
Abstract
We aimed to examine the cross-sectional associations of plasma total homocysteine (tHcy) concentrations and methylenetetrahydrofolate reductase (MTHFR) C677T genotype with dyslipidemia. A total of 231 patients with mild-to-moderate essential hypertension were enrolled from the Huoqiu and Yuexi communities in Anhui Province, China. Plasma tHcy levels were measured by high-performance liquid chromatography. Genotyping was performed by TaqMan allelic discrimination technique. Compared with MTHFR 677 CC + CT genotype carriers, TT genotype carriers had higher odds of hypercholesterolemia (adjusted odds ratio [OR] [95% confidence interval (CI)]: 2.7 [1.4-5.2]; P = .004) and higher odds of abnormal low-density lipoprotein cholesterol (adjusted OR [95% CI]: 2.3 [1.1-4.8]; P = .030). The individuals with the TT genotype had higher concentrations of log(tHcy) than those with the 677 CC + CT genotype (adjusted β [standard error]: .2 [0.03]; P < .001). Patients with tHcy ≥ 10 μmol/L had significantly higher odds of hypercholesterolemia (adjusted OR [95% CI]: 2.4 [1.2-4.7]; P = .010). Furthermore, patients with both the TT genotype and the tHcy ≥ 10 μmol/L had the highest odds of hypercholesterolemia (adjusted OR [95% CI]: 4.1 [1.8-9.4]; P = .001) and low-density lipoprotein cholesterol (adjusted OR [95% CI]: 2.4 [1.0-6.0]; P = .064). This study suggests that both tHcy and the MTHFR C677T gene polymorphism may be important determinants of the incidence of dyslipidemia in Chinese patients with essential hypertension. Further studies are needed to confirm the role of tHcy and the MTHFR C677T mutation in the development of dyslipidemia in a larger sample.
Introduction
Cardiovascular disease (CVD) is one of the leading threats to human health worldwide. In China, 3.5 million people die of this disease each year. Hypertension, diabetes, dyslipidemia, obesity, and smoking are regarded as the traditional risk factors for CVD and are limited for explaining the risk of CVD. More and more evidence has emerged that even moderate hyperhomocysteinemia (HHcy) may be a new independent and important risk factor for CVD. 1 –3 However, the relationship between dyslipidemia and HHcy has been studied very little. An increase in 5 mmol/L homocysteine (Hcy) may increase the risk of CVD by the same factor as an increase in cholesterol level of 0.5 mmol/L. 4 Thus, understanding the underlying mechanisms of HHcy, dyslipidemia, and their joint effects on CVD may be helpful to reduce the incidence of the disease and provide an efficient strategy for prevention.
Homocysteine, a sulfur-containing amino acid, is formed in the demethylation of the essential amino acid methionine. In recent years, various studies confirmed that serum Hcy is positively correlated with total cholesterol (TC). 5 –8 O K et al have reported that Hcy stimulates the production and secretion of cholesterol and apolipoprotein B100 in HepG2 cells. 5 Woo et al have found that there was a marked hepatic lipid accumulation and an elevation in plasma cholesterol concentration in hyperhomocysteinemic rats. 7 Werstuck et al have shown a significant increase in the levels of cholesterol and triglycerides in the liver, although not in plasma, of hyperhomocysteinemic mice. 8 Some further data have shown that diet-induced HHcy can result in elevated TC and triacylglycerol (TG) in mouse livers, although, in contrast, total homocysteine (tHcy) decreases high-density lipoprotein cholesterol (HDL-C). 8,9 Wang et al have found that plasma TC level in apoE−/−/CBS−/− mice was significantly increased, whereas HDL-C cholesterol and TG concentrations were decreased. 10 Namekata et al also found that serum cholesterol or triglyceride distribution in lipoprotein fractions was altered in CBS−/− mice. 11 The numerous findings mentioned previously indicated that HHcy is likely to have a close link with lipid metabolism; however, the exact role of Hcy in lipid metabolism is unclear.
Methylenetetrahydrofolate reductase (MTHFR) is a key enzyme in the tHcy metabolic pathway that converts 5,10-methylenetetrahydrofolate to 5-methyltetrahydrofolate, thus generating the active form of folate required for methylation of tHcy into methionine. The MTHFR C677T is a common missense mutation that can lead to the substitution of alanine for valine in position 222, thus creating a thermolabile enzyme with 50% reduced activity at 37°C. Our previous study by Jiang et al has found that the MTHFR C677T gene polymorphism could be an important genetic determinant of serum lipid levels in Chinese patients with hypertension. 12
In the present study, we aimed to further investigate the relationship between the occurrence of dyslipidemia and tHcy and the MTHFR C677T gene polymorphism in Chinese patients with hypertension.
