
Abstract
Background:
Sheikh Khalifa Medical City’s (SKMC) surgery institute was identified as a high outlier in the incidence of venous thromboembolism (VTE; deep vein thrombosis [DVT] and pulmonary embolism [PE]) based on the semiannual report of the American College of Surgeon’s National Surgical Quality Improvement Program (ACS NSQIP) in June 2010.
Aim:
To report our rates of VTE at SKMC, the results, and 5-year follow-up after an ACS NSQIP quality improvement program.
Methods:
A multidisciplinary VTE task force was established in June 2010. We instituted a compulsory risk assessment for VTE and utilized the ACS NSQIP best practice guidelines to review cases of VTE. We prospectively evaluated the observed/expected (O/E) ratio for DVT/PE after implementing the action plan.
Results:
The O/E ratio for PE/DVT in general and general/vascular (GV) surgery was 6.00 and 4.86 in June 2010. Our compliance with ordering antithrombotic prophylactic measures was as low and it improved to 100% and our O/E ratio decreased to 1.18 and 1.5 in July 2011 and stabilized for the next 4 years. Currently, our compliance with ordering antithrombotic prophylactic measures is 100%, and our last 2 O/E ratio for DVT/PE are 0.74 and 0.75 in GV surgery and 0.82 and 0.78 in the entire surgery institute, respectively, and we are considered an exemplary site of the ACS NSQIP in GV surgery.
Conclusion:
A compulsory risk assessment for VTE has led to an overall improvement in DVT/PE rates in the surgery institute and for GV surgery to become an exemplary site for the ACS NSQIP.
Introduction
The prevention of venous thromboembolism (VTE) in the hospital is a priority, since pulmonary embolism is the most common preventable cause of death in hospital admissions. 1,2 The cost of VTE (deep venous thrombosis [DVT] and pulmonary embolism [PE]) is enormous. Most hospitalized patients will have at least one or more risk factors for developing VTE, and programs to protect these patients are vital in order to decrease the morbidity associated with the disease. Despite educational efforts, physician’s use of VTE prophylaxis remains low in many hospitals. 3
Sheikh Khalifa Medical City (SKMC) was identified as a high outlier for VTE based on the semiannual report (SAR) of the ACS NSQIP in June 2010. 4 In an internal audit, we found that our compliance with instituting prophylaxis against DVT/PE was low. We aimed to measure the impact of a quality improvement project (QIP) in the reduction of VTE rates among surgical patients in SKMC.
Methods
The SKMC is a tertiary referral center with 790 beds and a Joint Commission International (JCI)-accredited hospital. Our surgery institute has been an ACS NSQIP multispecialty participating site since August 2009, and we submit all our cases to the ACS NSQIP, except transplant, cardiac, and pediatric surgery cases. Our study is a prospective evaluation of a QIP utilizing the risk-adjusted SARs of the ACS NSQIP at SKMC. The statistical analysis of these risk adjusted reports is done by ACS NSQIP comparing SKMC to more than 450 other ACS NSQIP hospitals. The sampling of patients enrolled to the ACS NSQIP at SKMC is done randomly by an independent surgical clinical reviewer by a standardized sampling method similar to all other ACS NSQIP hospitals.
Our semiannual report (SAR) in 2010 identified the division of general/vascular (GV) surgery and the entire surgery institute as high outliers (worse 90th percentile compared to other ACS NSQIP hospitals) for VTE. A hospital-wide multidisciplinary VTE task force was established in June 2010. The task force included members from surgery, nursing, quality, medicine, pharmacy, IT, the ACS NSQIP surgeon champion, and surgical clinical reviewer and was chaired by an experienced hematologist. Our initial high rates of VTE represented in our high O/E ratios placed our institute as a high outlier for DVT/PE compared to other hospitals participating in the ACS NSQIP.
Intervention
An initial chart review of cases of VTE picked up by the ACS NSQIP showed that we were not always prescribing antithrombotic prophylactic measures appropriately. In addition, we realized that we had poor adherence to risk assessment for VTE in many of our surgery patients admitted to SKMC. The recommendations of the task force were rolled out at the end of 2010 and included reviewing and updating the hospital’s VTE prophylaxis policy, physician and nursing staff education about the importance of performing VTE risk assessment, implementing a compulsory risk assessment to all patients undergoing surgery or being admitted to the surgery institute, and a continuous internal audit to evaluate the compliance with implementation of accepted prophylactic measures for VTE was done. This compulsory risk assessment form was attached to each patient’s file whether the patient was admitted through the emergency department or scheduled for elective surgery. Once the initial implementation phase of the VTE risk assessment form was done, the form was converted to an electronic form which was embedded in the electronic medical record (Figure 1). Furthermore, education about the importance of assessing patients for the risk of VTE both on admission and at discharge was done for the nursing and house staff.
