
Abstract
Objective: To investigate the effects of different aminoglycoside antibiotics on platelet aggregation and blood coagulation, as well as the underlying mechanisms. Method: Blood samples were collected and prepared as platelet-rich plasma and platelet-poor plasma samples. Then assigned into different groups for the following antibiotics treatments: gentamicin, streptomycin, etimicin, amikacin, and kanamycin, as group 0 mg/L, group 30 mg/L, group 91mg/L, and group 910 mg/L for each drugs. The maximum platelet aggregation rate induced by adenosine diphosphate, expression levels of CD62p and FIB-R, prothrombin time, activated partial thromboplastin time, thrombin time, and fibrinogen were measured. The sodium citrate and sodium heparin were used in whole blood tests for the whole blood coagulation time as well as the Ca2+ in blood plasma. Results: Amikacin and gentamicin could inhibit the aggregation of platelets, which contributed to the whole blood clotting disorder. Conclusion: Amikacin and gentamicin might inhibit the platelet aggregation by blocking the activation and release of FIB-R or probably the inhibition of endogenous clotting factor as well. This effect was not dependent on calcium ions.
Introduction
Disrupted hemorrhage is caused by the imbalance of coagulation and anticoagulation system. 1–2 It was showed that glycoside drug amikacin could affect the hemorrhage processes. 3–4 However, the potential anticoagulation effects of other aminoglycoside antibiotics on platelet aggregation were not known. In the present study, fresh whole blood was collected from healthy donors and tested the effects of gentamicin, streptomycin, etimicin, amikacin, and kanamycin on platelet aggregation and blood coagulation. The potential underlying mechanisms were discussed as well.
Materials and Methods
Participants
Twenty healthy volunteers (10 males and 10 females; aged 20-25) were recruited for present study (from March 01, 2009 to May 10, 2009). The fresh vein blood samples were collected in the morning with overnight starving with routine procedures. The study was approved by the local ethics committee on the use of clinical human samples for research of the hospital and has the informed written consent of all participants.
Instruments and Reagents
SYSMEX XE-2100 blood cell analyzer (Ji’Ao, Shanghai, China), SYSMEX CA-7000 Coagulation Analyzer (SYSMEX, Shanghai), Model Beckman-Coulter LX20 automatic biochemical analyzer (Ji’Ao), Saikexide platelet aggregation SC-2000 analyzer (Beijing, China), Beckman-Coulter EPICS-based flow cytometry (Beckman-Coulter, Shanghai, China), horizontal centrifuge (Ji'Ao). The reagents used in the study included etimicin sulfate, streptomycin, amikacin (0.1 g/mL, size 2 mL, batch 8040351FA), and gentamicin injections were from Renmin Hospital, Hangzhou, platelet aggregation inducer ADP (Huadong Medicine Company, Hangzhou, China), mouse anti-human CD62p-FITCF monoclonal antibody (Immunotech Company, Beckman Coulter), PAC-1-FITC monoclonal antibody (Immunotech Company, Beckman Coulter), hemagglutination reagent (Dehring company, Dade Dehring Inc, USA), heparin sodium injection (6250 IU/mL, size 2 mL, approved no 080901), and sodium citrate (self-made).
The Preparation of Platelet-Rich Plasma
After the samples were collected in a tube containing citrate disodium as the anticoagulant, the fresh whole blood was subjected to 200g centrifugation (radius 26 cm) at room temperature for 10 minutes. The supernatant was the platelet-rich plasma (PRP), which was adjusted with platelet-poor plasma (PPP) to reach the final concentration of platelet at 200 × 10 9 /L to examine the activation marker of platelets and the aggregation rate. The rest of the PPP was used for blood coagulation test.
Groups and Sample Treatments
The groups for each drug included 0 mg/L (control group), 30 mg/L, 91 mg/L, and 910 mg/L group, respectively; the PPP/PRP was mixed with saline or drugs gently and left at room temperature for 20 minutes, prior to all tests.
Platelet Aggregation and Coagulation Test
The platelet aggregation analyzer was preheated to 37°C. Adenosine triphosphate (30 μL) was added into 300 μL PRP to reach the final concentration of 5 μmol/L. We have repeated the experiment eight times in order to record the rate of aggregation and inhibition in the drug-treated groups. Aminoglycoside inhibition of aggregation rate percentage = (saline control group rate of platelet aggregation − the maximum platelet aggregation rate of the drug group)/saline control group victory platelet aggregation × 100%. For the coagulation test of PPP, prothrombin time (PT), activated partial thromboplastin time (APTT), thrombin time (TT), and fibrinogen (FIB) levels were measured with coagulation analyzer and were repeated for 8 times.
