
Abstract
Aim:
This study assessed the long-term benefits and side effects of low-to-medium dose of danazol therapy in primary immune thrombocytopenia (ITP).
Methods:
The retrospective analysis included 319 patients with ITP who accepted danazol therapy. Patients accepted danazol alone or in combination with glucocorticoids. Clinical outcome and tolerance were assessed in all patients.
Results:
Among patients with persistent or chronic ITP, the overall response rate of danazol therapy was 65.0%. Sixty-five (63.1%) of the 103 patients reached remission with danazol alone, and 93 (48.7%) of the 191 patients who accepted combination therapies acquired remission and discontinued glucocorticoids successfully. Age and previous treatments were 2 risk factors for response rate. In newly diagnosed patients with ITP, the response rate and median response time did not differ significantly with or without danazol. However, the relapse rate was significantly lower in patients administered danazol combined with glucocorticoids than those accepted glucocorticoids alone. Totally, 21.1% of the patients experienced mild or moderate side effects, and 1.2% of the patients discontinued treatment due to intolerable side effects.
Conclusion:
Low-to-medium dosage of danazol is better tolerated and effective in patients with ITP, even in those refractory to other treatments. Combination of danazol and glucocorticoids for initial treatment may decrease relapse rates to achieve well-tolerated long-term remission.
Introduction
Primary immune thrombocytopenia (ITP) is an acquired autoimmune disease characterized by decreased platelet counts resulting from increased platelet destruction and insufficient platelet production. 1 Recent epidemiological data estimate an ITP incidence of 3.3 per 100 000 adults. 2 In adults, the disease is usually chronic, and treatment is usually required in patients with platelet counts <30 × 109/L and obvious signs of bleeding. 3 The standard first-line treatment of ITP is glucocorticoids, and intravenous immunoglobulins are effective in emergency settings. 4,5 Glucocorticoids can induce responses in two-thirds of adult patients, but relapses are common when corticosteroids are reduced or discontinued, and only 10% to 20% of patients can experience long-term remissions. 6 Splenectomy was previously considered as the main second-line treatment for relapse or first-line refractory patients. 4,5 However, splenectomy is irreversible and immune compromising, and a number of patients are reluctant or unsuitable to undergo the procedure. 7 New therapeutic agents such as rituximab and thrombopoietin receptor agonists have been used recently, but they are costly and have unsatisfactory long-term remission rates. 8 –10 Therefore, there is a need for a treatment that can maintain lasting remissions economically in ITP.
Danazol is a synthetic attenuated androgen with reduced masculinizing capacity that was initially formulated for the treatment of endometriosis. 11 Some studies have shown that danazol can induce platelet elevation by antagonizing estrogen and immune modulation. 12 Ahn et al 13 first described encouraging results of danazol therapy in ITP in 1983. Since then, it has been used as a second-line treatment for chronic, relapsed, and refractory ITP. 4,5
To date, there has been no long-term, large-scale research about the effects and side effects of danazol therapy in Chinese patients with ITP. The optimal usage of danazol also remains undetermined. To clarify the effects, safety, and appropriate dosage and duration of danazol therapy, we performed a retrospective analysis in adult patients with primary ITP.
Patients and Methods
Patients
A total of 381 adult patients with ITP received danazol therapy in our center between January 2010 and December 2014, and 319 cases were included in this retrospective cohort. The other 62 patients were excluded from the study due to insufficient therapy time (<3 months), and 4 of them discontinued danazol due to intolerable side effects. The diagnosis and classifications of ITP were based on previously reported criteria. 5 The patients were classified into 3 categories according to disease duration: newly diagnosed ITP (<3 months), persistent ITP (3-12 months), and chronic ITP (>12 months). 5 With standard courses of steroid therapy, patients with platelet counts of more than 30 × 109/L, who had at least a 2-fold increase in baseline count, or who showed no signs of bleeding were considered steroid responsive. By contrast, the rest were considered steroid refractory. Steroid dependence is defined as the ongoing need for continuous corticosteroid administration or frequent courses of corticosteroids to maintain a platelet counts at or above 30 × 109/L and/or to avoid bleeding. 4,5 Detailed information regarding patient characteristics, medical histories, hemorrhagic symptoms, signs, treatments, responses, and adverse events (AEs) were all obtained from medical records. Patients who had not been followed up in recent years were contacted by telephone for further follow-up information. Follow-up was performed in patients from the first visit in our hospital to December 31, 2014. In this retrospective study, 306 (96%), 296 (93%), and 290 (91%) patients had complete data available for analysis at 6, 12, and 24 months, respectively. At the time of the analysis, a total of 287 (90%) patients had completed the follow-up period and had complete data from all study visits. Table 1 summarized the clinical characteristics of these 319 patients. The study was approved by the hospital ethics committee.
Clinical Characteristics of Patients With ITP Who Received Danazol Therapy.
