
Abstract
Obstructive sleep apnea syndrome (OSAS) is a risk factor for arterial thrombosis and cardiovascular morbidity. Activated platelets play key roles in the development of atherothrombosis, thus may be involved in these complications of OSAS. Herein, we evaluated the relationship between severity of OSAS and the degree of platelet aggregates as a marker of activated platelets in 64 patients with OSAS. Platelet aggregations were determined by means of optical aggregometry, using adenosine diphosphate (ADP) as an agonist. Compared with the control group, ADP-induced platelet aggregability was increased in patients with total OSAS, severe OSAS, and in mild to moderate OSAS. Moreover, ADP-induced platelet aggregation was correlated with the Epworth sleepiness scale (ESS) in patients with severe OSAS. Obstructive sleep apnea syndrome is associated with enhanced platelets aggregations, which may predispose the cardiovascular sequels. The ESS may be important in predicting platelet activation and thus atherothrombotic complications in those with OSAS.
Keywords
Introduction
Obstructive sleep apnea syndrome (OSAS) is characterized by recurrent episodes of complete or partial collapse of the upper airway during sleep, leading to apneas or hypopneas, respectively. These repetitive obstructions cause intermittent fall in blood oxygen, increase in carbon dioxide levels, and frequent arousal from sleep. 1 The most significant complications are cardiovascular diseases, resulting in severe morbidity and mortality. 2
Platelets play an evident role in cardiovascular disease, both in the pathogenesis of atherosclerosis and in the development of acute thrombotic events. 3 This role has been evidenced by the benefit of antiplatelet agents in these disorders. 4 The status of platelet activation in patients with OSAS had been assessed in some studies using different methodologies. Its results indicated either increased platelet activation in OSAS, 5 –13 a slight effect, 14 or none at all. 15 –18 So a more unified method is warranted.
Platelet aggregability may be a simple, direct screening method of investigating platelet activation in OSAS. However, few limited studies with conflicting results are present until now. 14,15,19,20 These controversies about the state of platelet activation/aggregability in patients with OSAS encouraged us to investigate adenosine diphosphate (ADP)-induced platelets aggregability in polysomnographically (PSG) verified obstructive sleep apnea patients of our sleep laboratory.
Methods
Study Design and Participants
Between September 2012 and August 2014, a total of 180 patients admitted to the sleep unit underwent a PSG evaluation and were diagnosed as patients with OSAS. Of the180 patients, 64 were enrolled in this study. Inclusion criteria were patients with symptoms of nocturnal snoring and/or excessive daytime sleepiness. Exclusion criteria were age <18 years; platelets count <150 × 109/L or > 400 × 109/L; hemoglobin level <100 g/L and/or hematocrit value <35%; any hematological diseases, especially platelet disorders; cardiovascular disorder, or any cardiac disease; lung disease (chronic obstructive pulmonary disease and idiopathic pulmonary fibrosis); diabetes mellitus; hypertension; chronic renal or hepatic diseases; drug intake, especially nonsteroidal anti-inflammatory drugs within 21 days; smoking or tobacco use; a history of recent blood transfusion (three weeks); and caffeine ingestion on the day of testing. Additionally, there was no history of herbal remedies, garlic, alcohol, and excess vegetables ingestion. Moreover, patients diagnosed with obesity hypoventilation, overlap syndrome, complex sleep apnea, central sleep apnea, or Cheyne-Stokes sleeping disorder were excluded from the study.
Detailed medical history, physical examination, a respiratory function test, electrocardiogram, and chest X-ray were investigated. Initially, patients were grouped according to the severity of OSAS into 3 categories: mild (apnea–hypopnea index [AHI] 5 to <15), moderate (AHI 15 to <30), and severe (AHI >30). Further, we combined mild and moderate groups into 1 group (AHI 5 to <30). As regards the control group, 60 individuals (ages 44-63) diagnosed with simple snoring (AHI <5) were chosen.
