
Abstract
Background:
Management of patients with acute pulmonary embolism has evolved from obligatory hospitalization to home treatment of carefully selected low-risk patients. The purpose of this investigation is to determine national trends in the prevalence of home treatment of pulmonary embolism.
Methods:
The Nationwide Emergency Department Sample was used to determine the number of patients seen in emergency departments throughout the United States with a primary (first-listed) diagnosis of pulmonary embolism and the proportion hospitalized according to age, from 2007 to 2012. The National (Nationwide) Inpatient Sample was used to determine in-hospital all-cause mortality and length of stay of hospitalized patients. Patients were adults (≥18 years) of both genders and all races from all regions of the United States. Excluded patients were those in shock or on ventilator support. International Classification of Diseases, Ninth Revision, Clinical Modification codes were used to identify patients and comorbid conditions.
Results:
Home treatment was selected for 54 494 (6.0%) of 915 702 stable patients with acute pulmonary embolism. The proportion of patients treated at home was age-dependent, highest in those aged 30 years or younger, 12.1%, and lowest in those >80 years, 2.9%. Most patients treated at home, 66.8%, and had no comorbid conditions. In-hospital all-cause deaths were 2.6%. Deaths were ≤0.9% in those ≤40 years and 4.8% in those >80 years. Length of stay was 6 days or longer in 37.6% of patients.
Conclusion:
In view of the lower death rate among younger patients, they might be a group in whom home treatment would be more advantageous than in elderly patients.
There has been an evolution of thought on the management of patients with acute pulmonary embolism. The traditional opinion was that all patients with acute pulmonary embolism should be hospitalized. 1 However, many reports have shown that carefully selected low-risk patients with pulmonary embolism can be managed safely entirely at home or after 2 days or less of hospitalization.2 –16 The 2016 CHEST guideline and expert panel now recommend home treatment or early discharge in patients with low-risk pulmonary embolism whose home circumstances are adequate. 17 The previous CHEST recommendation, 2012, stated that appropriately selected patients may be discharged early, but did not recommend home treatment. 18,19 The British Thoracic Society, in 2003, suggested that outpatient treatment of pulmonary embolism may be considered if the patient is not unduly breathless, there are no medical or social contraindications, and there is an efficient protocol in place. 20 The purpose of this investigation is to determine national trends in the prevalence of home treatment of pulmonary embolism.
Materials and Methods
This investigation required the use of 2 databases, the Nationwide Emergency Department Sample (NEDS) and the National (Nationwide) Inpatient Sample (NIS). The NEDS—Healthcare Cost and Utilization Project (HCUP), Agency for Healthcare Research and Quality—was used to determine the number of patients seen in emergency departments throughout the United States with a primary (first-listed) diagnosis of pulmonary embolism, the proportion of such patients hospitalized according to age, and deaths in the emergency department. 21 We analyzed data from 2007 to 2012. Each year, this database includes 26 to 29 million emergency department visits, with 955 to 980 hospital-based emergency departments in 24 to 29 states. The NIS—HCUP, Agency for Healthcare Research and Quality—was used to determine in-hospital all-cause mortality and length of stay of hospitalized patients with stable pulmonary embolism from 2007 to 2012. 22 Each year, the NIS provides information on approximately 8 million inpatient stays from about 1000 hospitals. The NIS is designed to approximate a 20% sample of US nonfederal, short-term, general, and other specialty hospitals. Beginning with 2012 data, the NIS was redesigned to improve national estimates. 22 To highlight the design change, beginning with 2012 data, the database was renamed from the “Nationwide Inpatient Sample” to the “National Inpatient Sample.” The NIS is now a sample of discharge records from all HCUP-participating hospitals, rather than a sample of hospitals from which all discharges were retained.
Included patients were adults (≥18 years) of both genders and all races from all regions of the United States with a primary (first-listed) diagnosis of pulmonary embolism. We assume that patients with a first-listed diagnosis were seen in the emergency department or hospitalized because of pulmonary embolism. Excluded patients were those in shock or on ventilator support, who we define as unstable. Patients younger than 18 years were excluded.
The International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes used were pulmonary embolism 415.1, shock 785.5, and ventilator dependence V46.1.
We determined the comorbid conditions listed in the Charlson comorbidity index among the patients treated entirely at home, hospitalized for any duration, and hospitalized >5 days. 23 The comorbid conditions listed in the Charlson comorbidity index and the ICD-9-CM codes used to identify these conditions are shown in Table 1. Five days is the length of stay that might be required to initiate therapy with warfarin if the patient was hospitalized only for the initiation of anticoagulant therapy. Length of stay >5 days might be considered longer than required for the initiation of anticoagulant therapy.