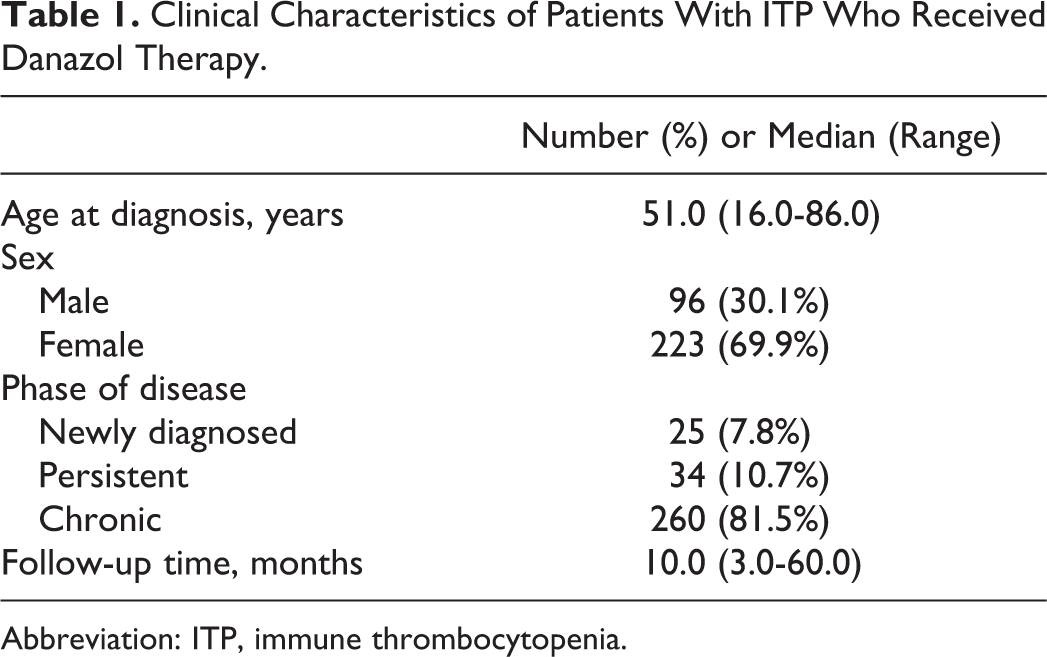
Abbreviation: ITP, immune thrombocytopenia.
Treatment Procedures
All patients with persistent or chronic ITP in our study were steroid refractory or steroid dependent after standard first-line therapy. Danazol was used alone or combined with glucocorticoids. Patients with other concomitant medications (vincristine, azathioprine, cyclosporine A, interleukin 11, rituximab, and thrombopoietin receptor agonists) were excluded. Generally, patients with platelet counts between 20 × 109/L and 30 × 109/L or without obvious bleeding were given danazol alone. For those patients with concomitant therapy, glucocorticoids were gradually tapered and discontinued during danazol therapy. When dosage reduction or discontinuation was associated with relapse, glucocorticoids were decreased more slowly or kept at a minimum dose (equivalent to prednisone 5-10 mg daily or less). Danazol was used at a dose of 200 or 300 mg daily for at least 3 months consecutively unless stopped earlier due to side effects. If no response was observed within 3 months, treatment was discontinued or continued to wait for response in a part of patients. In patients who responded to treatment, danazol was maintained at the same dose, tapered gradually, or discontinued.
In order to evaluate the effect of danazol in early treatment of ITP, in our center, danazol was combined with glucocorticoids as the initial treatment in newly diagnosed patients with ITP randomly. All participating patients provided written informed consent. Glucocorticoids were used at 0.5 to 1.0 mg/kg/d for 2 to 4 weeks and then tapered off. Danazol was used at a dose of 200 or 300 mg daily for 3 months consecutively.
During danazol therapy, all of the clinical symptoms, signs, and AEs were recorded. Liver function was monitored monthly. The common terminology criteria for AEs, version 4.0 (CTCAE 4.0), from the National Cancer Institute (NCI), were used to grade the severity of AEs. 14 Danazol treatment was discontinued in patients with intolerable or severe side effects (grades 3-4), and the dose was reduced by 100 or 200 mg daily in patients with moderate side effects (grades 1-2).
Response and Relapse Criteria
Complete response (CR) was defined as an increase in platelet counts to ≥100 × 109/L and an absence of bleeding. Response (R) was defined as platelet counts ≥30 × 109/L and a greater than 2-fold increase in platelet count from baseline, with an absence of bleeding. No response (NR) was defined as platelet counts <30 × 109/L or less than 2-fold increase in platelet count from baseline or the presence of bleeding. Platelet counts were remeasured after at least 1 day for defining NR or after at least 7 days for defining CR and R. Relapse (following CR or R) was defined as platelet counts dropping below 100 × 109/L or bleeding (from CR) or below 30 × 109/L or less than 2-fold increase in the baseline platelet count or bleeding (from R). 5
Statistical Analysis
Data were analyzed using the software SPSS 17.0. Results were expressed as medians and ranges or absolute numbers and percentages as appropriate. Categorical variables between groups were compared using the χ2 tests. Quantitative values were analyzed using Mann-Whitney U tests. A logistic regression model was used to evaluate variables related to the likelihood of a response to therapies. Kaplan-Meier analyses were performed to estimate relapse-free survival, and the equality of relapse-free survival times between groups was assessed using log-rank tests. P values <.05 were considered statistically significant.