Materials and Methods
Study Population
In total, 231 patients with mild to moderate hypertension from the Huoqiu and Yuexi communities in Anhui Province, China, were recruited. The mean age of the participants was 47.63 ± 7.26 years. There were 104 (45%) men and 127 (55%) women in our study. In summary, participants with hypertension who met the following criteria were enrolled: (1) diastolic blood pressure (DBP) between 90 and 120 mm Hg or systolic blood pressure (SBP) between 140 and 200 mmHg, (2) age 35 to 65 years, and (3) no consumption of any lipid-lowering drugs within 4 weeks of the start of the study. In order to eliminate the influence of certain factors, participants who had a history of any of the following conditions were excluded: secondary hypertension, pregnancy, hypercalcemia, chronic CVD, chronic cerebrovascular disease, chronic liver or renal diseases, or body mass index (BMI) > 33 kg/m2. This study was approved by the Ethics Committee of Anhui Medical University, Hefei, China. The purpose and procedures of the study were carefully explained to all participants, and a written informed consent was obtained.
Laboratory Determinations
After overnight fasting, blood was collected for biochemical examination. The samples were then centrifuged at 3000 rpm for 10 minutes to obtain the serum. At our analytical center, automated biochemical analysis was used for the laboratory determinations. Levels of TC, HDL-C, low-density lipoprotein cholesterol (LDL-C), and TGs were determined with enzymatic colorimetric assays from Roche Diagnostics (Indianapolis, Indiana). The intra-assay and interassay coefficients of variation were <5% for all assays performed. Total plasma Hcy concentration was measured in plasma by high-performance liquid chromatography coupled with fluorescence detection. The intra-assay and interassay coefficients of variation were 3.5% and 4.2%, respectively.
Genotyping of MTHFR C677T
TaqMan allelic discrimination technique was used for detecting the MTHFR C677T (Ala222Val) genotypes in our central laboratory. The 198-base pair fragment of the MTHFR C677T gene locus was amplified by a polymerase chain reaction (PCR) with the following pairs of primers: 5′-GCA CTT GAA GGA GAA GGT GTC T-3′ and 5′-TGT GTC AGC CTC AAA GAA AAG CT-3′. The universal reaction conditions for genotyping were as follows: 4 ng dried DNA, 0.08 μL 40× assay locus-specific probe, and 2.0 μL TaqMan (Applied Biosystems, Foster City, CA, USA) universal PCR master mix made to a final volume of 4 μL with 1.92 μL sterile water. The PCR cycle conditions consisted of an initial denaturation at 95°C for 10 minutes followed by 50 cycles at 92°C for 15 seconds and 60°C for 1 minute. All sample sets genotyped for the single-nucleotide polymorphism in our present study had overall call rates of ≥95% after excluding samples that consistently failed. We selected 10% of the total samples for replication, and concordance of 100% was repeated for all samples for quality control.
Statistical Analysis
The Epidata 3.1 software package (The EpiData Association, Odense, Denmark), Chinese version, was used for database design, data entry, and data check. Abnormal TC was defined as TC > 5.18 mmol/L, abnormal TG was defined as TG > 1.76 mmol/L, abnormal LDL-C was defined as LDL-C > 3.37 mmol/L, and abnormal HDL-C was defined as HDL-C < 1.04 mmol/L. 13 Hyperhomocysteinemia was defined as Hcy level > 10 μmol/L. 14 Continuous variables are presented as mean values ± standard deviation, while categorical variables are presented as percentages. The means for continuous variables among the 3 groups were compared using analysis of variance tests, and the significance of categorical variables was compared using χ2 tests. Logistic regression was used to analyze the association of the MTHFR C677T gene polymorphism with hyperlipidemia risks, including abnormal TG, HDL-C, LDL-C, and TC levels, and HHcy odds. Multiple linear regression analysis was used to estimate the associations of the MTHFR C677T polymorphisms with plasma Hcy levels. A logistic regression model was also used to analyze gene–HHcy joint associations on hyperlipidemia risk. All analyses were adjusted for age, sex, height, weight, and community. A 2-sided P value <.05 was considered to be significant. All statistical analyses were conducted using the IBM SPSS software package (version 19.0 for windows; IBM Inc, Armonk, New York).
Results
General Characteristics of the Study Population
In total, 231 patients with mild to moderate hypertension were recruited from the Huoqiu and Yuexi communities in Anhui, China. The characteristics of all patients among the 3 genotypes are shown in Table 1. We found that tHcy and age distributions across the 3 groups were significantly different (P < .05), while no significant differences in TG, TC, LDL-C, HDL-C, DBP, SBP, BMI, and the MTHFR C677T genotypes were observed across the 3 groups.
Clinical and Epidemiologic Characteristics of Population Grouped by MTHFR Genotypes.
