Increased d-dimer is indicative of a hypercoagulable state and found to be associated with acute coronary syndromes. The present study aimed to evaluate whether plasma d-dimer levels could predict subsequent major clinical events in patients with coronary artery disease (CAD). First, 2209 angiographic-proven patients with CAD were consecutively enrolled. Then, all patients were subjected to follow up for an average of 18 months (ranged from 14 to 1037 days). The relationships of the plasma d-dimer with the severity of CAD and future clinical outcomes were evaluated. We found that plasma d-dimer was higher in patients with prior myocardial infarction (MI) than that in patients with nonprior MI (P = .006). Multivariate linear regression analysis suggested that the plasma d-dimer was linked to the severity of CAD assessed by Gensini score (β = 0.052, 95% confidence interval [CI]: 1.20-6.84, P = .005) even after adjusting for confounding factors. During the follow-up, 42 patients underwent prespecified outcomes. After adjustment for multiple variables in the Cox regression model, the d-dimer levels remained to be a potential predictor of total outcome (hazard ratio = 1.22, 95% CI: 1.09-1.37, P = .001). Therefore, plasma d-dimer levels appeared to be a useful predictor for the severity of CAD and the subsequent major clinical events.
Acute coronary syndrome (ACS) usually results from thrombosis of atherosclerotic plaque rupture, therefore, it has been proposed the circulating markers that reflect activated coagulation and fibrinolysis may be linked with the pathogenesis of coronary artery disease (CAD).1,2d-Dimer is a product of the degradation of cross-linked fibrin, and its plasma levels reflect active fibrin formation and degradation.3 D-Dimer together with circulating tissue plasminogen activator antigen and von Willebrand factor, and other markers have been paid much attention on cardiac events.4,5 Meanwhile, d-dimer has been concerned in stoke events field.6
Actually, the concentrations of d-dimer were demonstrated to remain elevated for several months after acute myocardial infarction (AMI), suggesting that the patients with AMI had an enhanced coagulable state.7 Meanwhile, such an enhanced coagulable state is associated with myocardial infarction (MI) and mortality.8 Thus, d-dimer as an indicator of coagulable state might be a useful biomarker in predicting cardiovascular ischemic events.9 Indeed, several previous studies suggested a positive association of the d-dimer levels with CAD and stoke risk in essentially general and secondary prevention populations,6,9–11 while other reports indicated that the plasma d-dimer was not always a useful predictor of major adverse cardiovascular events (MACE) in cardiovascular diseases.12,13 Nevertheless, most of previous studies did not indicate whether anticoagulant drugs such as heparin was used in the enrolled study participants. Prior study showed that heparin could influence d-dimer level,14 which might influence the predicted value of d-dimer in CAD clinical outcome.
Therefore, in the present study, we aimed to estimate whether plasma d-dimer levels were associated with MI and the extent of CAD assessed by 2 different coronary assessment systems (number of stenosed coronary vessels and Gensini score [GS])15 in patients without anticoagulant treatment on admission. Furthermore, we sought to gather evidence evaluating the value of the d-dimer baseline level to predict subsequent clinical outcome in patients with CAD for an average of 18 months follow-up.
Materials and Methods
Study Population
This was a single-center, prospective follow-up study. From April 2011 to March 2014, a total of 2410 patients with angiographic-proven CAD (>50% diameter stenosis of at least 1 major coronary artery) (74.1% men) aged 22 to 84 years (average age: 58.58 years) were consecutively enrolled. Patients with malignancy, significant hematologic (anemia, thrombocytopenia, leukocytosis, leukemia) and febrile disorders (body temperature more than 38°C), and anticoagulant therapy (heparin, low-molecular-weight heparin, warfarin) before admission were excluded from the present study. Data including the demographic, clinical, laboratory findings, and angiographic examination were collected. The protocol of this study was approved by Fu Wai hospital ethics committee and complied with the Declaration of Helsinki (Fu Wai Hospital & National Center for Cardiovascular Diseases, Beijing, China). The informed consents were obtained from all participants.
Diagnostic Criteria
Diabetes mellitus (DM) was diagnosed in patients with fasting glucose level of >6.99 mmol/L by multiple determinations, 2-hour plasma glucose ≥200 mg/dL (11.1 mmol/L) during an oral glucose tolerance test, HbA1C ≥6.5% or under active treatment with insulin, or oral hypoglycemic agents.16 Body mass index was calculated by dividing the weight (kg) of an individual by the square of his or her height (m). Coronary artery disease was defined as the presence of significant obstructive stenosis, at least 50% of the vessel lumen diameters, in any of the main coronary arteries by at least 2 independent senior interventional cardiologists based on quantity coronary angiography. Myocardial infarction was diagnosed according to the World Health Organization criteria including AMI and old MI.17
Laboratory Measurements
The laboratory measurements in the present study were conducted by the clinical chemistry department of Fu Wai hospital. Blood samples of the patients were obtained at 7:00 am in the next morning of the day of admission from the cubital vein after a 12-hour overnight fast at rest state. The blood was collected into EDTA-containing tubes and stored at 4°C until transport for detection within 1 hour. Concentrations of total cholesterol (TC) and triglyceride (TG) were measured using enzymatic methods and high-density lipoprotein cholesterol by a direct method (Roche Diagnostics, Basel, Switzerland). Low-density lipoprotein cholesterol (LDL-C) was obtained by Friedewald’s formula (if fasting TGs < 3.39 mmol/L) or by ultracentrifugation. Levels of high-sensitivity C-reactive protein (hs-CRP) were determined using immunoturbidimetry (Beckmann Assay, Bera, California). White blood cell count was also determined after admission by the automated hematology analyzer XE-1200 (Sysmex, Kobe, Japan). Plasma d-dimer levels were measured using immunoassays turbidimetry (STA Compact Diagnostica Stago assay instrument, France) where the intra-assay coefficient of variation was 8.37% and the interassay coefficient of variation was 10.46%. Samples for determination of d-dimer were centrifuged immediately, and the results collected are expressed in micrograms per milliliter (µg/mL). The normal reference range of plasma d-dimer is less than 0.5 µg/mL, as recommended by the manufacturer. All other included biomarkers were analyzed by standard hematological and biochemical tests.