Results
Danazol Therapy in Persistent or Chronic ITP
The therapeutic effect of danazol was analyzed in persistent or chronic ITP; 103 patients received danazol alone and 191 patients received danazol combined with glucocorticoids therapy (Table 2). The response time of danazol varied considerably: 70 (36.6%) patients responded within 1 month, 148 (77.5%) patients responded within 3 months, 170 (89.0%) patients responded within 6 months, 185 (96.9%) patients responded within 12 months, and 6 (3.1%) patients needed more than 1 year.
Danazol Therapy in Patients With Persistent or Chronic ITP.
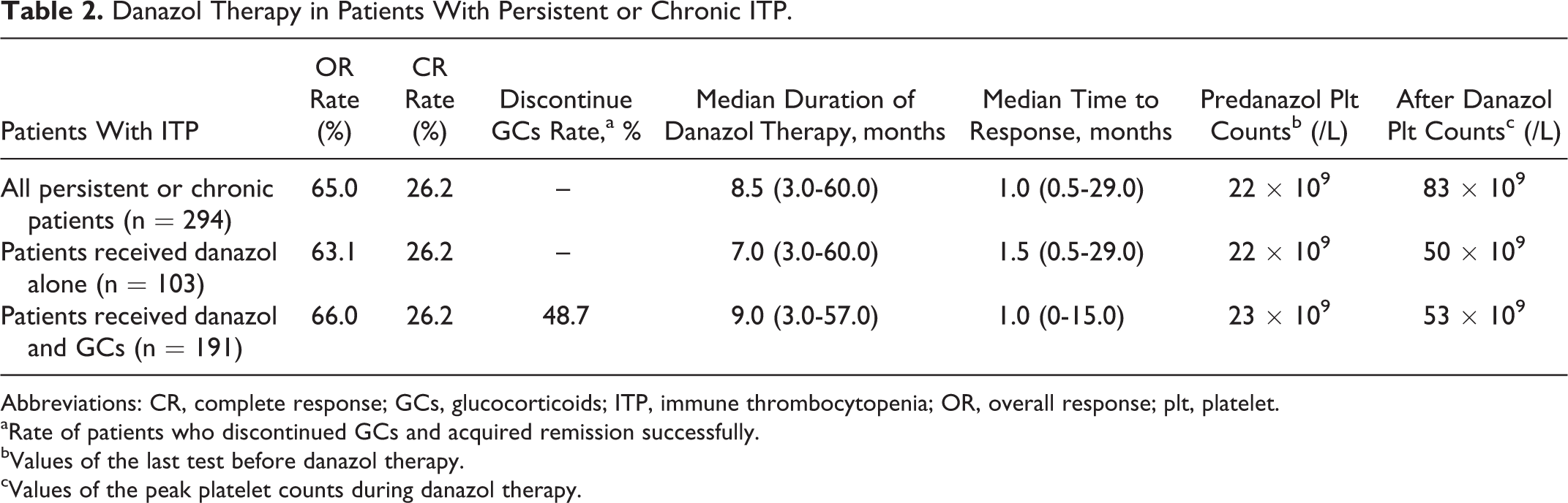
Abbreviations: CR, complete response; GCs, glucocorticoids; ITP, immune thrombocytopenia; OR, overall response; plt, platelet.
aRate of patients who discontinued GCs and acquired remission successfully.
bValues of the last test before danazol therapy.
cValues of the peak platelet counts during danazol therapy.
Logistic regression analysis showed that age (P = .011; Figure 1) and number of previous therapies (P = .031) influenced the response, although other variables such as sex, disease stage, danazol dose, time from diagnosis to initiation of danazol treatment, predanazol platelet counts, and spleen status were not associated with the response rate (data were not shown).
