
Abstract
Many risk factors may contribute to renal disease in patients with hemophilia A.
Aim:
We aimed to evaluate functional and structural renal abnormalities among a group of Egyptian children with severe and moderate hemophilia A using technetium-99m diethylene triamine pentaacetic acid (99mTc-DTPA) and technetium-99 m dimercaptusuccinic acid (99mTc-DMSA) scan. We also aimed to determine the relation between these abnormalities and different risk factors and disease severity.
Patients and methods:
Forty male patients, 16 with severe and 24 with moderate hemophilia A, were enrolled in this study. Their mean age was 10.2 ± 4.3 years (range, 5-17 years). Full history taking, clinical examination, laboratory, and radionuclide investigations including serum creatinine, blood urea nitrogen (BUN), urine analysis, creatinine clearance, 24-hour urinary protein, 99mTc-DTPA scan, and 99mTc-DMSA scan were performed to all enrolled patients.
Results:
Serum creatinine and BUN were normal in all patients, and corrected creatinine clearance was diminished in 2 patients. However, 99mTc-DTPA results yielded 19 (47.5%) patients with diminished glomerular filtration rate (GFR). Moreover, it showed that 14 (35%) had obstructive uropathy, 15 (37.5%) had obstructive nephropathy, while 11 (27.5%) patients showed normal scan. One patient had atrophy of 1 kidney on 99mTc-DMSA scan. Among our cohort, 5 (12.5%) patients were hypertensive. Microscopic hematuria was detected in 14 (35%) patients while 72.5% had proteinuria. We found an association between hematuria and hypertension with diminished GFR.
Conclusion:
Despite normal kidney functions (serum creatinine and BUN), we found a high rate of diminished GFR and obstructive uropathy and nephropathy as detected by 99mTc-DTPA scan among children with hemophilia A.
Introduction
Hemophilia A is an X-linked inherited bleeding disorder, which results from deficiency of coagulation factor VIII. According to the degree of factor VIII deficiency, mild, moderate, and severe forms are recognized. Patients with severe hemophilia experience frequent episodes of spontaneous or excessive bleeding after minor trauma, especially in the joints. 1 Kulkarni et al 2 changed the general belief that renal disease is a rare complication of patients with hemophilia and found acute or chronic renal disease in 2.9% of hospitalized patients with hemophilia.
Several risk factors may predispose patients with hemophilia to develop renal disease including hypertension, older age, diabetes, viral infection, and kidney bleeding. 2 Spontaneous gross or microscopic hematuria is relatively common in patients with hemophilia A and is often incidentally detected. 3 Acute renal obstruction may occur following treatment of a bleeding episode with an antifibrinolytic agent such as tranexamic acid or epsilon aminocaproic acid. 4,5 Transfusion-acquired infections with HIV and hepatitis may occur in patients receiving plasma-derived concentrates thus causing a spectrum of renal diseases. 6
Nuclear medicine techniques are mostly used for functional renal imaging and quantification, often providing information not possible with the anatomic or structural modalities. This includes evaluation of blood flow and viability, differentiation of obstructive and nonobstructive hydronephrosis, confirming urinary leaks, and diagnosing acute pyelonephritis. Dynamic functional studies by diethylene triaminepentaacetic acid
Renal cortical imaging by dimercaptosuccinic acid (DMSA) scan evaluates viability, infection, and structural abnormalities difficult to assess by ultrasound and computed tomography. Roughly 40% of the injected dose localizes in the cortex, predominantly in the proximal tubules. 7
There are few publications about the evolution of renal abnormalities in pediatric patients with hemophilia A. In view of previous data, this study was designed to evaluate functional and structural renal abnormalities among a group of Egyptian children with severe and moderate hemophilia A using technetium-99m diethylene triamine pentaacetic acid (99mTc-DTPA) and technetium-99 m dimercaptusuccinic acid (99mTc-DMSA) scans. We also aimed to determine the relation between these abnormalities and different risk factors and disease severity.
Patients and Methods
Patients
This cross-sectional study was conducted at the Pediatric Hematology Clinic in collaboration with Nuclear medicine Unit, Ain Shams University, in the period from January to November 2014. Forty patients with hemophilia A were consecutively enrolled in this study during their regular follow-up visits in the clinic. They comprised 16 patients with severe hemophilia A and 24 patients with moderate hemophilia A. Their age ranged from 5 to 17 years. Severity level was categorized as moderate if factor VIII activity > 1% to 5% and severe if factor VIII activity ≤1%. Four patients with severe hemophilia A were on modified prophylaxis with factor VIII concentrates, while the remaining 14 patients with severe and all patients with moderate hemophilia A were receiving on-demand therapy. Exclusion criteria included patients with inhibitors, patients with known congenital or acquired renal disease and renal stones, and patients with diabetes mellitus. Patients were further divided into subgroups according to age (≤12 and >12 years), presence or absence of hematuria, hypertension, hepatitis C virus (HCV) infection, and obstructive uropathy/nephropathy. Obstructive uropathy is defined as renal outflow blockade of variable causes with preserved renal function. If it is left untreated it may result in permanent renal damage, that is, obstructive nephropathy. 7 The study was approved by the Medical Ethics Committee of Human Experimentation of Ain Shams University. Informed consent was obtained from patients or their legal guardians before enrollment.
