
Abstract
The role of anticoagulants in the prevention of pregnancy complications, including recurrent miscarriage, late fetal loss, and preeclampsia, continues to be an area of active research and debate. Although prophylactic anticoagulation with heparin and aspirin is considered the standard of care in some conditions, such as obstetric antiphospholipid antibody syndrome, the optimal management of pregnant women with factor V Leiden mutation, prothrombin G20210A mutation, and other inherited thrombophilias without a history of thrombosis remains unknown. Some studies suggest a benefit of heparins in preventing late-term losses but not earlier miscarriages in the inherited thrombophilias. In the following review, we will discuss the recent literature regarding anticoagulation and pregnancy complications and conclude with our suggested approach to the management of these challenging patients.
Keywords
Introduction
Pregnancy complications including recurrent miscarriage, late fetal loss, and preeclampsia/hemolysis, elevated liver function tests, low platelets (HELLP) syndrome have widespread psychological and economic repercussions, affecting not only women and their communities but also the health care system at large. 1 Physicians often prescribe anticoagulants such as heparins and aspirin in an attempt to prevent recurrent pregnancy complications; however, it is not clear that such interventions are always beneficial. Over the last few decades, efforts have been made to recognize predictors of recurrent pregnancy complications, identify those women at increased risk, and determine who might benefit from antenatal treatment.
Thrombophilias, both inherited and acquired, are a major risk factor for venous thromboembolic event (VTE) before and after delivery. 2 The odds ratio (OR) for the development of VTE during pregnancy is 15.8, 3 34.4, and 26.36 4 in women with antiphospholipid antibody syndrome (APS), homozygous factor V Leiden mutation (FVL), and homozygous prothrombin gene mutation (PGM), respectively. However, the data regarding the association between thrombophilia and recurrent pregnancy loss are less conclusive. Although some acquired thrombophilic disorders such as APS have a recognized association with recurrent pregnancy loss, 5 the impact of FVL and PGM on nonthrombotic complications of pregnancy is less certain. 6 These inherited disorders likely have little impact on miscarriage or placental-mediated complications such as preeclampsia, with only modest effect on late-term loss. Multiple studies have attempted to determine whether recurrent pregnancy loss may be mitigated with prophylactic anticoagulation 7 –13 ; however, these trials are often plagued by small numbers, heterogeneous patient populations, and differing definitions of early versus late loss and prior pregnancy complications. 14
Hemostatic Changes in Pregnancy