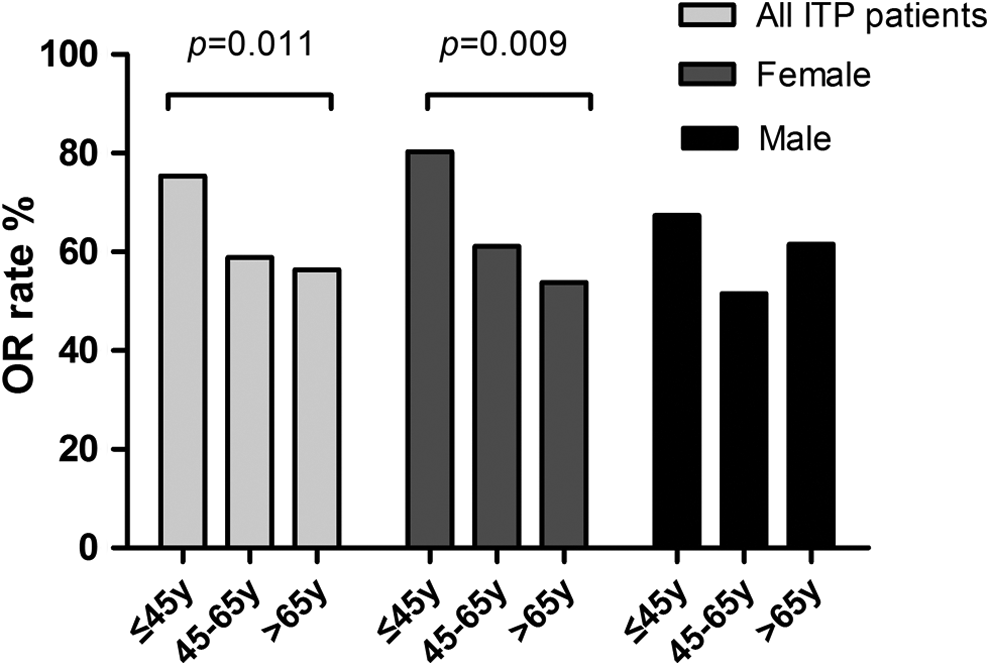
Response to danazol in different age and sex groups.
Among 191 responders, the median duration of remission was 10.0 months (0.1-60.0 months). Except for patients lost to follow-up, a total of 42 (22.0%) patients had relapses. Maintenance therapy status was related to the relapse: Patients who had taken danazol continuously had lower relapse rates than those who discontinued danazol therapy (P = .000; Table 3). Kaplan-Meier analysis also showed that patients who had received danazol treatment longer had better remission than others (P = .000; Figure 2). However, among responders, neither the initial danazol dosage nor the reduction in danazol subsequently affected the relapse rate (P = .357).
Maintenance Therapy and Relapse in Persistent or Chronic ITP.
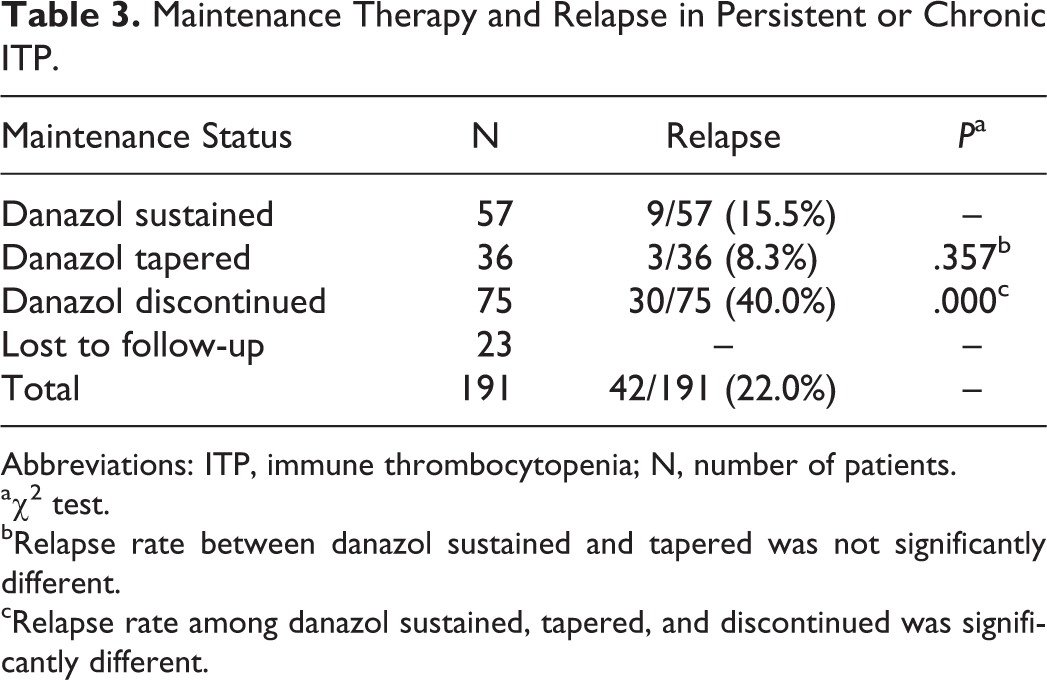
Abbreviations: ITP, immune thrombocytopenia; N, number of patients.
aχ2 test.
bRelapse rate between danazol sustained and tapered was not significantly different.
cRelapse rate among danazol sustained, tapered, and discontinued was significantly different.