ICD-9-CM Comorbid Conditions Included in the Charlson Comorbidity Index. 23
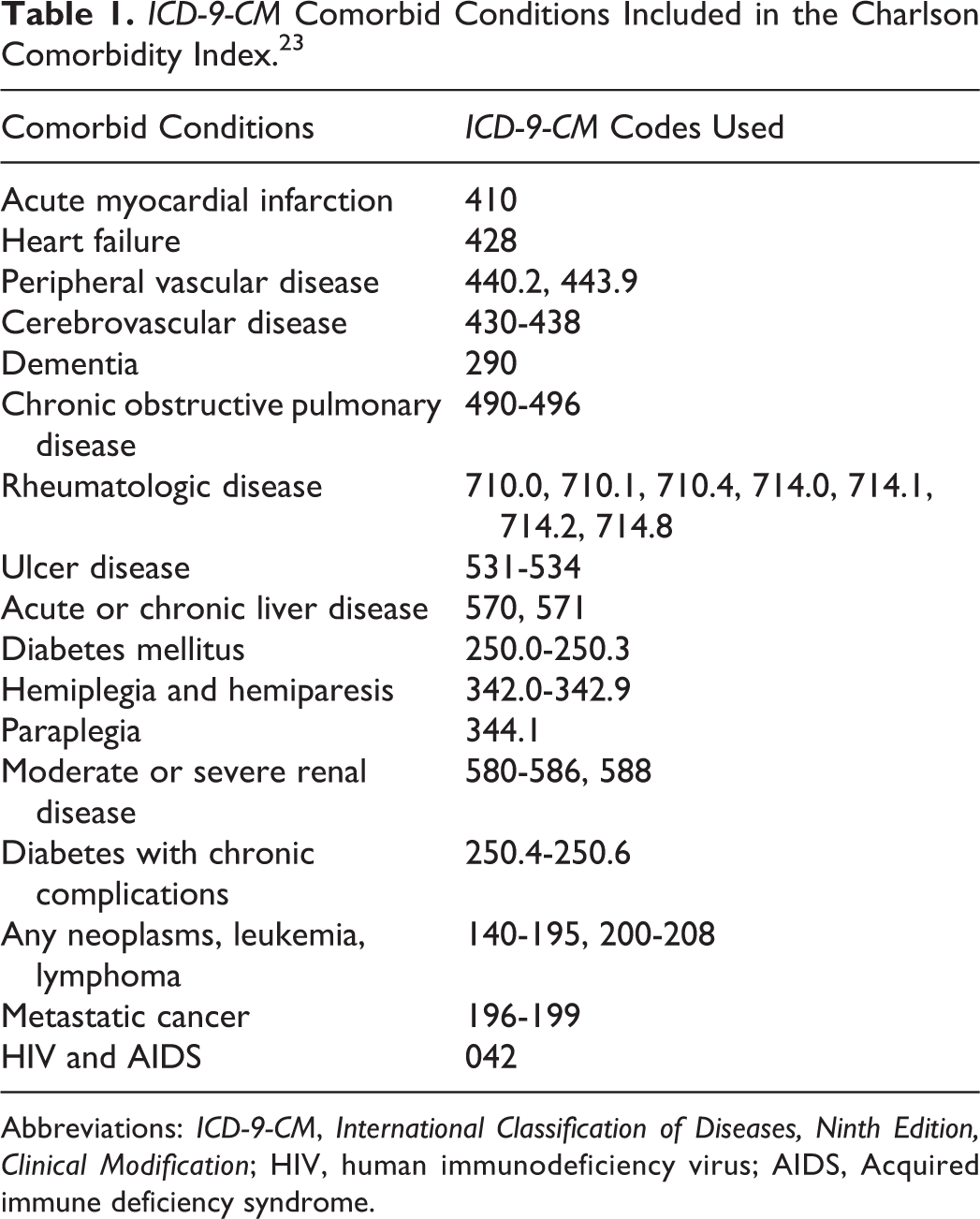
Abbreviations: ICD-9-CM, International Classification of Diseases, Ninth Edition, Clinical Modification; HIV, human immunodeficiency virus; AIDS, Acquired immune deficiency syndrome.
Statistical Analysis and Methodological Considerations
Descriptive statistics were used to graphically display trends over time in case volumes. Linear regression analyses (InStat version 3.0; GraphPad Software, San Diego, California) were used to calculate the slopes of linear segments describing the data. Pearson correlation analyses were used to assess the extent of dispersion of points around the regression lines.
Results
From 2007 to 2012, 928 600 patients were seen in emergency departments throughout the United States with a primary diagnosis of pulmonary embolism (Figure 1). Among these, 915 702 (98.6%) were stable (not in shock or on ventilator support; Figure 1 and Table 2), of which 54.0% was women (Table 2). The number of patients seen in emergency departments