Platelet P-Selectin, GPIIb/IIIa, and FIB-R
The PRP with ADP activation was mixed with Tris-EDTA-Nacl(TEN) buffer (1:3, v/v), then fixed with 2% paraformaldehyde at room temperature. Then mouse anti-human CD62-FITC (P-selectin), CD41-PE, and CD61-FITC (FIB-R) were added and the solution was subjected to flow cytometry for positive rate counting out of 10 000 platelets. The aminoglycoside inhibition of aggregation rate was calculated as above and repeated for 8 times.
Clotting Time of the Whole Blood and Plasma Ca2+
Fresh blood (1.8 mL) was mixed with 0.2 mL saline, sodium heparin, sodium citrate, and different concentrations of aminoglycosides for clotting time (CT) examination (in seconds, repeated for 8 times). Another same preparation was incubated at 37°C for 30 minutes, then 1500g centrifugation for 5 minutes in prior to the blood gas analyzer for plasma Ca2+ (repeated for 8 times).
Statistics
The results were expressed as mean (standard deviation). The statistical analyses were done with SPSS12.0 software, with single factor analysis of variance to determine the differences in drug effects, q test for comparisons between groups, and chi square test for comparisons of percentages. P < .05 was considered statistically significant.
Results
The Effects of Different Aminoglycoside Antibiotics (30mg/L) on Platelet Aggregation and Coagulation
The effects of different aminoglycoside antibiotics (30 mg/L) on platelet aggregation and coagulation are shown in Table 1 . The platelet aggregation in saline control group was 86.2% ± 8.9%; the maximum platelet aggregation rate and aggregation inhibition rate in amikacin group were 71.5% ± 7.7% and 16.51%, with significant differences from saline group (P < .01); in gentamicin group, the rates were 70.2% ± 10.2% and 15.46%, respectively, with significant differences from saline group (P < .01). The APTT in Amikacin group (51.9 ± 4.2) and gentamicin group (53.7 ± 4.6) were significantly higher than saline control group, with significant differences (P < .001; Table 1).
Effect of Aminoglycoside Antibiotics on Platelet Aggregation and Blood Coagulation
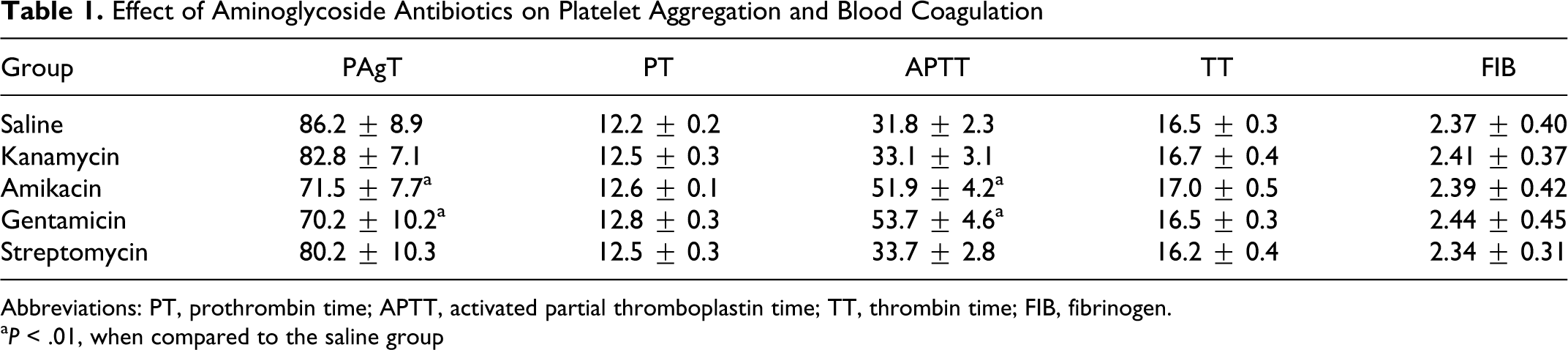
Abbreviations: PT, prothrombin time; APTT, activated partial thromboplastin time; TT, thrombin time; FIB, fibrinogen.
a P < .01, when compared to the saline group
Different Concentrations of Amikacin on Platelet Aggregation and Coagulation
In the amikacin groups with different concentrations, 30 mg/L group showed significantly lower platelet aggregation rate (P < .01 compared to saline group), which showed further decrease in higher concentration group: 910 mg/L group showed no coagulation of plasma, with APTT longer than 240 seconds (P < .001 compared to saline group). There were no changes in PT, TT, and FIB (P > .05; Table 2 ).