Severity Assessment of Coronary Atherosclerosis
The first assessment of the severity of CAD was based on number of stenosed coronary vessels. Patients were grouped as: 1 (single-vessel disease), 2 (2-vessel disease), and 3 (3-vessel disease and/or left main stem disease).
The second method was GS assessment. The GS was computed by assigning a severity score to each coronary stenosis according to the degree of luminal narrowing and its geographic importance. Two experienced cardiologists who were blinded to the study protocol and each other’s interpretation calculated GS from initial angiograms. First, reduction in lumen diameter and angiographic appearance of concentric lesions and eccentric plaques were evaluated. Reductions in 25%, 50%, 75%, 90%, 99%, and complete occlusion were assigned as 1, 2, 4, 8, 16, and 32, respectively. Second, a multiplier was assigned to each main vascular segment based on the functional significance of the myocardial area supplied by that segment: 5 for the left main coronary artery, 2.5 for the proximal segment of the left anterior descending (LAD) coronary artery, and the proximal segment of the circumflex artery, 1.5 for the mid-segment of the LAD, 1.0 for the right coronary artery, the distal segment of the LAD, mid-distal region of the circumflex artery, the posterolateral artery, and the obtuse marginal artery, and 0.5 for small segments.15,18
Follow-Up
The study nurses who were blinded to the study protocol conducted the standardized telephone interviews and collected follow-up data after 6, 12, 24, and 36 months. Once patients reported that they had been hospitalized, appropriate hospital records were consulted. The prespecified clinical end points were defined as cardiac death, nonfatal MI, recurrence of MI, and stroke. Death of a patient was reported by relatives or the general practitioners who treated the patient. Three experienced physicians who were masked to any of the study data independently classified the event.
Statistical Analysis
The values were expressed as the mean ± standard deviation or median (Q1-Q3 quartiles) for the continuous variables and as the number (percentage) for the categorical variables. Values of d-dimer, TG, hs-CRP, and N-terminal probrain natriuretic peptide levels were logarithm transformed to normalize their distributions. Continuous variables and categorical variables were analyzed by the chi-square statistic tests, the one-way analysis of variance test, or the t test when appropriate. The relationship of the d-dimer levels with GS was evaluated by univariate and multivariate linear regression models (including potential factors such as age, gender, DM, hypertension (HT), smoking, and lipid profile) using forward stepwise selection process. The association of the d-dimer levels with outcomes was determined with Cox proportional hazard models using forward stepwise selection process. Event-free survival curves were constructed using the Kaplan-Meier methods and compared using log-rank test. A P value < .05 was considered statistically significant. The statistical analysis was performed with SPSS version 19.0 software (SPSS Inc, Chicago, Illinois).
Results
Baseline Characteristics
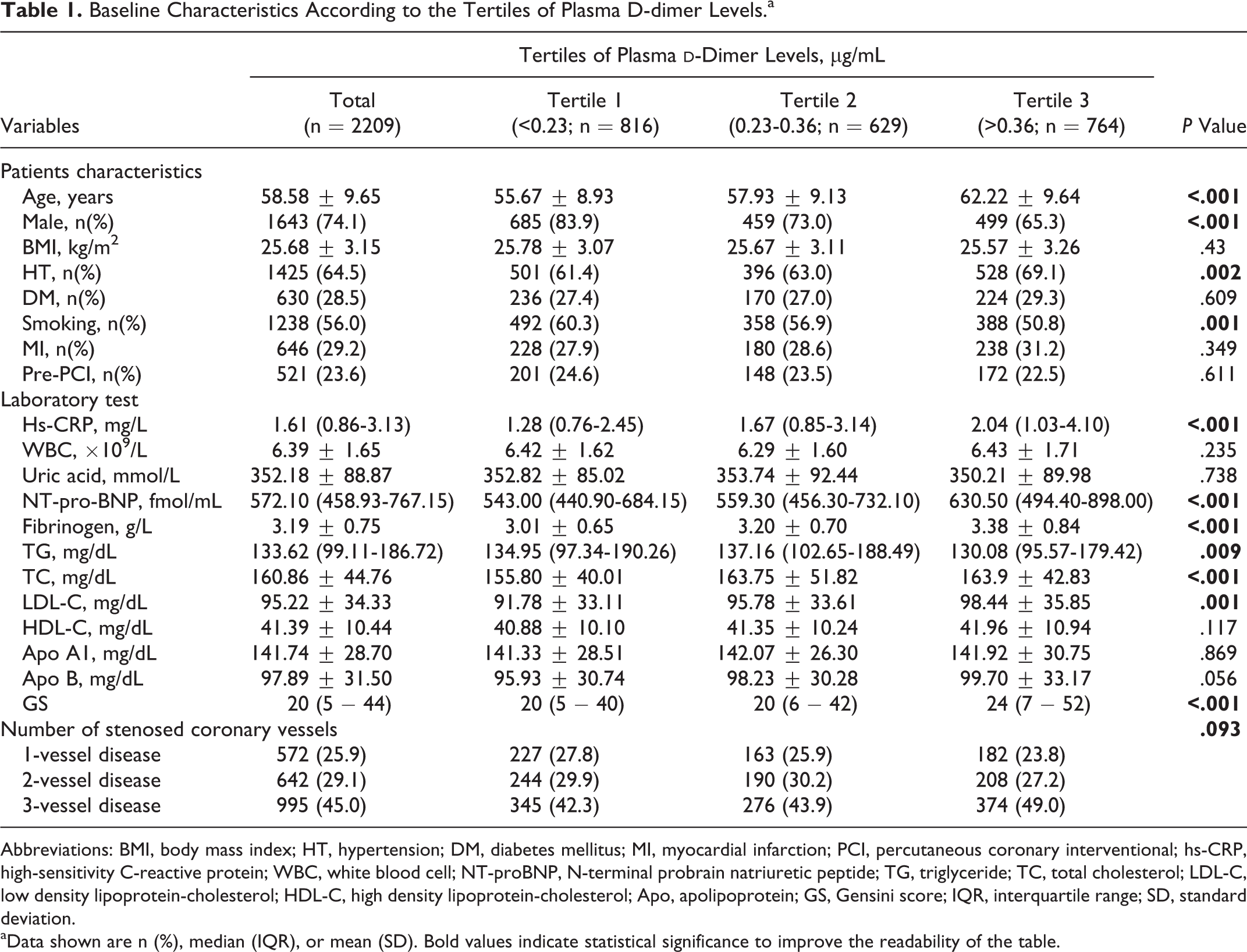