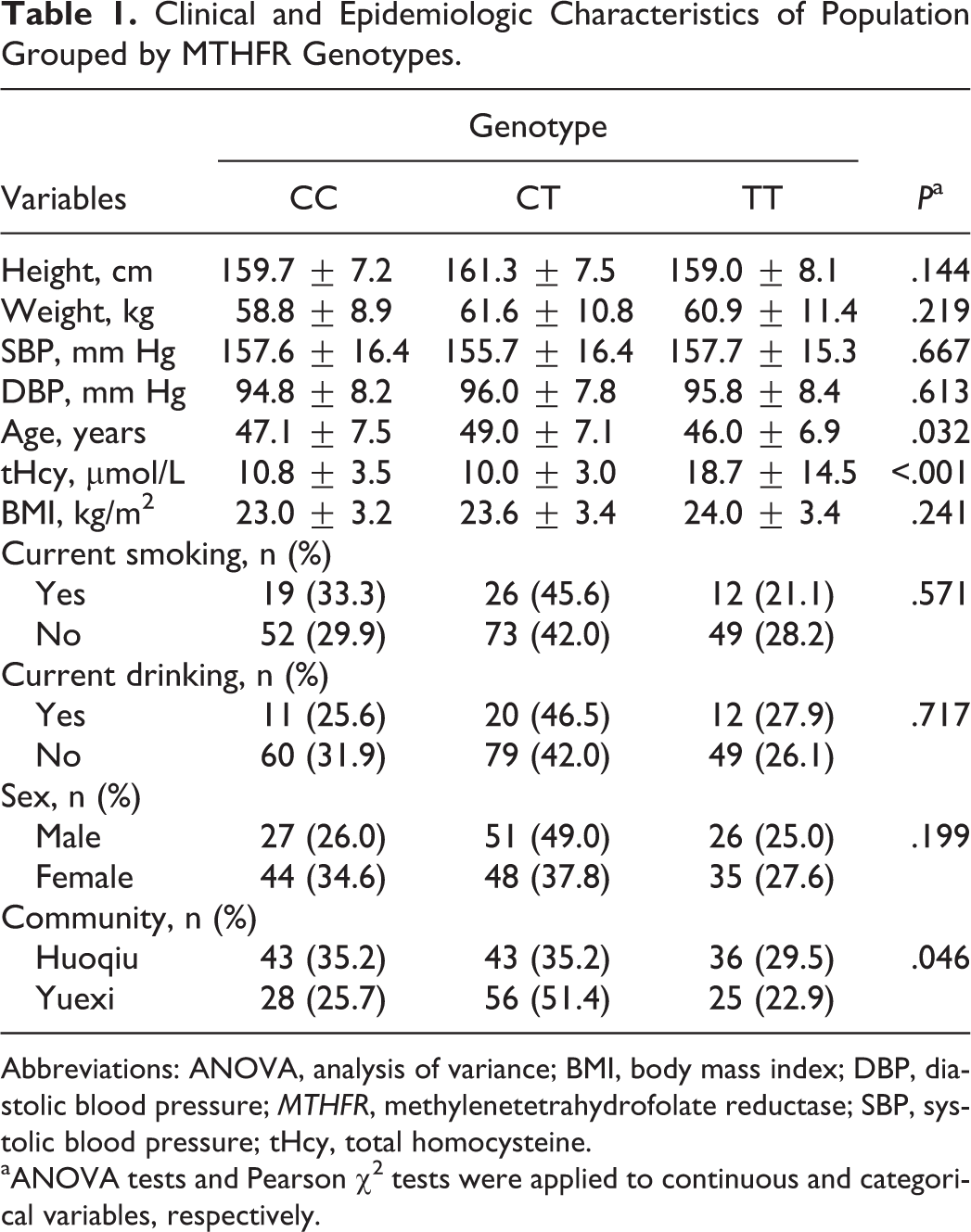
Abbreviations: ANOVA, analysis of variance; BMI, body mass index; DBP, diastolic blood pressure; MTHFR, methylenetetrahydrofolate reductase; SBP, systolic blood pressure; tHcy, total homocysteine.
aANOVA tests and Pearson χ2 tests were applied to continuous and categorical variables, respectively.
Comparison of Dyslipidemia Odds by Genotypes of MTHFR C677T
As shown in Table 2, the odds of abnormal TC and LDL-C were significantly different across the 3 genotypes of the MTHFR C677T polymorphism. Logistic regression analysis showed that compared with CC + CT genotype carriers, the TT carriers had a higher odds of abnormal TC (odds ratio, OR, [95% confidence interval (CI)]: 2.8 [1.5-5.2], P = .001) and a higher abnormal LDL-C risk (OR [95% CI]: 2.6 [1.3-5.1], P = .007). However, after adjustment for confounding factors, the P values became slightly larger, although still statistically significant, increasing to .004 and .030 for TC and LDL-C, respectively. There was no significant difference in the odds of abnormal TG and HDL-C across the 3 genotypes of MTHFR C677T.
Logistic Regression Was Used to Analyze the Association Between Abnormal TG, HDL, LDL, TC risks, and MTHFR C677T Polymorphism.
