
Abstract
We hypothesized that patients taking warfarin require frequent hospital follow-up and they are at higher risk for complications, so the incidence of depression and anxiety is higher in patients with atrial fibrillation (AF) in the period of taking warfarin compared to the period of taking dabigatran. Fifty patients having AF without valvular diseases under treatment of warfarin in whom a transition to dabigatran was planned were consecutively enrolled in this study and followed up prospectively between July 2013 and July 2014. All patients completed Beck Depression Inventory and Hamilton Anxiety Scale (HAS) at the initiation of study and 6 months after initiation of study. Of the patients enrolled in the study, age, gender, smoking status, and comorbidities were questioned. A total of 50 patients (28 women; mean age 74.6 ± 8.7 years) treated with warfarin in whom a transition to dabigatran was planned were included. Basal mean value of BDS (15.6 ± 7.8 vs 11.5 ± 4.8, P < .001) and HAS (16.8 ± 10.4 vs 12.6 ± 8.1, P < 0.001) was significantly higher in patients when they used warfarin than when they switched to dabigatran. In categorical analysis, frequency of patients with depression (mild, moderate, and severe) was significantly higher in period of warfarin use than after dabigatran transition (n = 24, 48% vs n = 14, 28%, P = .039). Our study demonstrates that patients with nonvalvular AF under treatment of dabigatran had lower BDS and HAS scores compared to warfarin. These findings suggest that dabigatran may increase quality of life and decrease morbidity and mortality due to reduction in anxiety and depression.
Introduction
The prevalence of atrial fibrillation (AF) is approximately 1.5% to 2% of the general population. It is associated with an increased risk of stroke, congestive heart failure, and mortality. Lately, its medical, social, and economic aspects are gradually becoming important in modern societies in next years. 1 The prevention of thromboembolism, control of heart rate, and restoration of sinus rhythm are the major goals in the management of AF. 2 The patients with AF and whose risk factor(s) ≥1 are recommended to receive effective stroke prevention therapy, which is essentially oral anticoagulation (OAC) with either well-controlled vitamin K antagonist (eg, warfarin) therapy or one of the novel oral anticoagulants (eg, dabigatran). 1
Warfarin has been used as the only effective oral anticoagulant to prevent thromboembolism in patients with AF for many years. However, it has a narrow therapeutic window, extensive drug and food and alcohol interactions, and frequent monitoring. 3,4 One of the many problems with warfarin is the high interindividual and intraindividual variation in international normalized ratios (INRs). 3 Moreover, suboptimal anticoagulation can lead to stroke or life-threatening bleeding. Dabigatran is a prodrug, which is rapidly absorbed in the gastrointestinal tract and metabolized in the liver, it is predictable with low inter- and intraindividual variability and generally requires no coagulation monitoring. The cytochrome P450 system is not involved in its metabolism, and only a small number of important drug interactions are identified so far. 4 The Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY) study showed that the rate of the systemic embolism or stroke was significantly lower, with dabigatran at a dose of 150 mg twice daily, and the incidence of nonhemorrhagic stroke was also significantly lower, with 150 mg of dabigatran etexilate. 5 Depression and anxiety disorders are the most common psychiatric diseases occurring in patients with somatic diseases and they usually coexist. 6 Worsening in the quality of life (QoL), functional disability, and direct biological effects of organic diseases are the main reasons for development of depression. 7 Previously, we found that patients with prosthetic heart valve disease (all of these patients have to take warfarin) had higher prevalence of depression and higher scores of anxiety and depression. 8
We hypothesized that patients taking warfarin require frequent hospital follow-up and they are at higher risk for complications, so the incidence of depression and anxiety is higher in patients with AF in the period of taking warfarin compared to the period of taking dabigatran.
Methods
Patients
Fifty patients having AF without valvular diseases under treatment of warfarin in whom a transition to dabigatran was planned were consecutively enrolled in this study and followed up prospectively between July 2013 and July 2014. These patients had been taking warfarin for at least 1 year prior to the trial. The reasons for transition from warfarin to dabigatran in study patients are labile INR and transient ischemic attack while on warfarin and patient preference (problems of INR monitoring). All patients completed Beck Depression Inventory and Hamilton Anxiety Scale (HAS) at the initiation of study and at the end of the sixth month of taking dabigatran. Of the patients enrolled in the study, age, gender, smoking status and comorbidities (hypertension, obesity, diabetes, chronic renal failure, cerebrovascular disease), history of bleeding, and transfusion were questioned. Patients were excluded if they were less than 18 years old or if they suffered from any major psychiatric disorder and or if they were taking medication to relieve anxiety or depression.