Pregnancy is characterized by physical and physiologic changes that contribute to a tendency to clot. Congestion within the pelvic veins from a gravid uterus leads to decreased blood flow to the lower extremities, and compression of the left iliac vein by the right iliac artery is a well-known phenomenon. 2 Yet, aside from the physical transformations of pregnancy, physiologic and hormonal changes within the placenta itself are key to the pathogenesis of many adverse pregnancy outcomes. 15,16 The placenta is a highly vascular organ composed of low-resistance vessels, and it is reasonable to infer that clot formation within the placental vasculature might result in placental insufficiency, intrauterine growth restriction, and other complications of gestation. During pregnancy, there is an increase in clotting factors VII, VIII, and X as well as a rise in the levels of von Willebrand factor and fibrinogen. 2 There is also a marked decrease in the activity of protein S as well as acquired resistance to activated protein C (Table 1). 17 Of note, there is little change in protein C activity during pregnancy, 18 and antithrombin levels remain constant. 19
Physiologic Changes During Pregnancy.a
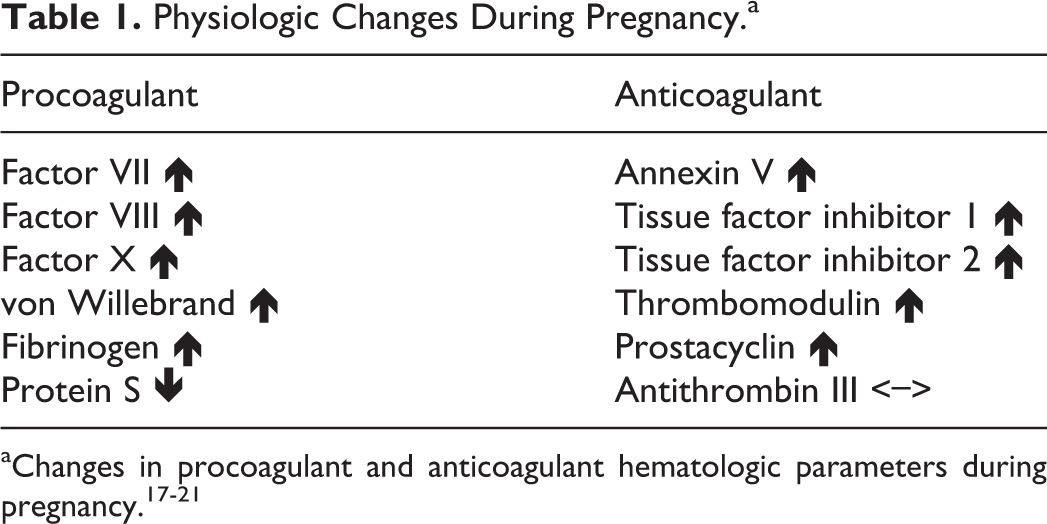
The placental circulation is shifted toward the procoagulant state, likely to counterbalance the risk of hemorrhage during placental implantation and as maternal blood flows through the intervillous space. 20 Trophoblasts, which line the spiral arteries of the uterus and eventually develop into the placenta, have a decreased capacity to lyse fibrin as compared with other endothelial cells. This is thought to be due to high levels of plasminogen activator inhibitors (PAI-1 and PAI-2), which lay down a framework of fibrin on the placental bed and impair the action of the anticoagulant tissue-type plasminogen activator. 19,22,23 Trophoblasts also express large amounts of tissue factor and phosphatidylserine, thus tipping the balance further toward hemostasis. 20 Microparticles—extracellular vesicles shed during cell signaling and apoptosis 24 —have also been implicated in the development of thrombotic pregnancy complications. 25 In a case–control analysis of 74 women with a history of pregnancy loss, 41 had increased levels of procoagulant circulating microparticles. 26
However, as in any biologic model, compensatory mechanisms exist within the placental milieu to offset the prothrombotic state, and these include annexin V, which is critical to preventing intervillous thrombosis, tissue factor pathway inhibitors (TFP-1 and TFP-2), thrombomodulin, and prostacyclin. 20,21,27 Yet, when the procoagulant factors overwhelm the anticoagulant ones, the risk of placental thrombosis rises. 22 Might not maternal thrombophilia disrupt this delicate equilibrium, potentiating clotting and potentially fetal loss? Although a hypercoagulable state is often invoked as the cause of adverse placenta-mediated events, this theory is not supported by therapeutic trials of anticoagulation. Excessive thrombosis may be only one of the several mechanisms contributing to the overall pathophysiology of adverse pregnancy outcomes.
Antiphospholipid Antibody Syndrome
Antiphospholipid antibody syndrome, an acquired thrombophilia defined by certain clinical and laboratory characteristics (Table 2), has been linked to myriad pregnancy complications, including VTE, preeclampsia, eclampsia, small for gestation age (SGA), preterm delivery, and fetal loss at all stages of gestation. Antiphospholipid antibody syndrome can present with thrombosis or manifest as “pure” obstetric APS. Obstetric APS refers specifically to a syndrome of recurrent early loss or sporadic late loss with positive antiphospholipid antibodies—lupus anticoagulant, anti–β2-glycoprotein 1, and anticardiolipin antibodies—without concurrent VTE.