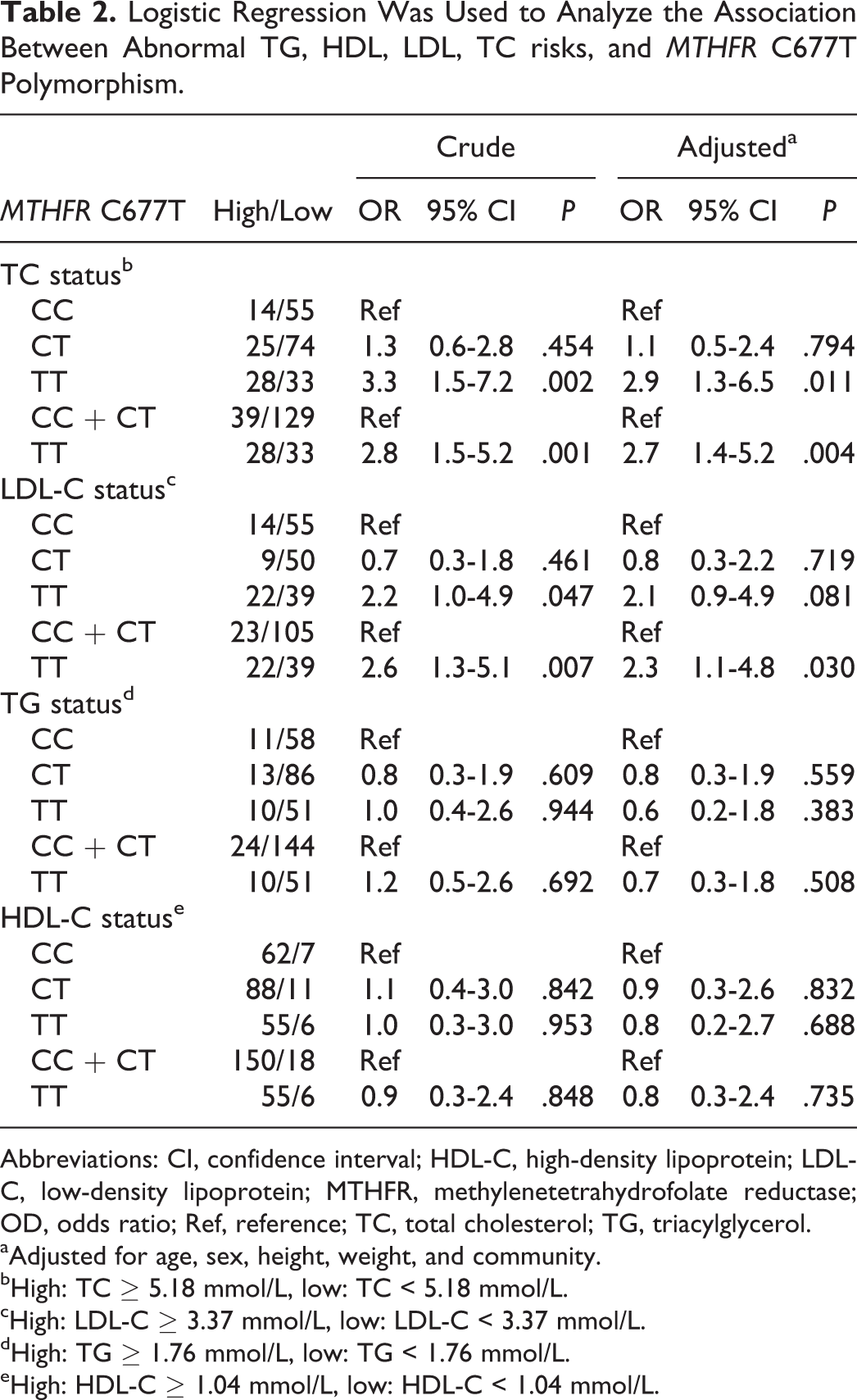
Abbreviations: CI, confidence interval; HDL-C, high-density lipoprotein; LDL-C, low-density lipoprotein; MTHFR, methylenetetrahydrofolate reductase; OD, odds ratio; Ref, reference; TC, total cholesterol; TG, triacylglycerol.
aAdjusted for age, sex, height, weight, and community.
bHigh: TC ≥ 5.18 mmol/L, low: TC < 5.18 mmol/L.
cHigh: LDL-C ≥ 3.37 mmol/L, low: LDL-C < 3.37 mmol/L.
dHigh: TG ≥ 1.76 mmol/L, low: TG < 1.76 mmol/L.
eHigh: HDL-C ≥ 1.04 mmol/L, low: HDL-C < 1.04 mmol/L.
Comparison in Association of tHcy With MTHFR C677T Polymorphism
Table 3 shows the tHcy distribution by MTHFR C677T locus in the patients. Multiple linear regression analysis estimated that compared with the CC and CT genotype carriers, the TT genotype carriers had a higher tHcy concentration (adjusted β [standard error]: .22 μmol/L [0.03 μmol/L]; P < .001). A comparison of HHcy prevalence across the different genotypes was also performed (results shown in Table 4), and a significant difference in HHcy odds was observed across the 3 genotypes. The odds of HHcy in the TT carriers were significantly higher than those in the CC + CT carriers (adjusted OR = 7.1, 95% CI: 3.2-15.7, P < .001).