History and Examination
All recruited patients were subjected to detailed history taking and complete physical examination. Data collected included age of the patients at evaluation, type and severity of hemophilia, history of gross hematuria including number of attacks, history of abdominal trauma, lumbar pain, and medications associated with the episodes of hematuria. Data of inhibitors (neutralizing antibodies against factor VIII), HCV, HBV, and HIV status were recorded from patients’ medical records. The age of the patients at the first episode of gross hematuria was 8 to 10 years (mean age 9.1 years). The number of episodes of gross hematuria was once in 1 patient and twice in 3 patients. Patients with gross hematuria needed hospital admission for 4 to 10 days, where they received factor VIII concentrates or cryoprecipitate till the resolution of hematuria. During the episodes of hematuria (either gross or microscopic), no patient received tranexamic acid.
Blood pressure was measured in accordance with the current recommendations of the American Heart Association. 8 Hypertension in children and adolescents is defined as systolic and/or diastolic blood pressure that is consistently equal to or greater than the 95th percentile of the blood pressure distribution. 9 Patients with hypertension received oral angiotensin-converting enzyme inhibitor to control hypertension.
Laboratory Tests
Routine urine analysis and culture were done to detect patients with microscopic hematuria and to diagnose urinary tract infection. Hematuria was defined as the presence of at least 5=red blood cells per microliter of urine. 10 Urine analysis was repeated 3 consecutive times to detect patients with persistent microscopic hematuria. Colorimetric estimation of total 24-hour urinary protein was done using “pyrogallol red” (DiaSys, Diagnostic Systems International, USA). 11 Normal protein excretion in children is defined as 150 mg/24 hour or more specifically ≤4 mg/m2/h, mild proteinuria is defined as 4 to 40 mg/m2/h, and nephrotic range is defined as >40 mg/m2/h. 12
Serum creatinine, blood urea nitrogen (BUN), and creatinine clearance assessment was carried out on Synchron CX7 auto analyzer (Beckman Instruments, Brea, California). Serum creatinine and BUN were classified according to standard normal ranges for age and sex. 13 Creatinine clearance (CrCl) was calculated from 24-hour urine specimens. Normal value ranges from 97 to 137 mL/min/1.73m2. 14 All patients were referred to the nuclear medicine unit in radiodiagnosis department to perform renal (99mTc-DTPA and 99mTc-DMSA) scintigraphy for renal function and cortical scarring assessment.
99mTc-DTPA Scan
For 99mTc-DTPA dynamic renography, children received an intravenous hydration with dextrose 5% in 0.45% normal saline, 10 to 15 mL/kg over 30 minutes. Patients voided before starting the study. The dose of 99mTc-DTPA in children was 200 μCi/kg (2 mCi minimum and 10 mCi maximum). Large field-of-view Phillips Bright view gamma camera was used with a low-energy, parallel-hole collimator, and a photo peak of 15% to 20% window centered over 140 keV. One- to 2-second frames for 60 secondds were taken for blood flow phase, and 30-second frames for 25 minutes were taken for dynamic phases. Furosemide (1 mg/kg up to 40 mg) was slowly infused intravenously. Postvoid images were taken. Region of interests were drawn around kidneys and for background area. Time–activity curves were generated for 60-second flow phase and for 25-minute dynamic study. The differential renal function was calculated based on the relative counts accumulated in each kidney during the second minute after injection of furosemide. 7 Patient’s glomerular filtration rate (GFR) as estimated from DTPA was described as normal or decreased according to the chronic kidney disease (CKD) classification. Cutoff values were determined for the 2 different age-groups, 2 to 12 and 13 to 21 years. For 2 to 12 age-group, GFR less than 106 was considered decreased, while for group 13 to 21, GFR less than 110 was considered decreased. 15
99mTc-DMSA Scan
To perform cortical renal scintigraphy the dose of 99mTc-DMSA was 50 mg/kg (minimum dose of 600 μCi) the same steps of patient hydration as diuretic dynamic renography were followed. Large field-of-view Phillips Bright view gamma camera was used with a parallel-hole collimator for differential calculation and a pinhole collimator for cortical images. Radiopharmaceutical was injected intravenously. Images were taken at 2 hours after injection. Posterior and posterior oblique views were taken, and an additional anterior view was performed in case of horseshoe kidney or ectopic pelvic kidney. Large regions of interest were drawn around the kidneys, using highly contrasted images. Parallel collimator images were acquired for 500 k on anterior and posterior views for differential calculation. Function was quantified as geometric mean (square root of the product of anterior and posterior counts). 7
Statistical Methods
Data were analyzed using Statistical Software Package SPSS (version 10). Numeric data were expressed as mean values and standard deviation (SD). Data analyzed using Student t test for quantitative data and chi square test (χ2) for qualitative data. Analysis of variance (ANOVA F test) was used for comparing means of more than 2 groups. P values <.05 were considered significant.