increased with age until 71 to 80 years of age (Table 2). Hospitalization was selected for 850 548 (92.9%), home treatment for 54 494 (6.0%), and other in 10 660 (1.1%; Figure 1). “Other” included transfer to a skilled nursing facility (4938), discharged against medical advice (2181), unknown (873), died in the emergency department (2659), or discharged alive (8).
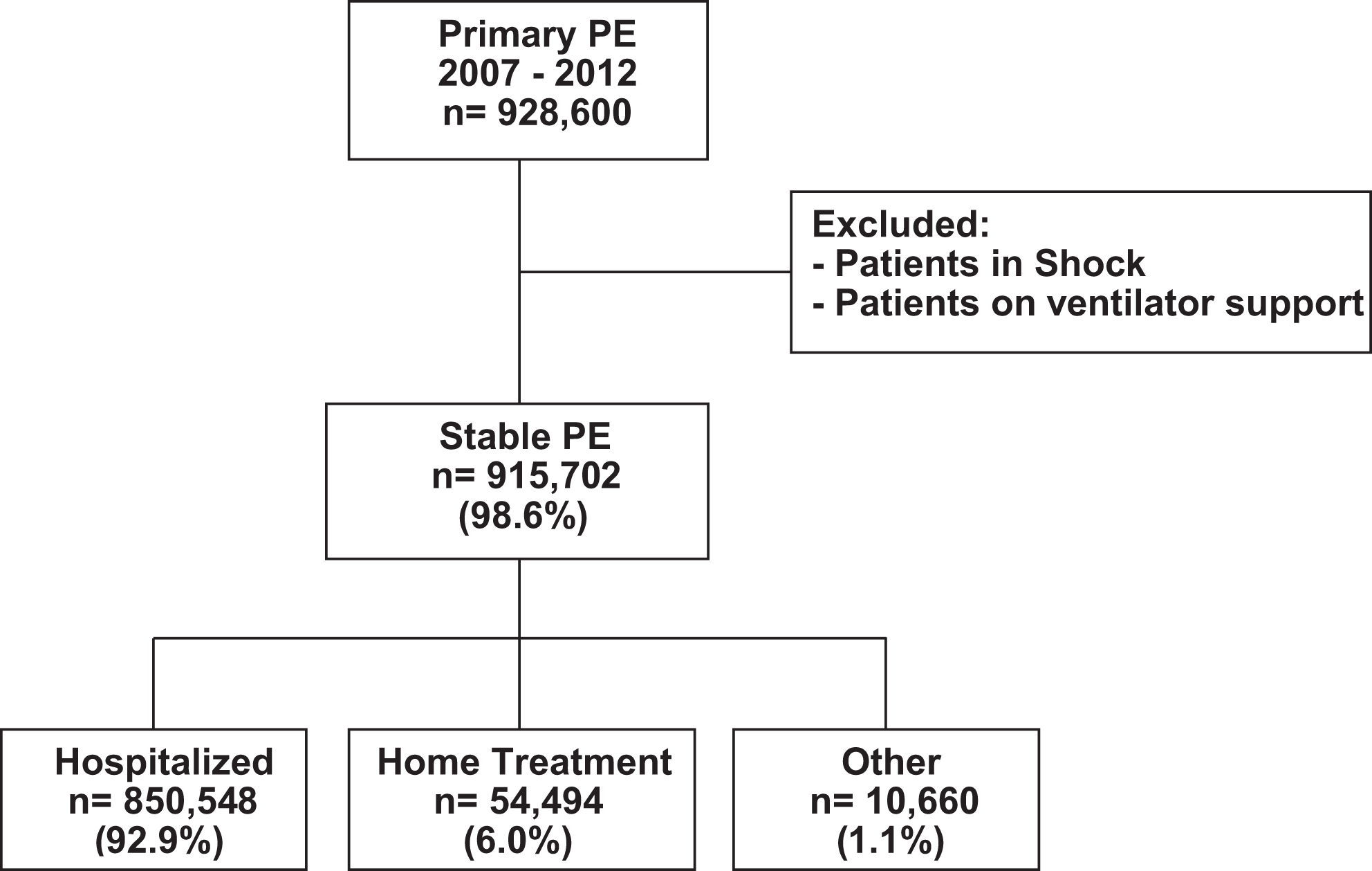
Flow diagram showing number and proportion of recruited patients according to home treatment. “Other” included transfer to a skilled nursing facility (4938), discharged against medical advice (2181), unknown (873), died in the emergency department (2659), or discharged alive (8). Data are from the Nationwide Emergency Department Sample. A larger number of hospitalizations were shown in the National Inpatient Sample (1 017 466 compared with 850 548).
Home Treatment According to Year, Age, and Gender.a
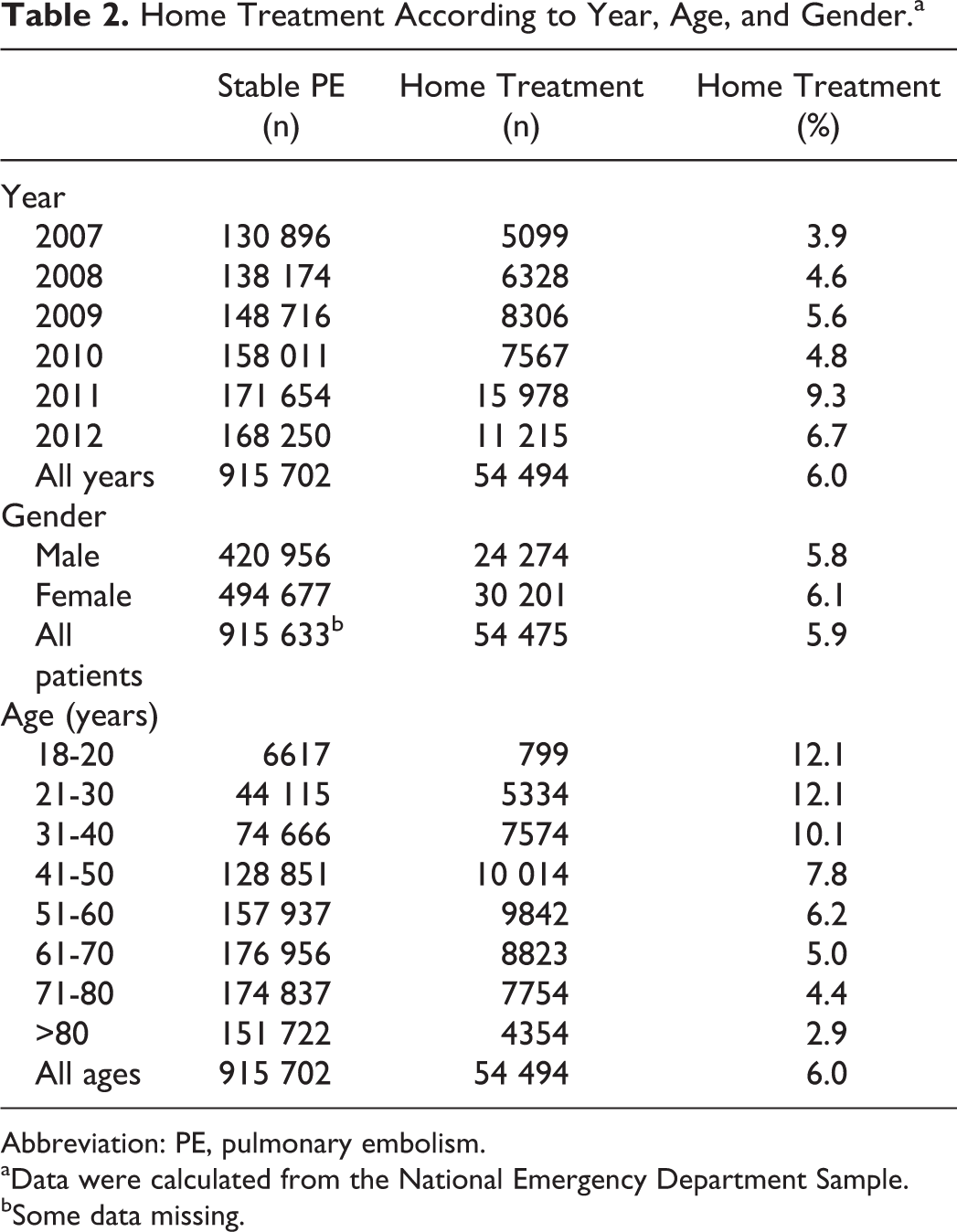
Abbreviation: PE, pulmonary embolism.
aData were calculated from the National Emergency Department Sample.
bSome data missing.