At the initiation of study complete blood count, prothrombin time, INR, and biochemical parameters were assayed, and echocardiogram was recorded. The study conforms to the principles outlined in the Declaration of Helsinki and was approved by the ethics committee for clinical research in Duzce University School of Medicine Hospital.
Beck Depression Inventory
The Beck Depression Scale (BDS), created by Aeron Beck in 1961, is one of the most common scales used for assessment of mood disorders and depression. 9 It consists of 21 questions, 15 for emotional and 6 for somatic symptoms, and is filled by the patient. In BDS, for each question the scoring ranges from 0 to 3. The total score is calculated by summation of all the patients’ responses, so the maximum possible sum is a score of 63. Higher BDS scores on the scale indicate a greater level of depressive symptoms, 0 to 11 indicates no depression, 12 to 16 mild depression, 17 to 29 moderate depression, 30 to 39 severe depression, and above 40 indicates very severe depression. 9
Hamilton Anxiety Scale
The HAS measures the severity of anxiety level and symptom distribution. It is a 14-item test including mood and somatic symptoms administered by an interviewer. Each item is rated on a 5-point Likert-type scale ranging from 0 to 4, so the sum of the score range is between 0 and 56. The patients must complete the test within 72 hours from the admission. 6
Statistical Analysis
Statistical Package for Social Sciences software (SPSS 20, Chicago, Illinois) was used for analysis. Continues variables were shown as mean ± standard deviation and categorical variables were stated as number and percentages. One sample Kolmogorov-Smirnov test was used to determine whether the study population is normally distributed. Chi-square, paired sample correlations, and t tests were used to compare related variables. Differences were considered significant at a P value of < .05.
Results
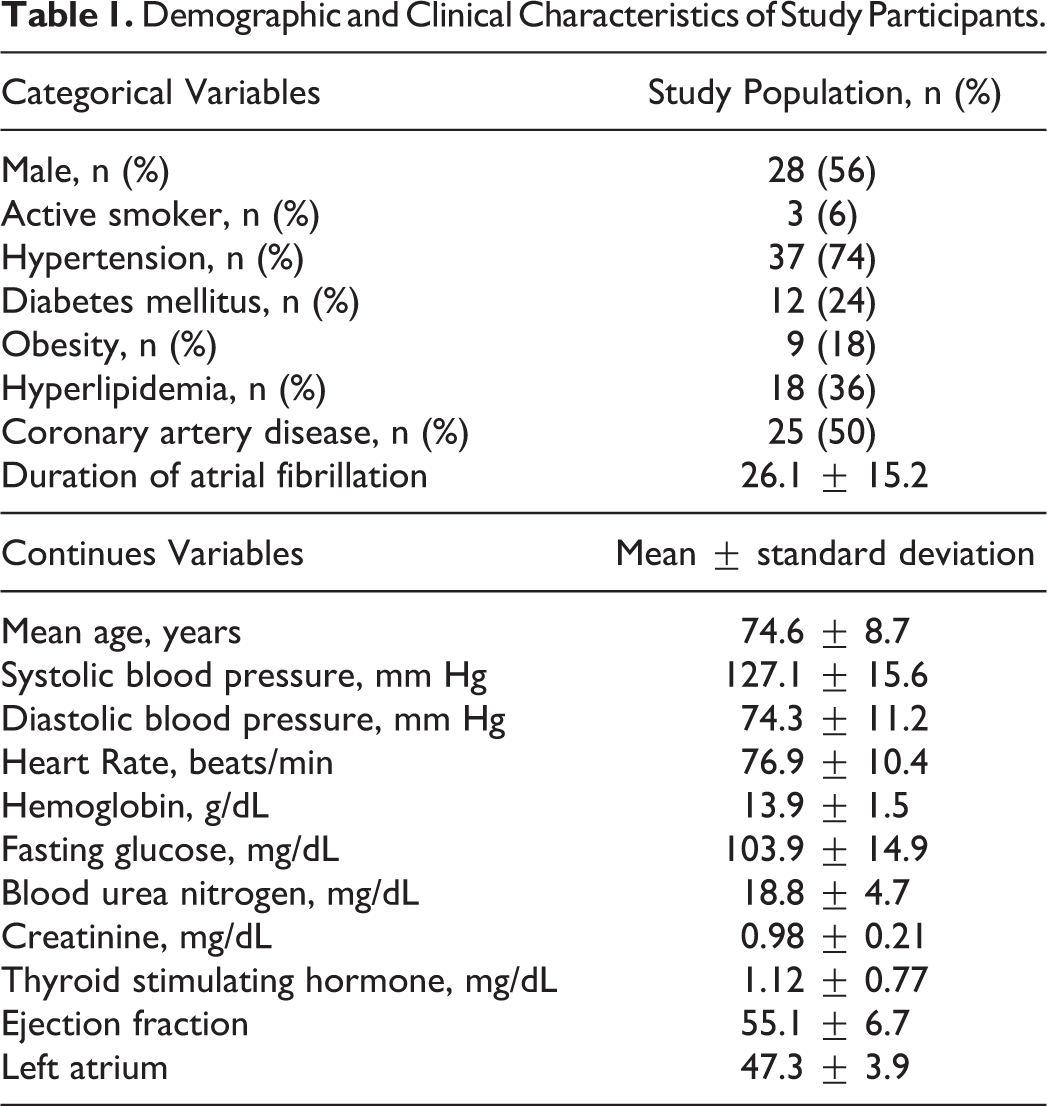
A total of 50 patients (28 women; mean age 74.6 ± 8.7 years) treated with warfarin in whom a transition to dabigatran was planned were included. Duration of AF was 26.1 ± 15.2 months at the beginning of study. Table 1 shows basic demographic and clinical characteristics of study patients.