Revised Criteria for APS.a
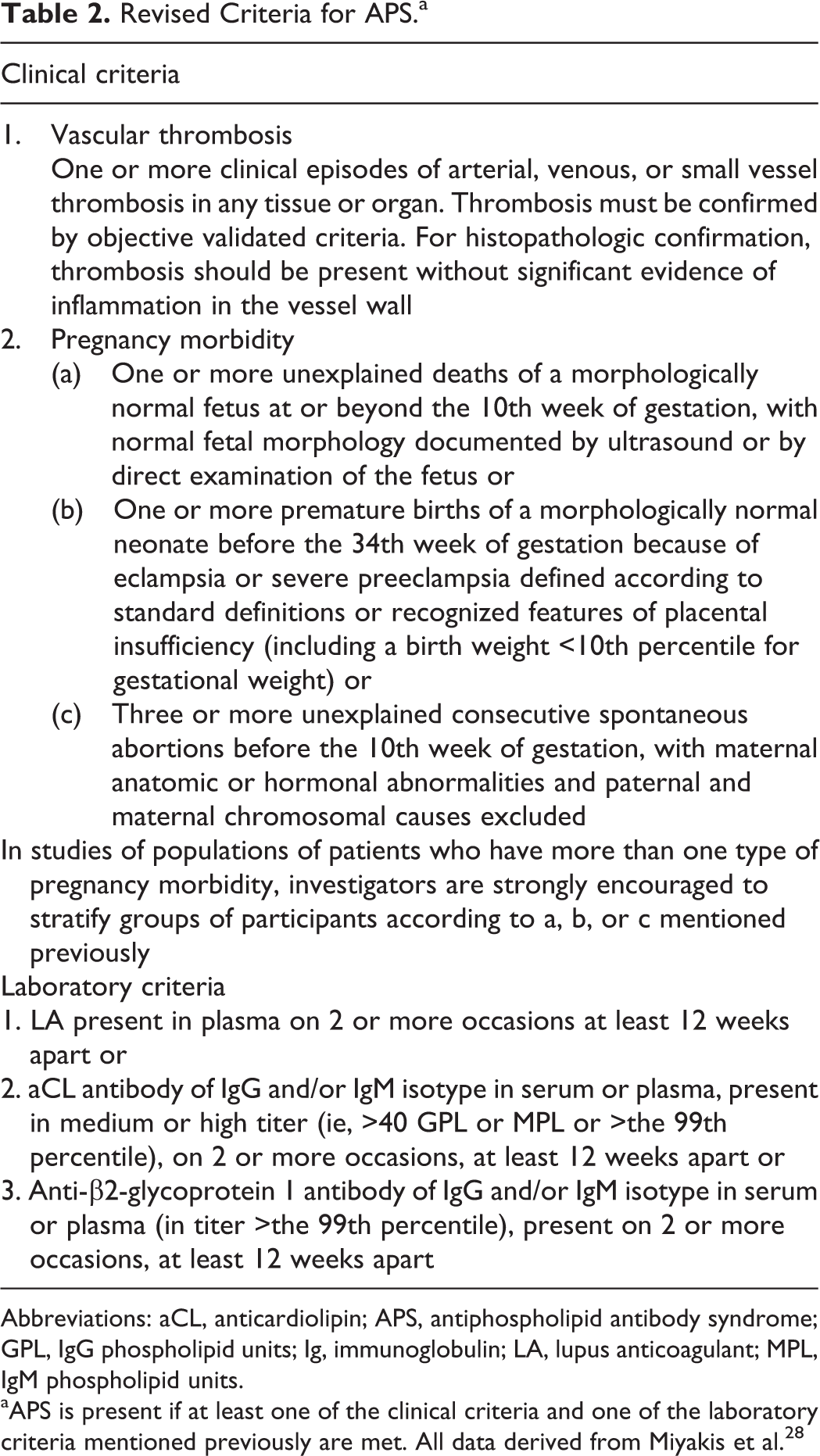
Abbreviations: aCL, anticardiolipin; APS, antiphospholipid antibody syndrome; GPL, IgG phospholipid units; Ig, immunoglobulin; LA, lupus anticoagulant; MPL, IgM phospholipid units.
aAPS is present if at least one of the clinical criteria and one of the laboratory criteria mentioned previously are met. All data derived from Miyakis et al. 28
Antiphospholipid antibody syndrome is a complex disorder characterized by abnormalities of coagulation, complement dysfunction, and other autoimmune phenomena. Antiphospholipid antibodies are known to increase the risk of maternal thrombosis during pregnancy 3 and are also thought to impair trophoblast growth and development, ultimately leading to placental insufficiency. 29 In 1997, a randomized control trial of 90 women with recurrent miscarriage and persistently positive antiphospholipid antibodies found a beneficial effect on live birth rate in women treated with antepartum low-molecular-weight heparin (LMWH) and aspirin (71% live birth rate) versus aspirin alone (42% live birth rate). 5 However, this study has been critiqued for a heterogeneous study population, a lower than expected birth rate in the aspirin-alone group, and for the inclusion of women with very low titers of anticardiolipin antibodies. 30 And although some trials evaluating LMWH plus aspirin in women with antiphospholipid antibodies and recurrent loss have failed to show such positive results, 31 –33 antepartum treatment with LMWH and aspirin is endorsed by the American College of Chest Physicians 34 and The American College of Obstetricians and Gynecologists 35 in women with obstetric APS. However, it should be noted that there are no data to support the use of aspirin alone in the prevention of recurrent miscarriage in patients with APS. Three placebo-controlled trials and one meta-analysis found no difference in outcome in women treated with and without aspirin. 33,36
Data indicate a stronger association between pregnancy complications and APS depending on the type of antibody present. 37 –39 Of the 3 most prevalent antiphospholipid antibodies, the lupus anticoagulant is thought to be the most predictive of adverse pregnancy outcomes. 40 Moreover, a recent retrospective analysis concluded that patients with APS having thrombosis and “triple” antibody positivity (ie, lupus anticoagulant, anti–β2-glycoprotein 1, and anticardiolipin antibodies) are at highest risk of pregnancy complications and benefit most from combined antepartum anticoagulation. 38 These women had a live birth rate of 58.3% when treated with just heparin or low-dose aspirin alone, but the birth rate increased to 92.9% when at least 2 medical therapies were used (ie, aspirin plus heparin).