Multiple Linear Regression Analysis Was used to Estimate the Association Between MTHFR C677T Polymorphism and tHcy Levels.
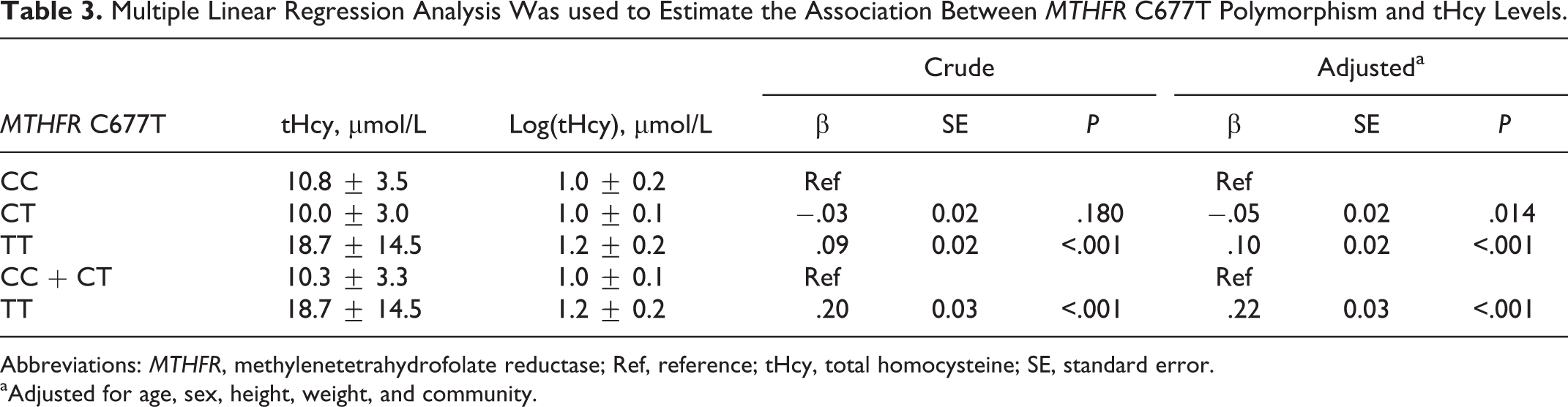
Abbreviations: MTHFR, methylenetetrahydrofolate reductase; Ref, reference; tHcy, total homocysteine; SE, standard error.
aAdjusted for age, sex, height, weight, and community.
Logistic Regression Was Used to Analyze the Association of MTHFR C677T and HHcy.
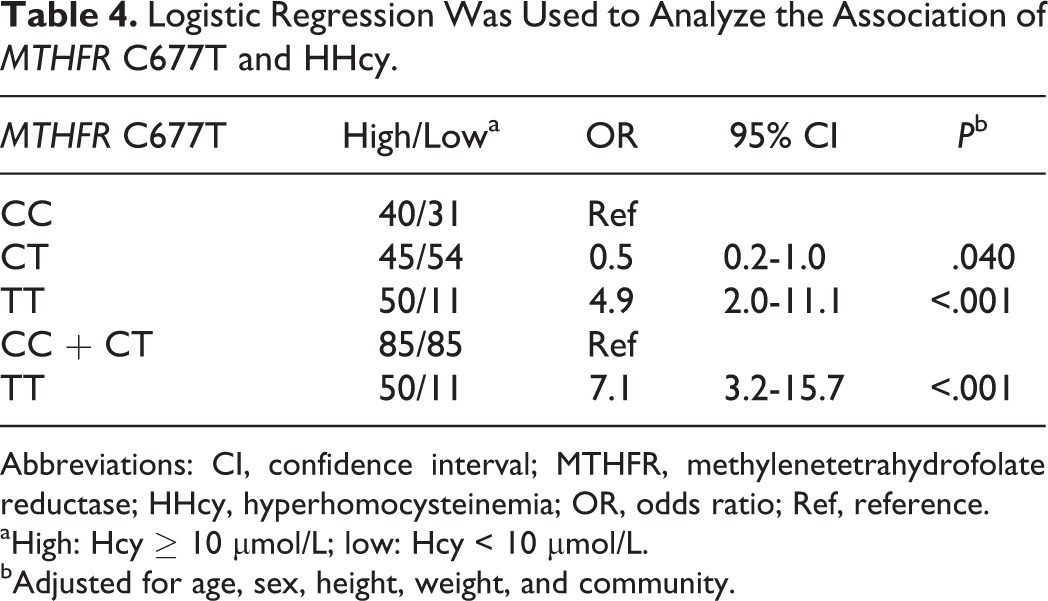
Abbreviations: CI, confidence interval; MTHFR, methylenetetrahydrofolate reductase; HHcy, hyperhomocysteinemia; OR, odds ratio; Ref, reference.
aHigh: Hcy ≥ 10 μmol/L; low: Hcy < 10 μmol/L.
bAdjusted for age, sex, height, weight, and community.
