
Abstract
Fibrinogen and fibrin formation have a key role in perioperative hemostasis. The aim of this study is to examine the association of postoperative hemostasis with a combined evaluation of the fibrinogen level and fibrin polymerization in cardiac surgery. We retrospectively classified 215 consecutive cardiac surgery patients into 4 groups (Fuji-san classification) that were divided by fibrinogen level <150 mg/dL (ie, hypofibrinogenemia) and fibrinogen thromboelastometry value at 10 minutes with rotational thromboelastometry <6 mm (ie, low fibrin polymerization) at the warming of cardiopulmonary bypass. Four groups resulted; group I, the acceptable range (n = 85); group II, only hypofibrinogenemia (<150 mg/dL, ≥6 mm, n = 63); group III, hypofibrinogenemia and low fibrin polymerization (<150 mg/dL, <6 mm, n = 60); and group IV, only low fibrin polymerization (≥150 mg/dL, <6 mm, n = 7). The risk of chest tube drainage volume greater than 500 mL within the first 24 hours after surgery (with group I as the reference) was increased in group II (odds ratio [OR], 3.3; 95% confidence interval [CI], 1.5-7.4; P < .01) and group III (OR, 8.5; 95% CI, 3.5-21.7; P < .01), and the risk greater than 1000 mL (with group I as the reference) was increased in group III (OR, 4.0; 95% CI, 1.1-17.3; P = .03) and group IV (OR, 23.1; 95% CI, 3.2-201.0; P < .01). Intraoperative blood transfusions were decreased by 24.5%, after stratifying the starting amount of fresh frozen plasma by the 4-group classification in the recent consecutive 65 (30.2%) patients (P < .01). The 4-group classification is associated with postoperative bleeding and may improve the quality of perioperative blood transfusion in cardiac surgery.
Introduction
A blood clot, which is formed by platelet aggregation and a fibrin network, is essential for perioperative hemostasis. Thrombocytopenia, dilutional or consumptive coagulopathy, or hyperfibrinolysis causes difficulty in hemostasis or causes abnormal bleeding in patients undergoing cardiovascular surgery. 1,2 Blood transfusion independently contributes to postoperative mortality and morbidity. 3 Recent studies indicate that fibrinogen replacement therapy offers effective hemostasis and reduces transfusion requirements in patients with bleeding. 4 –6
The fibrinogen level is the traditional indicator for therapeutic targets in fibrinogen replacement. 7,8 Rotational thromboelastometry (ROTEM) quickly estimates the quality of fibrin polymerization in whole blood and distinguishes hypofibrinogenemia from thrombocytopenia; therefore, as a point-of-care monitor, it can be used to indicate the necessity for fibrinogen replacement or platelet transfusion. 9 The combined assessment of the fibrinogen level and fibrin polymerization may offer additional information for perioperative hemostasis and blood transfusion strategy. Few studies have reported on the association between postoperative bleeding outcome and the combined evaluation of fibrinogen levels and fibrin polymerization.
The aim of this retrospective study was to examine the association between postoperative bleeding outcome and a 4-group classification that was divided by a fibrinogen level less than 150 mg/dL (ie, hypofibrinogenemia) and fibrinogen thromboelastometry value at 10 minutes (FIBTEM A10) with a ROTEM value less than 6 mm (ie, low fibrin polymerization) during cardiopulmonary bypass in cardiac surgery.
Methods
Study Participants
The institutional review board at the Committee of Ethics in the Hamamatsu Rosai Hospital (Hamamatsu, Japan) approved this study. We retrospectively investigated a cohort of 215 consecutive patients (130 [60.4%] male patients older than 20 years) who underwent cardiac surgery that required cardiopulmonary bypass between October 1, 2010, and May 31, 2014. Patients who underwent cardiovascular operations that involved aortic surgery were excluded. All patients provided written informed consent for medical care and procedures in the clinic and hospital. Preoperative anticoagulants and antiplatelet agents were routinely stopped 7 to 10 days before surgery and were exchanged for the continuous administration of heparin.
Patient Management
In all patients, general anesthesia was achieved using sevoflurane (1%-2%) supplemented with fentanyl, remifentanil, and muscle relaxants under tracheal intubation. Radial arterial catheterization was performed in advance of the operation. A central venous catheter and pulmonary artery catheter were placed into the right internal jugular vein. A gastric tube was also inserted. Transesophageal echocardiography was monitored.
The patients underwent cardiac surgery with or without aortic clamping under mild hypothermia during cardiopulmonary bypass (the nadir of the bladder temperature was 32°C-35°C). Before cardiopulmonary bypass, all patients received an initial dose of heparin at 300 to 400 units/kg, which was followed by additional doses of heparin to maintain a celite-activated clotting time greater than 400 seconds (measured by the Hemochron system; International Technidyne Corporation, Edison, New Jersey). A centrifugal pump cardiopulmonary bypass circuit was routinely used. Oxygenated warm blood cardioplegia was used for myocardial protection.
At the conclusion of the cardiopulmonary bypass, protamine was administered for heparin neutralization (at a ratio of 10-13 mg of protamine for 1000 units of heparin). If the activated clotting time remained above the baseline value, an additional 30 to 50 mg of protamine was administered. After terminating cardiopulmonary bypass, the contents of the oxygenator were returned to the patient. A cell salvage device (Cell Saver 5; Haemonetics Corp, Braintree, Massachusetts) was used in all patients. Red blood cell concentrates were transfused if the patient’s hematocrit was less than 20% during cardiopulmonary bypass or were transfused if the patient’s hematocrit was less than 23% after surgery. Filling pressures were maintained by an appropriate plasma expander if the patient’s hematocrit was above this critical threshold. Platelet concentrates were transfused if the patient’s platelet level was less than 50 × 103/μL after surgery. These guidelines did not preclude the transfusion of red blood cell concentrates, platelet concentrates, or other blood products if the patient’s condition required it in the opinion of the clinician.
