
Abstract
Celiac disease (CD) is a disease of the small intestine caused by an immune response to ingested gluten. Idiopathic thrombocytopenic purpura (ITP) is a common acquired bleeding disorder of childhood. It may follow a viral infection or immunization and is caused by an inappropriate response of the immune system. Autoimmune thyroiditis (AT) is a disease that occurs due to autoimmune mechanisms. Celiac disease associated with autoimmune thyroid disease is well known, but the association of CD, autoimmune thyroid disease, and ITP has been reported very rarely in the literature. In the current report, we have presented a case with CD, AT, and acute ITP, because this association is rarely seen, and to emphasize that CD and AT should be kept in mind in patients with ITP.
Introduction
Celiac disease (CD) is a disease of the small intestine caused by an immune response to ingested gluten. This response results in characteristic damage to the villi, leading to malabsorption. 1 Idiopathic thrombocytopenic purpura (ITP) is a common acquired bleeding disorder in the childhood period. It may follow a viral infection or immunization and is caused by an inappropriate response of the immune system. 2 The disease is characterized by thrombocytopenia, shortened platelet survival, antiplatelet antibodies in plasma, and increased number of megakaryocytes in bone marrow. 2 Idiopathic thrombocytopenic purpura mostly appears as extensive cutaneous bleeding, such as petechia, purpura, and ecchymosis, in an otherwise healthy child, and it usually has a short duration and good prognosis. 3 Autoimmune thyroiditis (AT) is a disease that occurs due to autoimmune mechanisms. Stimulation of B-lymphocytes responsible for humoral immunity by T-lymphocytes which are responsible for cellular immunity, and autoantibodies produced by B cells against thyroid tissue components and their secretions play roles in the development of the disease. 3 Autoimmune thyroiditis is more commonly seen in patients with genetic susceptibility and in girls. 3
In the present report, we have presented a case with CD, AT, and acute ITP due to this rare association and emphasized that CD should be kept in mind in a patient with ITP.