A recent prospective observational study of 6318 women with pregnancy complications was undertaken at the University Hospital of Nimes, France (the Nimes Obstetricians and Hematologists Antiphospholipid Syndrome [NOH-APS] observational study). 41 The authors enrolled women without a history of thrombosis who had experienced at least 3 consecutive spontaneous abortions before the 10th week of gestation or 1 fetal loss at or beyond the 10th week of gestation (late loss) and observed them during subsequent pregnancies. The control group consisted of women with prior pregnancy loss without antiphospholipid antibodies or inherited thrombophilia (N = 796). 38,42 A total of 517 women with obstetric APS were included in the study, 3.3% of whom had concurrent antiphospholipid antibodies and an inherited thrombophilia. All women with confirmed obstetric APS were treated with low-dose aspirin 100 mg/d while not pregnant, and prophylactic enoxaparin 40 mg/d was initiated at the time of positive pregnancy test through delivery.
Women with APS and prior late fetal loss were found to be at increased risk of subsequent fetal loss, preeclampsia, premature birth, and other placenta-mediated pregnancy complications when compared to women with APS and recurrent early losses. Patients with obstetric APS and previous spontaneous abortions had similar rates of early loss as women in the control group; however, women with obstetric APS experienced more late losses. Moreover, despite treatment with LMWH and aspirin, the incidence of pregnancy complications in all women with obstetric APS was higher than that of the controls. 41 Thus, although the data are somewhat mixed, and despite the fact that women with APS treated with LMWH and aspirin still have higher rates of pregnancy complications, we recommend the combination of these agents in obstetric APS. However, there is an urgent need for further randomized trials exploring additional treatment options in these patients.
Recommendation
In women with obstetric APS, we recommend prophylactic LMWH combined with aspirin 81 mg/d once pregnancy is confirmed.
Inherited Thrombophilias: FVL and PGM
There are no sufficiently powered trials to adequately determine the effect of inherited thrombophilias on recurrent pregnancy loss, preeclampsia, SGA, or other placenta-mediated complications. 6,43,44 An observational study assessed the effect of LMWH with or without aspirin on miscarriages in 1011 pregnancies amongst 416 women with FVL or PGM. 6 After adjusting for multiple variables, the authors concluded that LMWH had a protective effect on late pregnancy loss with an OR of 0.52 (95% confidence interval [CI]: 0.01-0.21). Aspirin appeared to have no effect on recurrent miscarriage. 6 However, this observational study was fraught with heterogeneity, and it is difficult to draw definitive conclusions from the data. In another trial, the HABENOX (Habitual abortion and enoxaparin) group randomized 207 women with at least 3 consecutive first trimester miscarriages, 2 or more second trimester miscarriages, or 1 third trimester loss combined with 1 first trimester miscarriage to enoxaparin 40 mg and placebo once daily (n = 68), enoxaparin 40 mg and aspirin 100 mg (n = 63), or aspirin 100 mg alone (n = 76). About 25% of patients in each arm had a history of thrombophilia. There was no difference in live birth rate among all 3 arms, with an overall live birth rate of 65% (95% CI: 58.66-71.74). 8
Some data suggest that inherited thrombophilias contribute more to late losses than to earlier miscarriages. 45 –47 The NOH-APS study enrolled a third cohort of women (n = 279) with FVL and PGM, no prior thrombosis, and a history of 3 consecutive spontaneous abortions before 10 weeks’ gestation or 1 fetal death (considered a late loss) after 10 weeks. 42 Only women with a history of late loss were given prophylactic LMWH at a dose of 40 mg/d. The incidence of fetal death, premature live birth, early and late onset preeclampsia, and other placenta-mediated complications was recorded.