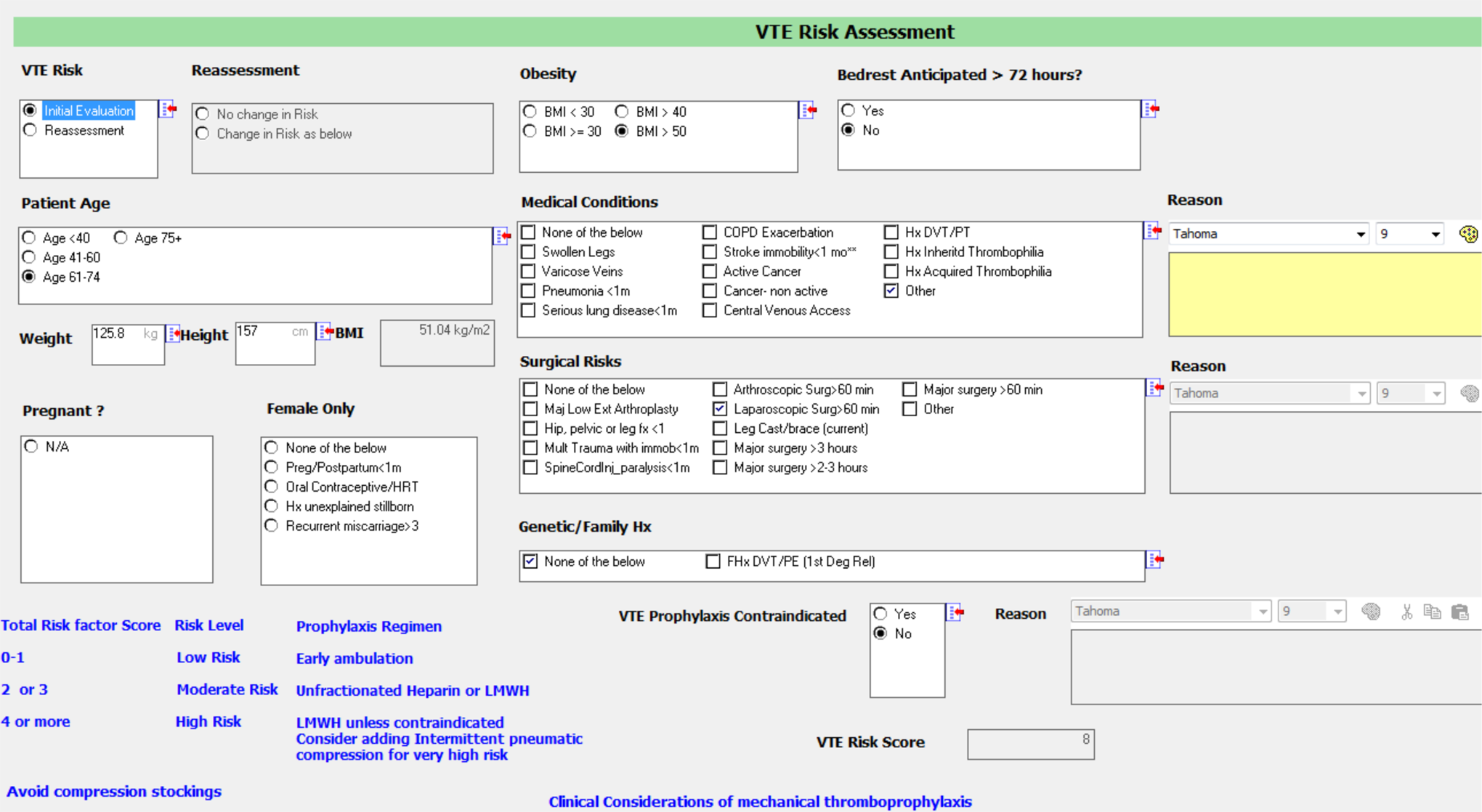
Electronic medical record venous thromboembolism risk assessment form.
To improve the compliance with performing VTE risk assessment, a hard stop was instituted from the start of the implementation of the risk assessment if the VTE risk assessment form was not completed. Other efforts to improve compliance included reminders to fill the risk assessment form in our electronic medical record to alert physicians and improve our compliance with instituting antithrombotic prophylactic measures. The physicians would be prompted when opening the patient’s electronic medical record to complete the VTE risk assessment form.