Case Report
A 2-year-old girl was admitted to the emergency department with fatigue and petechial rash lasting for a week. We also learned that she had 4 abundant bleeding attacks from noise, which had begun 1 week ago and which had been noted on the day prior to admission to our hospital. In her previous history, abdominal distention was noted, which had begun at the age of 6 months, after the start of nutrition other than breast milk. Family history was unremarkable. Both body weight (7.4 kg, −3.4 standard deviation score [SDS]) and height (71 cm, −3.9 SDS) were under the third percentile. Vital signs were normal. On physical examination, pale skin and mucosa, petechial rash on the lower extremities, and melena were noted. Other system examinations were normal. On laboratory analysis, complete blood count was normal, except for a mild anemia (hemoblobin: 8 g/dL) and thrombocytopenia (41x109L−1). On peripheral blood smear examination, no blasts or immature cells were seen. The reticulocyte count was measured as <1% (N: <1%). Serum electrolytes, serum glucose, liver and renal function tests, cholesterol, and triglyceride levels were within normal ranges. Although thyroid hormone values were normal, thyroid peroxidase antibodies (anti-TPO), and anti-thyroglobulin antibody (anti-TG) were found to be 26.48 IU/mL (N: 0.00-5.61 IU/mL) and 36.6 IU/mL (N: 0-4.11 IU/mL), respectively. Thyroid ultrasonographic examination revealed hypoechogenic areas and heterogeneity due to these hypoechogenic areas. C-reactive protein was negative; erythrocyte sedimentation rate was 12 mm/h. Serum vitamin B12 (937 pg/mL; N: 198-987 pg/mL) and folate (8.51 ng/mL; N: 3-17 ng/mL) levels were normal. Prothrombin time and activated partial thromboplastine time were 10.7 seconds (normal: 11-14 seconds) and 24.2 seconds (normal: 30-40 seconds), respectively. Serum iron, iron-binding capacity, and ferritin level were 69.8 μg/dL (N:40-100 mg/dL), 376 μg/d L
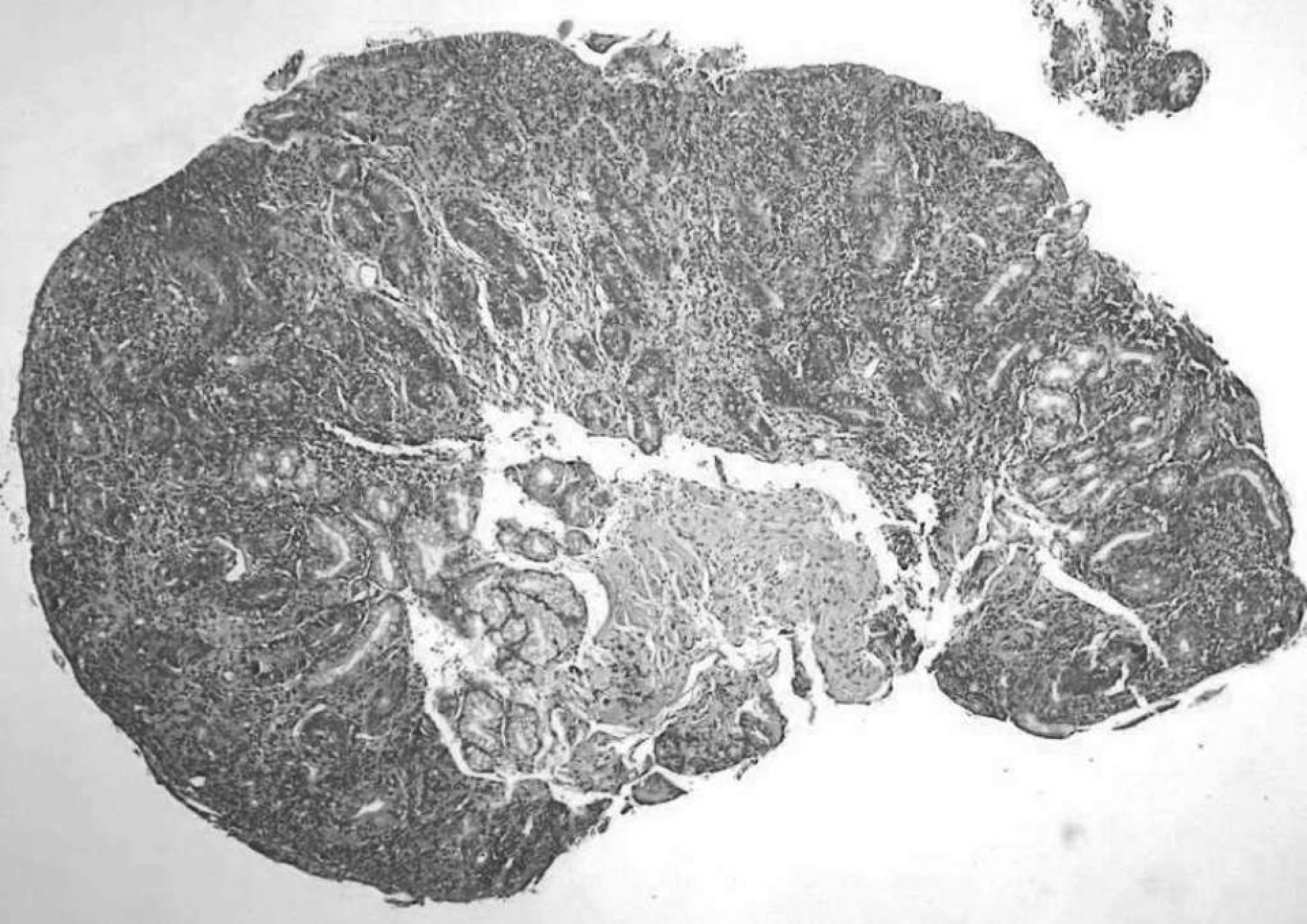
Intestinal biopsy shows villous atrophy with hyperplasia of the crypts.