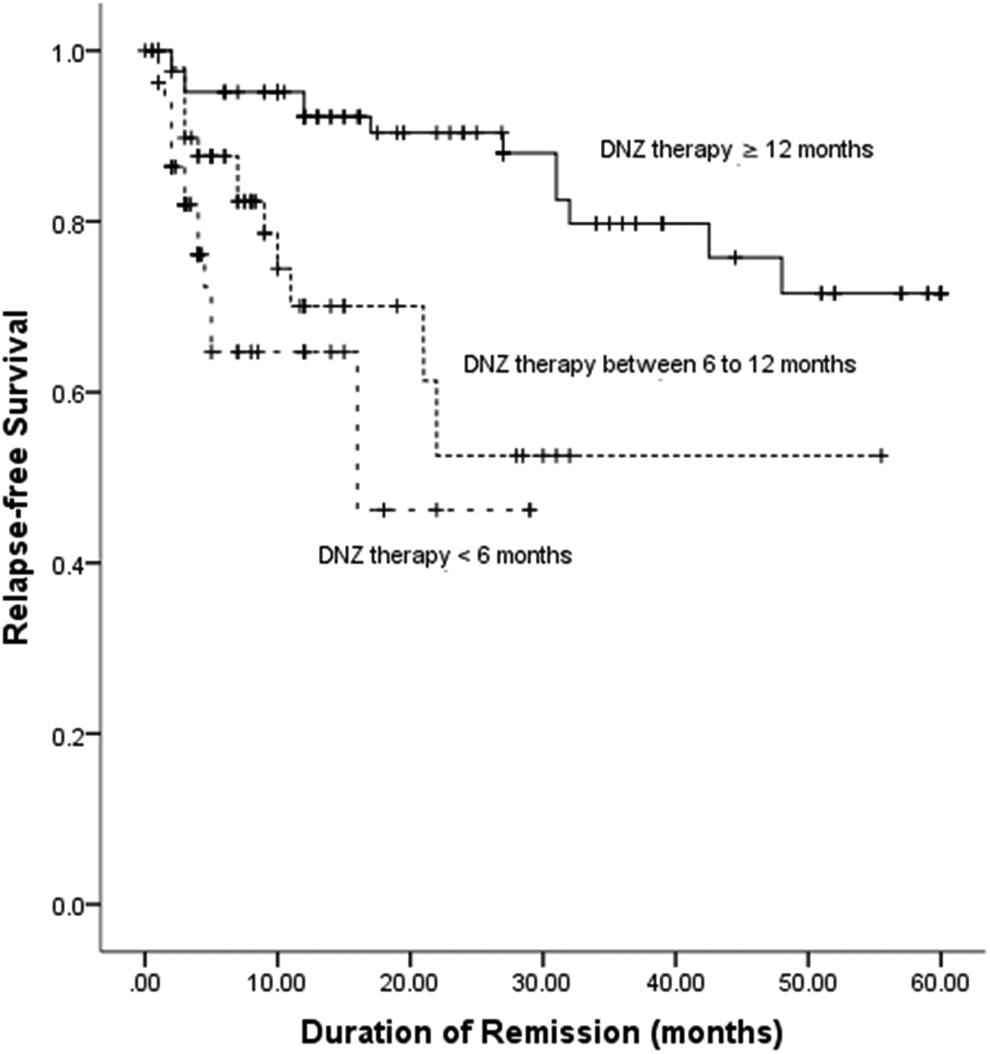
Relapse-free survival after danazol therapy.
Danazol Therapy in Newly Diagnosed ITP
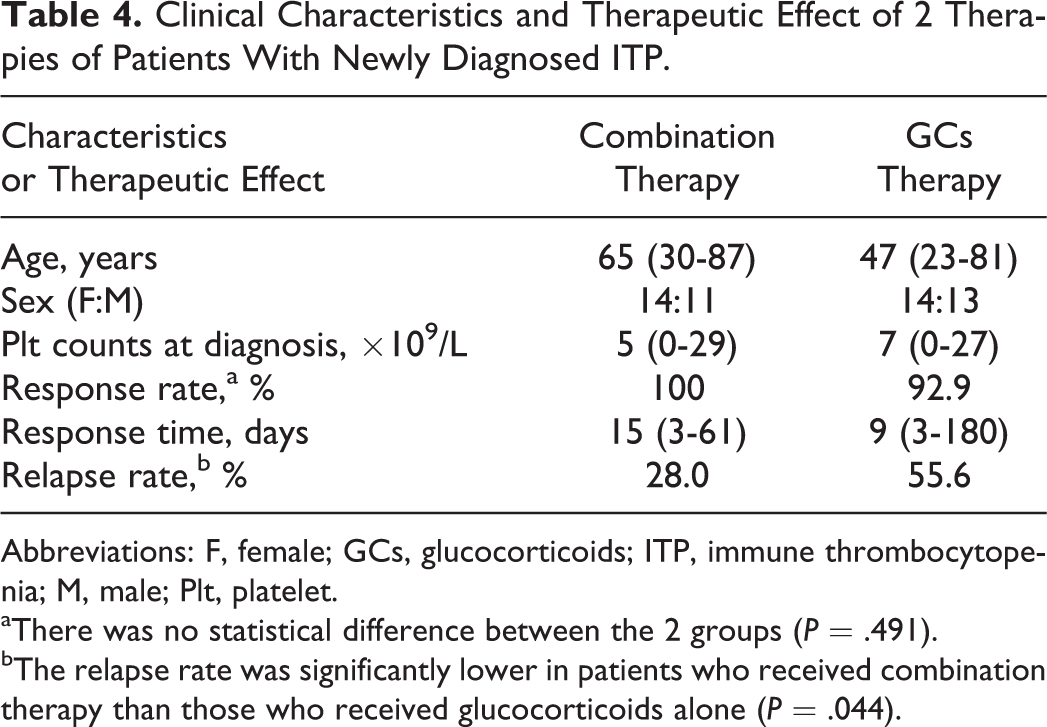
In our study, a total of 25 newly diagnosed patients with ITP in our studyhad received a combination therapy of danazol and glucocorticoids. In order to evaluate the effect of danazol in early treatment of ITP, we compared the responses of the 25 patients to 27 patients who received glucocorticoids alone during the initial treatment stage; these patients were diagnosed consecutively in our hospital from January to July 2014. The response rates and median response time between the 2 therapies were not significantly different (P = .491). However, the rate of relapse was significantly lower in patients who received combination therapy than those who received glucocorticoids alone (P = .044; Table 4). Recurrence cases were divided into 3 groups based on the recurrence time: within 1 month, 3 months, and 6 months. Relapse rates in the 3 periods for glucocorticoids therapy were 37.0%, 48.1%, and 55.6%, respectively. In contrast, the respective relapse rates for combination therapy were 12.0%, 16.0%, and 28.0%. These findings suggest that combination therapies of danazol and glucocorticoids can markedly decrease relapse at any time.
Clinical Characteristics and Therapeutic Effect of 2 Therapies of Patients With Newly Diagnosed ITP.
