
Abstract
Aim:
The goal of this study was to determine the levels of factor VII (FVII), factor VIIa–antithrombin complexes (FVIIa-AT), total tissue factor (TF), and tissue factor-bearing microparticles (MPs-TF) in patients with acute ischemic stroke. Further, we sought evidence of an association between hemostatic markers, time of blood sampling, type of treatment, and patient outcomes.
Methods:
Venous blood samples were collected from 33 patients on the first day and on the seventh day after stroke diagnosis. Age-matched controls were also included (n = 20). Plasma levels of FVII, FVIIa-AT, total TF, and MPs-TF were measured by enzyme-linked immunosorbent assay. We divided patients into 2 groups: thrombolysis group (n = 13) and nonthrombolysis group (n = 20). Furthermore, evaluation of the National Institutes of Health Stroke Scale and the Barthel Index was performed on the first day and the seventh day.
Results:
Patients with ischemic stroke showed significantly lower plasma FVII, FVIIa-AT, and total TF levels than controls (median, 112.25% vs 132.05%, P = .004; 107.97 pmol/L vs 154.94 pmol/L, P < .001; 81.74 pg/mL vs 105.71 pg/mL, P < .001, respectively). In contrast, levels of plasma MPs-TF were significantly higher in patients with stroke compared to healthy controls (1.60 pg/mL vs 0.74 pg/mL, P < .001). Additionally, the thrombolysis group had lower FVII levels on the seventh day compared to the first day (median, 109.80% vs 115.74%, P = .04).
Conclusion:
Factor VII, FVIIa-AT, and total TF are decreased, while MPs-TF are elevated in patients with ischemic stroke. We observed a slight but significant effect of alteplase on FVII plasma levels.
Keywords
Introduction
Stroke remains a consequential health problem worldwide resulting in high rates of morbidity and mortality. 1 It has been reported by investigators of the American Heart Association that on average, every 40 seconds someone in the United States has a stroke. 2 It is also essential to pay special attention to the high costs of stroke care. 2,3
Ischemic stroke accounts for 87% of strokes, 2 and, recently, as demonstrated by Bembenek et al, this rate is over 90% in a highly urbanized Polish area. 4 A large body of evidence demonstrates that the key features of the ischemic stroke pathophysiology are hemostatic disturbances. 5 –7 Although experimental and clinical studies have shown that ischemic stroke is a thromboinflammatory disease, 5 the pathophysiological mechanism of this phenomenon has remained unclear, mostly due to its multifactorial character.
Factor VII (FVII) is a vitamin K-dependent glycoprotein, which after its activation by tissue factor (TF) initiates the extrinsic pathway of blood coagulation. The resulting factor VIIa–tissue factor complex (FVIIa-TF) catalyzes a series of reactions leading to the tenase complex activation. 8,9 Two key pathways are involved in the regulation of FVIIa-TF complex activity. To begin with, TF pathway inhibitor (TFPI) is the major endogenous inhibitor of FVIIa-TF catalytic complex and acts by forming quarternary complexes with factor Xa, FVIIa, and TF. 10 Additionally, it has been demonstrated that antithrombin (AT), a fundamental regulator of the coagulation system, inactivates FVIIa but only when it is bound to TF. 11 Rao and colleagues reported that the binding of AT to FVIIa-TF complexes results in formation of factor VIIa–antithrombin (FVIIa-AT) complexes. 12 The authors of recent studies have suggested that the levels of FVIIa-AT complexes could be used as a marker of intravascular TF exposure, notwithstanding it still remains a matter of controversy. 13,14 In addition, the role of FVIIa-AT in adult patients diagnosed with ischemic stroke has not yet been investigated. Thus, it is understandable that the current study was designed to evaluate whether plasma FVIIa-AT levels were associated with type of treatment and outcomes of patients with ischemic stroke. Moreover, for a better understanding of the relationship between clinical findings and hemostatic abnormalities, we assessed plasma levels of FVII, FVIIa-AT, total TF, and tissue factor-bearing microparticles (MPs-TF) on the first day and the seventh day after stroke diagnosis. Our study predominantly fills the knowledge gap on the role of FVIIa-AT in the pathophysiology of acute ischemic stroke.
Materials and Methods
The current study included 33 patients diagnosed with acute ischemic stroke, with ages ranging from 42 to 87 years. All patients were recruited from the Neurology and Stroke Care Unit (Jan Biziel University Hospital № 2, Bydgoszcz, Poland). Ischemic stroke was diagnosed by a highly qualified neurologist based on World Health Organization criteria, 15 confirmed by computed tomography on admission. At the time of initial diagnosis, clinical and demographic features of the patients were recorded, including well-documented risk factors for ischemic stroke: hypertension, diabetes mellitus, cigarette smoking, and atrial fibrillation (AF). For the present study, we excluded patients with (1) hemorrhagic stroke, (2) transient ischemic attack (TIA; symptoms duration < 24 hours), (3) systemic malignancy, (4) renal and hepatic dysfunction, (5) sepsis, and (6) pregnancy. Stroke severity on admission (first day) and 1 week after (seventh day) was assessed with the National Institutes of Health Stroke Scale (NIHSS) score (range: 0-42 points). Concurrent, disability was assessed in each patient using the Barthel Index (BI; range: 0-100 points). Moreover, ischemic stroke was subtyped according to the Oxfordshire Community Stroke Project (OCSP) classification: partial anterior circulation infarct (PACI), lacunar infarct (LACI), posterior circulation infarct (POCI), and total anterior circulation infarct (TACI).