Polysomnographic sleep study
All patients had been clinically assessed in the sleep laboratory by subjecting them to full night PSG sleep study (Viasys, Germany) in the supine position for a definitive diagnosis. Polysomnography was performed and scored according to standard criteria using nasal pressure cannulae and tracheal sounds (suprasternal microphone) for airflow measurement. Respiratory events were scored manually. Apnea was defined as cessation of airflow for ≥10 seconds. Hypopnoea was defined as either 30% decrease in the airflow with 4% decrease in capillary oxygen saturation (SpO2) or 50% reduction in the airflow accompanied by 3% decrease in SpO2. The oxygen desaturation index is the number of times per hour of sleep that the blood’s oxygen level drops by 3% or more from baseline. The AHI is the index used to indicate the severity of sleep apnea. It is represented by the number of apnea and hypopnea events per hour of sleep. Epworth sleepiness scale (ESS) is a scale intended to assess daytime sleepiness through a short questionnaire of 8 questions answered by the patient concerning the daily activities. 21
Measurement of Platelet Aggregation
Blood sampling and preparation of platelet-rich plasma
Venous blood samples were obtained from resting patients and healthy controls who signed the informed consents. Fasting blood samples (8 hours) were collected by venipuncture from the cubital vein using citrated blood collection system, with minimal stasis. Blood of 1.8 mL was delivered into the citrated plasma blood collection system sterile vacutainer tube containing 200 µL sodium citrate (3.2%) in a 9:1 v/v ratio (0.129 mol/L) solution as anticoagulant (9 parts of blood with 1 part of anticoagulant; Vacutest, Kima s.r.l., Italy). From the citrated blood samples, platelet-rich plasma (PRP) was prepared by slow-speed centrifugation (MPW 350 R, MED. Instruments, Warsaw, Poland) at 170g for 10 minutes at room temperature (RT). After centrifugation, the PRP was collected. The remaining blood was centrifuged at 2000g for 15 minutes at RT for the preparation of the platelet-poor plasma (PPP) that may be used for autologous dilution of high platelets count in PRP (if any). 22
In vitro platelet aggregation assay
Platelet-rich plasma was obtained freshly by centrifugation of whole citrated blood sample as mentioned previously. The platelet count of PRP was measured for each sample to ensure that the platelet count was in the range of ∼ 250 × 109/L. The PRP (480 µL) was incubated for 5 minutes at 37°C in the aggregation cuvette. Aggregation agonist adenosine 5’ diphosphate (ADP; final concentration: 10 μmol/L) of 5 μL was then added (Chrono-Log Corporation, Havertown, Pennsylvania). The resulting aggregation was monitored and recorded for 6 minutes using the dual-channel Lumi-aggregometer (Chrono-Log 540-VS Platelet Aggregometer; Chrono-Log Corporation). All measurements were done in less than 1 hour. The results are expressed as the percentage of agonist-induced platelet aggregation. 22
Statistical Analysis
All variables were tested for normality with the Kolmogorov-Smirnov test. Nonnormally distributed continuous variables are summarized as medians (ranges). Categorical variables are expressed as numbers (percentages). Comparisons between independent groups were made using the Mann-Whitney U test. Correlations between noncontinuous variables and continuous variables with a nonnormal distribution were assessed using Spearman correlation. Correlations between continuous variables were assessed using Pearson correlation. Univariate and multivariate linear regression analysis were performed to determine the independent correlations of studied parameters. P value <.05 was considered statistically significant. The statistical analysis was performed with SPSS for Windows version 18.0 (SPSS, Chicago, Illinois).
Results
Baseline Characteristics
The demographic and clinical characteristics of the patients and controls are shown in Table 1. We included a total of 64 patients with OSAS (30 [46.9%] patients with mild to moderate and 34 [53.1%] patients with severe OSAS] and 60 simple snoring control cases. There were no significant differences between the 2 groups or subgroups regarding age, sex distribution, body mass index (BMI), hemoglobin, and hematocrit.