The proportion of patients treated at home tended to increase from 2007 to 2012 (Figure 2). The proportion of patients treated at home was age-dependent and highest in those aged 30 years or younger (12.1%; Figure 3). The proportion of patients treated at home decreased to 2.9% in those older than 80 years.
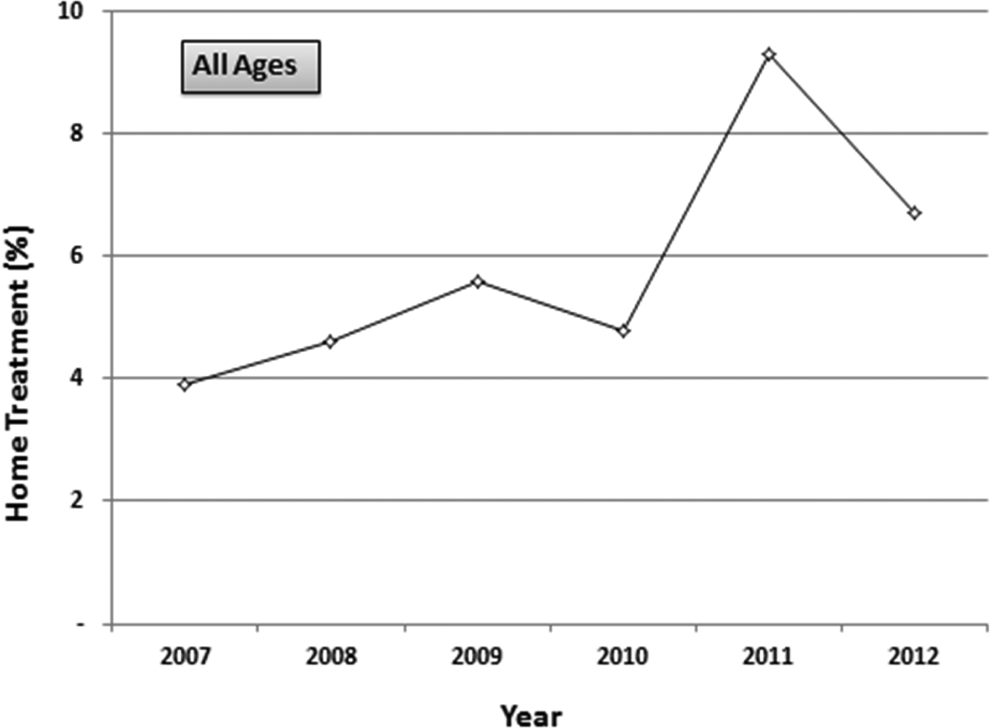
Proportion of patients with pulmonary embolism who received home treatment according to year. r = .476, P = .089.
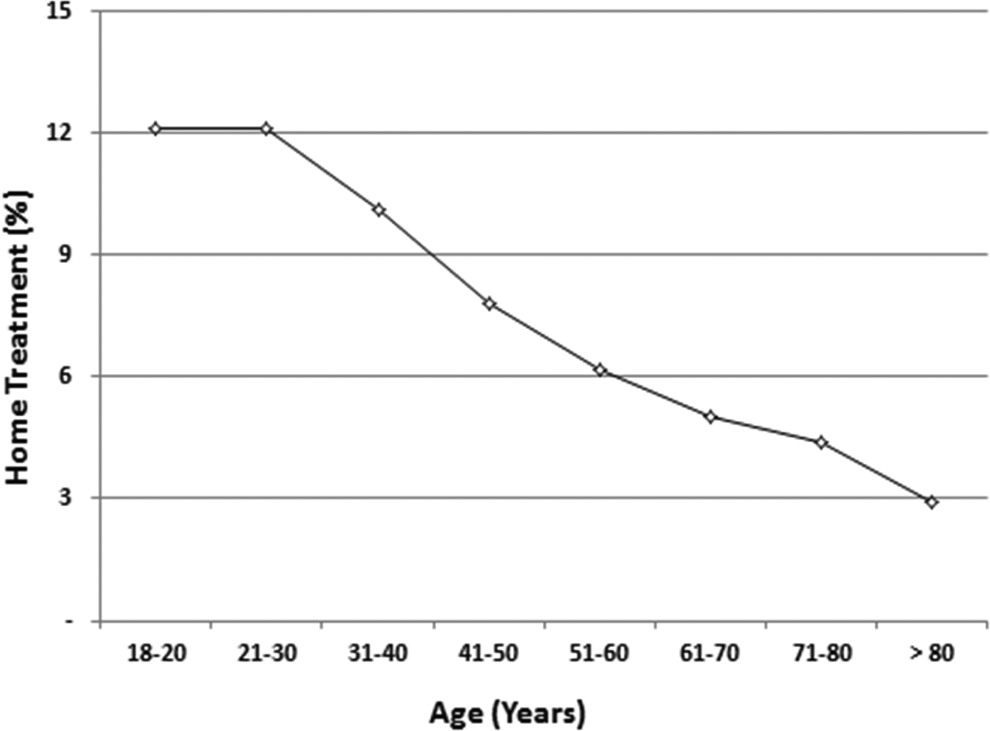
Proportion of patients with pulmonary embolism who received home treatment according to age. r = .957, P < .0001.