On the grounds that alteplase (recombinant tissue plasminogen activator [rtPA]) is the only thrombolytic agent presently approved for treatment of ischemic stroke, 16 the patient population was divided into 2 groups: the 13 individuals treated with intravenous rtPA at 0.9 mg/kg body weight (maximum dose, 90 mg; Actilyse 50 [Boehringer Ingelheim, Ingelheim, Germany]) and the 20 individuals who were not treated with rtPA. The criteria set by the American Heart Association/American Stroke Association to determine eligibility for rtPA infusion have been used in the current research. 17 Participants assigned to the control group (n = 10 males and n = 10 females) were enrolled from the Neurological Outpatient Clinic in Jan Biziel University Hospital № 2, Bydgoszcz, Poland. These age-matched (age range, 42-86 years; median, 68 years) individuals were without any neurologic conditions or previous stroke. Control participants with diabetes mellitus and/or hypertension were also deemed ineligible. All of the patients with ischemic stroke and the controls were of Polish ancestry.
Ethical approval for this study was obtained from the Regional Ethical Committee of Collegium Medicum of Nicolaus Copernicus University (Bydgoszcz, Poland). Written informed consent was ratified from all participants, which was carried out in accordance with the Declaration of Helsinki.
Definitions of the Disorders
Hypertension was defined according to the American Heart Association, as a systolic blood pressure level ≥140 mmHg and diastolic blood pressure ≥90 mmHg or as the need for antihypertensive therapy. Diabetes mellitus was diagnosed whenever at least one of the following criteria was satisfied: treatment with insulin or oral hypoglycemic agents, or fasting blood glucose ≥7 mmol/L (≥126 mg/dL) on two occasions. Current cigarette smokers were defined as those reporting smoking prior to the stroke onset. Atrial fibrillation was defined according to the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society definition, 18 based on electrocardiographic findings on admission.
Blood
For detection of FVII, FVIIa-AT, total TF, and MPs-TF, blood samples were collected 2 times from each patient with stroke: (1) at the time of diagnosis (first day) and (2) at 1 week after diagnosis (seventh day). Venous blood from patients treated with intravenous rtPA was drawn 2 hours after drug administration. Patients who did not receive rtPA underwent a venous blood draw during first 2 hours after stroke diagnosis. Blood samples were collected into tubes (BD Vacutainer, Franklin Lakes, New Jersey) containing 3.2% (0.109 mol/L) sodium citrate. Fasting blood was collected from each healthy individuals from control group only once. Plasma samples of controls were prepared in the same way as in the group of patients with stroke.
Centrifugation was performed twice for the determination of MPs-TF: (1) first, blood was centrifuged for 15 minutes at 1500 g (room temperature), and the supernatant of plasma was decanted; (2) next, supernatant was rapidly centrifuged for 2 minutes at 13 000 g (room temperature) to obtain final material for analysis, which was then divided into portions of 200 µL each and stored at −80°C. Plasma samples for MPs-TF were never stored or centrifuged at 4°C. Blood plasma for the determination of FVII, FVIIa-AT, and total TF was centrifuged for 20 minutes at 1500 g (+4°C), and the supernatants were decanted and placed in 200-µL portions, which were then stored at −80°C. No repeated freeze–thaw cycles were performed before analysis.
Measurement of FVII, FVIIa-AT, Total TF, and MPs-TF
Commercially available enzyme-linked immunosorbent assay (ELISA) kits for FVII, FVIIa-AT, total TF, and MPs-TF were used according to the manufacturers’ instructions. Absorbance was read on a plate reader (Multiskan EX; Thermo Fisher Scientific Inc, Waltham, USA). The optical density of the final reaction plate was detected at a wave length of 405 nm (MPs-TF) or at 450 nm (FVII, FVIIa-AT, and total TF). Levels were expressed as picomoles (pmol/L) for the FVIIa-AT complexes, as percentage for FVII, and as pg/mL for total TF and MPs-TF. The estimation of hemostatic markers was done at the Department of Pathophysiology, Collegium Medicum of Nicolaus Copernicus University (Bydgoszcz, Poland).
Plasma levels of FVII were measured by ZYMUTEST Factor VII kit (HYPHEN BioMed, SAS, Neuville-sur-Oise, France), which is a 2-site immunoassay for measuring human FVII antigen. The FVII levels in healthy adults is usually in the range of 70% to 130%. According to the manufacturer, no significant heparin interference up to 2 IU/mL is observed in this kit, and the detection threshold of the assay system is ≤5%. Of note, in the current study, FVII abbreviation means total levels of factor VII (antigen).
Circulating plasma FVIIa-AT levels were detected by the Asserachrom VIIa-AT kit (Diagnostica Stago S.A.S., Asnières-sur-Seine, France). In brief, the FVIIa-AT complex is captured by mouse monoclonal antihuman FVIIa antibody coated on the wall of a microplate. Next, the second monoclonal anti-AT antibody coupled with peroxidase binds to the remaining free antigenic determinants of the bound FVIIa-AT complex. As stated in the product data sheet, the FVIIa-AT complex levels for 95% of the tested normal human plasmas were between 75 and 220 pmol/L. The detection limit of this assay is 40 pmol/L of FVIIa-AT.