Demographic, Clinical. and Laboratory Characteristics of the Studied Groups.a
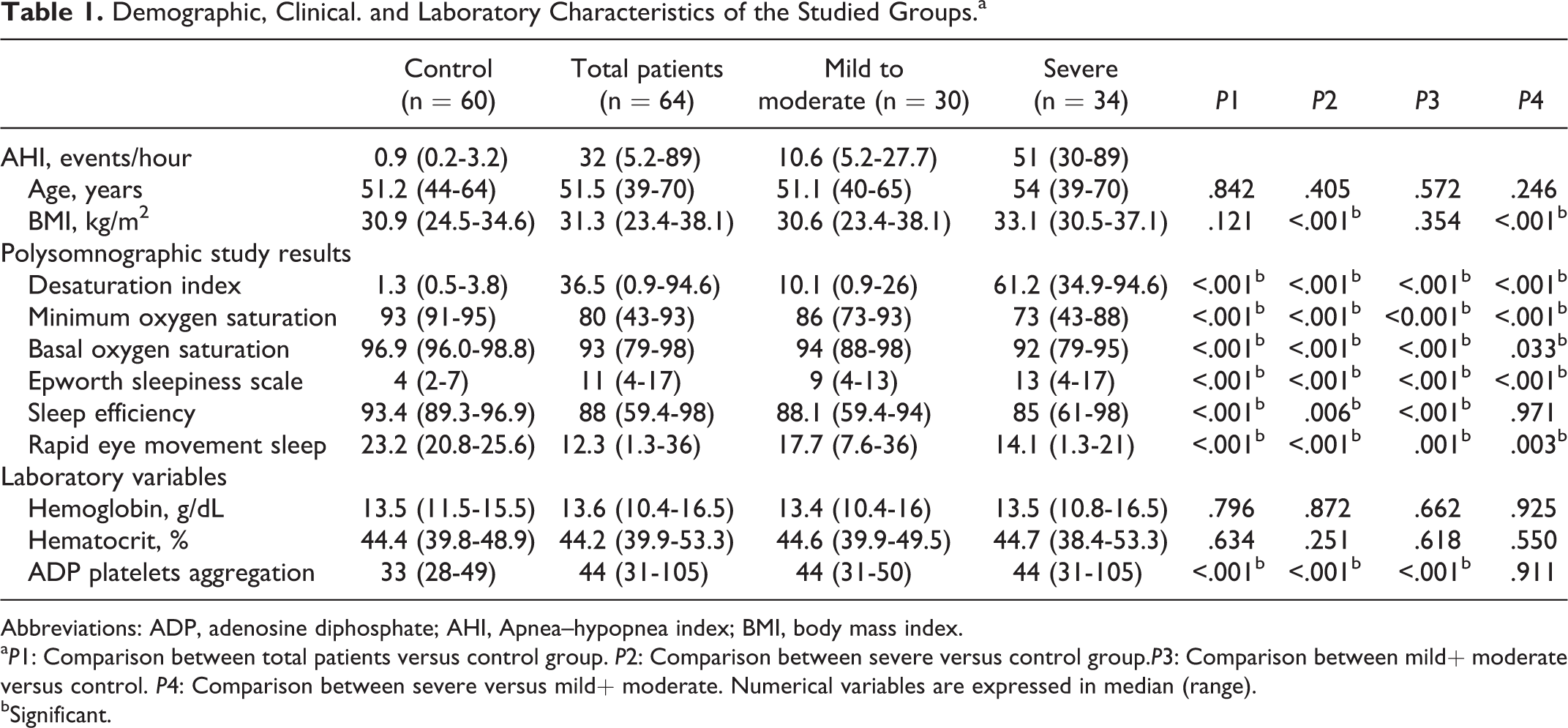
Abbreviations: ADP, adenosine diphosphate; AHI, Apnea–hypopnea index; BMI, body mass index.
a P1: Comparison between total patients versus control group. P2: Comparison between severe versus control group.P3: Comparison between mild+ moderate versus control. P4: Comparison between severe versus mild+ moderate. Numerical variables are expressed in median (range).
bSignificant.
Patients with OSAS had significantly higher desaturation index, ESS, and significantly lower minimal, basal oxygen saturation, sleep efficiency, and rapid eye movement sleep when compared to control participants (Table 1). The AHI showed significantly positive correlation with oxygen desaturation index, ESS, and significantly negative correlation with minimal oxygen saturation, basal oxygen saturation in the OSAS group. The AHI showed significantly positive correlation with oxygen desaturation index and ESS and significantly negative correlation with minimal oxygen saturation in severe OSAS group (Table 2 and Figure 1).