The authors found that women receiving LMWH for a history of late fetal loss had lower rates of fetal death (10.3% vs 23.2%) and premature birth (12.3% vs 25%). Moreover, treated women with prior late pregnancy loss were more likely to give birth to a live infant than their untreated counterparts (70.3% vs 50.2%). The difference in the rate of recurrent miscarriage between thrombophilic women with prior early losses and nonthrombophilic women was similar. Although there was a trend toward higher rates of fetal death (8.8% vs 2.3%), preeclampsia (6.6% vs 2.9%), preterm live birth rates (16.4% vs 9.2%), and neonatal mortality (2.7% vs 0.5%) in the untreated thrombophilic group, there was no statistically significant difference. 42 These data suggest the benefit of prophylactic LMWH in women with FVL or PGM and late loss and question recommendations not to use LMWH in thrombophilic women with early loss or other complications. 34
In the Thrombophilia in Pregnancy Prophylaxis Study (TIPPS), investigators enrolled 292 pregnant women with a history of thrombophilia and VTE or placenta-related adverse event and randomized them to receive either dalteparin or no drug. 48,49 Women with FVL and PGM were included in the study, and aspirin use was not controlled. There were many primary composite outcome measures including symptomatic VTE, preeclampsia, birth of SGA infant, or pregnancy loss. A total of 17.1% of women receiving antepartum dalteparin experienced one of the primary outcomes, as compared with 18.9% of patients in the untreated group, revealing no statistical difference. However, when compared to the Nimes Obstetricians and Hematologists (NOH) study, the number of women with FVL and PGM was smaller in the TIPPS study, and patients were not stratified according to early or late loss or thrombophilic risk factor. In another negative study, the Scottish Pregnancy Intervention (SPIN) trial, 294 women with a history of 2 or more fetal losses at <24 weeks were randomized to treatment with enoxaparin 40 mg once daily and aspirin 75 mg daily or surveillance alone. There was no difference in the rate of recurrent miscarriage, although very few thrombophilic women were included. 7 A recent Cochrane review of 9 studies with a total of 1228 women concluded that there are no definitive data to recommend the use of anticoagulation in women with recurrent miscarriages who have inherited thrombophilias. 50 An ongoing trial, Anticoagulants for Living Fetuses in Women with Recurrent Miscarriages and Inherited Thrombophilia study (ALIFE2), hopes to shed further light on this subject. Women who are actively trying to conceive, and with a history of thrombophilia and 2 or more prior miscarriages, will be randomized to prophylactic LMWH once daily or no intervention. We anxiously anticipate these results.
Recommendation
We do not routinely recommend prophylactic anticoagulation for women heterozygous for FVL or PGM with a history of recurrent early miscarriage or late loss. However, anticoagulation may be prescribed depending on VTE risk.
Protein C, S, and Antithrombin Deficiency
The data supporting the use of prophylactic anticoagulation for the prevention of miscarriage and late-term losses in women with inherited deficiencies of the endogenous anticoagulants protein C, S, and antithrombin III are fraught with heterogeneity. The European Prospective Cohort on Thrombophilia (EPCOT), a large retrospective case–control study, enrolled 843 women with thrombophilia, 571 of whom had 1524 pregnancies, and compared them with a control group of 541 women, of whom 395 had 1019 pregnancies. The overall risk for late loss was higher than for early loss in women with thrombophilia: OR 3.6 (95% CI: 1.4-9.4) versus 1.27 (95% CI: 0.94-1.71). The OR for fetal loss after 28 weeks was 2.3 for women with protein C deficiency (95% CI: 0.6-8.3), 3.3 with protein S deficiency (95% CI: 1.0-11.3), and 5.2 with antithrombin deficiency (95% CI: 1.5-18.1). The OR for late loss in women with combined thrombophilias was 14.3 (95% CI: 2.4-86.0). Antithrombin deficiency was the only defect statistically associated with loss less than 28 weeks. 10
A prior study from the Nimes group evaluated 232 women with a history of late fetal loss and compared them with 464 matched controls. The OR of a woman with protein C deficiency sustaining a late loss was 1.00 (95% CI: 0.09-10.9), whereas the OR of late loss in a woman with protein S deficiency was 22.0 (95% CI: 2.8-170). 51 A case–control study by Many et al evaluated 40 women with late unexplained intrauterine fetal deaths and compared them with a reference group of 80 healthy women with at least 1 normal pregnancy. Although there was a trend toward late loss in women with protein S deficiency, it was not statistically significant. 52 Alfirevic et al found increased numbers of late pregnancy losses in women with antithrombin deficiency, but this did not reach statistical significance likely given the small sample size. 53 A meta-analysis of 31 cohort, case–control, and cross-sectional studies concluded that protein S deficiency portended an OR of 7.39 for late nonrecurrent fetal loss (95% CI: 1.28-42.63). Although the protein C and antithrombin deficiency were not associated with fetal loss, the numbers were too small to determine. 11
Recommendation
We do not recommend anticoagulation in women with protein C, protein S, and antithrombin III deficiency for the prevention of placenta-medicated complications. However, anticoagulation may be prescribed depending on VTE risk.