The amount of MPs-TF in plasma was determined using ZYMUPHEN MP-TF kit (HYPHEN BioMed, SAS). In this assay, a micro ELISA plate is coated with a murine monoclonal antibody, specific for an extracellular domain of human TF, and which does not interfere with TF activity. Following overnight incubation of the assayed specimens and a washing step, FVIIa and factor X are added to each wells. The TF-FVIIa complex forms and activates factor X (X→Xa) in the presence of Ca2+. The generation of factor Xa is dependent on TF and phospholipids present in the microparticles. This kit has been optimized to avoid interferences due to the MPs that do not bear TF. The kit doesn’t react with truncated TF nor synthetic liposomes. The detection threshold is ≤1 pg/mL of MPs-TF.
Plasma specimens were assayed for TF levels using ZYMUPHEN Total Tissue Factor kit (HYPHEN BioMed, SAS), which is a 2-site, enhanced, immunoassay for measuring human truncated and full length TF (total tissue factor). The kit has been optimized to minimize the interference of the potential presence of heterophilic antibodies in some particular plasmas, which could otherwise result in an overestimation of TF concentration. The detection threshold of the test is ≤10 pg/mL. The intraassay and interassay coefficients of variation for all tests were below 10%.
Statistical Analysis
All statistical analyses were performed using STATISTICA 12.0 (StatSoft, Cracow, Poland). Normality was assessed using the Shapiro-Wilk test. The groups were compared using the Fisher exact test for the categorical data and the Mann-Whitney U test for the numerical data. The differences in FVII, FVIIa-AT, total TF, and MPs-TF levels between the first and the seventh days were assessed using the Wilcoxon signed-rank test. Correlation was tested by Spearman rank test. The Spearman correlation coefficient (R) was interpreted according to Zou et al 19 as follows: R = .0—no association, R = .2—weakly correlated, R = .5—moderately correlated; R = .8—strongly correlated; and R = 1.0—perfectly correlated. All results are expressed as the median and interquartile range (IQR). Differences were considered significant for P < .05.
Results
Demographic and Clinical Characteristics of Stroke Victims
A total of 33 patients with acute ischemic stroke were studied. The median age of them was 70 years (IQR, 65-80 years). Thirty-nine percent (n = 13) of all individuals were female. The median NIHSS score on the first day was 8 (IQR, 6-10) and on the seventh day was 4 (IQR, 2-7). On the first day, the median BI score was 35 (IQR, 0-70) while on the seventh day was 95 (IQR, 60-100). Compared to the seventh day, the first day NIHSS score was statistically significantly higher, whereas the BI score was statistically significantly lower (P < .001 for both). Of all patients, 27 (82%) had hypertension, 10 (30%) had diabetes mellitus, 12 (36%) had AF, and 8 (24%) were smokers. The OCSP classification for stroke victims was as follows: PACI (n = 20), LACI (n = 5), POCI (n = 5), and TACI (n = 3).
The present cohort was divided into 2 groups depending on therapy: those who had received rtPA (thrombolysis group, n = 13) and those who had not received rtPA (nonthrombolysis group, n = 20). The 2 groups did not significantly differ in age, sex, and OCSP classification, except that the thrombolysis group tended to have a lower median BI score at the first day compared to the nonthrombolysis group (median, 25 vs 55, P = .04). Additionally, patients from the nonthrombolysis group were more likely to have hypertension but not others risk factors. The NIHSS and the BI scores showed significant differences between the first day and the seventh day in each treatment group. The main clinical features in the patients with stroke are described in Table 1.
Demographic and Clinical Characteristics of Patients With Acute Ischemic Stroke Grouped According to the Type of Treatment (Thrombolysis Group = Patients Treated With Alteplase; Nonthrombolysis Group = Patients not Treated With Alteplase).