Results
This study included 40 male patients with hemophilia A, and their mean age was 10.2 ± 4.3 years (range, 5-17 years). Fourteen (35%) patients were more than 12 years. They comprised 16 patients with severe hemophilia A and 24 patients with moderate hemophilia A. Table 1 shows the characteristics of the studied population. Protein excretion in 24 hours urine was normal in 11 (27.5%) patients, 29 (72.5%) patients had mild proteinuria, however, none of the enrolled patients showed nephrotic range proteinuria. Serum creatinine and BUN were within normal ranges among the studied patients. However, corrected creatinine clearance was diminished in 2 (5%) patients, and 99mTc-DTPA GFR was diminished in 19 (47.5%) patients (10 patients with severe hemophilia Aand 9 patients with moderate hemophilia A).
Characteristics of the Studied Patients With Hemophilia A.
Abbreviations: BMI, body mass index; GFR, glomerular filtration rate; HBV, hepatitis B; HCV, hepatitis C virus; SD, standard deviation; 99mTc-DTPA, technetium-99m diethylenetriamine pentaacetic acid.
Fourteen (35%) patients had microscopic hematuria detected upon routine urine examination; 4 (28.6%) of them had history of previous attacks of gross hematuria, and they were all patients with severe hemophilia A. In these patients, hematuria was not related to trauma, infection, or medications. In all, 57% of them were older than 12 years of age showing a statistical significant difference compared to patients without hematuria (P = .03). They had significantly higher mean value of 24-hour urinary protein (P = .008), yet presence of hematuria was not associated with disease severity or HCV infection (P = .34, .08, respectively). Moreover, they had significantly lower mean value of 99mTc-DTPA GFR (P = .02; Table 2). Three patients with severe hemophilia A and gross hematuria had a suboptimal 99mTc-DTPA GFR due to bilateral obstructive uropatehy and early nephropathy. Figure 1 shows 99mTc-DTPA scan of a patient with gross hematuria and obstructive nephropathy.
Comparison Between Patients With and Without Hematuria Regarding Demographic, Clinical, and Laboratory Parameters.