Different Concentrations of Amikacin on Platelet Aggregation and Coagulation
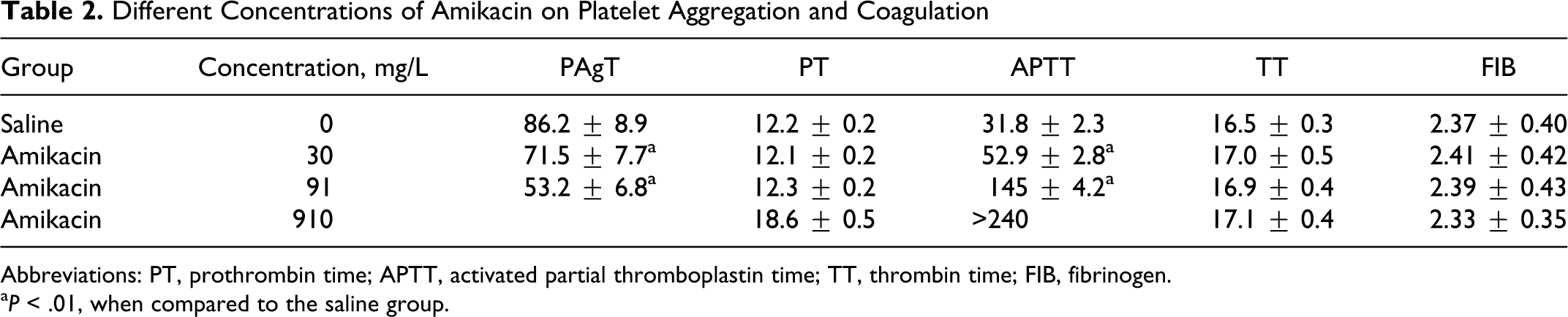
Abbreviations: PT, prothrombin time; APTT, activated partial thromboplastin time; TT, thrombin time; FIB, fibrinogen.
a P < .01, when compared to the saline group.
Different Concentrations of Gentamicin Platelet Aggregation and Coagulation
The results were similar to amikacin. The 30 mg/L group showed significantly lower platelet aggregation rate (P < .01 compared to saline group), which showed further decrease in higher concentration group: 910 mg/L group showed no coagulation of plasma, with APTT longer than 240 seconds (P < .001 compared to saline group). There were no changes in PT, TT, and FIB (P > .05; Table 3 ).
Different Concentrations of Gentamicin Platelet Aggregation and Coagulation
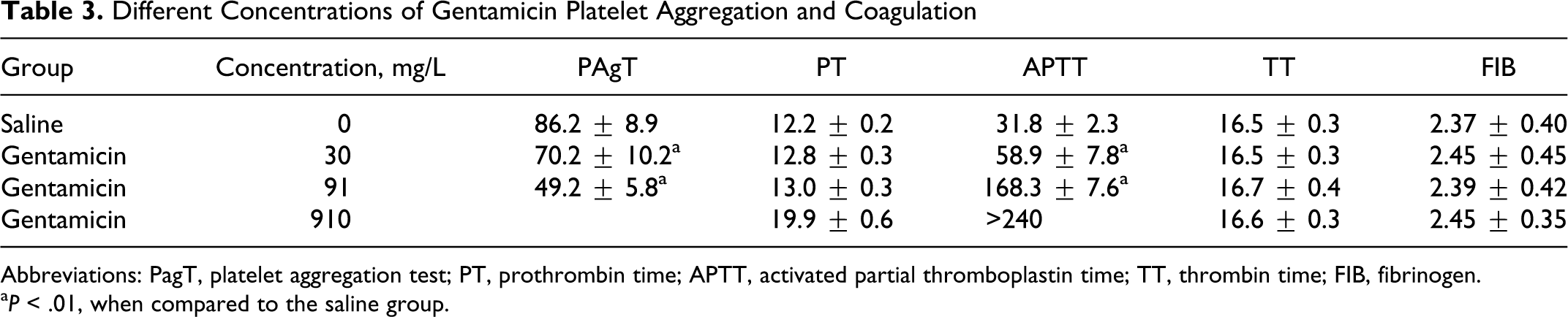
Abbreviations: PagT, platelet aggregation test; PT, prothrombin time; APTT, activated partial thromboplastin time; TT, thrombin time; FIB, fibrinogen.
a P < .01, when compared to the saline group.
The Effects of Aminoglycosides on FIB-R Expression and P-Selectin on Platelets
The different groups of amikacin and gentamicin showed FIB-R (g/L) inhibition and CD62p expression (percentage) in a dose-dependent manner (Table 4 ). On the other hand, there were no significant changes in the plasma Ca2+ (mmol/L).