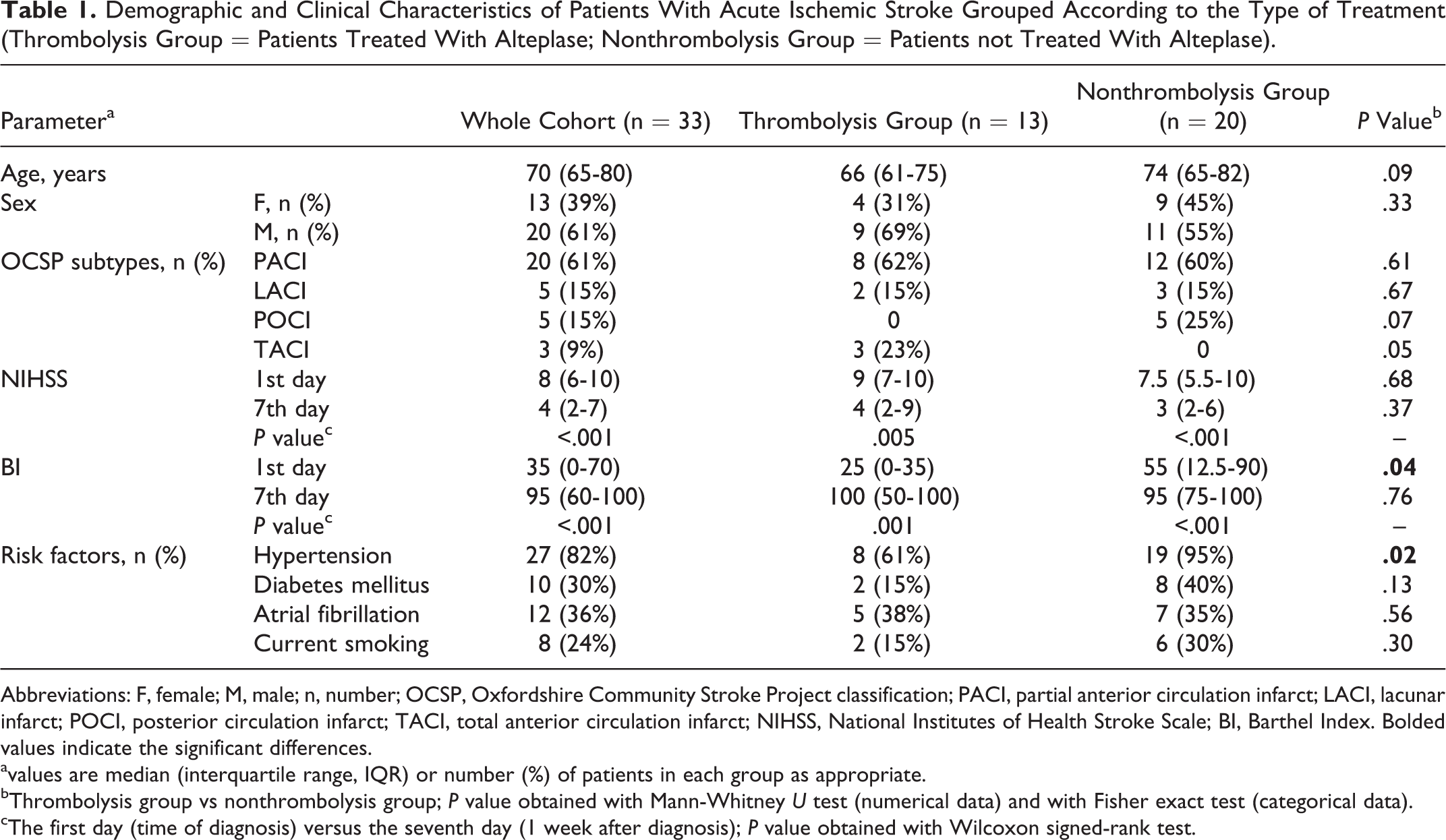
Abbreviations: F, female; M, male; n, number; OCSP, Oxfordshire Community Stroke Project classification; PACI, partial anterior circulation infarct; LACI, lacunar infarct; POCI, posterior circulation infarct; TACI, total anterior circulation infarct; NIHSS, National Institutes of Health Stroke Scale; BI, Barthel Index. Bolded values indicate the significant differences.
avalues are median (interquartile range, IQR) or number (%) of patients in each group as appropriate.
bThrombolysis group vs nonthrombolysis group; P value obtained with Mann-Whitney U test (numerical data) and with Fisher exact test (categorical data).
cThe first day (time of diagnosis) versus the seventh day (1 week after diagnosis); P value obtained with Wilcoxon signed-rank test.
Factor VII, FVIIa-AT, Total TF, and MPs-TF Levels in Stroke Victims on the First Day (at the Time of Diagnosis) and Controls
We first addressed whether there were differences in FVII, FVIIa-AT, total TF, and MPs-TF levels between patients diagnosed with ischemic stroke and healthy participants. As can be seen from Figure 1A to C, the median plasma FVII, FVIIa-AT, and total TF levels were significantly lower in patients with stroke compared to control participants. By contrast, patients with stroke showed significantly higher plasma levels of MPs-TF than controls (Figure 1D), which confirmed our previous observation. 7