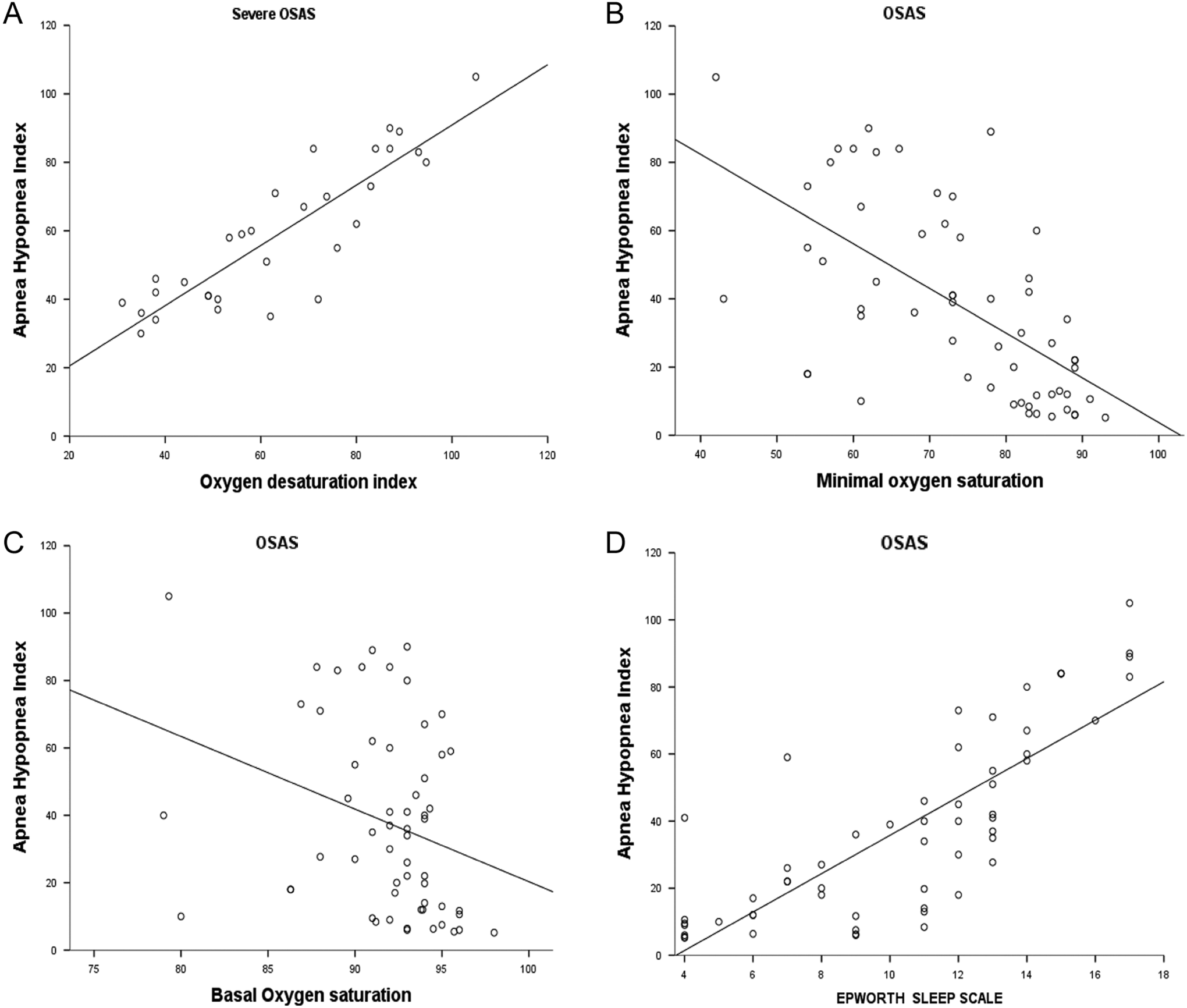
Correlations between apnea-hypopnea index (AHI) and Oxygen Desaturation index in severe obstructive sleep apnea syndrome (OSAS) group (A), AHI and minimal oxygen saturation (B), basal oxygen saturation (C), and Epworth sleep scale (D) in total OSAS group.
Correlations Between AHI and Different Parameters in the Studied Groups.
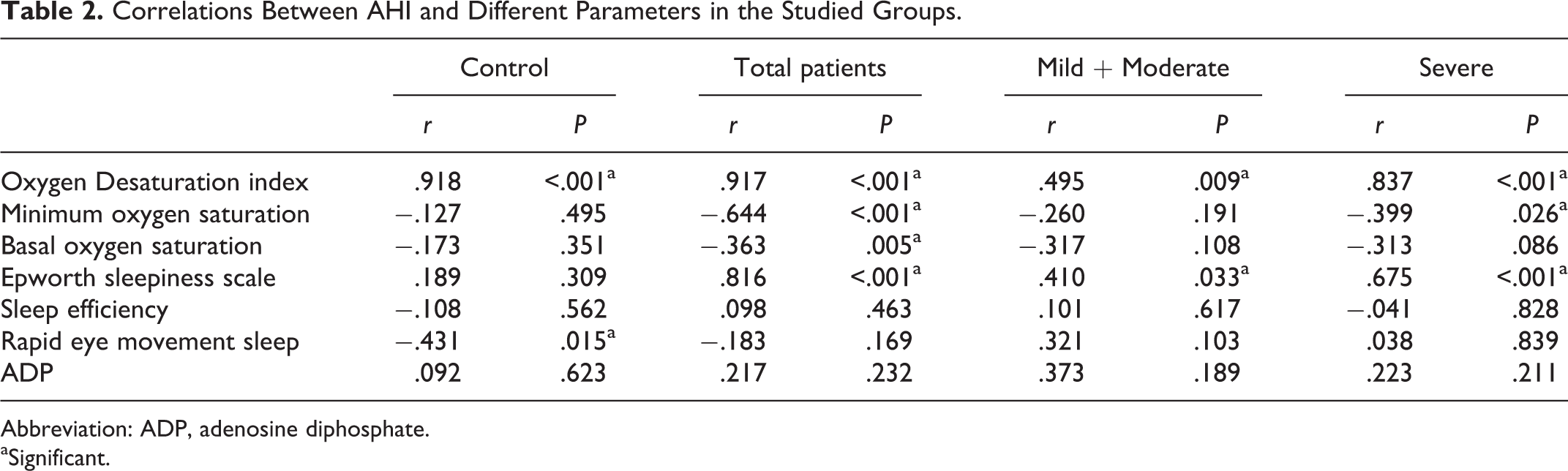
Abbreviation: ADP, adenosine diphosphate.