Anticoagulation in Preeclampsia, HELLP Syndrome, and Placental Abruption
Women with a history of preeclampsia have a 25% to 65% risk of recurrent preeclampsia, and those with a history of HELLP syndrome have about a 19% to 27% chance of recurrence. 54 –56 Women with previous preeclampsia also have about a 3% risk of placental abruption and a 10% risk of having an SGA child. 54,57
A meta-analysis of 32 217 women at risk of preeclampsia, randomized to receive either aspirin or dipyridamole versus placebo, concluded that for women who received an antiplatelet agent, the relative risk of developing preeclampsia was 0.90 (95% CI: 0.83-0.98). 58 As such, aspirin has been touted as providing a small but important advantage in reducing the risk of preeclampsia. However, it is thought to be most advantageous when given prior to 16 weeks’ gestation and in the prevention of severe and early-onset preeclampsia. 59,60
In a prospective randomized controlled trial (RCT) conducted by the HAPPY (Adverse Pregnancy outcome to improve the rate of successful PregnancY) study group, 135 women with a history of preeclampsia, HELLP syndrome, and other placental-mediated complications received either medical surveillance or 3800 IU of nadroparin daily. The primary outcome was late pregnancy complications. A total of 13 (21%) of 63 women in the observation arm and 12 (18%) of 65 in the treatment arm reached the primary outcome, with an absolute risk difference of 2.2 (95% CI: 11.6-16.0) that was not statistically significant. 61 However, in the HAPPY study, prophylaxis with nadroparin only began after the 13th week of gestation, and it is possible that earlier institution of anticoagulation would have resulted in a different outcome. In a multicenter retrospective study, 58 women with a history of preeclampsia and thrombophilia were evaluated for recurrent preeclampsia during subsequent pregnancies. Twenty-six women received LMWH plus aspirin, 22 received aspirin alone, and 10 received no intervention. No benefit was seen with the addition of LMWH. 62
One of the largest RCTs to evaluate the effect of LMWH on preeclampsia and the HELLP syndrome was the FRUIT (FRactionated heparin in pregnant women with a history of Utero-placental Insufficiency and Thromophilia) study. 63 Inclusion criteria for the study were (1) history of thrombophilia, (2) prior delivery at less than 34 weeks’ gestation, and (3) previous pregnancy complicated by preeclampsia, eclampsia, HELLP, or SGA. In this study, 139 women were randomly assigned to receive aspirin 80 mg once daily with or without dalteparin 5000 IU daily beginning at less than 12 weeks’ gestation. The primary outcomes were recurrence of preeclampsia, eclampsia, or HELLP at any gestational age or at <34 weeks’ gestation. There was no statistically significant difference in the development of these disorders irrespective of gestational age: 18.6% of women randomized to LMWH and ASA (n = 13 of 70) developed preeclampsia, eclampsia, or HELLP as compared with 21.7% (n = 15 of 69) of those taking aspirin alone (95% CI: 10.5-16.7). However, of the women who developed hypertensive disorders at <34 weeks’ gestation, 0 were in the dalteparin and ASA arm and 6 (8.7%) were in the ASA-alone group.