Demographic and Clinical Characteristics of Study Participants.
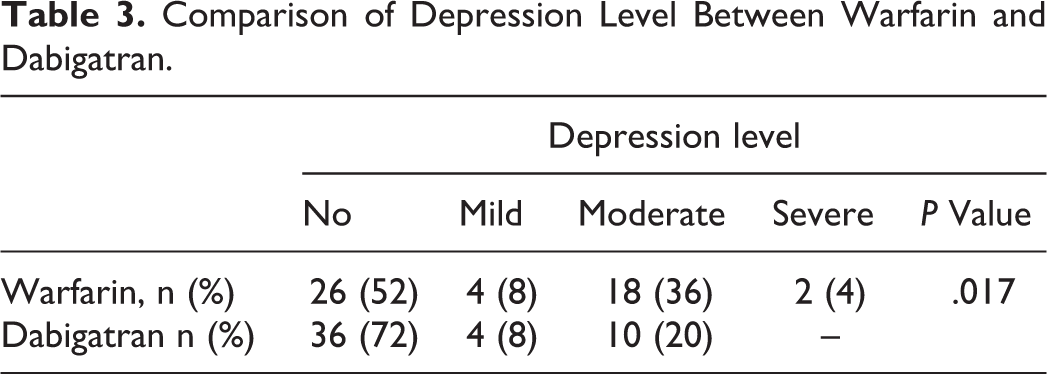
The mean follow-up period was 9.5 ± 2.2 months (range 6-12) after the baseline admission. Table 2 gives comparison of mean values of BDS and HAS in patients before and after switching from warfarin to dabigatran. Mean scores of BDS (15.6 ± 7.8 vs 11.5±4.8, P < .001) and HAS (16.8 ± 10.4 vs 12.6 ± 8.1, P < .001) were significantly higher in patients while they used warfarin before they were switched to dabigatran. In categorical analysis, frequency of patients with depression depending on back depression scale (mild, moderate, and severe) was significantly higher while they were under treatment of warfarin use than under treatment of dabigatran (n = 24, 48% vs n = 14, 28%, P = .039). According to BDS categories, comparison of depression level between the period of warfarin and dabigatran use was shown in Table 3.
Comparison of BDS, HAS, and Frequency of Depression in Study Patients While Using Warfarin and While Using Dabigatran.
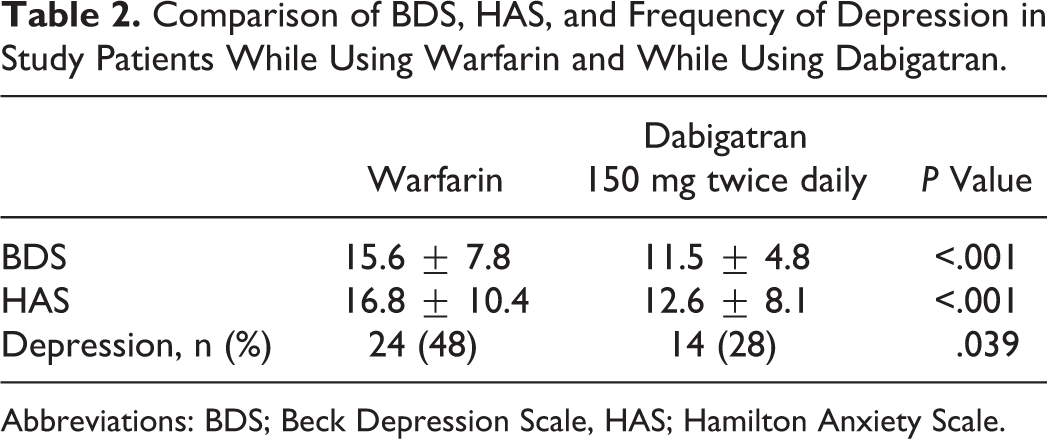
Abbreviations: BDS; Beck Depression Scale, HAS; Hamilton Anxiety Scale.