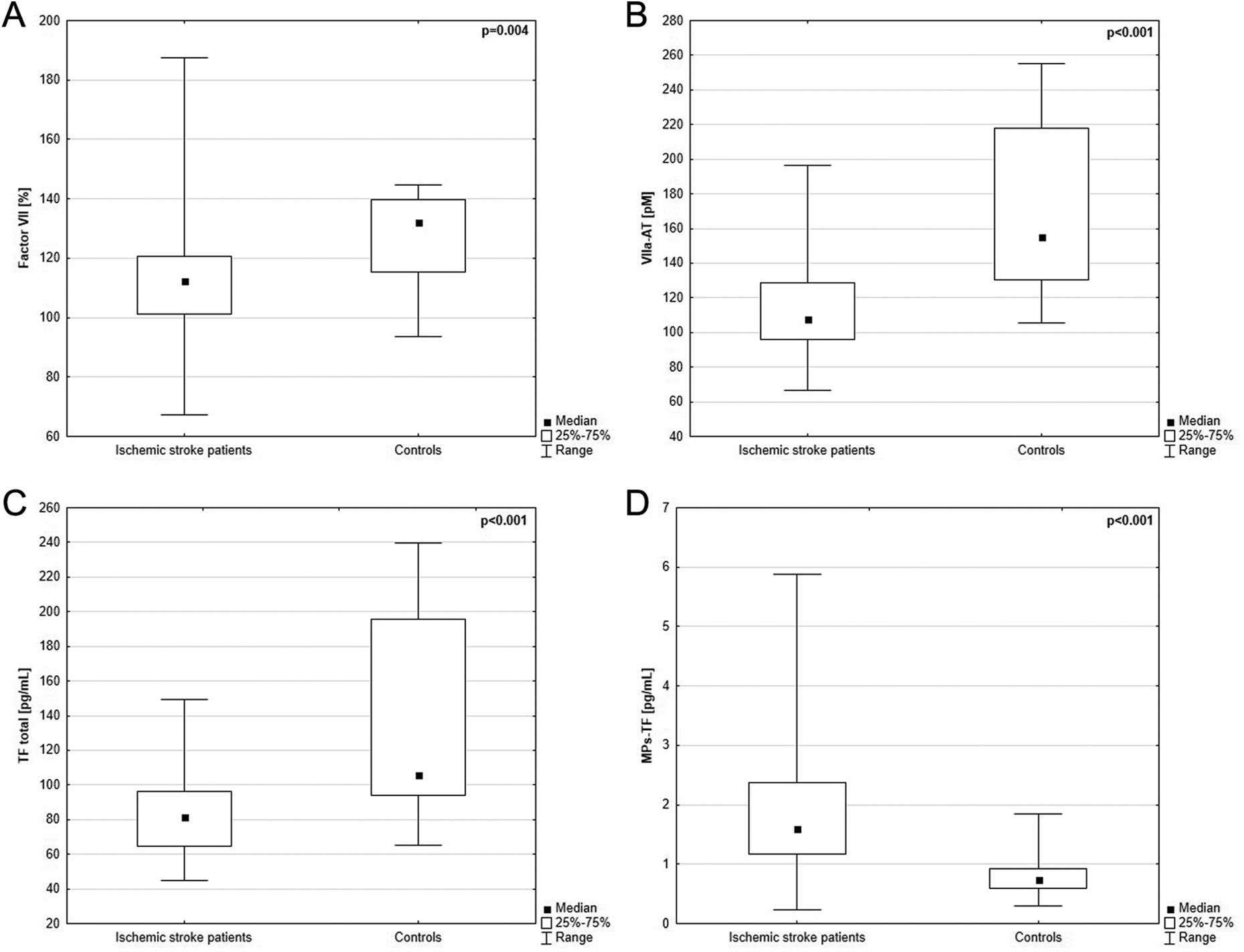
Acute ischemic stroke population versus control group: the first day (time of diagnosis) plasma levels of (1A) factor VII (FVII); (1B) factor VIIa–antithrombin (VIIa-AT); (1C) total tissue factor (TF); and (1D) tissue factor-bearing microparticles (MPs-TF) in patients with stroke (n = 33) compared to healthy individuals (n = 20); P value obtained by using Mann-Whitney U test.
Effect of Timing of Blood Collection and Type of Treatment on Levels of Hemostatic Parameters (FVII, FVIIa-AT, Total TF, and MPs-TF)
(a) Hemostatic parameters in whole cohort of stroke victims (n = 33) on the first day (at the time of diagnosis) and on the seventh day (1 week after diagnosis)
To further explore the relationship between hemostatic parameters and ischemic stroke, we compared levels of FVII, FVIIa-AT, total TF, and MPs-TF on the first day and the seventh day after stroke onset. Plasma levels of these markers were similar between the first day and the seventh day (Table 2).
The First Day (Time of Diagnosis) and the Seventh Day (1 Week after Diagnosis) Plasma Levels of Factor VII, VIIa-AT, Total TF and MPs-TF in Stroke Patients Grouped According to their Therapies.
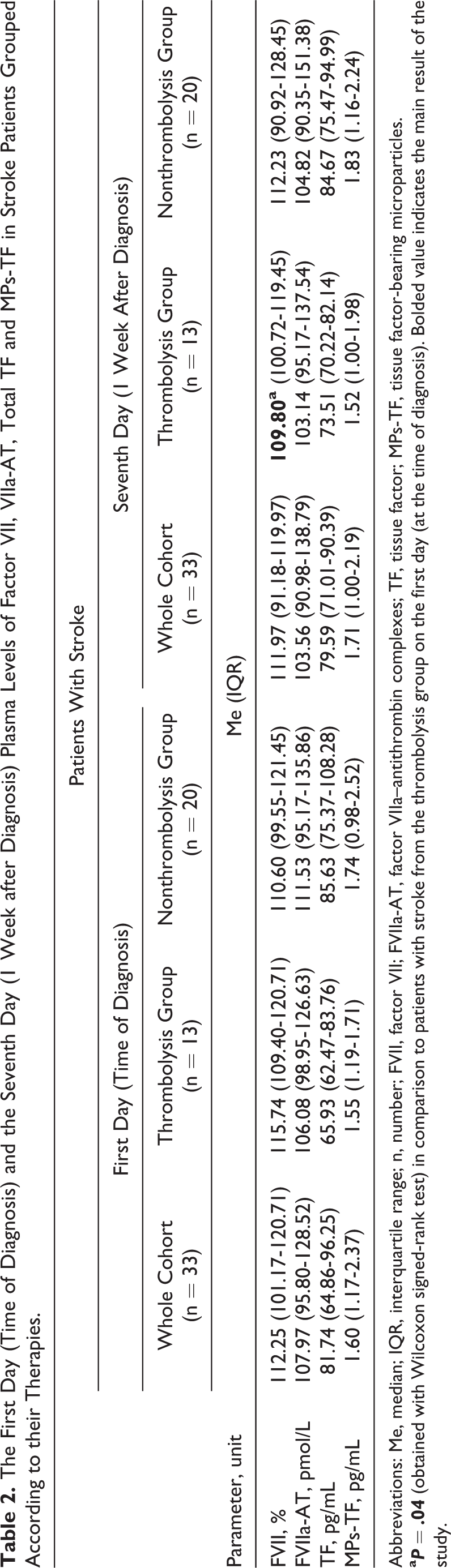
Abbreviations: Me, median; IQR, interquartile range; n, number; FVII, factor VII; FVIIa-AT, factor VIIa–antithrombin complexes; TF, tissue factor; MPs-TF, tissue factor-bearing microparticles.