Of 2410 consecutive patients who underwent selective coronary angiography, 2209 (91.7%) patients were followed up. The baseline demographic, clinical characteristics, and laboratory findings were summarized according to tertiles of the plasma d-dimer levels (tertile 1 < 0.23 μg/mL, n = 816; tertile 2, 0.23-0.36 μg/mL, n = 629; tertile 3 > 0.36 μg/mL, n = 764) in Table 1. As shown in Table 1, patients with higher d-dimer levels were older than that with lower levels, and patients had the higher proportion of females and history of HT with increasing tertiles of plasma d-dimer. However, the inverse relationship of the d-dimer tertiles with the prevalence of smoking and patients with pre- percutaneous coronary interventions (PCI) were found. In addition, the markers of inflammation including hs-CRP and fibrinogen levels were increasing with the tertiles of the plasma d-dimer, and TG was significantly lower but TC and LDL-C were higher with increasing tertiles of the plasma d-dimer. Importantly, patients with the higher levels of d-dimer were accompanied by high GS. Furthermore, prior patients with MI were with a higher d-dimer compared with nonprior patients with MI (0.42 ± 0.48 μg/mL vs 0.38 ± 0.64 μg/mL, P = .006).
Baseline Characteristics According to the Tertiles of Plasma D-dimer Levels.a
Variables
Tertiles of Plasma d-Dimer Levels, μg/mL
P Value
Total (n = 2209)
Tertile 1 (<0.23; n = 816)
Tertile 2 (0.23-0.36; n = 629)
Tertile 3 (>0.36; n = 764)
Patients characteristics
Age, years
58.58 ± 9.65
55.67 ± 8.93
57.93 ± 9.13
62.22 ± 9.64
<.001
Male, n(%)
1643 (74.1)
685 (83.9)
459 (73.0)
499 (65.3)
<.001
BMI, kg/m2
25.68 ± 3.15
25.78 ± 3.07
25.67 ± 3.11
25.57 ± 3.26
.43
HT, n(%)
1425 (64.5)
501 (61.4)
396 (63.0)
528 (69.1)
.002
DM, n(%)
630 (28.5)
236 (27.4)
170 (27.0)
224 (29.3)
.609
Smoking, n(%)
1238 (56.0)
492 (60.3)
358 (56.9)
388 (50.8)
.001
MI, n(%)
646 (29.2)
228 (27.9)
180 (28.6)
238 (31.2)
.349
Pre-PCI, n(%)
521 (23.6)
201 (24.6)
148 (23.5)
172 (22.5)
.611
Laboratory test
Hs-CRP, mg/L
1.61 (0.86-3.13)
1.28 (0.76-2.45)
1.67 (0.85-3.14)
2.04 (1.03-4.10)
<.001
WBC, ×109/L
6.39 ± 1.65
6.42 ± 1.62
6.29 ± 1.60
6.43 ± 1.71
.235
Uric acid, mmol/L
352.18 ± 88.87
352.82 ± 85.02
353.74 ± 92.44
350.21 ± 89.98
.738
NT-pro-BNP, fmol/mL
572.10 (458.93-767.15)
543.00 (440.90-684.15)
559.30 (456.30-732.10)
630.50 (494.40-898.00)
<.001
Fibrinogen, g/L
3.19 ± 0.75
3.01 ± 0.65
3.20 ± 0.70
3.38 ± 0.84
<.001
TG, mg/dL
133.62 (99.11-186.72)
134.95 (97.34-190.26)
137.16 (102.65-188.49)
130.08 (95.57-179.42)
.009
TC, mg/dL
160.86 ± 44.76
155.80 ± 40.01
163.75 ± 51.82
163.9 ± 42.83
<.001
LDL-C, mg/dL
95.22 ± 34.33
91.78 ± 33.11
95.78 ± 33.61
98.44 ± 35.85
.001
HDL-C, mg/dL
41.39 ± 10.44
40.88 ± 10.10
41.35 ± 10.24
41.96 ± 10.94
.117
Apo A1, mg/dL
141.74 ± 28.70
141.33 ± 28.51
142.07 ± 26.30
141.92 ± 30.75
.869
Apo B, mg/dL
97.89 ± 31.50
95.93 ± 30.74
98.23 ± 30.28
99.70 ± 33.17
.056
GS
20 (5 − 44)
20 (5 − 40)
20 (6 − 42)
24 (7 − 52)
<.001
Number of stenosed coronary vessels
.093
1-vessel disease
572 (25.9)
227 (27.8)
163 (25.9)
182 (23.8)
2-vessel disease
642 (29.1)
244 (29.9)
190 (30.2)
208 (27.2)
3-vessel disease
995 (45.0)
345 (42.3)
276 (43.9)
374 (49.0)
Abbreviations: BMI, body mass index; HT, hypertension; DM, diabetes mellitus; MI, myocardial infarction; PCI, percutaneous coronary interventional; hs-CRP, high-sensitivity C-reactive protein; WBC, white blood cell; NT-proBNP, N-terminal probrain natriuretic peptide; TG, triglyceride; TC, total cholesterol; LDL-C, low density lipoprotein-cholesterol; HDL-C, high density lipoprotein-cholesterol; Apo, apolipoprotein; GS, Gensini score; IQR, interquartile range; SD, standard deviation.
aData shown are n (%), median (IQR), or mean (SD). Bold values indicate statistical significance to improve the readability of the table.