aSignificant.
The ADP-induced platelet aggregation was significantly higher in OSAS, mild to moderate, and severe OSAS versus control participants (Table 1; Figure 2). The ADP-induced platelet aggregation showed significantly positive correlation with ESS in severe OSAS group (Table 3 and Figure 3).
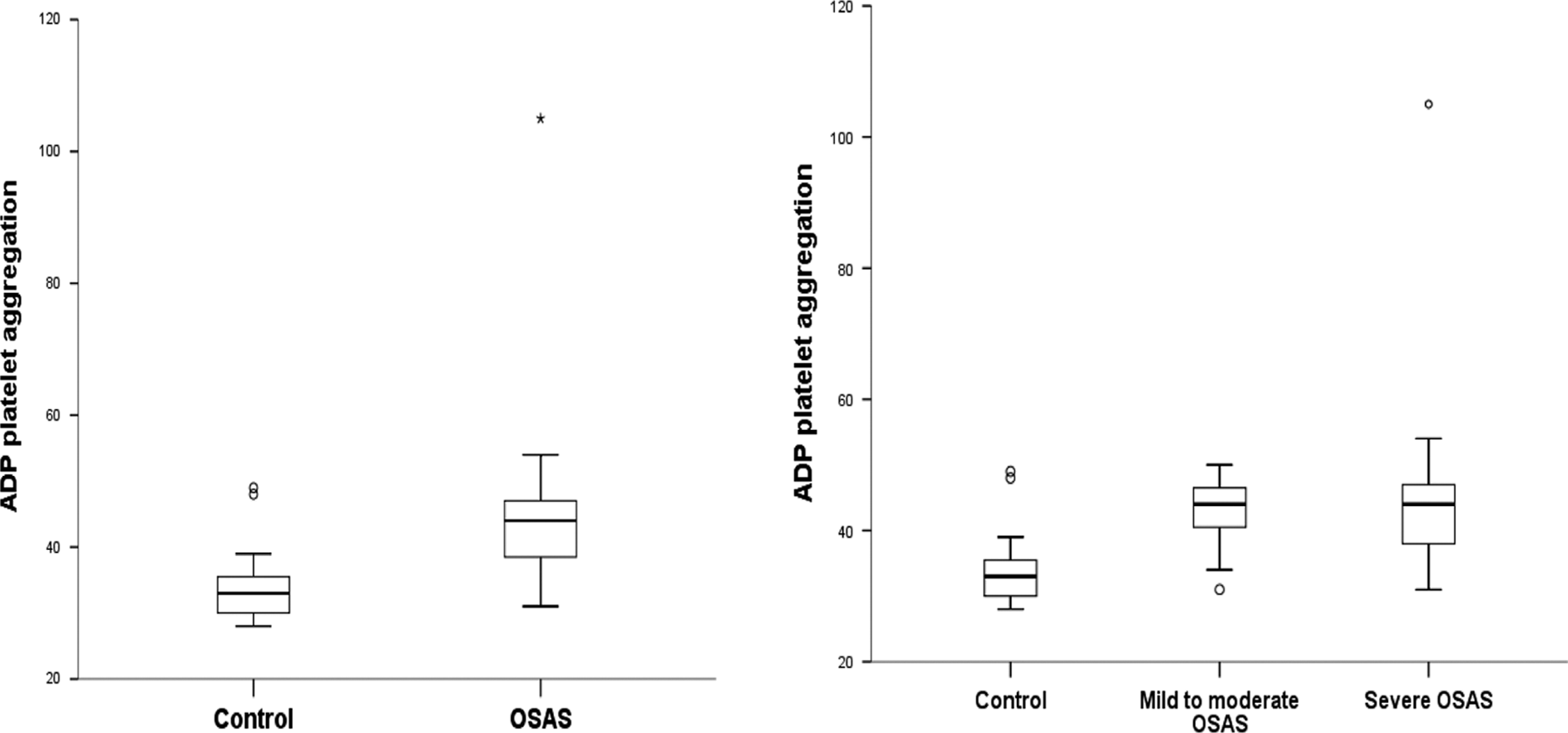
Adenosine diphosphate (ADP) platelet aggregation distribution in patients with obstructive sleep apnea syndrome (OSAS) and control participants.