Comparison of Dyslipidemia Odds by HHcy
As shown in Table 5, in order to analyze the association between HHcy and dyslipidemia profiles in the patients, all patients were divided into 2 subgroups by baseline Hcy levels with a cutoff point of 10 μmol/L. Compared to the patients with baseline Hcy < 10 μmol/L, the patients with baseline Hcy ≥ 10 μmol/L had a higher risk of hypercholesterolemia (adjusted OR [95% CI]: 2.4 [1.2-4.7]; P = .010). However, no other dyslipidemia odds were observed to be associated with HHcy.
Logistic Regression Was used to Analyze the Associations of HHcy With Dyslipidemia.
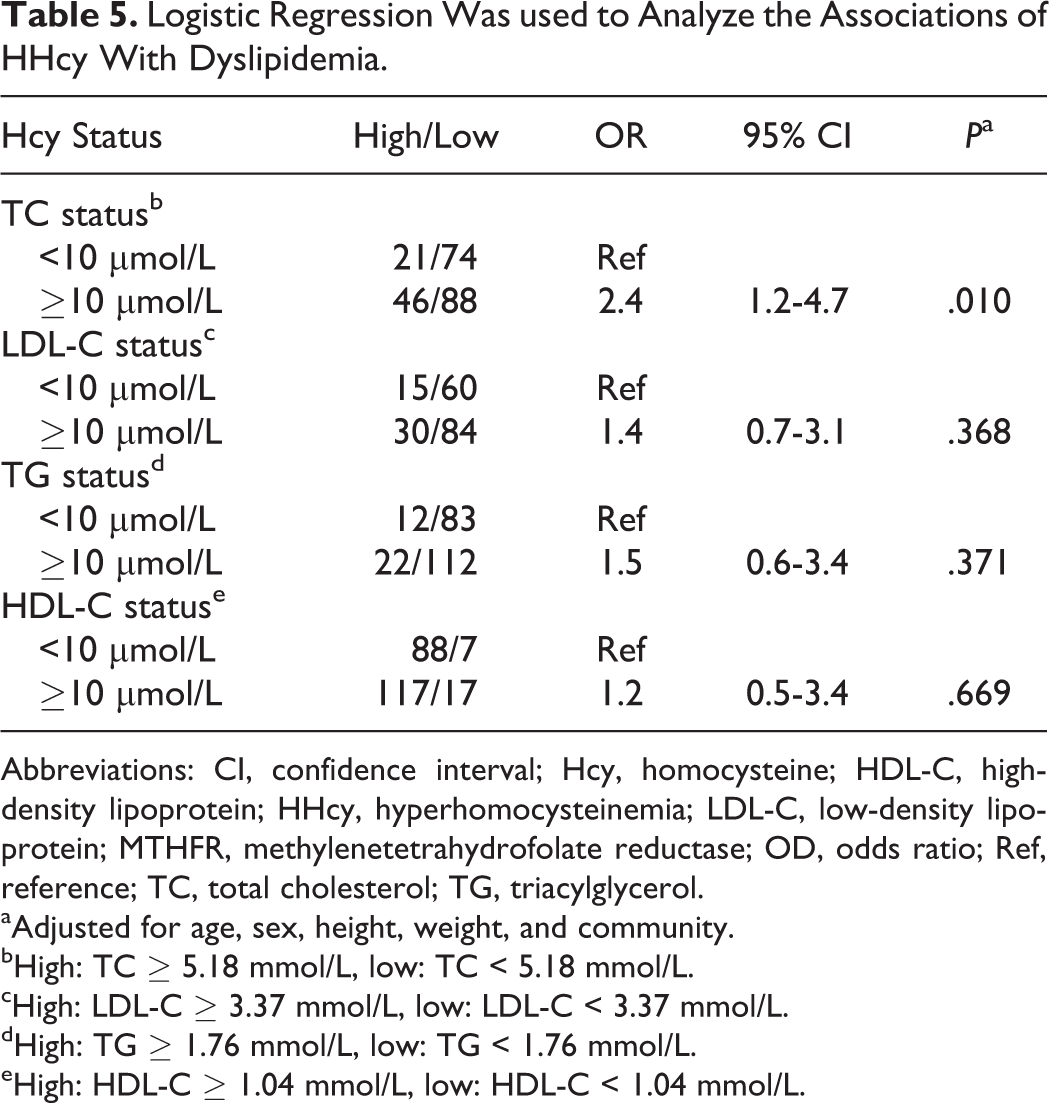
Abbreviations: CI, confidence interval; Hcy, homocysteine; HDL-C, high-density lipoprotein; HHcy, hyperhomocysteinemia; LDL-C, low-density lipoprotein; MTHFR, methylenetetrahydrofolate reductase; OD, odds ratio; Ref, reference; TC, total cholesterol; TG, triacylglycerol.
aAdjusted for age, sex, height, weight, and community.
bHigh: TC ≥ 5.18 mmol/L, low: TC < 5.18 mmol/L.
cHigh: LDL-C ≥ 3.37 mmol/L, low: LDL-C < 3.37 mmol/L.
dHigh: TG ≥ 1.76 mmol/L, low: TG < 1.76 mmol/L.
eHigh: HDL-C ≥ 1.04 mmol/L, low: HDL-C < 1.04 mmol/L.