Association of d-Dimer and the Extent of CAD
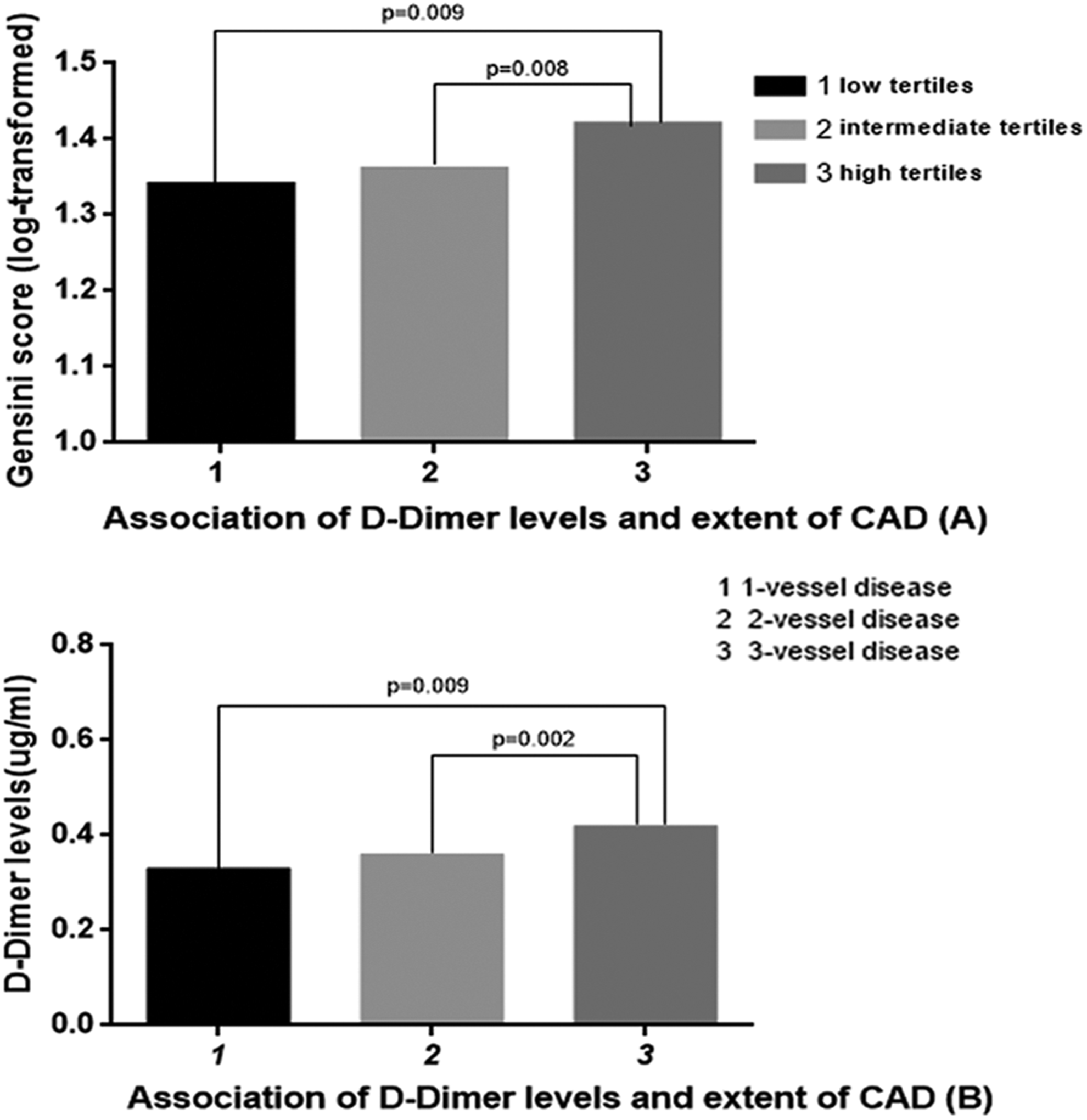
The median (Q1-Q3 quartiles) of GS was 20 (5-44). The percentage of 1-vessel disease, 2-vessel disease, and 3-vessel disease of stenosed coronary was 25.9%, 29.1%, and 45.0%. Although there was no statistically significant correlation between the d-dimer tertile and the number of stenosed coronary vessel (chi-square for trend, P = .093, Table 1), GS was significantly different from the tertiles of the d-dimer levels (P < .001, Table 1, Figure 1A), and the difference was strong especially between high tertiles and low-mid tertiles. In addition, the d-dimer concentrations were also different from the groups with various numbers of stenosed coronary vessel (Figure 1B), especially comparing with groups of 1-vessel disease and 3-vessel disease.
Association of d-dimer levels with extent of CAD. GS assessment was significant statistical difference between the tertiles of d-dimer (Figure 1A). In addition, continuous variable of d-dimer concentration was different between numbers of stenosed coronary vessel groups (Figure 1B).