Abbreviations: BMI, body mass index; GFR, glomerular filtration rate; HCV, hepatitis C virus; SD, standard deviation; 99mTc-DTPA, technetium-99m diethylenetriamine pentaacetic acid.
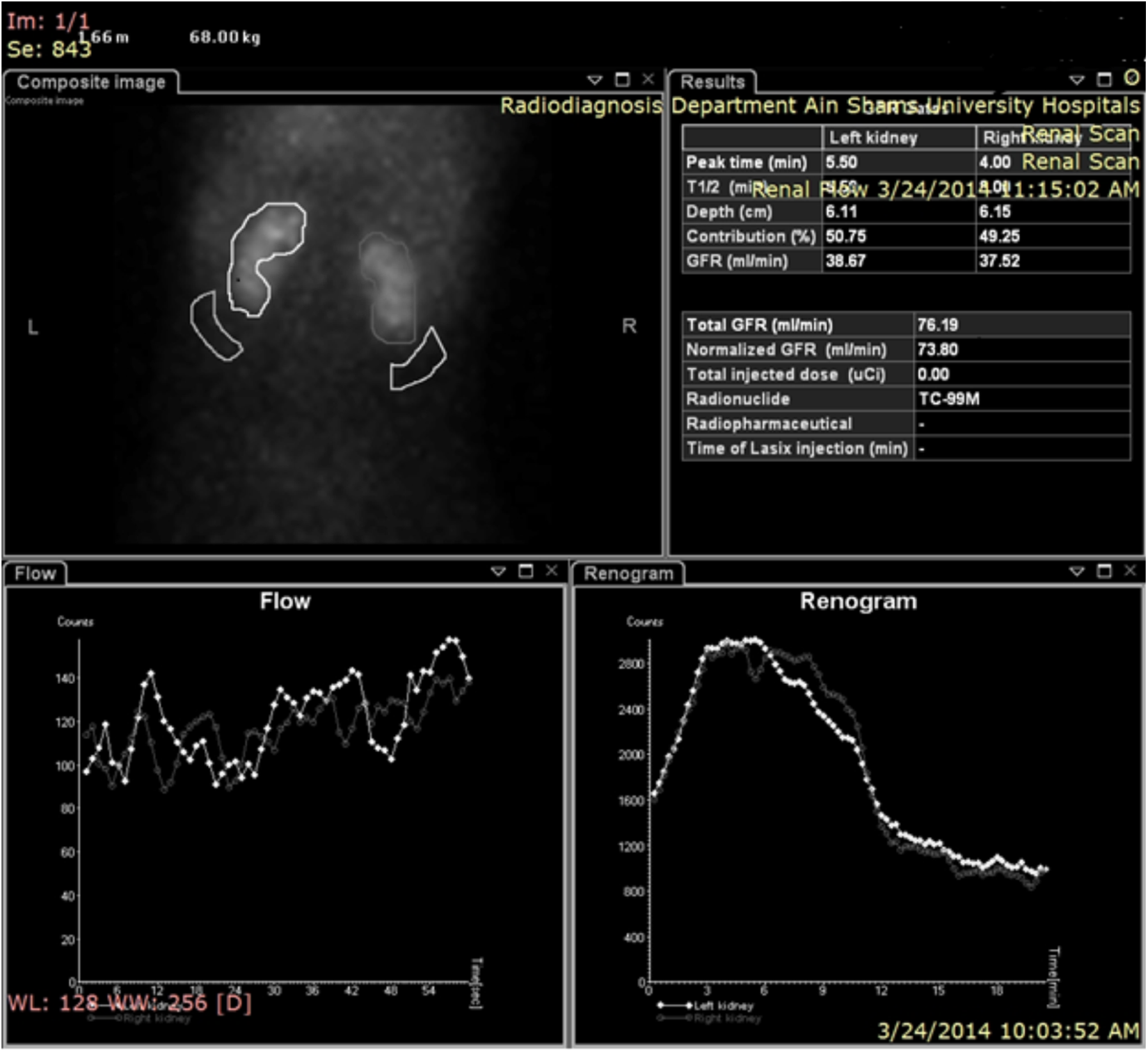
Haemophilia A patient aged 14 years old presented with gross haematuria. Diuretic DTPA renography revealed bilateral tracer stasis in the pelvicalyceal system manifested as prolonged transit time in both renograms in the lower right quadrant of the image. GFR is suboptimal.
Among our cohort, hypertension was found in 5 (12.5%) patients. Showing an association with hematuria, where, 80% (4 out of 5) of the patients with hypertension suffered attacks of gross hematuria (P = .04; Table 2). Patients with hypertension compared to normotensive ones were significantly older (all were older than 12 years, P = .003), with higher mean weight SD (t = 2.97, P = .005), height SD (t = 2.57, P = .04), and body mass index (BMI; t = 4.69, P = .0001). Also, they showed significantly lower mean value of 99mTc-DTPA GFR (t = 2.25, P = .03) and higher 24-hour urinary protein (t = 2.88, P = .006). Figure 2 shows DTPA scan of a patient with hypertension having suboptimal GFR and early nephropathy. Furthermore, there was an association between hypertension and HCV infection, where 80% of patients with hypertension suffered from chronic HCV infection (P = .003).
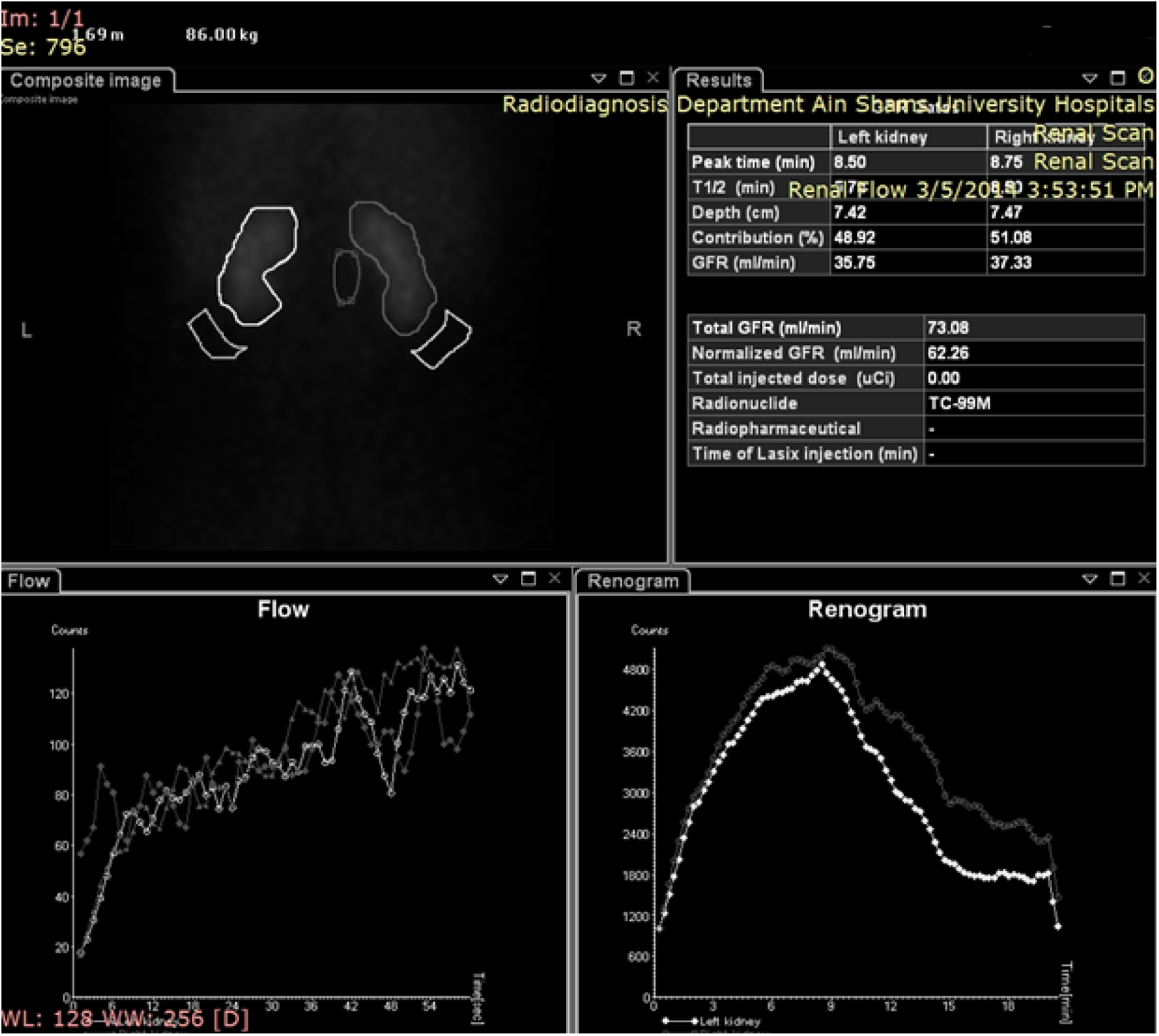
Haemophilia A patient aged 17 years is presented with hypertension. DTPA diuretic renography revealed early nephropathic changes manifested by delayed upstroke and low amplitude of both renograms in the right lower quadrant of the image. GFR is suboptimal.
Regarding structural abnormalities evident by 99mTc-DTPA renogram curve, 14 (35%) patients had obstructive uropathy (4 unilateral and 10 bilateral) and 15 (37.5%) patients had obstructive nephropathy (3 unilateral and 12 bilateral). Eleven (27.5%) patients had normal 99mTc-DTPA renogram. Patients with obstructive uropathy had a preserved renal perfusion, however with tracer stasis in the dilated pelvicalyceal system that was partially relieved after intravenous (IV) furosemide injection. The associated renogram showed delayed broad peak with rapid