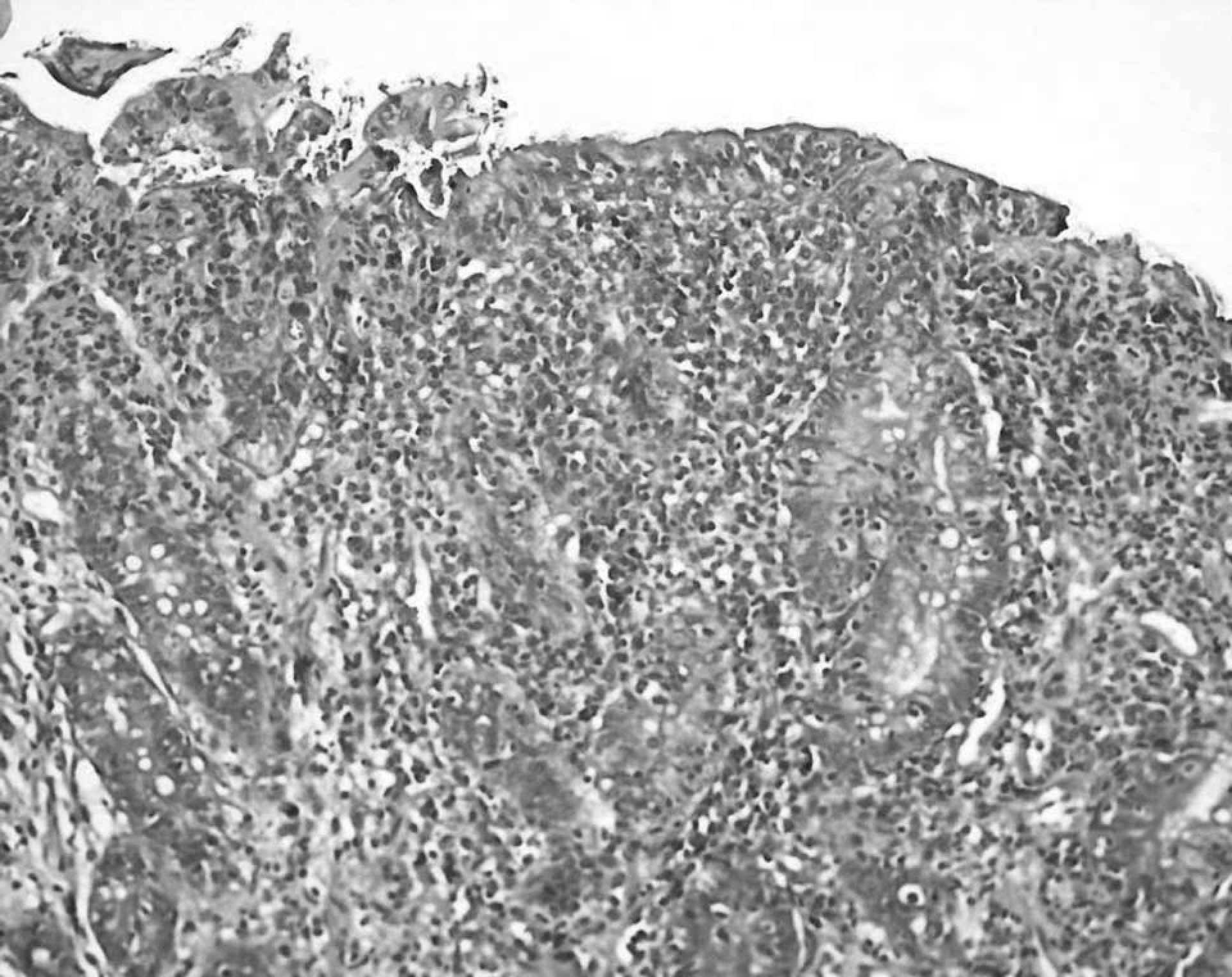
Intestinal biopsy shows lymphoplasmocyter cells infiltration in lamina propria and increased intraepithelial lymphocyte count (above 40%; Marsh type 3c).