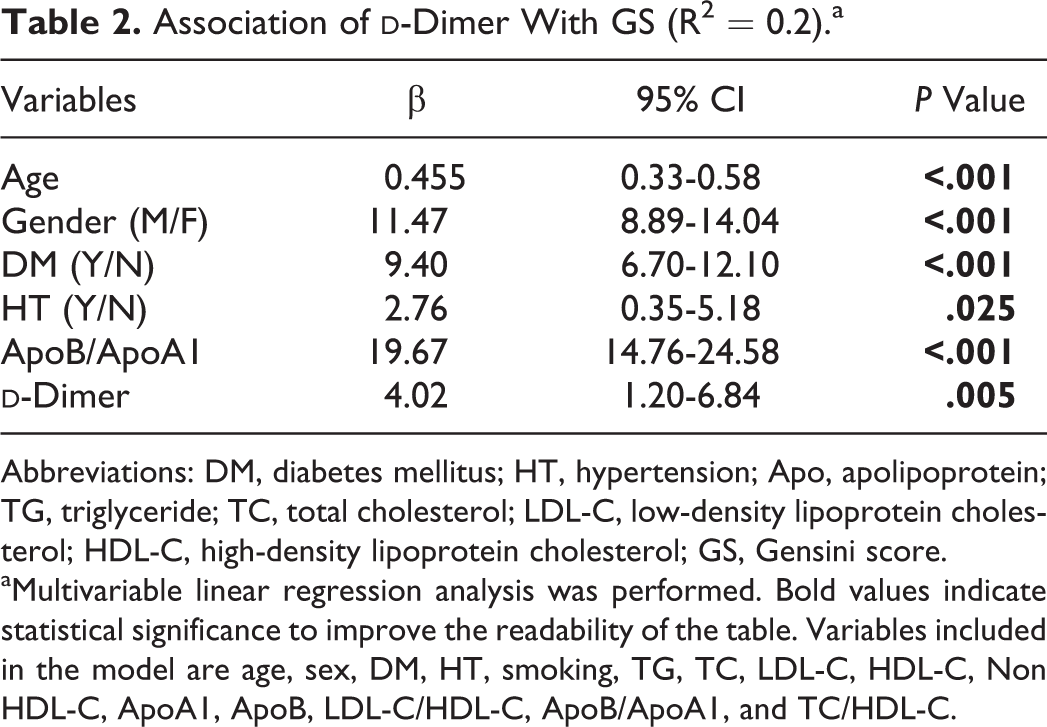
The multivariate linear regression analysis showed that the plasma d-dimer level was a potential predictor of GS after adjustment for conventional risk factors of CAD (β = 4.02, 95% confidence interval [CI]: 1.20-6.84, P = .005, Table 2).
aMultivariable linear regression analysis was performed. Bold values indicate statistical significance to improve the readability of the table. Variables included in the model are age, sex, DM, HT, smoking, TG, TC, LDL-C, HDL-C, Non HDL-C, ApoA1, ApoB, LDL-C/HDL-C, ApoB/ApoA1, and TC/HDL-C.
d-Dimer for Predicting Subsequent Outcomes
The population of the present study was followed up for an average of 18 months (ranged from 14 to 1037 days). During the follow-up, 42 patients had adverse outcome. Seventeen patients had MI and 16 patients had stoke, while 9 patients had fatal cardiac death.
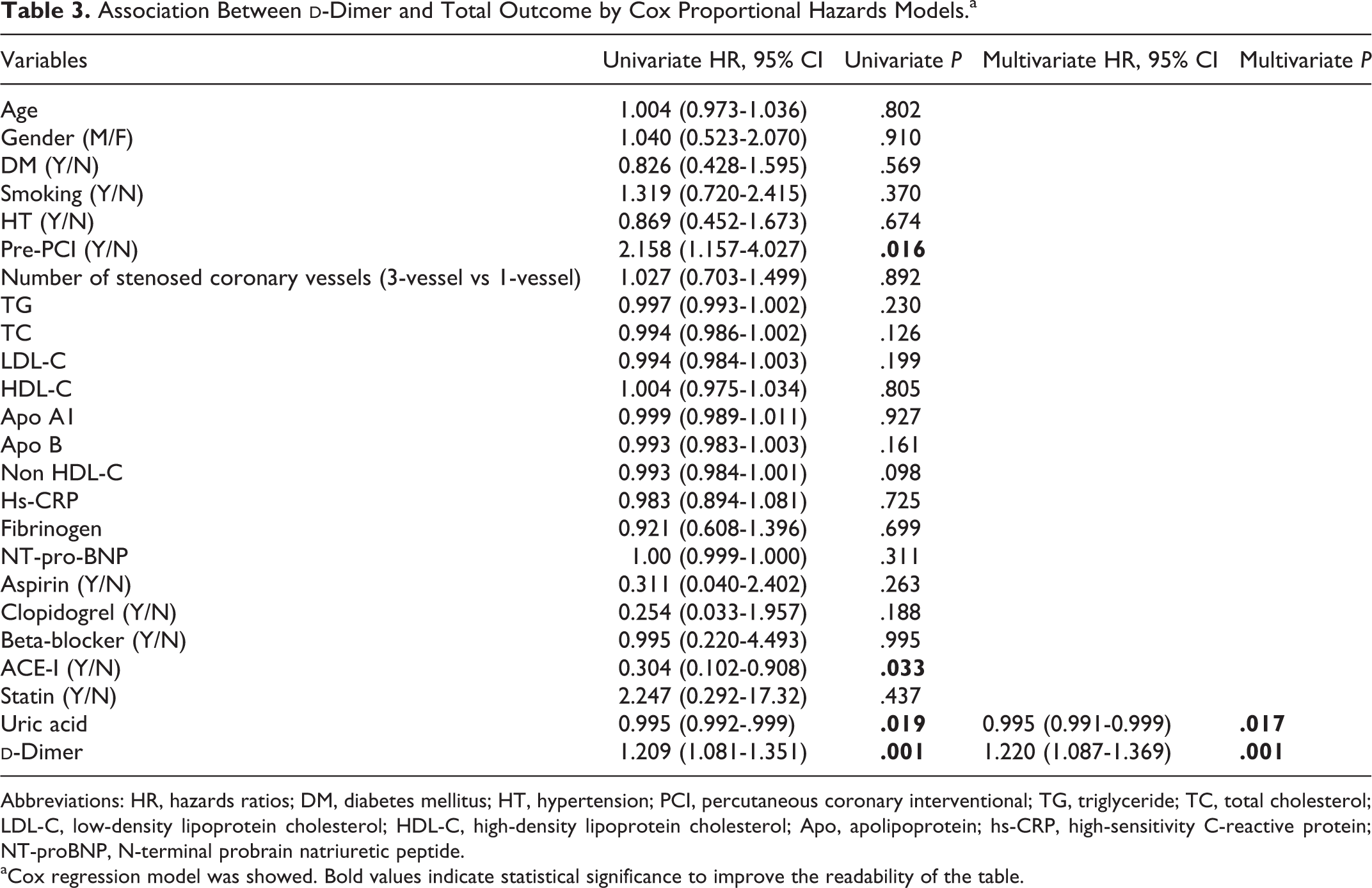
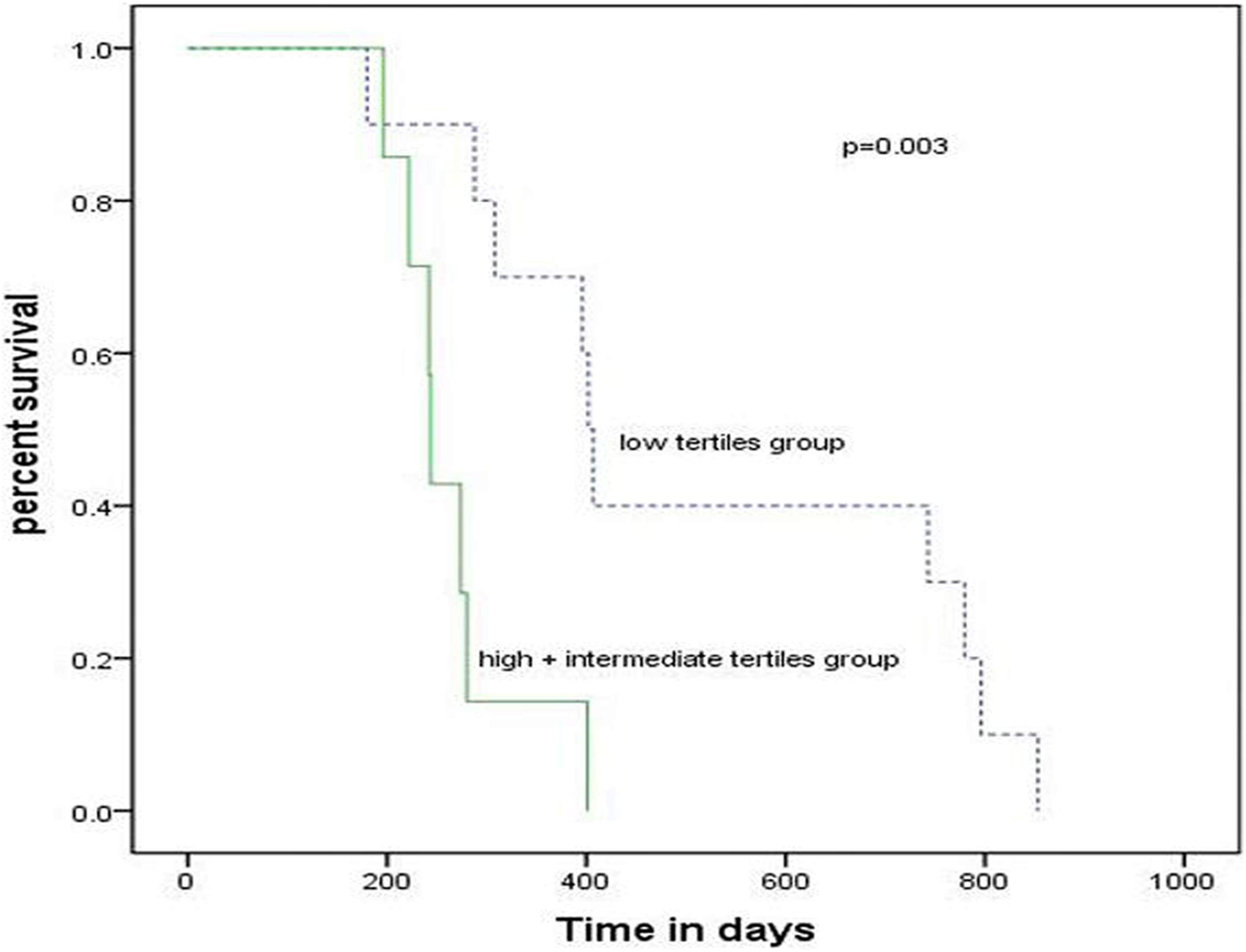
There was an association between baseline plasma d-dimer levels and incidence of total outcome and MI (P = .001 and P = .015, respectively) but not for stoke or cardiac death independently (P = .99 and P = .548, respectively). After adjustment for multiple variables including age, gender, cardiovascular risk factors, and medicine treatment, the d-dimer levels remained to be an independent predictor of total outcome (hazard ratio [HR] = 1.22, 95% CI: 1.09-1.37, P = .001; Table 3) suggested by the Cox regression model. Kaplan-Meier curves