In-hospital mortality is based on data from the NIS. The number of stable patients (1 017 466) with acute pulmonary embolism hospitalized from 2007 to 2012 was 19.6% higher than that calculated from the National Emergency Department Sample (850 548). All-cause in-hospital deaths were 26 298 (2.6%) of 1017 466 (Table 3). Deaths in hospital were 0.9% or less in those aged 40 years or younger and 4.8% in those over 80 years of age (Table 3 and Figure 4).
Hospitalizations With Stable Pulmonary Embolism and In-Hospital Deaths According to Year, Age, and Gender.a
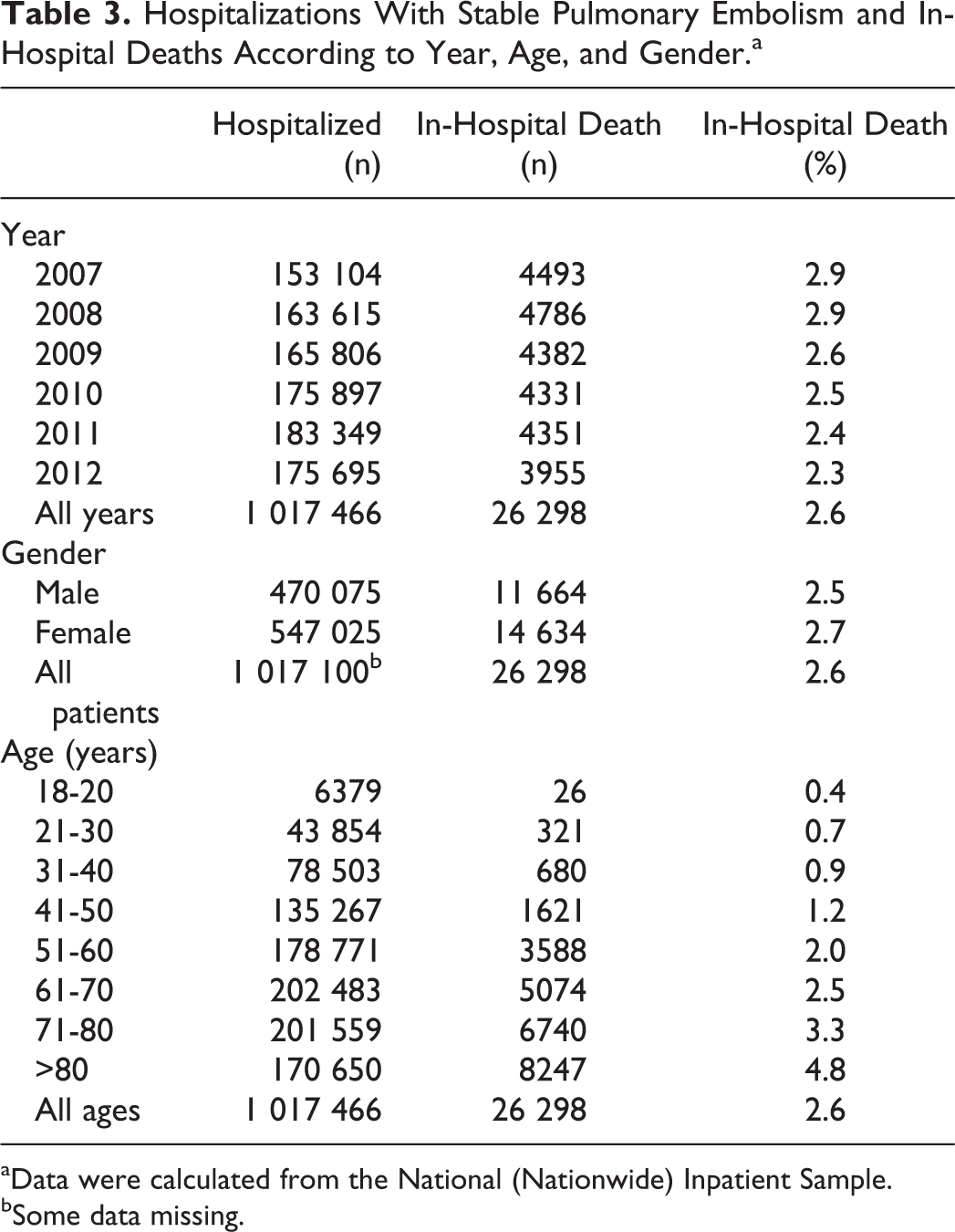
aData were calculated from the National (Nationwide) Inpatient Sample.
bSome data missing.
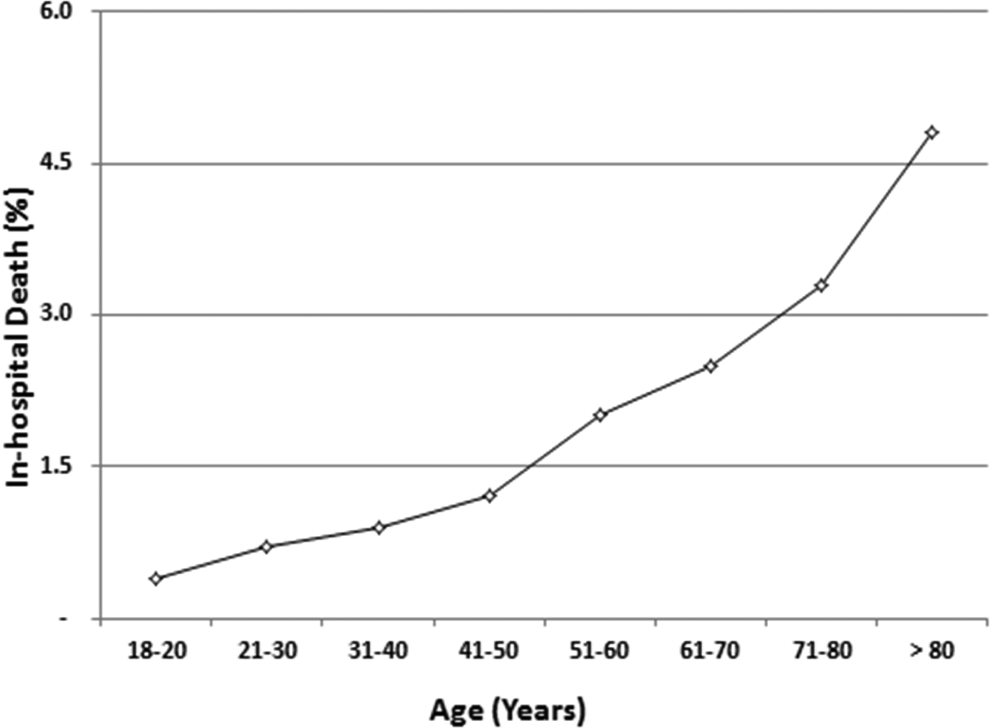
Proportion of in-hospital all-cause deaths according to age. r = .986. P < .0001.