Discussion
Celiac disease is one of the most common chronic disorders in childhood. Between the ages of 2.5 and 15 years, its prevalence is 3 to 13 per 1000 children. 1 In genetically susceptible individuals, the disorder develops after exposure to gluten, which is found in cereals like wheat, rye, and barley. Environmental factors such as the amount and timing of gluten administration in infancy, and breastfeeding, may also play a role in the expression of the genetic predisposition. 1 Although serological markers such as antiendomysial and tissue transglutaminase antibodies are highly sensitive and specific, false-negative results can be encountered, especially in children under 2 years of age and children with mild enteropathy or IgA deficiency. 4 Histological examination of small bowel biopsy is the gold standard for the diagnosis of CD. In our patient, all of the serological markers for CD were positive. Furthermore, the diagnosis was confirmed by intestinal biopsy. The hematological manifestations of CD include anemia owing to iron, folate, or vitamin B12 deficiency, coagulopathy owing to vitamin K deficiency, and rarely leukopenia and thrombocytopenia.1,4 Our patient had thrombocytopenia on admission. Although iron, folate, or vitamin B12 deficiency anemias are frequent in classic CD, serum folate, vitamin B12 levels, and transferrin saturation may be normal in silent forms. Anemia, in our case, was assumed to be due to epistaxis attacks.
Clinically, autoimmune thyroiditis (AT) can manifest, depending on the presence or absence of goiter, in either a goitrous form or an atrophic form. Both are characterized by the presence of thyroid antibodies in serum, with the goitrous form being more common in children. The diagnosis of AT can be made on the basis of either (a) cytomorphological features of chronic lymphocytic thyroiditis on fine-needle aspiration (FNAC) or (b) significant titers of thyroid antibodies. Furthermore, on ultrasonographic examination of the thyroid gland, the presence of a diffuse goiter or hypoechogenic areas, and heterogeneity due to these areas can be accepted as supporting findings. 5 In our patient, AT was diagnosed by the presence of thyroid autoantibodies (anti-TPO and anti-TG) and ultrasonographic examination.
Idiopathic thrombocytopenic purpura is a common acquired bleeding disorder in the childhood period. It is a benign disease characterized by increased destruction of the circulating platelets and diagnosed by excluding the other causes of thrombocytopenia. 2 The diagnostic criteria of acute ITP are as follows: thrombocytopenia (platelet count <150 × 109L−1), increased megakaryocytes in bone marrow aspiration examination, and absence of any other disease that can cause thrombocytopenia. 2 In our patient, the diagnosis of acute ITP was made by the presence of these criteria. Thrombocytopenia and increased megakaryocyte on bone marrow examination were found in our patient.
Autoimmune diseases such as diabetes mellitus, rheumatoid arthritis, thyroiditis, Addison disease, autoimmune hepatitis, myasthenia gravis, pernicious anemia, and alopecia have been reported at a higher than expected prevalence in patients with CD, particularly with subclinical or silent disease on gluten-containing diet.1,4 Celiac disease associated with AT is well known, but the association of CD, autoimmune thyroid disease, and ITP has been reported very rarely. One of them was presented by Altıntas et al 6 In that study, the authors investigated the prevalence of anti-TPO and anti-TG, AGA IgG, IgA, EMA IgG, and IgA antibodies in 74 patients with chronic ITP and in 162 healthy controls, and finally the author suggested that patients with chronic ITP should be examined for development of AT and CD. In another study which was carried out to investigate a possible association between CD and ITP and vice versa, a positive association between CD and both ITP of any type and chronic ITP was found. 7 The association between celiac disease, ITP, and thyroid disease probably reflects the general increase in autoimmune disease seen in celiac disease 8 and may be explained by the presence of shared genetic traits. Both human histocompatibility leukocyte antigen (HLA) DQ2 (HLA-DQA1*05-DQB1*02) and DQ8 (HLADQA1*03-DQB1*0302) are common in thyroid disease 9 and CD, 10 and patients with overlapping disease are often HLA-DQ2-positive. 11 Moreover, Eliakim et al have suggested that the link between CD and ITP may be genetic through the human leukocyte antigen (HLA) system. 12 Another potential explanation may be found in the increased expression of T lymphocyte-associated antigen 4 (CTLA4). CTLA4 is a T-cell surface molecule involved in the control of T cell proliferation. An increased expression of CTLA4 has been seen in both Graves' disease and hypothyroidism. 13 CTLA4 is also more common in celiac disease. 14 In a study performed by Zhang et al, the efficacy of CTLA4-immunoglobulin in suppressing the pathological autoimmune responses in ITP was demonstrated. 15 The presence of shared genetic risk factors may therefore explain the positive association between CD, ITP, and thyroid disease.