for cumulative event-free survival of MI based on the tertiles of baseline d-dimer were presented in Figure 2. The total number of patients who were experienced an MI only 17 (of 2209), that was 0.77%. In mid-high tertile group (d-dimer > .23 μg/mL), the number of patients with an MI was 10; and in low tertile group (d-dimer < .23 μg/mL), the number of patients was 7. Elevated plasma d-dimer levels were generally associated with increased adverse outcome (P = .003).
Association Between d-Dimer and Total Outcome by Cox Proportional Hazards Models.a
Variables
Univariate HR, 95% CI
Univariate P
Multivariate HR, 95% CI
Multivariate P
Age
1.004 (0.973-1.036)
.802
Gender (M/F)
1.040 (0.523-2.070)
.910
DM (Y/N)
0.826 (0.428-1.595)
.569
Smoking (Y/N)
1.319 (0.720-2.415)
.370
HT (Y/N)
0.869 (0.452-1.673)
.674
Pre-PCI (Y/N)
2.158 (1.157-4.027)
.016
Number of stenosed coronary vessels (3-vessel vs 1-vessel)
aCox regression model was showed. Bold values indicate statistical significance to improve the readability of the table.
Kaplan-Meier curve for cumulative event-free survival of MI based on tertiles of baseline plasma d-dimer levels. The total number of patients who were experienced an MI only 17 (of 2209) that was 0.77%. In mid-high tertile group (d-dimer > 0.23 μg/mL), the number of patients with an MI was 10; and in low tertile group (d-dimer < 0.23 μg/mL), the number of patients was 7. Elevated plasma d-dimer levels were generally associated with increased adverse outcome (P = .003).