(b) Hemostatic parameters on the first day (at the time of diagnosis) in the thrombolysis group and the nonthrombolysis group
At the time of diagnosis, no significant differences concerning plasma levels of FVII, FVIIa-AT, total TF, and MPs-TF were observed between the thrombolysis group and the nonthrombolysis group (Table 2).
(c) Hemostatic parameters on the seventh day (1 week after diagnosis) in the thrombolysis group and the nonthrombolysis group
We also analyzed hemostatic parameters on the seventh day after stroke onset in each treatment group. We failed to find differences in plasma levels of FVII, FVIIa-AT, total TF, and MPs-TF between the thrombolysis group and the nonthrombolysis group at 1 week after stroke diagnosis (Table 2).
(d) Hemostatic parameters on the first day (at the time of diagnosis) and the seventh day (1 week after diagnosis) in the thrombolysis group
To examine the effect of alteplase on hemostatic parameters, we further compared plasma levels of FVII, FVIIa-AT, total TF, and MPs-TF on the first and the seventh day after stroke diagnosis in the thrombolysis group. Using the Wilcoxon signed-rank test, we identified slightly lower levels of FVII 1 week after stroke diagnosis compared to the first day (P = .04). In contrast, plasma FVIIa-AT, total TF, and MPs-TF levels were similar on the first day and the seventh day (Table 2).
(e) Hemostatic parameters on the first day (at the time of diagnosis) and on the seventh day (1 week after diagnosis) in the nonthrombolysis group
As demonstrated in Table 2, there were no statistically significant differences in FVII, FVIIa-AT, total TF, and MPs-TF plasma levels between the first day and the seventh day in patients who did not receive alteplase.
Factor VII, FVIIa-AT, Total TF, and MPs-TF Levels on the First Day (at the Time of Diagnosis) in Relation to the First Day NIHSS Score
To investigate a possible association between hemostatic parameters and stroke severity, patients were categorized according to the NIHSS score into 2 groups: (1) patients with the admission NIHSS score of ≤7 (n = 16) and (2) patients with the admission NIHSS score of >7 (n = 17). A cut point of 7 on the NIHSS has been chosen according to the results of previous study. 20 The median NIHSS score in the first group was 5.5 (IQR, 4-7) while in the second group was 10 (IQR, 9-14), and this observation was highly significant (P < .001). Notwithstanding, no significant differences in plasma levels of FVII, FVIIa-AT, total TF, and MPs-TF were found between the 2 NIHSS groups.
Factor VII, FVIIa-AT, Total TF, and MPs-TF Levels on the First Day (at the Time of Diagnosis) in Relation to the First Day BI Score
Corresponding to the NIHSS, patients with stroke were further divided into 2 groups based on measures of the BI score: (1) patients with the admission BI score of <60 (n = 23) and (2) those with the admission BI score of ≥60 (n = 10). A cut point of 60 on the BI has been chosen according to previous findings. 21 The median of the BI was significantly lower in the first group than in the second group (median, 15 [IQR, 0-40] vs 90 [IQR, 85-100]; P < .001). When these 2 groups of patients were compared, no statistically significant differences were found in levels of FVII, FVIIa-AT, total TF, and MPs-TF at the time of diagnosis.
Correlation Analysis
Finally, the statistical analysis demonstrated a significant weak correlation between levels of FVIIa-AT and FVII on the first day (R = .4, P = .03; Figure 2A). Analogous to this observation, a significant moderate correlation between levels of FVIIa-AT and FVII on the seventh day was found (R = .5, P = .003; Figure 2B). Additionally, our results indicate statistically significant correlations between the first day and the seventh day in hemostatic markers, which are presented in Table 3.