downslope after IV furosemide injection. Patients with obstructive nephropathy had decreased perfusion of both kidneys with poor tracer handling throughout the whole study in both the early and the delayed scans. This was associated with an abnormal renogram, decreased amplitude, and broad peaking and abnormal shape (plateau). 99mTc-DMSA scan results were normal for all patients except one who had atrophic right kidney (Figure 3). Patients with obstructive nephropathy showed significantly higher age (60% were older than 12 years, P = .04), weight SD (P = .01), height SD (P = .004), mean value of 24-hour urinary proteins (P = .01) and significantly lower mean value of 99mTc-DTPA GFR (P = .0001) than patients with obstructive uropathy and those with normal 99mTc-DTPA scan. Also, there was a significant association between patients with obstructive nephropathy and hypertension (P = .03), and 80% (4 of 15) of patients with obstructive nephropathy were hypertensive (Table 3).
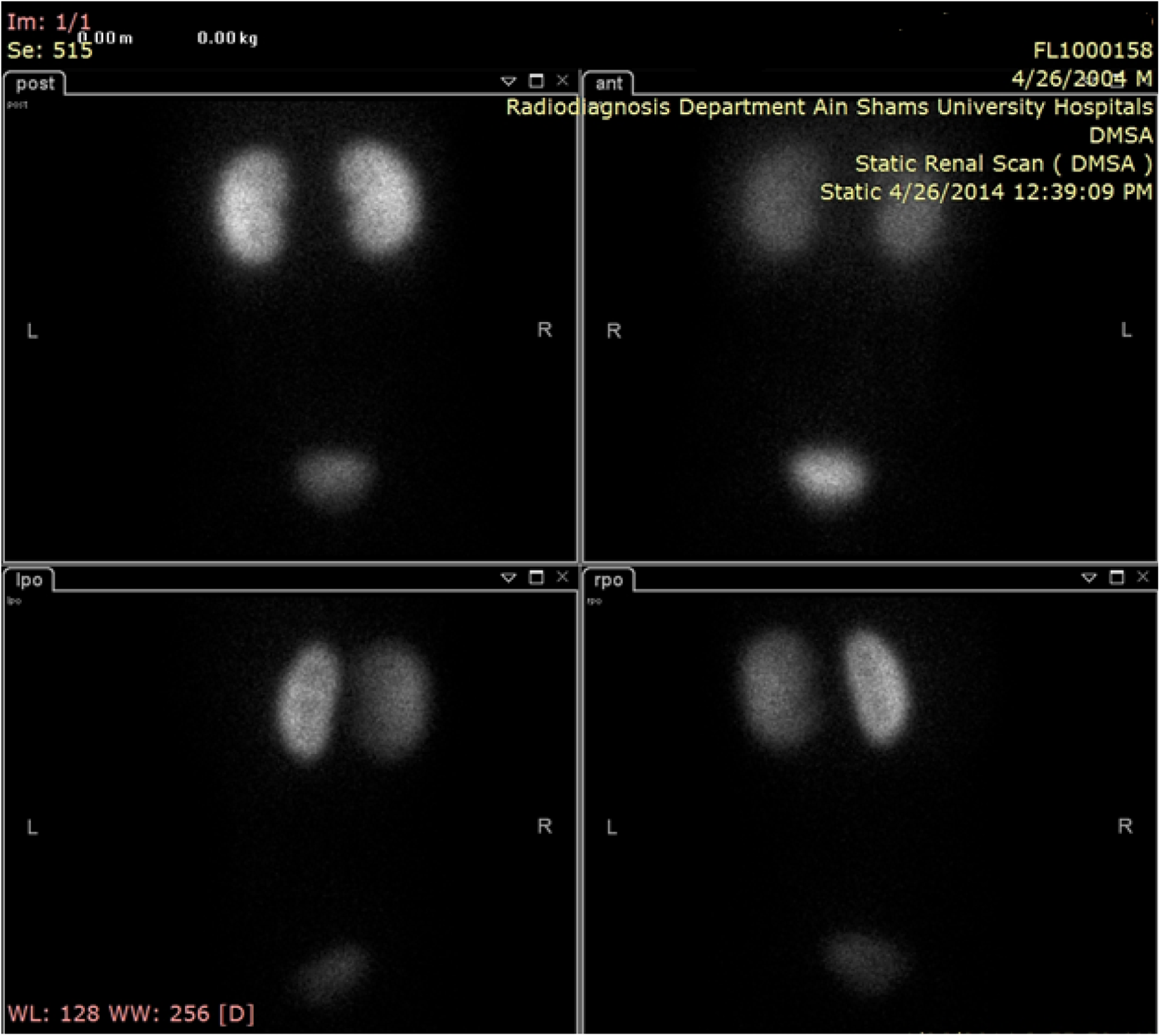
Haemophilia patient aged 10 years is evaluated by DMSA which proved to be negative for cortical scarring. Both kidneys show homogenous cortical regular smooth tracer uptake in anterior, posterior and both oblique views.
Comparison Between Patients With Normal DTPA Scan, Obstructive Uropathy, and Obstructive Nephropathy Regarding Demographic, Clinical, and Laboratory Parameters.
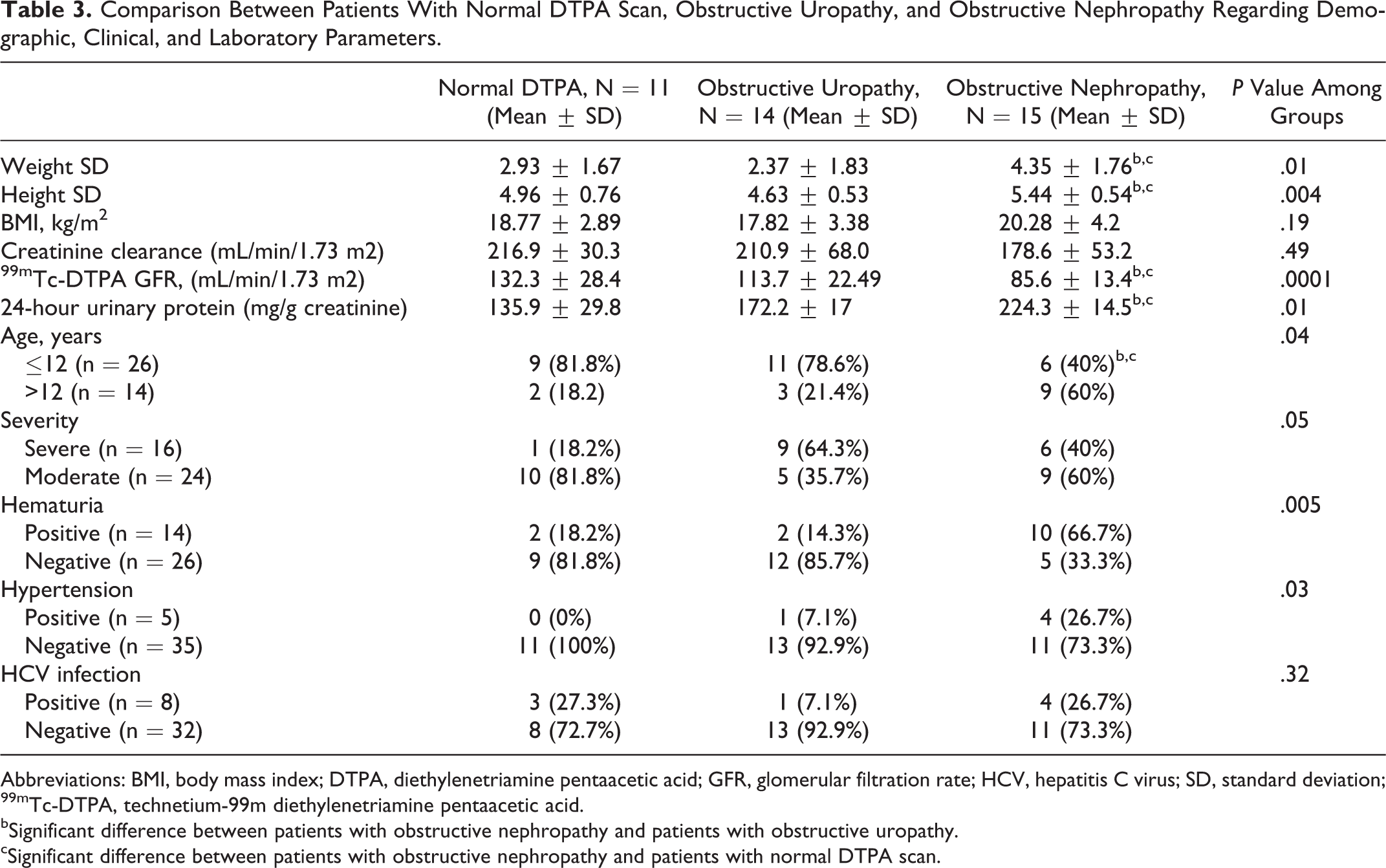
Abbreviations: BMI, body mass index; DTPA, diethylenetriamine pentaacetic acid; GFR, glomerular filtration rate; HCV, hepatitis C virus; SD, standard deviation; 99mTc-DTPA, technetium-99m diethylenetriamine pentaacetic acid.
bSignificant difference between patients with obstructive nephropathy and patients with obstructive uropathy.
cSignificant difference between patients with obstructive nephropathy and patients with normal DTPA scan.
Discussion