The data regarding the association between maternal thrombophilia and risk for placental abruption are mixed. In a single-center pilot study, Gris et al randomized 160 women with a history of placental abruption to either prophylactic enoxaparin or no enoxaparin beginning at the time of positive pregnancy test. Women with antiphospholipid antibodies were excluded, but those with FVL or PGM comprised a small percentage of the study population. The primary outcome included placental abruption, preeclampsia, low birth weight, or fetal loss after 20 weeks. The investigators found that enoxaparin reduced the composite outcome from 31.3% to 12.5% (hazard ratio: 0.37, 95% CI: 0.18-0.77). However, other studies have failed to yield such positive results. 64
A recent meta-analysis by Rodger et al sought to determine the utility of LMWH in the prevention of recurrent placenta-mediated pregnancy complications such as preeclampsia. 45 Six RCTs with a total of 848 pregnant women at risk for recurrent preeclampsia, SGA, placental abruption, or pregnancy loss >20 weeks were included. Overall, 67 (18.7%) of 358 women administered prophylactic LMWH had recurrent placental-mediated pregnancy complications as compared with 127 (42.9%) of 296 women receiving no intervention. The number of women with recurrent preeclampsia in the LMWH group was 34 (8.6%) of 391 versus 75 (21.6%) of 348 women who were not treated with anticoagulation. 45 The FRUIT study was the only trial that specifically included women with a history of thrombophilia. The authors emphasize that LMWH may be effective only in the most severe cases of placenta-mediated pregnancy complications, and call for more sophisticated multicenter trials help elucidate this issue.
Recommendation
We recommend antepartum aspirin 81 mg once daily in women with a history of preeclampsia. There is currently insufficient data to recommend LMWH for the secondary prevention of preeclampsia or other placenta-mediated pregnancy complications.
Anticoagulation for Recurrent Miscarriage Without Thrombophilia
We believe that the data do not support the use of anticoagulation (either with LMWH or aspirin) for the prevention of recurrent miscarriage in women without thrombophilia. This has been clearly demonstrated in the Anticoagulants for Living Fetuses (ALIFE1) trial, 9 TIPPS, and SPIN 7 among others. Pasquier et al recently published a randomized placebo-controlled trial of enoxaparin 40 mg once daily versus placebo in 258 pregnant women with a history of recurrent miscarriage without acquired or inherited thrombophilia. The primary end point was live birth rate. In an intention-to-treat analysis, 66.6% of women in the enoxaparin group and 72.9% of women in the placebo group had a live birth. 13 There was no statistically significant improvement in the primary or secondary end points with the addition of LMWH. Schleussner et al randomized 449 women with at least 2 consecutive early miscarriages or 1 late miscarriage to prophylactic dalteparin plus multivitamin or multivitamin alone. The majority of patients did not have inherited thrombophilia, and those with APS were excluded. Low-molecular-weight heparin did not improve ongoing pregnancy or live birth rates among participants. 65 Yet, despite what we feel are conclusive results, clinicians continue to prescribe anticoagulation for the prevention of recurrent miscarriage in women without thrombophilia, subjecting their patients to increased risk of bleeding, withholding of epidural anesthesia, and financial burden.
Recommendation
We do not recommend LMWH or aspirin to patients with 2 or more unexplained pregnancy losses without thrombophilia.
If Choosing to Anticoagulate, What to Use?
Heparins—LMWH, unfractionated heparin (UFH), and danaparoid—are the most commonly used anticoagulants during pregnancy as they do not cross the placenta. 66 Low-molecular-weight heparin is preferred over UFH, as LMWH is easier to administer, has more predictable pharmacokinetics, does not require monitoring, and is less likely to cause osteoporosis and heparin-induced thrombocytopenia than UFH. However, in the final weeks of pregnancy, women are often transitioned from LMWH to UFH given the shorter half-life of the latter, allowing for rapid epidural placement or cesarean section if needed. Warfarin is not recommended except in certain circumstances (such as in women with mechanical heart valves), and there is little data regarding the use of novel anticoagulants (including factor Xa inhibitors) in pregnancy. 34,67,68
For prophylactic anticoagulation dosing, we recommend enoxaparin 40 mg once daily, UFH 5000 U twice daily, or dalteparin 5000 U daily. However, as pregnancy progresses, women require higher doses of anticoagulation to achieve the same peak plasma concentrations. 69 For instance, the American College of Obstetricians and Gynecologists recommends UFH 5000 to 7500 U twice daily in the first trimester, UFH 7500 to 10 000 U twice daily in the second trimester, and UFH 10 000 U twice daily in the third trimester. 70 Although we do not routinely monitor anti-Xa levels, we target a goal of 0.1 to 0.3 four hours after the administration of LMWH.
Conclusion
Despite current available evidence, real-world decisions regarding anticoagulation for pregnancy complications are often difficult to make. Robust RCTs are lacking, and much has yet to be learned about the pathophysiology of recurrent pregnancy loss and placenta-mediated complications. Table 3 summarizes our approach to most patients. Of course, as each patient has unique risk factors, preferences, and values, recommendations must be tailored to the specific individual.