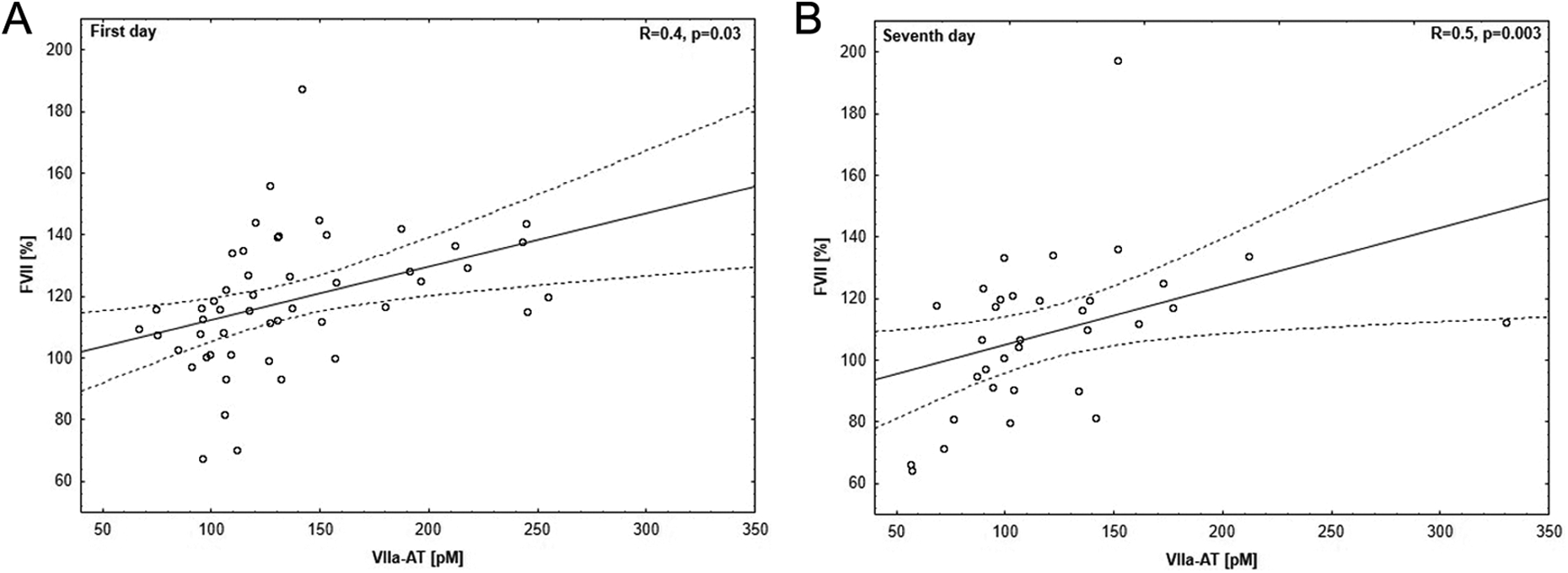
Correlation between factor VII (FVII) and factor VIIa–antithrombin (VIIa-AT) in plasma of patients with stroke: (2A) on the first day (at the time of diagnosis) and (2B) on the seventh day (1 week after diagnosis). Correlation between variables was determined using Spearman rank correlation coefficient.
Correlation Between the First Day (Time of Diagnosis) and the Seventh Day (1 Week After Diagnosis) Plasma Levels of FVII, FVIIa-AT, Total TF, and MPs-TF Among Whole Cohort.a
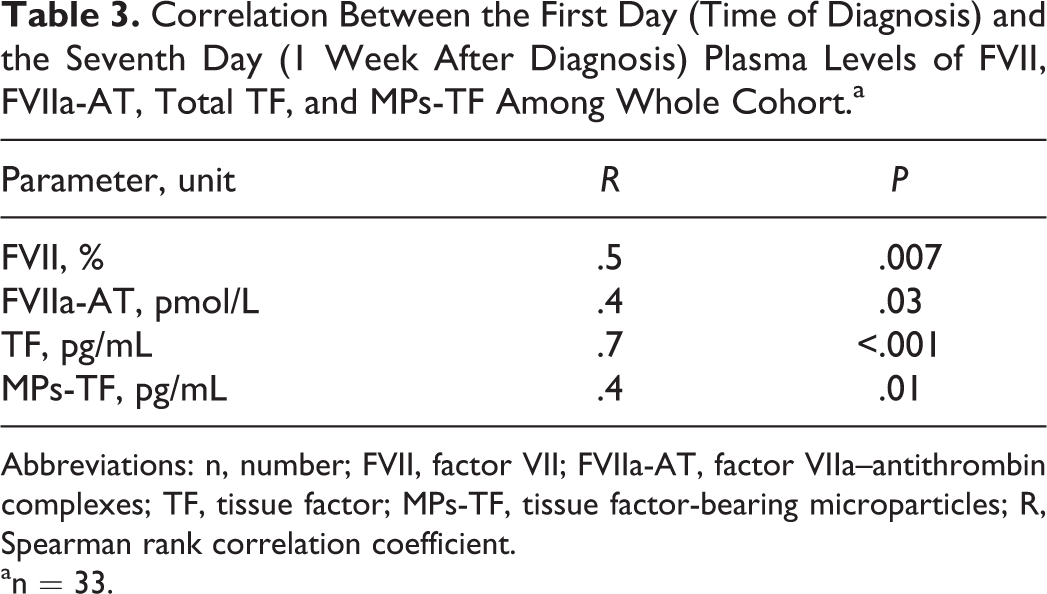
Abbreviations: n, number; FVII, factor VII; FVIIa-AT, factor VIIa–antithrombin complexes; TF, tissue factor; MPs-TF, tissue factor-bearing microparticles; R, Spearman rank correlation coefficient.
an = 33.
Discussion
The current study establishes 3 noteworthy results: (1) FVII, FVIIa-AT, and total TF levels were significantly lower in patients with ischemic stroke than in the control group; (2) levels of MPs-TF were significantly higher in patients with ischemic stroke than in the control group; and (3) patients treated with alteplase (rtPA) had lower levels of FVII 1 week after diagnosis compared to the time of diagnosis. This report extends our previous observation 7 on the hemostatic disturbances in ischemic stroke.