In this report, despite normal kidney functions as evaluated by serum creatinine and BUN for all patients with hemophilia A, corrected creatinine clearance was diminished in 5% and 99mTc-DTPA GFR was diminished in 47.5%. Kidney function is best measured as GFR, and a diminished or decreasing GFR is a good index of chronic kidney disease. A decrease in GFR precedes kidney failure in all forms of progressive kidney disease. Consecutively, monitoring of changes in GFR can detect kidney disease progression. Creatinine is a breakdown product of muscle metabolism. It is primarily excreted through the glomerular filtration and 10% is actively secreted by the proximal tubules. Tubular secretion increases when GFR decreases. Thus, serum creatinine is an insensitive measure of kidney function as it remains in the normal range until GFR falls by 30% to 40%. 16 ,17
99mTc-DTPA is used for GFR evaluation because no tubular secretion or reabsorption is observed, but it is completely filtered by the glomerulus. 18 Also, it is an established procedure for the investigation and diagnostic workup of upper urinary tract dilatation and for the follow-up of patients with urinary outflow obstruction. In routine clinical practice, diuretic renography is the method of choice for differentiating a dilated unobstructed urinary system from a true stenosis and contributes to the management of patients with hydronephrosis by assessing both urinary flow and renal function. 19
The current study showed a high frequency (72.5%) of structural renal abnormalities (in the form of obstructive uropathy and nephropathy) among children with hemophilia A detected by 99mTc-DTPA scan. Similarly, Small et al 4 in a prospective study found high incidence of structural abnormalities by intravenous urograms without impairment in renal functions. In our cohort, patients with obstructive nephropathy had significantly lower 99mTc-DTPA GFR and higher 24-hour protein in urine than patients with obstructive uropathy and those with normal DTPA scan. Despite the high incidence of structural renal tract abnormalities and the evidence of diminished renal function found in some patients, no serious renal functional impairment of clinical significance was found. Patients with obstructive nephropathy were significantly older than patients with obstructive uropathy and patients with normal 99mTc-DTPA scan. Kulkarni et al 2 reported that age was one of the risk factors that was positively associated with