Recommendations for the Prevention of Recurrent Loss or Placenta-Mediated Complications.a
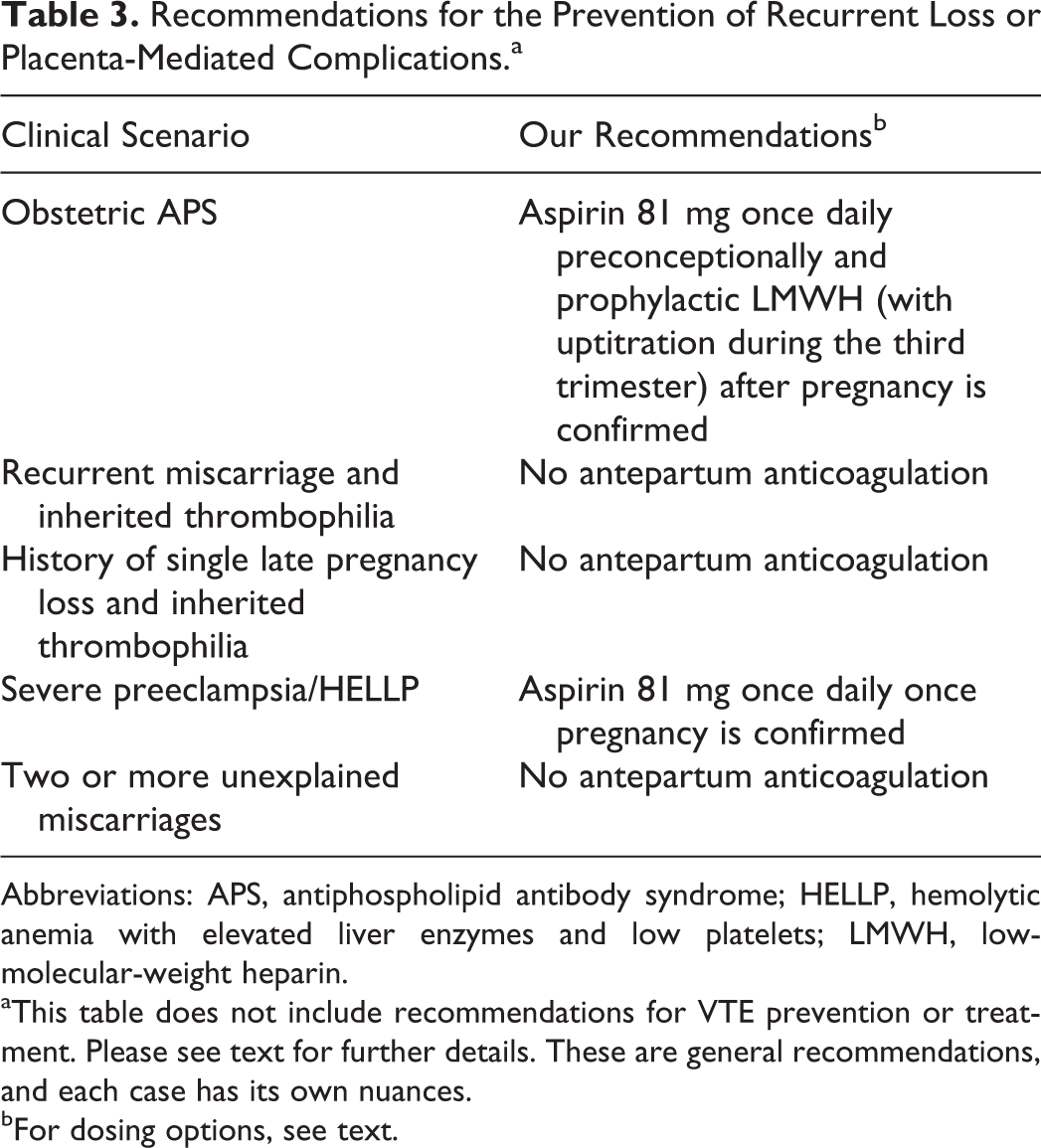
Abbreviations: APS, antiphospholipid antibody syndrome; HELLP, hemolytic anemia with elevated liver enzymes and low platelets; LMWH, low-molecular-weight heparin.
aThis table does not include recommendations for VTE prevention or treatment. Please see text for further details. These are general recommendations, and each case has its own nuances.
bFor dosing options, see text.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.