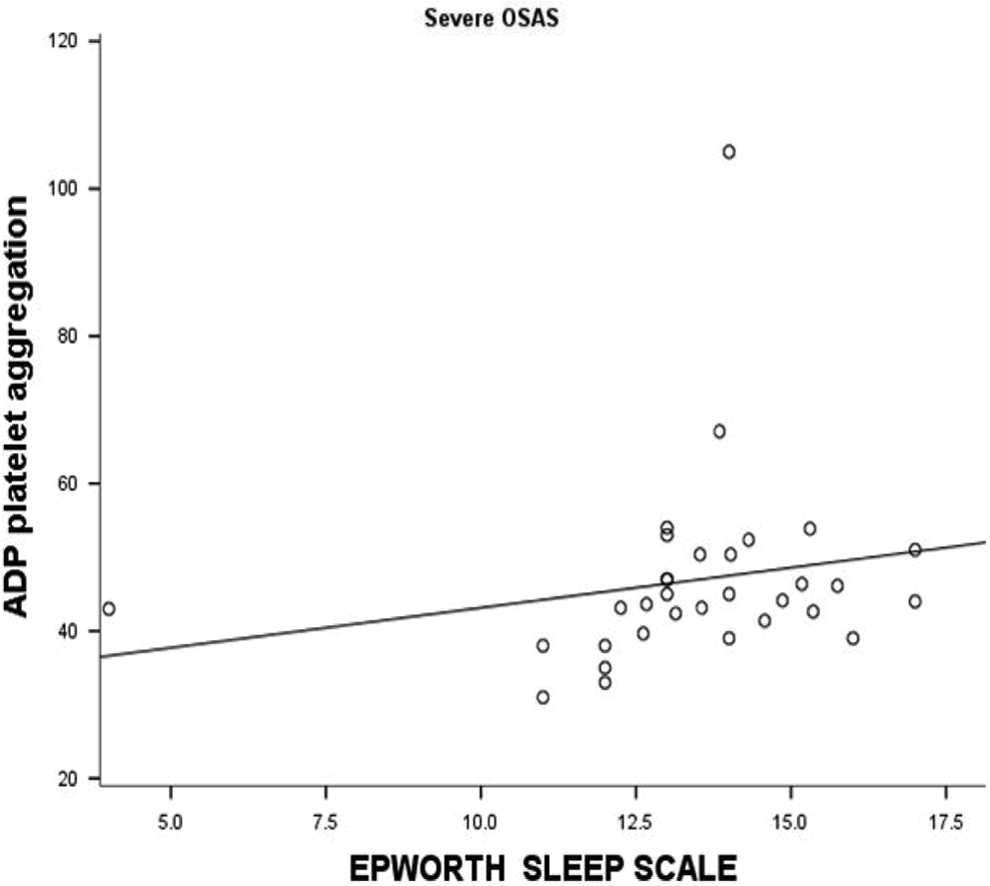
Correlations between adenosine diphosphate (ADP) and Epworth sleep scale in severe OSAS group.
Correlations between ADP Platelets Aggregation and Different Parameters in Studied Groups.