renal disease in patients with hemophilia. Regarding disease severity, we found no significant difference between severely and moderately affected patients as regards 99mTc-DTPA scan results as reported previously, 2 indicating that patients with moderate hemophilia should not be neglected and should be thoroughly investigated for abnormalities in the urinary tract. 20,21
99mTc-DMSA scanning provides better assessment for patients with recurrent attacks of pyelonephritis and those who are more prone to cortical scarring. 7 All of our patients had no prior renal infection, that’s why 99mTc-DMSA was negative for cortical scarring. Only 1 patient had an incidental discovery of an atrophic kidney by 99mTc-DMSA and 99mTc-DTPA scans. Renal atrophy is characterized by shrinkage of the kidney due to loss of its nephrons, which are the basic functional unit of the kidney. Several causes may predispose to renal atrophy, including primary renal diseases and acute or chronic pyelonephritis. Renal atrophy may also be caused by obstruction of the urinary tract. Obstructive uropathy causes a higher urinary pressure within the kidneys causing damage to the nephrons. 22
Urinary tract bleeding remains the most common manifestation after hemarthroses in persons with hemophilia, 23 and repeated kidney bleedings may contribute to renal damage in these patients. 24 This study has confirmed that hematuria is fairly common, occurring in 35% of the enrolled patients. The prevalence of hematuria reported from previous studies in Slovenia, Greece, and Argentina were 17.5%, 19.5% and 25%, respectively. 21,23,25 Results of previous studies on renal disease in relation to hematuria in hemophilia varied. 25 While our findings support an association between hematuria and both lower 99mTc-DTPA GFR levels and obstructive nephropathy, it cannot be determined from our study design whether or not renal bleeding led to the renal disease. Forbes and Prentice 26 reported a reduction in kidney function in patients with hematuria. However, data by Benedik-Dolnicar and Benedik 25 did not confirm these findings. Thus, the role of kidney bleeding in renal disease pathogenesis remains to be clarified.