To help physicians in prescribing VTE prophylaxis, once the paper-based or electronic form was completed, a score was calculated stratifying the patient’s VTE risk into low (0-1), moderate (2-3), and high (4 or more) for VTE. This stratification was linked to suggested prophylaxis for VTE based on the previously reported incidence of VTE according to the level of risk. Balancing the use of suggested pharmacologic prophylaxis for each group was the physician’s evaluation of the patients potential risk of bleeding. The risk assessment score is based on the Caprini et al VTE risk assessment scoring system. 5 Patients with score of 2 to 4 received antithrombotic prophylaxis while admitted to the hospital if there was no contraindication to anticoagulation, while patients with score 5 or above received chemoprophylaxis for 2 weeks postdischarge. We use low-molecular-weight heparin 40 mg once a day for patients with BMI less than 40 kg/m2 and 40 mg twice daily for patients with BMI >40 kg/m2. In addition, we send anyone with a Caprini score of 5 or more on 2 to 3 weeks of antithrombotic prophylaxis.
To evaluate and monitor our progress, we elected to use the adherence to the use of the compulsory VTE risk assessment form on a monthly basis and the observed/expected (O/E) ratio for VTE every 6 months. Our results were compared to the ACS NSQIPs utilizing the semiannual risk-adjusted reports.
Statistics
The data collected randomly by our independent surgical clinical reviewer were submitted to the ACS NSQIP. The statistical analysis and risk adjustment that compares our VTE rates to other US ACS NSQIPs are done by the statistical team at the ACS NSQIP headquarters in the United States.
Results
During the study period, we enrolled 2280 patients from 2010 to 2014, and our cases enrolled in 2010 were lower than 100 because we enrolled in the ACS NSQIP in August 2009 (4 months of data collection). Our adherence to filling the VTE risk assessment improved from below 80% to 100%, and at the same time, our rates of VTE decreased from a high rate of 3.1% (3 of 98) in 2010 to 0.9% (6 of 637) in 2011 and stabilized at a low exemplary rate of 0.1% (1 of 735) and 0.2% (2 of 810) in 2013 and 2014, respectively. Similarly, the O/E ratio for VTE in general surgery and GV surgery decreased from a high outlier status of 6.00 confidence interval [CI] (1.24-17.5) and 4.86 CI (1.0-14.19) in 2010 to an exemplary O/E ratio of 0.74 CI (0.43-1.32) and 0.75 CI (0.42-1.32), respectively, in 2013 and 2014 (Figure 2 and Table 1
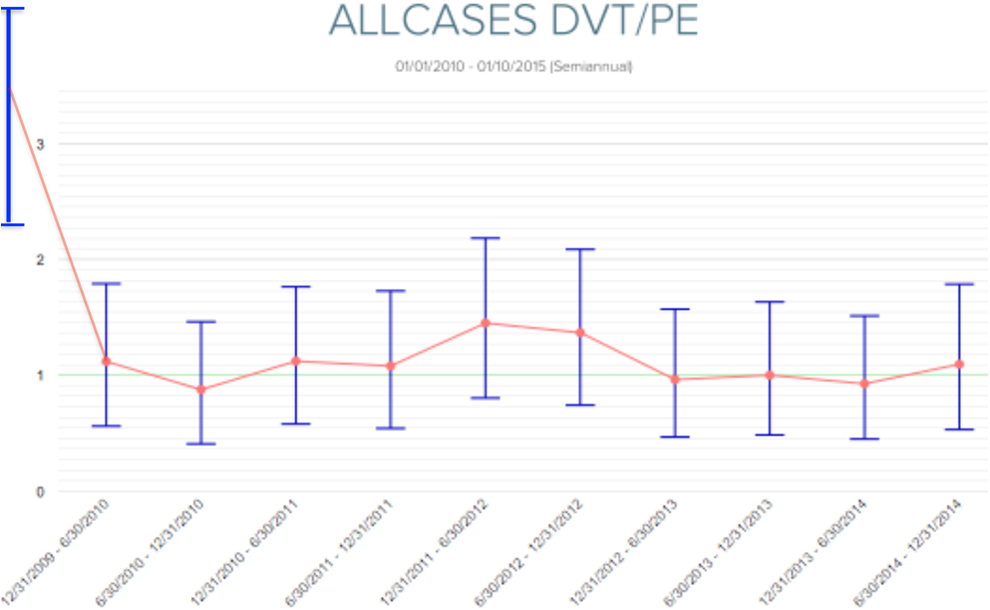
Real-time risk and shrinkage-adjusted projected odds ratio report.