Discussion
Although the clinical implication of d-dimer in cardiovascular medicine has intensively been investigated, whether the plasma D-dimer level is a useful predictor for the severity and outcome in patients with CAD has less been examined, especially in a large cohort of populations. In our prospective, short-term follow-up study, the data suggested that higher baseline plasma d-dimer levels were associated with the severity of coronary stenosis and poor outcome in patients with CAD.
d-Dimer and Other Risk Factors of CAD
d-Dimer is a product of the degradation of cross-linked fibrin and its plasma levels reflect both fibrin formation and degradation. Because of its potential to identify individuals with a hypercoagulable state, d-dimer was considered to be a useful biomarker worthy of continued attention.6,9–11 Mills et al found that d-dimer levels were significantly correlated with age, r = .32 and .40 (P = .01), and fibrinogen, r = .24 and .29 (P = .01) in patients with premature CAD and the controls, respectively.10 Kikkert et al found that the independent predictors for a high d-dimer level (> 0.71 μg/mL) were age, female, longer total ischemic time, and a history of heart failure.9
In consistent with the previous studies, our data suggested that baseline d-dimer levels were largely linked with age, female, and other cardiovascular risk factors including hs-CRP and fibrinogen (P < .001, all) in Chinese patients with CAD.
d-Dimer and the Severity of Coronary Stenosis
Alterations of the hemostasis and disturbances of fibrinolysis are detectable during the chronic phase of atherosclerosis.19 Thrombus formation at the site of atherosclerotic lesions, especially on a ruptured plaque, plays a central role in the “atherothrombosis.”19 However, a small sample size (305 patients with CAD) did not support d-dimer levels in association with the severity of CAD evaluated by the diseased number of coronary arteries but with the presence of CAD in patients with stable angina pectoris.11 To be inconsistent, in our large population study (n = 2209), we found that the elevated tertile of d-dimer levels were significantly associated with increased coronary stenosis using GS assessment. Also, the plasma d-dimer levels increased with the severity of CAD evaluated by the diseased number of coronary arteries. More interestingly, a novel finding using multivariate linear regression analysis showed that the plasma d-dimer level was an independent predictor of high GS after adjustment for conventional risk factors of CAD. The explanation between our finding and prior study may be that the severity of coronary stenosis could be strongly influenced by different coagulation factors in addition to different d-dimer level and sample size.20
Value of d-Dimer as a Predictor of Severity in CAD
The specificity of d-dimer for cardiovascular disease is debatable. Koenig et al studied 312 patients with stable angina pectoris and 477 healthy controls, and found that plasma d-dimer levels were strongly and independently associated with the presence of stable angina pectoris.11 A large, prospective studies in elderly population performed by Alehagen et al showed that d-dimer concentration had a value for predicting future AMI (odds ratio [OR]: 2.5) and cardiovascular death (OR: 4.0).19 Another study done in postmenopausal women indicated that d-dimer was independently associated with the occurrence of cardiac events (OR: 2.0).19 In a study of 257 participants with chest pain, authors found that raised d-dimer had an independent diagnostic value for AMI (positive and negative predictive values estimated as 92% and 41%, respectively) and increased the diagnostic sensitivity of the electrocardiogram and history from 73% to 92%.21 Moreover, Tokita et al found that d-dimer showed significantly higher positive test rate for the detection of ACS in the very early phase compared with troponin T and therefore they concluded that the d-dimer was regarded useful for the screening of ACS in the emergency setting.22 In contrast, Itakura et al reported that d-dimer did not distinguish patients presenting with AMI from those with stable angina.19 Another 2 large prospective studies suggested that d-dimer did not aid detection of ACS or predict prognosis above and beyond established risk factors.19 In the present study, our data suggested that the plasma level of d-dimer in patients with MI were higher than that in patients with stable CAD (0.42 ± 0.48 vs 0.38 ± 0.64, P = .006). But the specific value of d-dimer in predicting MI is still needed to be explored.
The Value of d-Dimer as a Predictor of MACE on CAD Population
The role of d-dimer in predicting outcomes are still conflicting in patients with established CAD. Previously, data from 3209 participants in the Framingham study indicated that plasma d-dimer was not predictive for MACE.12 In the Multiethnic Study of Atherosclerosis, the results suggested that elevated d-dimer levels were related to increased risk of death but not nonfatal cardiovascular events in more than 6000 individuals.19 A up-to-date meta-analysis conducted by Kleinegris et al showed that an increased d-dimer appeared to be independently associated with a 2-time increased risk of near-term cardiovascular events (relative risk 2.30, 95% CI 1.43-3.68),23 which refers to the cardiovascular events in the near-term period following the baseline characteristics measurement. Generally, the period which called near term is with a median follow-up of 2 to 4 years.
Furthermore, Kikkert et al suggested that high d-dimer levels at discharge were associated with a higher risk of MACE and non-coronary artery bypass graft major bleeding in patients with ST-segment elevation myocardial infarction undergoing PCIs.9 In our study, we found that higher d-dimer baseline levels on admission were related to a higher risk of MACE in patients without anticoagulant drugs. Of note, data suggested that after adjustment for multiple variables including age, gender, cardiovascular risk factors, and medicine treatment, d-dimer remained to be an independent predictor of total outcome (HR = 1.22, 95% CI: 1.09-1.37, P = .001). Additionally, previous studies showed that higher d-dimer level was at higher risk of CAD events, even if they are receiving oral anticoagulants in patients with atrial fibrillation,24–26 which also support our finding.
There are several limitations in our study. First, the present study is a single-center study. Second, short-term follow-up may be another limitation. Third, d-dimer level is easy to vary under different status, whereas we just investigated whether the baseline level of d-dimer was a predictor of short-term outcome in patients with CAD. Fourthly, although some patients with MI did not take anticoagulant drugs prior to admission, they might take oral anticoagulant drugs after admission, so whether the drugs could affect analysis did not exclude. Additionally, the sample is relatively small. Despite these limitations, our results still have a potential clinical significance and merit further researches.