Abbreviations: F, female; GCs, glucocorticoids; ITP, immune thrombocytopenia; M, male; Plt, platelet.
aThere was no statistical difference between the 2 groups (P = .491).
bThe relapse rate was significantly lower in patients who received combination therapy than those who received glucocorticoids alone (P = .044).
Adverse Effects
During danazol treatment, 68 (21.1%) patients experienced AEs, and all AEs were mild or moderate (grade 1-2). Four patients discontinued danazol (<3 months) due to unacceptable side effects, including liver damage (n = 1), hyperglycemia (n = 1), and amenorrhea (n = 2). The most frequent AEs were liver damage (n = 36). Mild or moderate elevation in aspartate or alanine aminotransferase was the most common damage. Liver function impairments were more frequent in patients who received danazol for more than 6 months (P = .048). Combination of liver protection drugs or reduction in danazol dosage could return liver function to normal. Other side effects were rare and mild, and all these symptoms disappeared when danazol administration was decreased or discontinued (Table 5). Among patients with newly diagnosed ITP, the combined therapy of glucocorticoids and danazol was well tolerated, and none reported AEs.
Adverse Effects of Danazol Therapy.
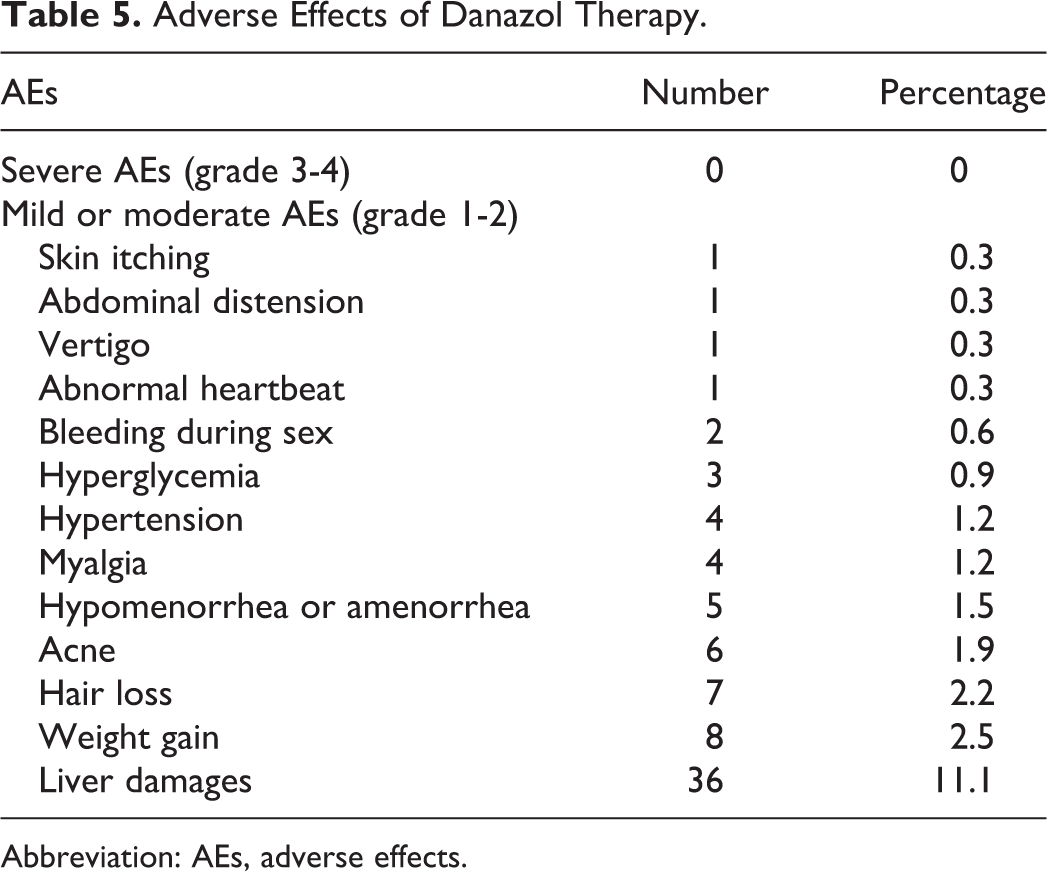
Abbreviation: AEs, adverse effects.