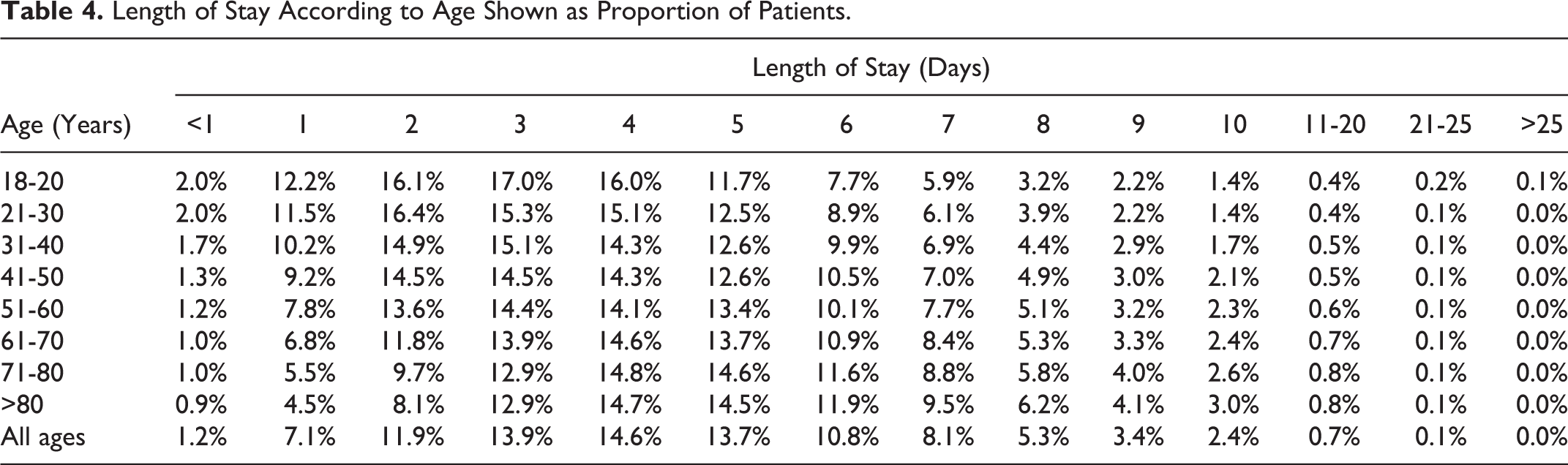
Discharge in 1 day or less was in 8.3% of stable patients, and discharge in 2 days or less was in 20.2% (Table 4 and Figure 5). Length of stay was 6 days or longer in 37.6% of patients. Length of stay increased with increasing age (Table 4 and Figure 6). Among those aged 21 to 30 years, length of stay was 6 days or longer in 27.1%, whereas in patients aged >80 years, length of stay was 6 days or longer in 44.4% (Table 4).
Length of Stay According to Age Shown as Proportion of Patients.
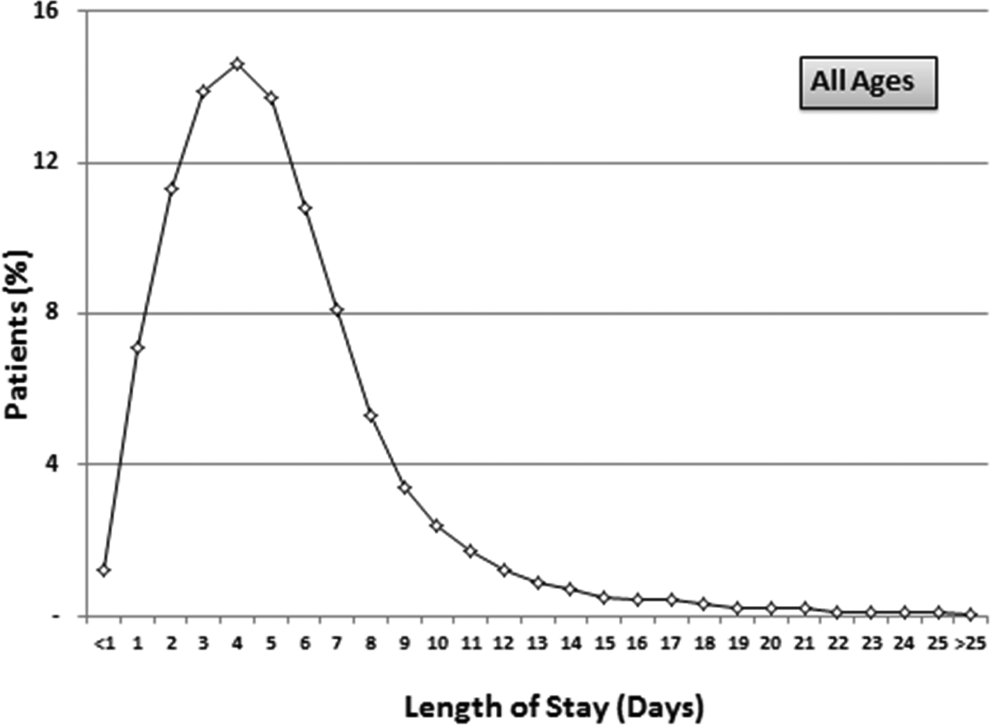
Proportion of stable patients with pulmonary embolism and length of stay (days).