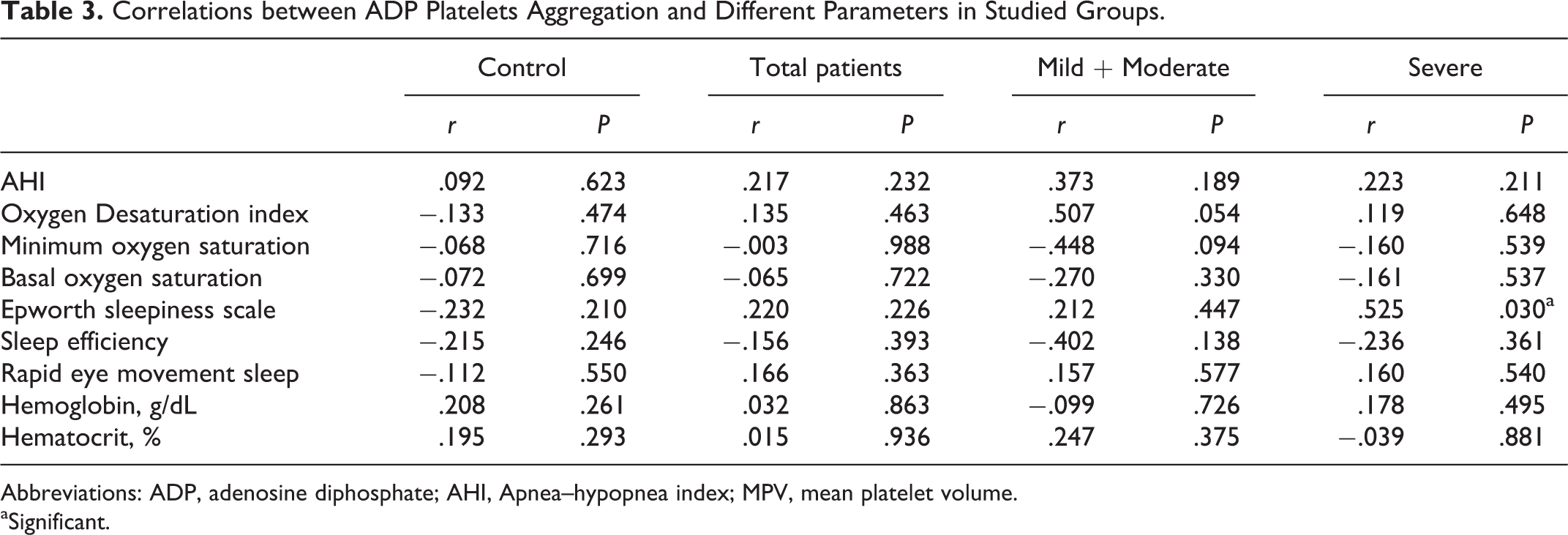
Abbreviations: ADP, adenosine diphosphate; AHI, Apnea–hypopnea index; MPV, mean platelet volume.
aSignificant.
Linear Regression Analysis
Independent variables including age, BMI, AHI, and oxygen desaturation index were recruited into linear regression analysis as predictors for ADP-induced platelet aggregation. No significant association was found between any of these predictors and ADP-induced platelet aggregation (Table 4).
Predictors of ADP-Induced Platelet Aggregation by Linear Regression Analysis.
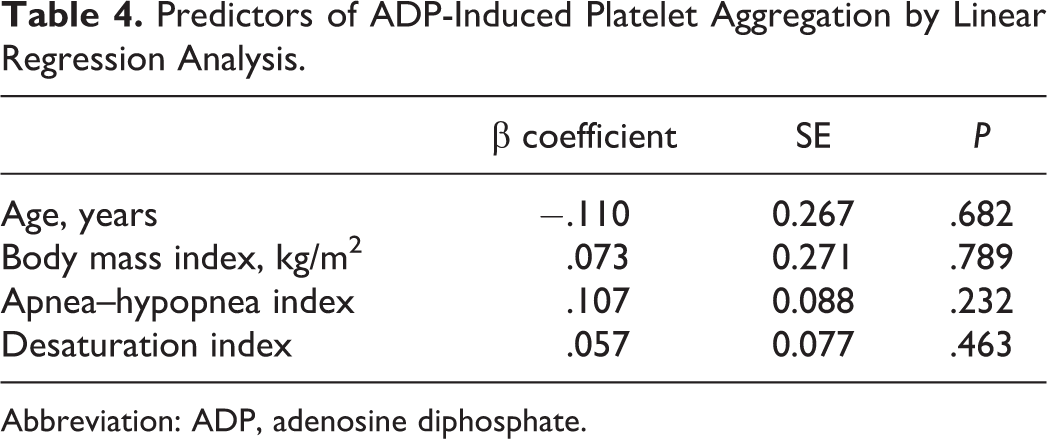
Abbreviation: ADP, adenosine diphosphate.