Joint Associations of HHcy and MTHFR C677T With Dyslipidemia Profiles
As shown in Table 6, we found that compared with the CC + CT carriers with < 10 μmol/L Hcy levels, the patients with HHcy with the TT genotype had a significantly higher incidence of hypercholesterolemia (adjusted OR [95%]: 4.1 [1.8-9.4]; P = .001), although there was also a marginally higher odds of abnormal LDL-C. For both models, the ORs for individuals with both risk factors together were larger than for those with either risk factor singly, and there was no evidence of interaction between the risk factors.
Logistic Regression Was Used to Analyze Gene-HHcy Joint Associations With Dyslipidemia.
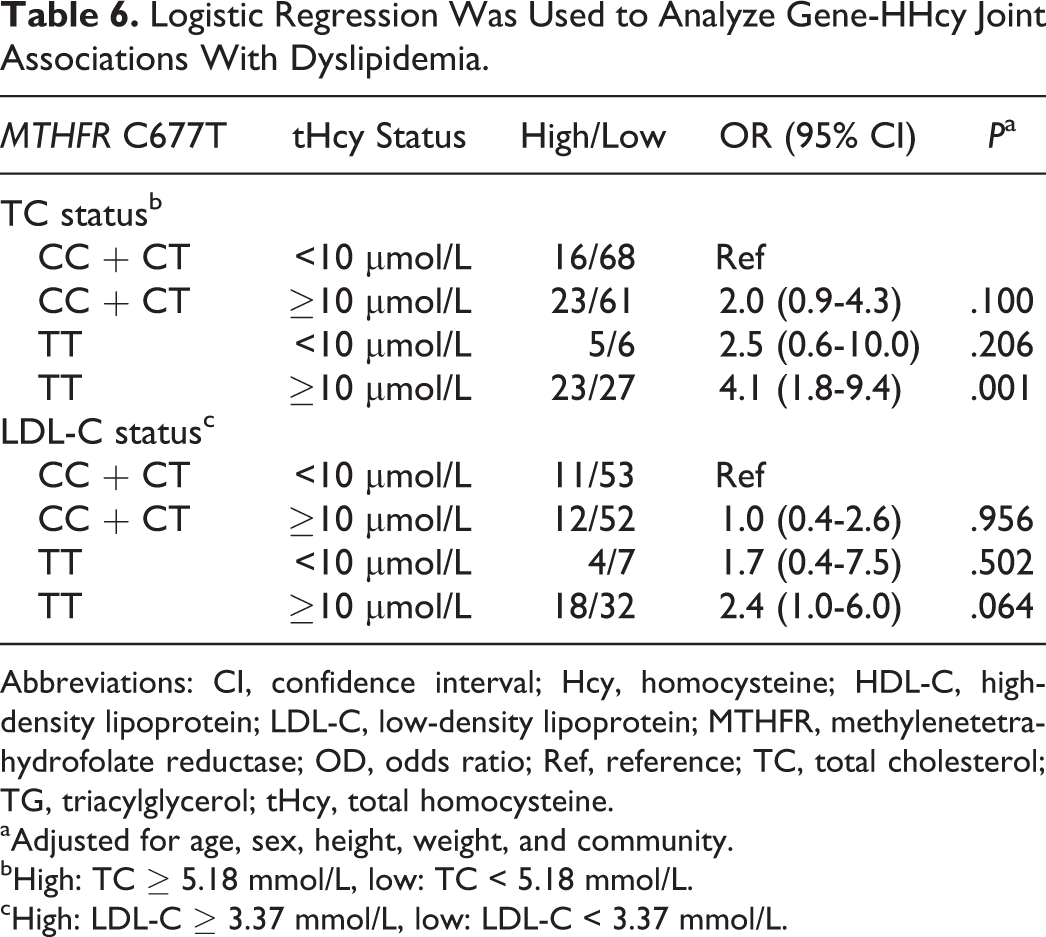
Abbreviations: CI, confidence interval; Hcy, homocysteine; HDL-C, high-density lipoprotein; LDL-C, low-density lipoprotein; MTHFR, methylenetetrahydrofolate reductase; OD, odds ratio; Ref, reference; TC, total cholesterol; TG, triacylglycerol; tHcy, total homocysteine.
aAdjusted for age, sex, height, weight, and community.
bHigh: TC ≥ 5.18 mmol/L, low: TC < 5.18 mmol/L.
cHigh: LDL-C ≥ 3.37 mmol/L, low: LDL-C < 3.37 mmol/L.
Discussion
Our present study demonstrated that the MTHFR C677T gene polymorphism was significantly associated with odds of dyslipidemia and HHcy in Chinese patients with hypertension. Furthermore, HHcy had an independent association with hypercholesterolemia and abnormal LDL-C (marginal association). The greatest odds of dyslipidemia were observed among those who were both TT genotype carriers and had HHcy.