VTE Odds Ratio at SKMC.
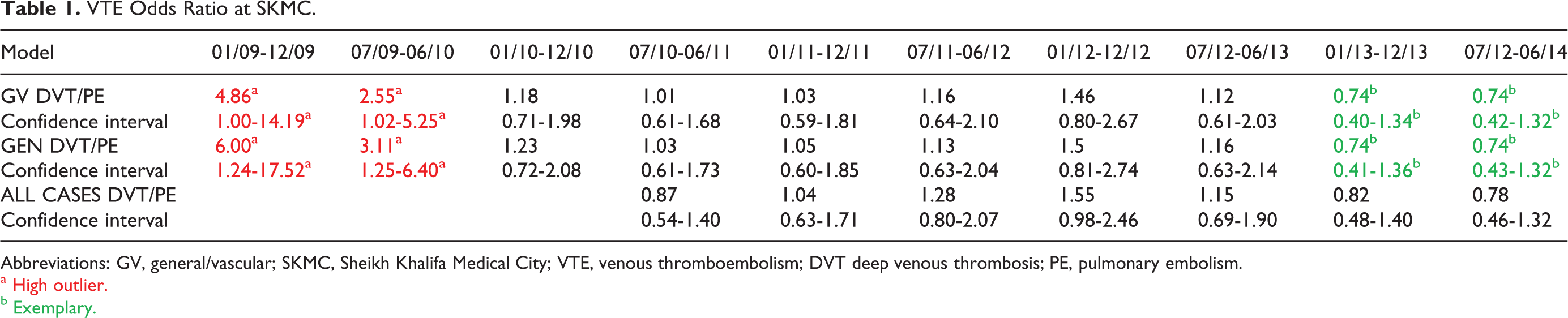
Abbreviations: GV, general/vascular; SKMC, Sheikh Khalifa Medical City; VTE, venous thromboembolism; DVT deep venous thrombosis; PE, pulmonary embolism.
a High outlier.
b Exemplary.
After implementation of the DVT/PE task force recommendations, the adherence to performing the VTE risk assessment improved to 100%. However, our adherence to prescribing antithrombotic prophylactic measures was still below 80% (Table 2).
Compliance Rates for Performing VTE Prophylaxis at SKMC.
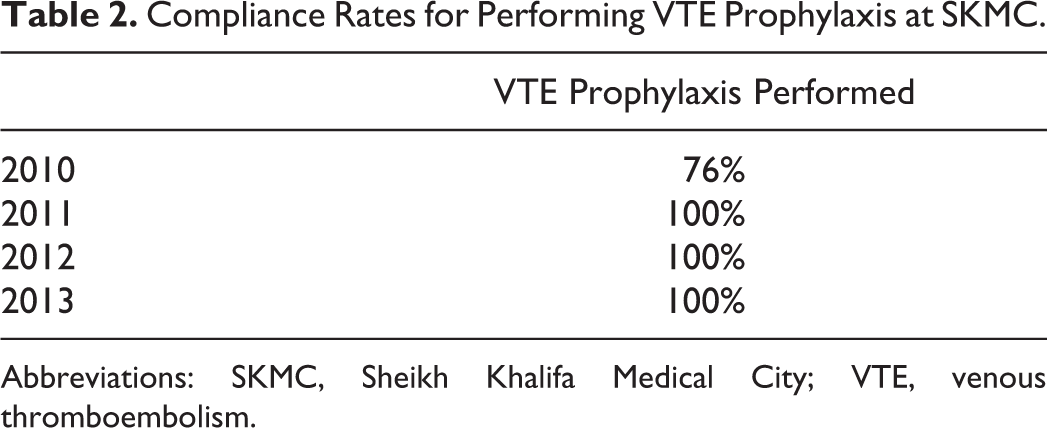
Abbreviations: SKMC, Sheikh Khalifa Medical City; VTE, venous thromboembolism.
In our last SAR, the O/E ratio for DVT/PE was 0.75 in general and GV surgery, and we are considered an exemplary site of the ACS NSQIP in general, GV surgery, and orthopedic surgery (Table 1).
Discussion
Our QIP proved that installing the Caprini model as a compulsory stratification method and VTE prevention strategies were effective in reducing VTE in general and vascular surgery patients. Several patient-related factors contributed to the incidence of VTE. In addition, major surgery is one of the well-recognized risk factors for VTE. 6 Despite the presence of recognized evidence-based guidelines by organizations such as the American College of Chest Physicians, 7 compliance worldwide continues to be suboptimal.