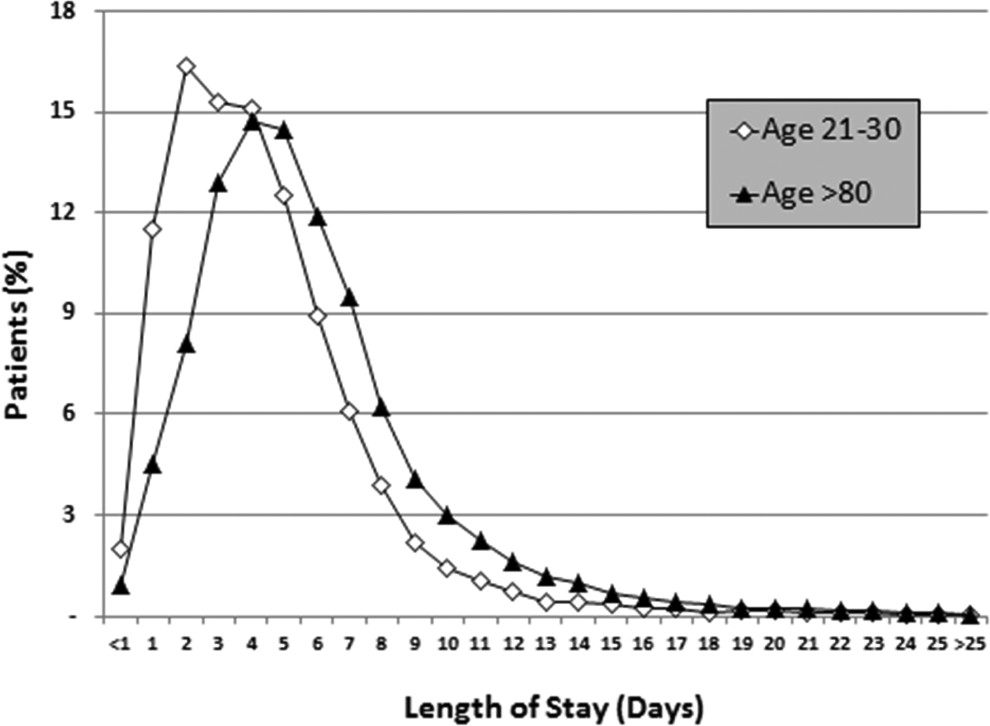
Length of stay according to whether aged 21 to 30 years or older than 80 years.
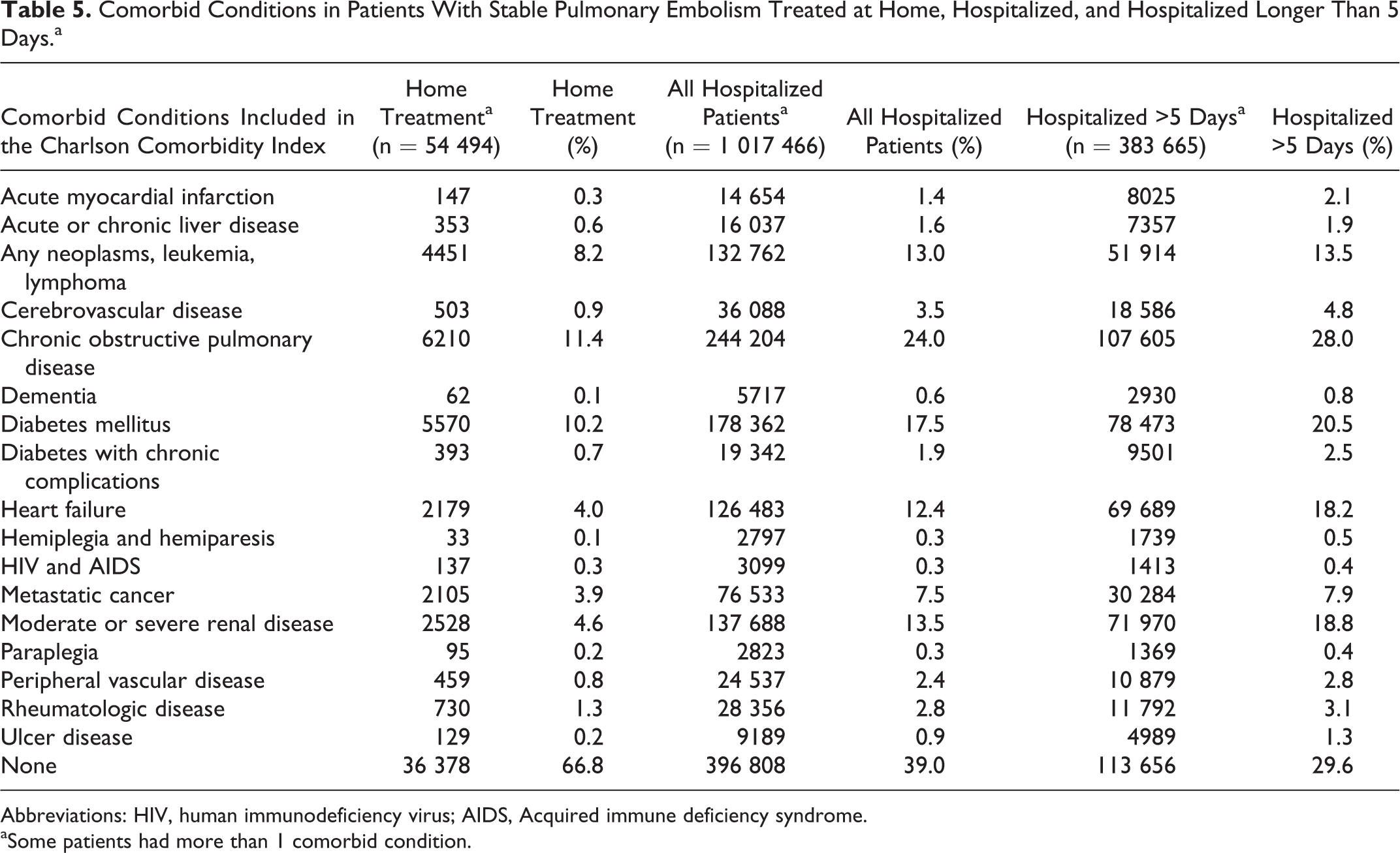
The majority of patients (66.8%) who received home treatment had none of the comorbid conditions listed in the Charlson comorbidity index (Table 5). Among hospitalized patients, 39.0% had no comorbid conditions and 29.6% of those hospitalized >5 days had no comorbid conditions. Among those who received home treatment, the most prevalent comorbid conditions were chronic obstructive pulmonary disease, 11.4%, diabetes mellitus, 10.2%, and neoplasms, 8.2% (Table 5). These conditions were present in 13.0% to 24.0% of hospitalized patients, as well as heart failure, 12.4%, and moderate or severe renal disease 13.5% (Table 5). The same comorbid conditions were most prevalent in patients hospitalized >5 days, but the prevalence of these comorbid conditions was higher.