The major focus of concern in patients with hemophilia is to reduce the risk of joint dysfunction, and additional coexisting conditions can develop including hypertension which can adversely affect renal system over time. 27 To the best of our knowledge, there are no studies on the prevalence of hypertension among children with hemophilia. Data from the National High Blood Pressure Education Program (NHBPEP) Working Group on Children and Adolescents reported that prevalence of hypertension in children is approximately 1% to 3%. 9 However, few studies have been conducted in children in developing countries. A study on blood pressure among preparatory schoolchildren in Alexandria found the prevalence of hypertension to be 4.3%. 28
In our cohort, hypertension seemed to occur in a frequency higher than that in the general population occurring in 12.5% of the patients. We found a significant association between hypertension and higher age and BMI. Of interest there was an apparent association between hypertension and both hematuria and HCV infection. Moreover, we found that patients with hypertension showed lower mean values of 99mTc-DTPA GFR compared to nonhypertensive group. However, these associations are not convenient because of the small number of patients with hypertension in this report. Further studies of these associations in larger cohorts of children with hemophilia are warranted. Kulkarni et al 2 reported the prevalence of hypertension in patients with hemophilia admitted for hematuria to be 10.1% compared to 4.5% among those admitted for other causes.
Reasons of increased prevalence of hypertension in patients with hemophilia are currently not well documented. Possible explanations could be reduced renal functions in patients with hemophilia either due to renal microbleeding or glomerulopathies caused by HCV or HIV infection. Another possible explanation is that patients with hemophilia may have increased BMI due to reduced physical activity than normal males either due to arthopathy or fear of bleeding. 29
Infusion of plasma-derived concentrates exposes patients with hemophilia to HIV and HCV resulting in additional chronic illness. Coinfection with HIV and HCV can increase the risk of renal problems in patients with hemophilia. 27 None of our patients had HIV, however 20% had HCV infection. Both glomerular and tubulointerstitial diseases associated with HCV have been described previously. 30 Mild proteinuria was detected in 72.5% of our patients, and no patient showed nephrotic range proteinuria. In contrast, lesser percentage (13.7%) of mild proteinuria was previously reported by Benedik-Dolnicar and Benedik 25 among their cohort with hemophilia. Half of them had HIV infection and were on antiretroviral therapy. In our study, there was no significant difference in mean 99mTc-DTPA GFR and 24-hour urinary protein among patients as regards HCV infection. Our results failed to reach statistical significance probably as our patients were very young to develop any renal disease.
Conclusion
Despite absence of clinically significant renal disease and normal kidney functions (serum creatinine and BUN), we found a high rate of diminished GFR as well as obstructive uropathy and nephropathy as detected by 99mTc-DTPA scan among children with hemophilia A. We found a significant association between diminished GFR and hematuria, hypertension, and obstructive nephropathy. Moreover, our study highlighted the problem of hypertension in children with hemophilia A. Further studies are required to identify the etiology and risk factors associated with hypertension in this population.
Recommendations
We recommend screening of patients with moderate and severe hemophilia A for microscopic hematuria as well as for presence of renal compromise and structural renal abnormalities by 99mTc-DTPA scan. Routine blood pressure measurement should be part of the general examination of children with hemophilia during the follow-up visits. Prospective studies are required to determine whether these renal abnormalities among this population are transient or will progress to a problematic renal dysfunction.
Footnotes
Authors’ Note
Ahmad A Hamed and Shereen M Abd El-Ghany designed the research study and analyzed the data. Shereen M Abd El-Ghany wrote the paper. Nihal S El-Kinawy performed the laboratory investigations of the study and revised the paper. Mennatallah H Shalaby interpreted the nuclear medicine procedures (DTPA diuretic demography and DMSA cortical scintigraphy) with assessment of the renal function of the patients and revised the paper. Alaa A Elamawey collected data of the research and performed the research. All of the authors have read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.