The Institute of Medicine has classified the failure to provide appropriate screening and preventive treatment to hospitalized, at-risk patients as a medical error, and the Agency for Healthcare Research and Quality has ranked the provision of such preventive treatment as one of the most important things that can be done to improve patient safety. 8
Our initial poor adherence to performing risk assessment for VTE is not a unique problem to SKMC. In 2008, results from the multinational ENDORSE (Epidemiologic International Day for the Evaluation of Patients at Risk for Venous Thromboembolism in the Acute Hospital Care Setting) trial showed that only two-thirds of at-risk surgical patients and fewer than half of at-risk medical patients received any form of antithrombotic prophylaxis. 9 In our institute, our initial adherence rate was less than 80% in surgery patients. The initial lack of adherence could have been attributed to the lack of awareness of VTE risk and its implications on both patients and health care systems or unreasonable fear of intra- or postoperative bleeding in surgical patients.
The concept of risk assessment is not new. Caprini et al developed a risk assessment tool in 1988 following several similar reports of noncompliance at the time. 5 Stratification was classified into low, moderate, and high risk, which is similar to the risk stratification we are using. Our risk stratification model follows the Caprini score model (Figure 1). We believe that the score generated at the end of the form gives the health care provider immediate feedback on the overall VTE risk of the patient. This score enhances the awareness for VTE further and helps in deciding on which patients need antithrombotic prophylaxis after discharge.
The goal of our QIP for prevention was to eliminate all episodes of preventable VTE events by improving compliance with antithrombotic prophylaxis guidelines. Our efforts in forming a task force to address our adherence problem and the recommendations of our VTE task force are similar to several reports in the literature. 10,11 For example, Vyas et al reported an audit on general internal medicine patients after implementing a VTE order set on all admissions. Similar to our improvement in adherence with VTE risk assessment form, Vyas et al showed that adherence increased from 75% to 91% at 2 months postintervention and to 95% at 1 year. 10 Likewise, Novis et al instituted a standardized computerized DVT risk assessment program. Pharmacological antithrombotic prophylaxis increased from 14% to 36%, and use of sequential devices doubled to 40%.
Adherence to performing VTE risk assessment was excellent in our study. We believe the hard stops we instituted as well as the education of nursing and house staff and the increased awareness to the problem of VTE helped in improving our adherence more than that seen by others. Our adherence rate with performing VTE risk assessment has reached 100%, but not all these patients actually received antithrombotic prophylaxis because the physician did the risk assessment but did not follow through in ordering antithrombotic prophylaxis. In an internal audit, we discovered that the adherence with performing the risk assessment has greatly improved, and it is done 100% of the time. However, when it comes to ordering VTE prophylactic measures, our compliance is still less than 80%.
Another reason for our excellent adherence to performing VTE risk assessment is embedding the VTE risk assessment form in the electronic medical record (EMR). Utilizing the EMR to improve adherence with VTE risk assessment is well described in the literature as well. Kucher et al demonstrated that the implementation of an electronic alert system increased prophylaxis and reduced the incidence of DVT or PE by 41% at 90 days. 12 A Cochrane database systematic review consolidated similar results for various methods of intervention, including electronic alerts and other interventions. The review concluded that interventions with an alert system were most effective. 13,18 Similarly, Bahl et al and Cassidy et al have shown that VTE risk assessment correlates with probability of VTE and that mandatory prophylaxis and physical ambulation in surgery patients can lower the risk of VTE postoperatively. 14,15
Improving physicians’ behaviors in the actual prescription of antithrombotic prophylaxis whether chemical or mechanical was of equal importance as completion of the compulsory assessment forms. Passive dissemination of guidelines as a QIP does not ensure actual compliance with prescription rates. 14 Our prescription rates before the compulsory form in SKMC was 76% in 2010 that improved to a 100% in 2013, after instituting the compulsory form. We have observed that appropriate education for physicians and other healthcare professionals also played an integral role in improving both compliance in assessment and prescription. Similarly, Cohn et al demonstrated an improvement in appropriate VTE prophylaxis from 43% to 86% at 12 months after instituting an educational program consisting of regular education and repeated audits and assessments. 15,19
Conclusion
A compulsory risk assessment for VTE has led to an overall improvement in VTE rates in the entire surgery institute, and our general and vascular rates of VTE have become among the best compared to other ACS NSQIP hospitals. The ACS NSQIP and the hospitals participating in the ACS NSQIP are the source of the data used herein. They are not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Footnotes
Author’s Note
This article was presented as an oral presentation at the ACS NSQIP National Conference in San Diego, California, on July 2013.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.