group was 5.9%, a finding similar to previous studies. 24,25,27 However, the prevalence of factor II mutation in our group is similar to that found in the general population (∼3%); while in other studies, the percentages have reached 15%. 13
Data for MTHFR mutation were originally collected. A recent meta-analysis demonstrated no association between MTHFR mutation and recurrent pregnancy in non-Chinese population. 28 Hence, our collected data for MTHFR were omitted.
No woman was found with factor II homozygote mutation and only 1 woman was found with an abnormal level of antithrombin III. Special attention must be paid to women with more than 1 thrombophilia; in our study group, 126 (25.7%) were found with more than 1 thrombophilia (Table 2).
Regarding the type of treatment the women received, the majority of women with thrombophilia received enoxaparin or a combination of enoxaparin and aspirin; in women without thrombophilia, 82% were treated with enoxaparin and 18% were treated with aspirin alone. Women without thrombophilia were given explanations regarding the types of treatment available and the research statistics to assist them in reaching an informed decision whether to choose treatment with enoxaparin or aspirin. However, there were cases in which treatment with enoxaparin was recommended, regardless of the absence of thrombophilia, given that it was considered a “precious” pregnancy.
Table 4 depicts the percentage of live births according to the type of thrombophilia. General analysis of pregnancy outcomes reveals a similar percentage of live births in both groups regardless of whether with or without evidence for thrombophilia, 71.7% and 67%, respectively. In the study by Brenner, the success of treatment with a dosage of 40 mg or 80 mg enoxaparin was around 84%. 10 In the study by Dolitsky et al, the success of treatment with enoxaparin was also 82%. 29 Our results are lower than those found in these studies. While in the study by Carp et al, the percentage of live births in women with thrombophilia treated with enoxaparin was 70%, 30 in the Anticoagulants for Living Fetuses study, the percentage was 69.1%, 19 similar to the results in our study group. 21
Recent study in the field is the NOH-APS study that included women with recurrent abortion or unexplained fetal loss; they have showed that women with nonthrombotic APLA had 69.6% live births with antithrombotic treatment. Our study showed 40% live birth success in patient with positive LAC treated with enoxaparin, which could be explained by only 60% LAC positivity in the APS group.
Another interesting finding in the NOH-APS study is 68.3% live births in women without APLA, with or without thrombophilia not receiving treatment. In comparison, our study showed 72.2% live births with enoxaparin treatment in women with or without thrombophilia (including LAC). However fair caparison is difficult since the study groups are different. 11
Examination of pregnancies according to the number of previous miscarriages reveals that in women with ≤3 previous miscarriages, the percentages of live births in women with and without thrombophilia are 74% and 68.4%, respectively. The success of a live birth in a fourth pregnancy following 3 recurrent miscarriages in the nontreated group is 60% in the general population. 31 In our group, the percentage was 63.4%. Difficulties remain attributing the rate of successful pregnancy outcomes to the treatment received.
In women with a higher number of previous miscarriages (>3), in our study, the percentages of live births in women with and without thrombophilia were 56.8% and 63.3%, respectively, whereas in the nontreated group, the percentages are lower, for example, following 5 miscarriages, the percentages are below 30%. 31
Our results are incongruous with the findings of 2 recent RCTs 21,22 that failed to show efficacy of anticoagulant treatment in this group of women. The study by Kaandorp et al unlike our study included women with thrombophilia excluding APS or with a high level of homocysteine. 21 The Scottish Pregnancy Intervention study by Clark et al also included women with thrombophilia and women with 2 or more miscarriages. 22 The pronounced results of our study demonstrate the efficacy of enoxaparin in the group of women with 4 or more miscarriages. This is a controversial issue that warrants future studies to yield conclusive evidence.
The cost-effectiveness of thrombophilia tests is questioned, since even women without evident thrombophilia would receive enoxaparin without changing the course of the treatment. One exception may be obstetric APLA.
In light of our study’s findings, it might be valid to skip testing and treat a select group of women with 4 or more miscarriages empirically with enoxaparin. There is, potentially, a much wider role for LMWH due to its ability to interact with a wide variety of proteins, selectins, cadherins, heparin-binding epidermal growth factor, and interleukin 6 that can alter the physiologic processes of implantation and trophoblast development. 30 It has been shown that LMWHs are able to promote extravillous trophoblast (EVTC) development due to their ability to stimulate the EVTC invasive properties. 32 Another observation recently reported was that LMWH exerts a cytoprotective effect by regulating trophoblast proliferation, invasion, and differentiation and that heparin-binding EGF is an important factor in the effects of LMWH on trophoblast function. 33,34 These observations may explain the biologic rationale for the use of LMWH in women without thrombophilia.
Indeed, these results can elucidate whether the possible success rate of treatment was associated with positive pregnancy outcomes in these women.
When examining the success of treatment according to the type of thrombophilia (Table 4), the highest success rates of treatment were demonstrated in women with protein C and protein S deficiencies, 77.4% (31 pregnancies) and 80% (125 pregnancies), respectively. Regarding pregnancies in women positive for factor V Leiden, the success rate of treatment is 66%, although lower compared to other types of thrombophilia examined in our study, yet similar to the rates in the general population without treatment.
Limitations
One of our study limitations was the lack of a control group; therefore, we compared our results to statistics found in other studies. In addition, the data were collected retrospectively from the clinic; therefore, each woman had a different number of tests that could have shown a bias in the results.
Conclusion
The prevalence of thrombophilia in women with recurrent miscarriages is higher than the percentage of thrombophilia in the general population. Our study results indicate that preventive treatment with enoxaparin can improve the rate of live births in women with or without evidence of thrombophilia. Statistically significant results were found in women with a high number of miscarriages (>4) in contradiction to the current common assumption that enoxaparin shows no efficacy in women without evidence for thrombophilia. However, since this is a retrospective study, we cannot be conclusive, and additional CRTs are warranted to elucidate this issue with greater accuracy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.