In the current report, first, the patient was diagnosed with ITP. Therefore, the patient was given IVIG treatment. Due to the presence of short stature and malnutrition, CD was investigated and diagnosed. After diagnosis of CD, the possible association of other autoimmune disorders was investigated and autoimmune thyroid disease was detected. On the follow-up, we observed that the patient was unresponsive to IVIG treatment. After establishment of the diagnosis of CD, a gluten-free diet was given to our patient. No additional treatment was administered. With the gluten-free diet, a recovery in the thrombocyte count was detected (Figure 3).
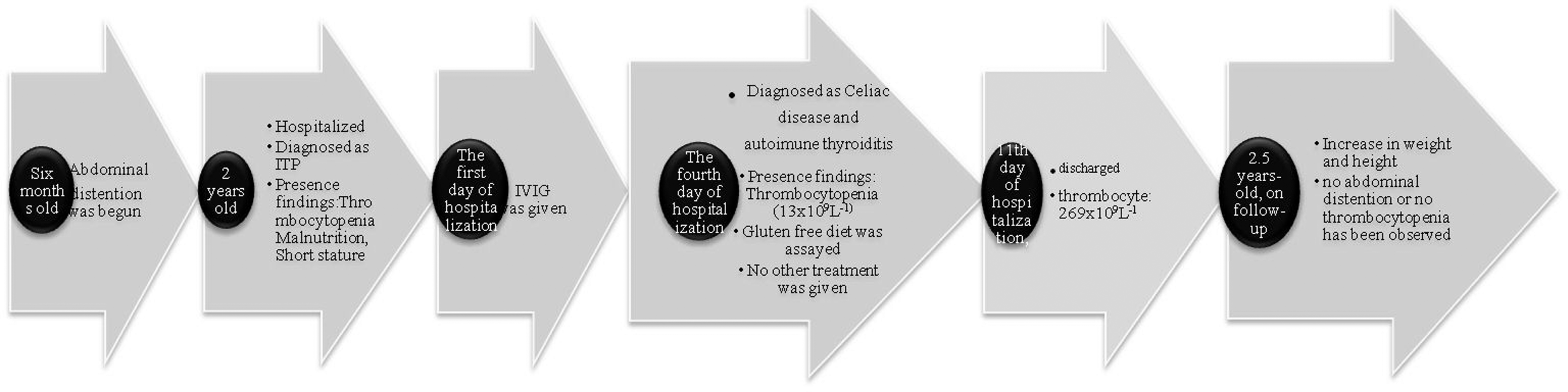
The important values for the 3 conditions serially over time are shown.
In conclusion, with this report, we emphasized that CD should be kept in mind in patients with ITP who have symptoms suggesting CD, such as abdominal distention, short stature or malnutrition, as in our case. We also think that a gluten-free diet may be an answer for the treatment of thrombocytopenia in acute ITP patients with CD. Furthermore, we also suggest that patients with ITP can be investigated for other autoimmune disorders, especially AT.
Footnotes
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
The authors received no financial support for the research and/or authorship of this article.