Our findings suggest that levels of FVIIa-AT complex in patients who were diagnosed with ischemic stroke may depend on plasma levels of FVII. This hypothesis is partially supported by a significant correlation between levels of FVIIa-AT and FVII as observed on the first day likewise on the seventh day after stroke diagnosis. A series of studies published by Spiezia and coworkers 13,22,23 highlighted the importance of FVIIa-AT complexes in blood coagulation. First, they reported that the plasma levels of FVIIa-AT were decreased in children with acute ischemic stroke compared to healthy children. Contemporaneously, lower FVIIa activity was observed in the stroke group, although the difference between stroke and control groups was not statistically significant. 22 Equally important, previous study indicated that levels of FVIIa-AT complex were lower in patients with either acute arterial or venous thrombosis than patients with previous arterial or venous thrombosis and than healthy controls. It is important to emphasize that the acute thrombosis group included, among others, 9 patients with acute ischemic stroke, while among the cases with previous thrombosis, 19 had an acute ischemic stroke. Additionally, lower levels of FVII have been reported in patients diagnosed with acute thrombosis compared to patients with previous thrombosis. 13 In line with this evidence, in our study, we found that plasma levels of FVIIa-AT and FVII decreased in stroke victims. Furthermore, FVIIa-AT complexes are formed in the presence of TF, 11 thus lower levels of TF detected in our stroke cohort may also result in decreased levels of circulating FVIIa-AT complexes. In spite of limitations that we did not measure the activity of FVII and that the clinical significance of FVIIa-AT complexes is still poorly understood, 24 we speculate that FVIIa-AT levels are related to both FVII and TF levels.
The precise mechanism of decreased FVII levels in patients with acute ischemic stroke remains uncertain. The association between levels or activity of FVII and stroke pathophysiology has been documented in previous studies, however these results are difficult to interpret due to the different methodology, including disparate age and ethnicity of participants as well as type of stroke (reviewed in the supplementary material to a paper by Stanne et al 25 ). Nonetheless, study of Stanne et al 25 demonstrated that FVII levels in ischemic stroke may depend on etiological subtypes and of AF: Patients with cardioembolic stroke or diagnosed with AF had lower levels of FVII. In our present analysis, we did not divide patients into groups, depending on etiological subtypes Trial of ORG 10172 in Acute Stroke Treatment (TOAST) due to the relatively small cohort. However, we found that FVII plasma levels were lower among patients with AF, when compared to non-AF patients (median, 107.91% vs 116.25%, P = .08; the Mann-Whitney U test, data not shown). Furthermore, some evidence suggests that plasma levels of FVII are associated with polymorphism in its gene (F7). 26,27 From an elegant study of Lopaciuk et al, we know that 3 F7 polymorphisms (353Q, P + 10, and +154AA), called as “FVII-lowering,” are associated with decreased plasma FVII levels in patients with stroke, while 2 others (“FVII-elevating”: −670C and IVS7 [intron 7] seven or higher) are associated with increased FVII levels. 28 Interestingly, a case of patient with FVII deficiency who presented with acute ischemic stroke has also been reported. 29
In this study, FVII, FVIIa-AT, total TF, and MPs-TF levels were assessed at the time of diagnosis and 1 week after in the 2 treatment groups. In our data, the patients with thrombolysis exhibited lower plasma FVII levels 1 week after stroke diagnosis in comparison with the first day levels. The unequivocal mechanisms underlying this change are unknown; notwithstanding, our current and preceding 7 observations suggest that alteplase (rtPA) may have a durable impact on hemostatic parameters in ischemic stroke victims. It is worth noticing that an experimental in vitro study has shown that t-PA enhances the activation of the coagulation system through FVII activation. Particularly, it was related to the observation that an increase in the FVIIa levels was observed after the incubation of FVII with t-PA together with plasminogen or only plasmin. 30 The long-term effect (≥1 week) of alteplase on hemostasis is unsatisfactorily understood. Previous clinical study indicated that thrombolysis with rtPA induced massive coagulation activation within the first hour after treatment that lasted for up to 72 hours. In contrast, this effect was not observed on day 5 during an experiment. 31 Further studies involving a large number of patients are needed to answer this problem.
In the current study, we noted that, compared to controls, patients with stroke showed significantly increased levels of MPs-TF. These data are in agreement with those reported earlier by our team. 7 Although we were not able to show the cellular origin of MPs, patients with stroke might be expected to have elevated levels of MPs-TF. Few studies have addressed this issue, 32 –34 and the main finding is consistent among these analyses: different phenotypes of MPs are increased in blood of patients with ischemic stroke. Consequently, the researchers found that increased MPs-TF generation may constitute a risk factor for the development of thrombosis. 35 Of note, Müller et al observed that plasma TF is mainly associated with circulating MPs and initiates coagulation, 36 which may explain why MPs-TF is strongly associated with thrombosis.
In conclusion, FVII, FVIIa-AT, and total TF are decreased while MPs-TF are elevated in patients with ischemic stroke. A slight but significant effect of alteplase on FVII plasma levels was observed in this study. Our pilot analysis provides a useful starting point for evaluation of the relationship between FVII, FVIIa-AT, and type of treatment for acute ischemic stroke. Future studies should focus on the effect of alteplase on the extrinsic pathway of coagulation. In addition, high-quality researches are required to confirm the clinical utility of FVIIa-AT as a biomarker for acute ischemic stroke.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.