Discussion
Danazol has been used as a second-line treatment of ITP for more than 30 years. 13 However, reliable research about the effects and side effects of danazol in Chinese patients with ITP was lacking. Through a long-term, large-scale retrospective study, we have validated the efficiency and safety of danazol therapy for ITP.
Consistent with most of previous reports, in our study, 65.0% and 26.2% of patients with persistent or chronic ITP acquired overall response (OR) and CR, respectively. 15 –19 In the largest study to date, Ahn et al 15 reported an OR rate of 61.4% among 96 patients. Maloisel et al 16 performed a prospective analysis in 57 patients with chronic ITP, with 67% of patients with acquired OR and 16% of patients with achieved CR. However, several studies have reported contradictory results with poor responses 20,21 (Table 6). These discrepancies may be associated with differences in sample sizes, study populations, and therapeutic approaches. Like the study of Ahn et al, 15 some patients in our study received glucocorticoids together, which may have improved response rates. Although we found that 63.1% of patients who received danazol alone achieved remission, 48.7% of patients who received combination therapies got rid of glucocorticoids successfully. These finding suggests that danazol was effective in increasing platelet counts, even after glucocorticoids were discontinued.
Review of Danazol Therapy in Patients With ITP.
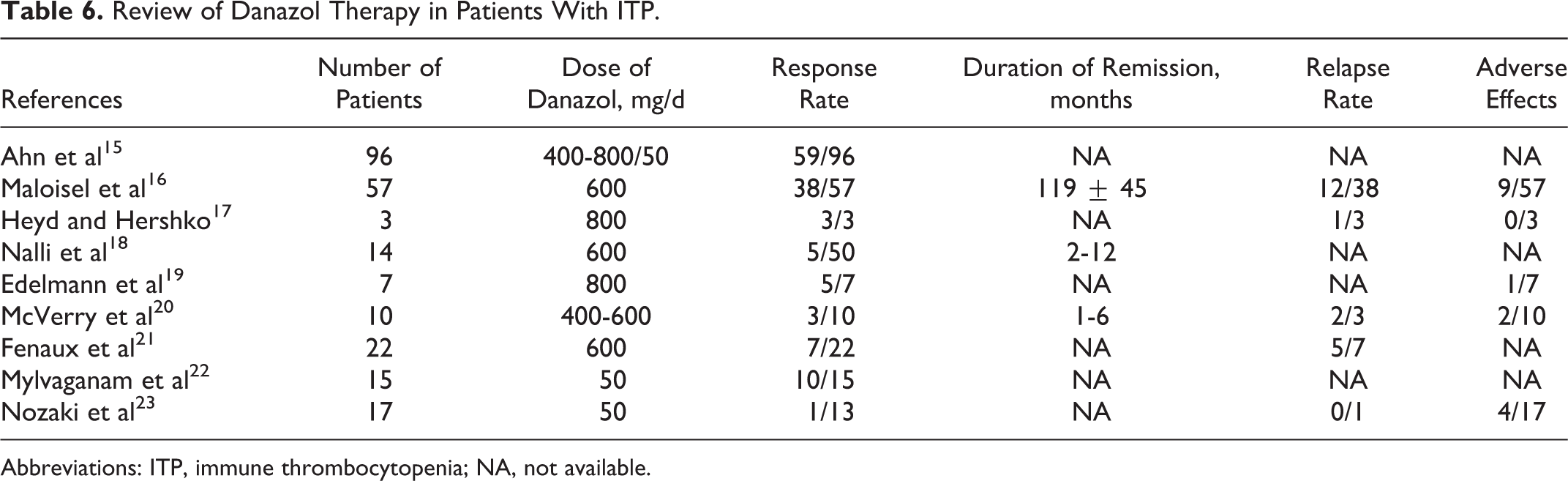
Abbreviations: ITP, immune thrombocytopenia; NA, not available.