Comorbid Conditions in Patients With Stable Pulmonary Embolism Treated at Home, Hospitalized, and Hospitalized Longer Than 5 Days.a
Abbreviations: HIV, human immunodeficiency virus; AIDS, Acquired immune deficiency syndrome.
aSome patients had more than 1 comorbid condition.
Discussion
From 2007 to 2012, only 6.0% of stable patients with a primary diagnosis of pulmonary embolism were treated entirely at home. The proportion treated at home tended to increase from 2007 to 2012. The proportion of patients treated at home was age-dependent and higher in younger patients than in elderly patients. The majority of patients treated at home had no comorbid conditions. Discharge in ≤1 day was in 8.3%. In-hospital all-cause mortality was 2.6% and it too was age-dependent.
Investigations of outpatient treatment of acute pulmonary embolism have been reported since 2000. 2 Review identified 1374 low-risk patients with pulmonary embolism who were treated entirely as outpatients, 2 –15 102 who were hospitalized ≤24 hours, 3,10,12 and 297 patients who were treated either at home or after ≤24 hours hospitalization. 16 Among these patients, death from pulmonary embolism occurred in 0.06% and nonfatal recurrent pulmonary embolism occurred in 1.5%. Fatal bleeding occurred in 0.11% and nonfatal major bleeding occurred in 1.5%. Typical exclusions were patients in shock, those who required oxygen, parenteral treatment for pain, and those with concomitant medical conditions. The Pulmonary Embolism Severity Index (PESI) score, 24 the simplified PESI score, 25 the Geneva Score, 26 multimarker models, 27,28 and other scoring systems 29 –31 assist in identifying low-risk patients.
A retrospective cohort study of 746 stable patients with pulmonary embolism diagnosed in 5 emergency departments, January 2013 to December 2014, showed a low prevalence of home treatment of stable patients, as shown in the present investigation. 32 The prevalence of home treatment was even lower than what we observed in the present investigation, 1.7%. Excluded patients were those who were hypotensive (systolic blood pressure <90 mm Hg), on vasopressors, on ventilator support, or had an arterial oxygen saturation of ≤90%. Discharge in ≤2 days was in 119 (16.2%) of 733 patients. Treatment of those treated entirely at home was with novel oral anticoagulants in 4 (30.8%) of 13 patients, and in those discharged in ≤2 days, novel oral anticoagulants were prescribed only for 34 (28.6%) of 119 patients. 32
The oral factor Xa inhibitors rivaroxaban and apixaban were approved for the treatment of deep venous thrombosis and pulmonary embolism by the US Food and Drug Administration on November 2, 2012, and August 21, 2014, respectively. 33,34 Therefore, the impact, if any, of home treatment with these drugs would not be shown in our data. A large proportion of the patients in the future may not be chosen for outpatient treatment, irrespective of the availability of novel oral anticoagulants, because of the need for prolonged hospital stay. Over one-third of patients in the present investigation were hospitalized 6 days or longer, indicating that early discharge in those patients was not discouraged by the difficulty of administering anticoagulants at home. Among those older than 80 years, 44% were hospitalized 6 days or longer, indicating that novel oral anticoagulant would not have impacted the length of stay in a large proportion of such elderly patients.
Strengths of this investigation are the large number of patients of both genders and all races from all regions of the United States. With the large number of patients, it was possible to show trends in the prevalence of home treatment, the proportion who received home treatment according to age, and the proportion who died in hospital according to age.
A weakness of this investigation is the inability to obtain outcome information on patients who received home treatment. As with all administrative data, the accuracy of coding may be questioned. Trends were clear, however, and coding errors would have affected the trends minimally, if at all. Finally, the number of patients hospitalized with stable acute pulmonary embolism differed by 19.6% according to whether data were from the NEDS or the National Hospital Discharge Survey. We believe that this difference is of no consequence and would not have affected the results in a substantive fashion.
Conclusion
Home treatment and early discharge of stable patients with a primary diagnosis of pulmonary embolism were selected in only a small proportion of patients. Deaths in hospital were less frequent among younger patients. In view of the lower death rate among younger patients, they might be a group in whom home treatment would be more advantageous than in elderly patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.