Dyslipidemia is a highly important but modifiable risk factor for atherosclerosis, stroke, and CVD. 1,15 –17 However, the underlying mechanisms by which dyslipidemia causes complications are unclear. The MTHFR C677T is a common mutation associated with an increased risk of cardiocerebrovascular diseases, 18 –21 which indicates a possible and potential link between MTHFR C677T and lipid profiles. Yilmaz et al have reported that participants with the CC genotype have the lowest TC and LDL-C. 22 A Chinese research team has found that the carriers of the 677T allele have significantly higher TC and LDL-C than 677T allele noncarriers in the Yao and Han people of Guangxi, China. 23 Kawamoto et al reported that the MTHFR gene polymorphism is an important independent contributor to TC and HDL-C. 24 Pitsavos et al have shown that TC and TG are statistically different across MTHFR genotypes. 25 Zuntar et al reported that oxidized LDL-C levels were higher in TT than in CC and CT. 26 Our previous study has found that the MTHFR C677T gene polymorphism could be an important genetic determinant of serum lipid levels in Chinese patients with hypertension. 12 Our present study consistently demonstrated that patients having hypertension with the 677TT genotype had higher odds of abnormal TC and LDL-C than those with the 677CC + CT genotypes.
Hyperhomocysteinemia, characterized by an elevated level of plasma tHcy, is linked to an increased risk of CVD and neurological disorders. 27 –29 The relationship between MTHFR C677T and tHcy level in plasma has been well established in various populations. Numerous studies have shown that MTHFR C677T is a key determinant of plasma tHcy levels. 30 –32 Our finding is consistent with this conclusive result.
Hyperhomocysteinemia and hyperlipidemia are 2 major risk factors for the occurrence of atherosclerotic vascular disease. 33,34 In recent years, many studies have demonstrated that plasma tHcy is positively associated with dyslipidemia in patients with HHcy as well as in experimental animals, 3,5 –8 which indicates a potential mechanism is plausible. Werstuck et al reported that Hcy-induced endoplasmic reticulum stress activates both the unfolded protein response and the sterol regulatory element–binding proteins (SREBPs) in cultured human hepatocytes, vascular endothelial, and aortic smooth muscle cells. However, activation of the SREBPs leads to increased expression of the genes responsible for cholesterol/triglyceride biosynthesis and uptake, as well as intracellular accumulation of cholesterol. 8 In the experiment by Woo et al, they investigated the underlying mechanisms of Hcy-induced hepatic cholesterol biosynthesis in an animal model. Feeding a high-methionine diet to HHcy rats for 4 weeks, the mRNA expression and enzyme activity of the 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase were significantly increased in the livers of hyperhomocysteinemic rats, and there was also a marked hepatic lipid accumulation and an elevation in plasma cholesterol concentration in these rats. 7 This can activate transcription factors, SREBP-2, cyclic adenosine monophosphate response element–binding protein (CREB), and nuclear factor Y (NF-Y). 7 Thus, HHcy can induce activation of SREBP-2, CREB, and NF-Y, which likely increases cholesterol biosynthesis by transcriptionally regulating HMG-CoA reductase expression in the liver, leading to hepatic lipid accumulation and subsequent hypercholesterolemia. 7
A strength of the present study was that we not only identified the association between the MTHFR C677T polymorphism and HHcy, but we also confirmed the association of MTHFR C677T with dyslipidemia risk. We further found that tHcy was associated with the odds of dyslipidemia and those with the greatest odds had both the TT genotype and HHcy. All the findings indicated that the previously described mechanism is definitely plausible, that is, the MTHFR C677T genetic variant causes an increased tHcy level, subsequently leading to an increased risk of dyslipidemia.
However, there are several limitations in our study. First, the sample size was relatively small, so we may not have had enough power to observe some associations. Thus, our findings need to be replicated in a larger sample. Second, we did not measure plasma vitamin B (eg, folate) level or intake of B vitamins by supplements or diet. This prevented us from exploring the interesting hypothesis that B vitamin levels could modify the association of MTHFR C677T with HHcy and dyslipidemia. Finally, we only concentrated on the effect of 1 gene polymorphism on odds of HHcy and dyslipidemia. Common polymorphisms in the methionine synthase (MTR), methionine synthase reductase (MTRR), Cystathionine β-synthase (CBS) genes also need to be explored.
In summary, our results confirmed that both tHcy and the MTHFR C677T gene polymorphism may be important determinants of dyslipidemia risk in Chinese patients with hypertension.
Footnotes
Acknowledgments
The authors gratefully acknowledge the assistance and cooperation of the faculty and staff of the Anhui Medical University and thank all of the participants in our study.
Authors’ Note
This study was conducted in accordance with the current regulations of the People’s Republic of China.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (Grant No. 81373484, 81141116, and 30700454) and the Academic Leader and Reserve Candidate of Anhui Province (No. 05010543).