In addition, we found that both age and number of previous therapies were related to danazol response. In our study, the response rate declined with increasing age in women, which was opposite to the findings reported by Ahn et al. 15 This discrepancy may be due to the following reasons: (1) variances in hormone levels between Chinese and other populations; (2) differences in disease stage and concomitant therapy administered to study patients; and (3) the low-to-medium danazol dose may be insufficient to completely override estrogen even in old women, and other immune modulation mechanisms of danazol such as enhancing cell responses to pokeweed mitogen, inhibiting lymphocyte blastogenic responses, and regulating lymphocyte ratios may play a dominant role in functional mechanisms. 22,24
Unlike most previous studies, we administered low-to-medium dosages of danazol instead of the traditional dosage (600 mg/d). 13,15 –21 We also observed beneficial effects with this dosage regimen and found no significant correlation between danazol dose and response. Some previous studies had evaluated the efficiency of very low danazol doses (50 mg) for the treatment of ITP, and some of them reported good responses. 22,23,25,26 These results verified the efficiency of low-dose danazol. In our study, the median time to response was shorter than the majority of previous studies, and 15,16,22,25 most of the patients (77.4%) acquired response within 3 months, while some others’ responses occurred as late as 12 months or even later. Therefore, we suggest that patients who did not respond to danazol can prolong the therapy time properly for responses.
Among responders in this study, maintenance therapy status was related to recurrence. Relapse increased when patients discontinued danazol treatment, although it was not related to the reduction in danazol dosage. Our study also showed that prolonged danazol treatment was more likely to result in sustained remission. In patients who received danazol treatment for more than 12 months, over 60% of patients remained in remission at the last follow-up. Therefore, it was more appropriate to use danazol at low doses for long-term therapy.
Although there was no difference in response between newly diagnosed patients with ITP who received danazol and those who did not, thrombocytopenia relapse was improved in those who received combination therapy. Barbieri et al 27 showed that danazol can bind to steroid-binding globulin and enhance their accessibility to other tissues by displacing and freeing active hormones. The synergistic action of glucocorticoid and danazol permitted tapering of glucocorticoids, which can lessen the side effects of high-dose glucocorticoid therapy. There were also no additional AEs with this combination therapy. Therefore, early administration of a combination of danazol and glucocorticoids can reduce recurrence in patients with ITP, which may be useful to “buy time” until “spontaneous” improvement occurs.
Danazol can also suppress menses effectively, providing additional benefit to women who have clinically significant menometrorrhagia. Moreover, as reported previously, 28 we noticed improvement in hemorrhagic symptoms even in nonresponders, suggesting the favorable effects of danazol on vessel wall integrity.
Concerns about excessive androgen and side effects had limited the application of danazol before. While in our 5-year follow-up, the side effects of low-to-medium dose of danazol were well within acceptable limits, and only 1.2% of patients discontinued therapy due to unacceptable side effects. All of the adverse reactions could be in remission after danazol reduction or withdrawal. Liver damage was the most common adverse effect of danazol therapy. However, the incidence of liver damage was lower in our study than others. 15,16 This may be related to the administration of low-to-medium doses of danazol. Farkas et al 29 suggested that when administered at the lowest effective dose, danazol does not induce liver injury. However, hepatic adenomas and cancer might have been related to high dose of danazol therapy (400-800 mg/d) over several years. 30,31 In our study, the occurrence of other side effects was also less than traditional therapies. 15,16 Therefore, low-to-medium dose of danazol was better tolerated in ITP therapy.
In conclusion, danazol appears to be an effective, well-tolerated, and cost-effective therapy for patients with ITP, as the major goal of ITP treatment is to provide safe platelet counts rather than correcting the values to normal levels. In patients with persistent or chronic ITP, danazol would be an attractive option to acquire remission without the long-term complications of glucocorticoids, with the potential to avoid the need for splenectomy. In addition, the combination of danazol and glucocorticoids for initial therapy can decrease relapse efficiently. Based on the results of this study, we suggest low-to-medium dose of danazol instead of traditional dosage. Danazol should be taken continuously for 3 months at least for responses, and prolonged therapy may be needed in some patients. Maintenance therapies of danazol were necessary to sustain remission. Due to its retrospective design, our study has several limitations. One was that we were not able to acquire all drug-related side effects extensively, and some mild AEs might be ignored or forgotten by patients. We also did not recommend a specific therapy scheme of danazol. Large-scale prospective randomized trials are needed to verify our findings and determine the optimal usage of danazol.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by grants of National Natural Science Foundation of China (81270581, 81300385, and 81470286), Tianjin Municipal Science and Technology Commission (14JCZDJC35100), Peking Union Medical College Innovation Fund (10023-0710-1007), and Specialized Research Fund for the Doctoral Program of Higher Education (20131106120039).