The Effects of Aminoglycosides on Expression of FIB-R and P-Selectin on Platelets
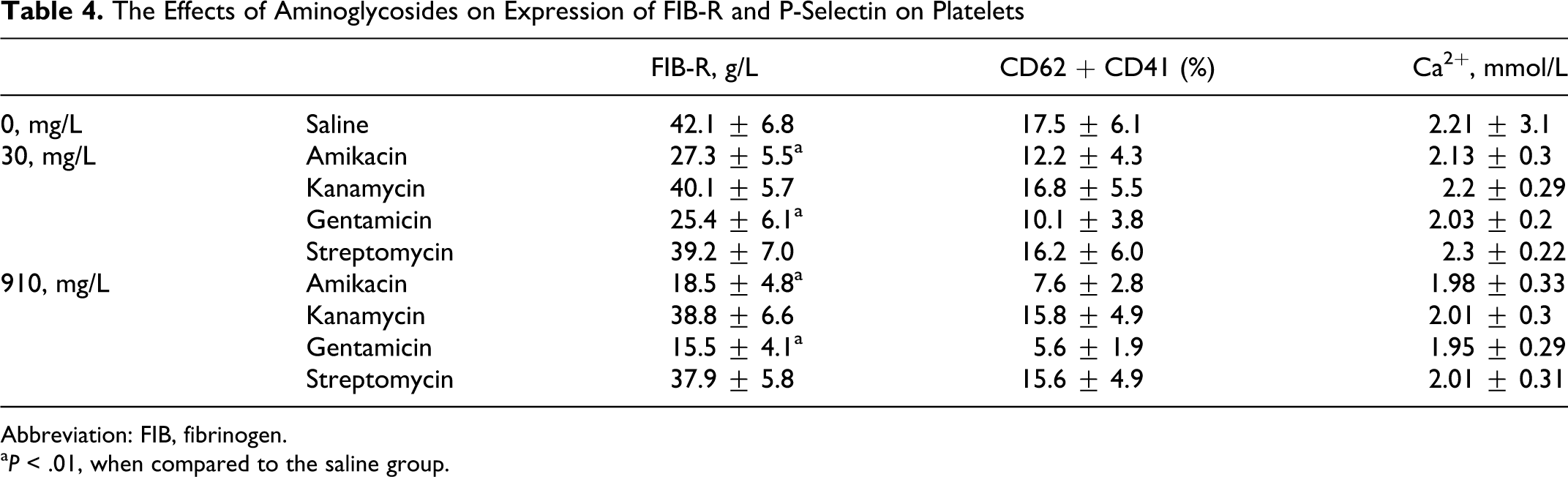
Abbreviation: FIB, fibrinogen.
a P < .01, when compared to the saline group.
Discussion
The increasing incidences of bleeding and thrombotic diseases to a large extent were caused by improper uses of drugs. The drugs exert their effects on platelets, the major player in the hemostasis. The inhibition of platelet functions leads to bleeding disease, while overactivation of platelets contributes to the thrombotic diseases. 5–6 Adenosine diphosphate could bind to the membrane receptors of platelet and activate the long G protein signal transduction pathway to trigger the platelet aggregation and release. 7–11 In the present study, amikacin and gentamicin treatments inhibited the effects of ADP-induced platelet aggregation in a dose-dependent manner. The aminoglycoside antibiotics could be divided into those produced from streptomyces, including streptomycin, neomycin, paromomycin, levy vancomycin, kanamycin, tobramycin, and amikacin (semisynthetic), and those produced from micromonospora strain, such as gentamicin, sisomicin, netilmicin (semisynthetic), and etimicin (semisynthetic). These drugs showed very similar chemical structures.
Prothrombin time, APTT, TT, and FIB represent the functional integrity of the second phase during blood coagulation. 12–16 The study showed that amikacin and gentamicin could cause prolonged APTT in a dose-dependent manner, without affecting other indicators; these suggested that amikacin and gentamicin inhibit blood coagulation through suppression of endogenous coagulation factors. The GPIIb/IIIa is the major platelet glycoprotein; its structure changes expose the FIB-R, leading to the binding of FIB and finally the platelet aggregation. The experiment showed that amikacin and gentamicin inhibit the FIB-R activation, thereby stopped the platelet aggregation. Additionally, CT values were significantly longer in amikacin and gentamicin groups. Last but not least, we found that the plasma Ca2+ is not involved in this process. In conclusion, the present study proved that amikacin and gentamicin could inhibit platelet activation and FIB-R release, therefore FIB increases the platelet aggregation. The process is Ca2+ independent.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.