Comparison of Depression Level Between Warfarin and Dabigatran.
Discussion
The present study showed that basal (warfarin used) average score of BDS and HAS was significantly higher than when dabigatran used. The Presence of depression was significantly higher when using warfarin than while using dabigatran according to the BDS.
Depression is the most common psychiatric disorder accompanying organic disorders. It is a significant clinical syndrome affecting mortality and morbidity in patients with organic disorders. 10 The prevalence of major depression was found to be 5% to 10% in inpatients and 9% to 16% in outpatients with organic disorders. 11 Depression and anxiety disorders usually coexist. Worsening in the QoL, functional disability, and direct biological effects of organic diseases are the main reasons for development of depression. 12 Depression was more frequent in our study patients when warfarin was used (48%) according to other studies. Comorbidities (hypertension [74%], diabetes mellitus [24%], and coronary artery disease [50%]) may explain more frequent depression in this study.
It was determined that patients undergoing heart operation experienced such physical and psychological problems as decrease in appetite, sleep disturbances, fatigue and activity intolerance, anxiety, and depression within 6 months of being discharged. 13
The relationship between biobehavioral stress and cardiac arrhythmias has been recognized before. 14,15 The patients with AF have significantly poorer QoL compared to healthy controls. 16,17 In another study, one third of patients with AF have elevated levels of depression and anxiety, and symptoms of depression were the strongest independent predictor of future QoL in these patients. 18
On the other hand, Eaker et al found that increased tension in men was significantly related to the development of AF; furthermore, anxiety was significantly related to total mortality. 19
Sang et al demonstrated that contributors to the improvement of depression, anxiety, and QoL included catheter ablation, avoidance of warfarin use, initial higher levels of depression and anxiety, and lower QoL. 20
Outpatients undergoing warfarin therapy had a significantly higher risk for death if they were burdened with symptoms of depression or anxiety showed in a very recent study. 21
Previous data have been conflicting on whether a positive impact on QoL from oral anticoagulant therapy or high levels of displeasure with OAC therapy perhaps associated with poor therapeutic control. 22,23 Cromheecke et al 24 and Gadisseur et al 25 showed that patients with better INR control score higher on measures of QoL. In another study, change in anxiety and treatment of QoL scores were compared between patient self-management of OAC and routine care with postal questionnaires at baseline and 12 months. Self-management of OAC does not adversely affect the level of anxiety and provides an increase in self-efficacy compared to routine care, which is greatest in patients achieving the highest level of therapeutic control. 26
One of the many problems with anticoagulation with warfarin is the high interindividual and intraindividual variation in INRs. Warfarin also has significant drug, food, and alcohol interactions. Patients may stay within the intended INR range of 2.0 to 3.0 for 60% to 65% of the time in clinical trials, but many “real-life” studies suggest that this figure may be 50%. Actually, having patients under the therapeutic range for 60% of the time may completely offset the benefit of warfarin. Dabigatran offer better efficacy, safety, and convenience compared with OAC with warfarin. 1 We supposed that the patients who have used dabigatran less admitted to health care service to monitor INR and less experienced with drug and food interactions with dabigatran than warfarin. That was why the patients who were switched to dabigatran from warfarin had low BDS and HDS scores.
We demonstrated before 8 a significant relationship between the depression and INR levels in mechanical prosthetic valve disease. The INR levels were lower than expected in the very severe depression group. These findings may indicate that patients with more depression and anxiety have lower sense of responsibility to protect themselves from possible complications that may occur due to prosthetic heart valve disease. Similarly, we believe that patients with depression having nonvalvular AF may harm themselves because of not checking INR and hence cannot reach target values. This problem can be avoided by dabigatran or other New Oral Anticoagulant (NOAC) agents.
Conclusion
Our study demonstrates that patients with nonvalvular AF under treatment of dabigatran had lower BDS and HAS scores compared to warfarin. These findings suggest that dabigatran may increase QoL and decrease morbidity and mortality due to reduction in anxiety and depression.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.