Conclusion
In conclusion, in this prospective and short-term outcome study, the data clearly suggested that the level of plasma d-dimer was an independent predictor of the severity of CAD as well as the future outcome for patients with CAD. Apparently, a long-term follow-up and a larger population may be needed in the further to reveal more information regarding the role of d-dimer in CAD.
Footnotes
Authors’ Note
The first two authors, Ping Gong and Sheng-Hua Yang, contributed equally to this study. Gong P and Li S completed the project, and analyzed the data, and wrote the manuscript. Li J-J established the study, interpreted the data, and contributed to reviewed/edited the manuscript. The other coauthors for this manuscript contributed to collect the data.
Acknowledgments
We thank the staff and participants of this study for their important contributions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partly supported by National Natural Scientific Foundation (81070171, 81241121), Specialized Research Fund for the Doctoral Program of Higher Education of China (20111106110013), Capital Special Foundation of Clinical Application Research (Z121107001012015), Capital Health Development Fund (2011400302), and Beijing Natural Science Foundation (7131014) awarded to Dr Jian-Jun Li, MD, PhD.
References
1.
BorissoffJISpronkHMten CateH. The hemostatic system as a modulator of atherosclerosis. N Engl J Med. 2011;364(18):1746–1760.
2.
LoweGD. Can haematological tests predict cardiovascular risk? The 2005 Kettle Lecture. Br J Haematol. 2006;133(3):232–250.
3.
LipGYLoweGD. Fibrin D-dimer: a useful clinical marker of thrombogenesis?Clin Sci (Lond). 1995;89(3):205–214.
4.
WilleitPThompsonAAspelundT. Hemostatic factors and risk of coronary heart disease in general populations: new prospective study and updated meta-analyses. PLoS One. 2013;8(2):e55175.
5.
GorogDA. Prognostic value of plasma fibrinolysis activation markers in cardiovascular disease. J Am Coll Cardiol. 2010;55(24):2701–2709.
MerliniPABauerKAOltronaL. Persistent activation of coagulation mechanism in unstable angina and myocardial infarction. Circulation. 1994;90(1):61–68.
8.
MeadeTWMellowsSBrozovicM. Haemostatic function and ischaemic heart disease: principal results of the Northwick Park Heart Study. Lancet. 1986;2(8506):533–537.
9.
KikkertWJClaessenBEStoneGW. D-dimer levels predict ischemic and hemorrhagic outcomes after acute myocardial infarction: a HORIZONS-AMI biomarker substudy. J Thromb Thrombolysis. 2014;37(2):155–164.
10.
MillsJDMansfieldMWGrantPJ. Tissue plasminogen activator, fibrin D-dimer, and insulin resistance in the relatives of patients with premature coronary artery disease. Arterioscler Thromb Vasc Biol. 2002;22(4):704–709.
11.
KoenigWRothenbacherDHoffmeisterAGriesshammerMBrennerH. Plasma fibrin D-dimer levels and risk of stable coronary artery disease: results of a large case-control study. Arterioscler Thromb Vasc Biol. 2001;21(10):1701–1705.
12.
WangTJGonaPLarsonMG. Multiple biomarkers for the prediction of first major cardiovascular events and death. N Engl J Med. 2006;355(25):2631–2639.
13.
PinedaJMarinFMarcoP. Premature coronary artery disease in young (age <45) subjects: interactions of lipid profile, thrombophilic and haemostatic markers. Int J Cardiol. 2009;136(2):222–225.
14.
SpeiserWMallekRKoppensteinerR. D-dimer and TAT measurement in patients with deep venous thrombosis: utility in diagnosis and judgement of anticoagulant treatment effectiveness. Thromb Haemost. 1990;64(2):196–201.
15.
GensiniGG. A more meaningful scoring system for determining the severity of coronary heart disease. Am J Cardiol. 1983;51(3):606.
16.
American Diabetes Association. Diagnosis and Classification of Diabetes Mellitus. Diabetes Care. 2014;37Suppl 1:S81–90.
17.
Nomenclature and criteria for diagnosis of ischemic heart disease. Report of the Joint International Society and Federation of Cardiology/World Health Organization task force on standardization of clinical nomenclature. Circulation. 1979;59(3):607–609.
18.
ZhangYLiSZhuCG. Risk Factors, Coronary Severity, Outcome and ABO Blood Group: A Large Chinese Han Cohort Study. Medicine (Baltimore). 2015;94(43):e1708.
19.
ItakuraHSobelBEBoothroydD. Do plasma biomarkers of coagulation and fibrinolysis differ between patients who have experienced an acute myocardial infarction versus stable exertional angina?Am Heart J. 2007;154(6):1059–1064.
20.
CampoGPavasiniRPollinaATebaldiMFerrariR. Coagulation factors and recurrence of ischemic and bleeding adverse events in patients with acute coronary syndromes. Thromb Res. 2013;132(2):151–157.
21.
Bayes-GenisAMateoJSantaloM. D-Dimer is an early diagnostic marker of coronary ischemia in patients with chest pain. Am Heart J. 2000;140(3):379–384.
22.
TokitaYKusamaYKodaniE. Utility of rapid D-dimer measurement for screening of acute cardiovascular disease in the emergency setting. J Cardiol. 2009;53(3):334–340.
23.
KleinegrisMCten CateHten Cate-HoekAJ. D-dimer as a marker for cardiovascular and arterial thrombotic events in patients with peripheral arterial disease. A systematic review. Thromb Haemost. 2013;110(2):233–243.
24.
SadanagaTKohsakaSOgawaS. D-dimer levels in combination with clinical risk factors can effectively predict subsequent thromboembolic events in patients with atrial fibrillation during oral anticoagulant therapy. Cardiology. 2010;117(1):31–36.
25.
MaheIBergmannJFChassanyO. A multicentric prospective study in usual care: D-dimer and cardiovascular events in patients with atrial fibrillation. Thromb Res. 2012;129(6):693–699.
26.
ChristerssonCWallentinLAnderssonU. D-dimer and risk of thromboembolic and bleeding events in patients with atrial fibrillation--observations from the ARISTOTLE trial. J Thromb Haemost. 2014;12(9):1401–1412.