Discussion
It has been established that there is a relationship between OSAS and cardiovascular disease. 2,23 Platelets are an important component of normal hemostasis; however, they also contribute to the development of thrombotic disorders, particularly cardiovascular disease. 3 Platelet activation results in a complex series of changes that can be used as a marker of platelet activation. These changes include redistribution and conformational molecular changes in the platelet receptors, secretion of granule contents, procoagulant surface and microparticles generation, and platelet aggregates production, which is the most important function of platelets. 24 Herein, we choose light transmission platelet aggregometry which is still deemed the gold-standard test for the assessment of the platelet functions in patients with OSAS. Platelet aggregometry is the most widely employed methodology and the first diagnostic step for detecting platelet function disorders and monitoring antiplatelet therapies. 25,26
In the literature, platelets activation has been investigated in patients with OSAS by different methods. 5 –20 The results, however, are still controversial and limited by methodological issues. More specifically, there have been only 3 studies in the literature with limited numbers of patients with OSAS which investigated platelet aggregability with no significant differences between OSAS and control groups. 14,15,19 In contrast, in a more recent study, 20 with a moderate number of patients, increased platelets aggregability was found more in patients with moderate to severe OSA. However, surprisingly, one major limitation of that study was that the diagnosis of OSAS was not proven by PSG. Traditionally, it is established that PSG has been used as a reference standard for the diagnosis of OSAS in a sleep laboratory. 27 The exclusion of OSAS by clinical criteria only may not be valid, since a discrepancy between the symptoms and the PSG findings has been reported. 27 –30
As an attempt to settle this controversy, we investigated ADP-induced platelets aggregation in clinically and PSG-verified patients with OSAS. In this study, ADP-induced platelet aggregability was increased in the total group of patients with OSAS, compared to the control group. The intermittent hypoxia in OSAS may contribute to a state of oxidative stress, inflammation, and endothelial dysfunction that may increase platelets activation. However, it is still unknown how intermittent hypoxemia contributes to vascular diseases. 30,31 The thromboxane A2 pathway is activated in OSAS, and this may be related to the the vascular remodeling in OSAS 32 ; thus, the enhanced platelets aggregations may be the major player in cardiovascular risk in OSAS. In this respect, thromboelastography, a unique test of hemostasis, has been suggested for risk evaluation of future cardiovascular disease in patients with OSAS. 33
Hemostatic measurements from studies that investigate OSAS are difficult to compare except if it addresses a relationship between AHI, the severity index of OSAS, and hemostasis variables. In this study, however, we could not document a significant relationship between ADP aggregation and the severity of OSAS, indicated by AHI or the oxygenation parameters. In contrast, few studies showed a relationship between platelet activity, not aggregation, and OSAS severity. 6,8 Specifically, in a later study, the severity of OSAS influenced platelet aggregability more than total hypoxic time. 20 Alternatively, in our study, ADP platelet aggregation was positively correlated with ESS in patients with severe OSAS. Importantly, the ESS has both a diagnostic and a prognostic value in OSAS. 21,34
Some interfering factors may account for the discrepancy of the results of platelet aggregation in OSAS in the literature. These factors are the different samples sizes, particularly for severe OSAS; the nonspecific diagnosis of OSAS by relying on oximetry or clinical criteria not PSG; and the absence of adjustment or exclusion of cardiovascular risk factors that may alter platelets aggregations. Notably, our study design had been strengthened by the exclusion of potential confounding variables of cardiovascular risk and preexisting cardiovascular diseases and the usage of the gold-standard diagnostic technique of in-laboratory PSG. In contrast, one limitation of this study is that we had not monitored the increased platelet response to ADP after continuous positive airway pressure (CPAP), the gold-standard treatment of OSAS. 35 Few available data suggested a decrease in platelet activation after CPAP treatment in patients with OSAS, although the duration of therapy required remains unknown. 36,37 In one study, platelets aggregation decreased significantly after both 1-night and 3-month CPAP therapy. 8 Others have found 1 month of CPAP therapy to be sufficient. 38,39 Conversely, Oga et al 20 found 1 month to be inadequate, and only after 3 months of CPAP therapy did they see a statistically significant reduction in platelet aggregability.
Conclusion
Platelet activation is a link between thrombosis and inflammation. We demonstrated enhanced ADP-induced platelets aggregations in patients with OSAS. Moreover, platelet aggregation was positively correlated with ESS in patients with severe OSAS. Our findings suggest that ESS may be important predictor of platelets activation and thus atherothrombotic complications in patients with severe OSAS. The hypercoagulable state induced by OSAS warrants more studies, particularly regarding the full assay of platelets markers to evaluate platelet activity and the role for antiplatelet medications to reduce morbidity in those who are unable to achieve optimum control of OSAS with currently available treatments.
Footnotes
Authors’ Note
The project was partly supported by the Department of Clinical Pathology, Mansoura Faculty of Medicine, Mansoura University, Egypt.
Acknowledgment
The authors gratefully acknowledge the assistance of Prof. Dr. Hanan Azzam (Professor of Clinical Pathology, Mansoura Faculty of Medicine, Mansoura University, Egypt) in the general support of the Study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.