After the operation, all patients were moved to the intensive care unit and managed carefully while on mechanical ventilation and sedation until subsequent extubation. The perioperative use of cardiotonic and vasoactive agents, tranexamic acid for antifibrinolytic therapy, and blood transfusions were administered at the discretion of the attending anesthesiologists and cardiac surgeons.
Blood Tests
The patients’ blood underwent routine laboratory examination in the present study. We used the Clauss method for the fibrinogen level and ROTEM (Tem International GmbH, Munich, Germany) for the FIBTEM test and extrinsic thromboelastometry (EXTEM) test. The FIBTEM test is used to estimate the quality of fibrin polymerization using extrinsic activation with human recombinant tissue factor and the powerful platelet inhibitor cytochalasin D; therefore, only a fibrin clot is formed and measured. The EXTEM test uses human recombinant tissue factor and phospholipids for mild extrinsic activation of the coagulation system. The values of the FIBTEM and EXTEM tests were measured after 10 minutes—defined as FIBTEM (A10) and EXTEM (A10), respectively—and were used for the analyses.
Four-Group Classification
We examined the linear correlation between the fibrinogen level and FIBTEM (A10) value at the warming of cardiopulmonary bypass in 215 patients. We classified the patients into 4 groups, which were divided by a fibrinogen level less than 150 mg/dL (ie, hypofibrinogenemia) and a FIBTEM (A10) value less than 6 mm (ie, low fibrin polymerization). In Hamamatsu Rosai Hospital, we chose the fibrinogen level of 150 mg/dL as the boundary because it is the lower limit of the acceptable range (150-450 mg/dL), and we chose the FIBTEM (A10) value of 6 mm as the boundary because it is the lower limit of the acceptable range (6-23 mm). The 4 groups consisted of group I (a fibrinogen level ≥150 mg/dL and FIBTEM [A10] ≥6 mm), group II (ie, only hypofibrinogenemia; a fibrinogen level <150 mg/dL and FIBTEM [A10] ≥6 mm), group III (ie, hypofibrinogenemia and low fibrin polymerization; a fibrinogen level <150 mg/dL and FIBTEM [A10] <6 mm), and group IV (ie, only low fibrin polymerization; a fibrinogen level ≥150 mg/dL and FIBTEM [A10] <6 mm). We have used this 4-group classification (also called the Fuji-san classification) as the routine laboratory examination for guiding the transfusion of fresh frozen plasma in cardiovascular surgery in the hospital.
Postoperative Outcome
Postoperative bleeding was defined as the total volume of chest tube drainage after sternal closure and during the first 24 hours after surgery or until the patients were reexplored because of bleeding. We compared the chest tube drainage volume within the first 24 hours after surgery and perioperative blood transfusions (ie, intraoperative and within the first 24 hours after surgery) among the patients who were classified into the 4 groups.
Stratification for Plasma Transfusion
Based on the 4-group classification used in this study, we determined the starting amount of fresh frozen plasma in 65 (30.2%) of the 215 consecutive patients treated from January 31, 2013, to the end of the study, as follows: group I, 0 mL; group II, 0 to 480 mL; group III, 480 mL or greater; and group IV, 720 mL or greater. We prospectively compared the perioperative transfusions of blood products before and after these stratifications.
Statistical Analysis
All statistical analyses were performed with JMP 10.0.2 software (SAS Institute, Inc, Cary, North Carolina). Continuous variables were expressed as the mean ± the standard deviation, and categorical variables were expressed as percentages. A linear regression analysis was performed to analyze the correlation between the fibrinogen level and the FIBTEM (A10) value and the correlation between the chest tube drainage volume and fibrinogen level or FIBTEM (A10) value. For continuous variables, generalized linear model (normal as a probability distribution, logarithm as a link function) was used with likelihood ratio chi-square test and the Tukey-Kramer honestly significant difference test was performed for multiple comparison among patients who were classified into the 4 groups. For categorical variables, the Pearson chi-square test was performed among the 4 groups. Multivariate logistic regression analysis was performed to estimate the risk of chest tube drainage volume of greater than 500 or 1000 mL within the first 24 hours after surgery among the patients of the 4-group classification, after adjusting for the preoperative hemoglobin level and platelets count, body mass index, and cardiopulmonary bypass time. A value of P <.05 (2 tailed) was statistically significant.
Results
Four-Group Classification
There was a linear correlation between the fibrinogen level and FIBTEM (A10) value at the warming of cardiopulmonary bypass among the 215 patients (r 2 = .61, P < .0001; Figure 1A). The patients were classified into 4 groups: group I (n = 85; 39.5%); group II, only hypofibrinogenemia (n = 63; 29.3%); group III, hypofibrinogenemia and low fibrin polymerization (n = 60; 27.9%); and group IV, only low fibrin polymerization (n = 7; 3.3%; Figure 1A). The patient characteristics based on the 4-group classifications are summarized in Table 1 (ie, preoperative characteristics) and in Table 2 (ie, intraoperative and postoperative characteristics).
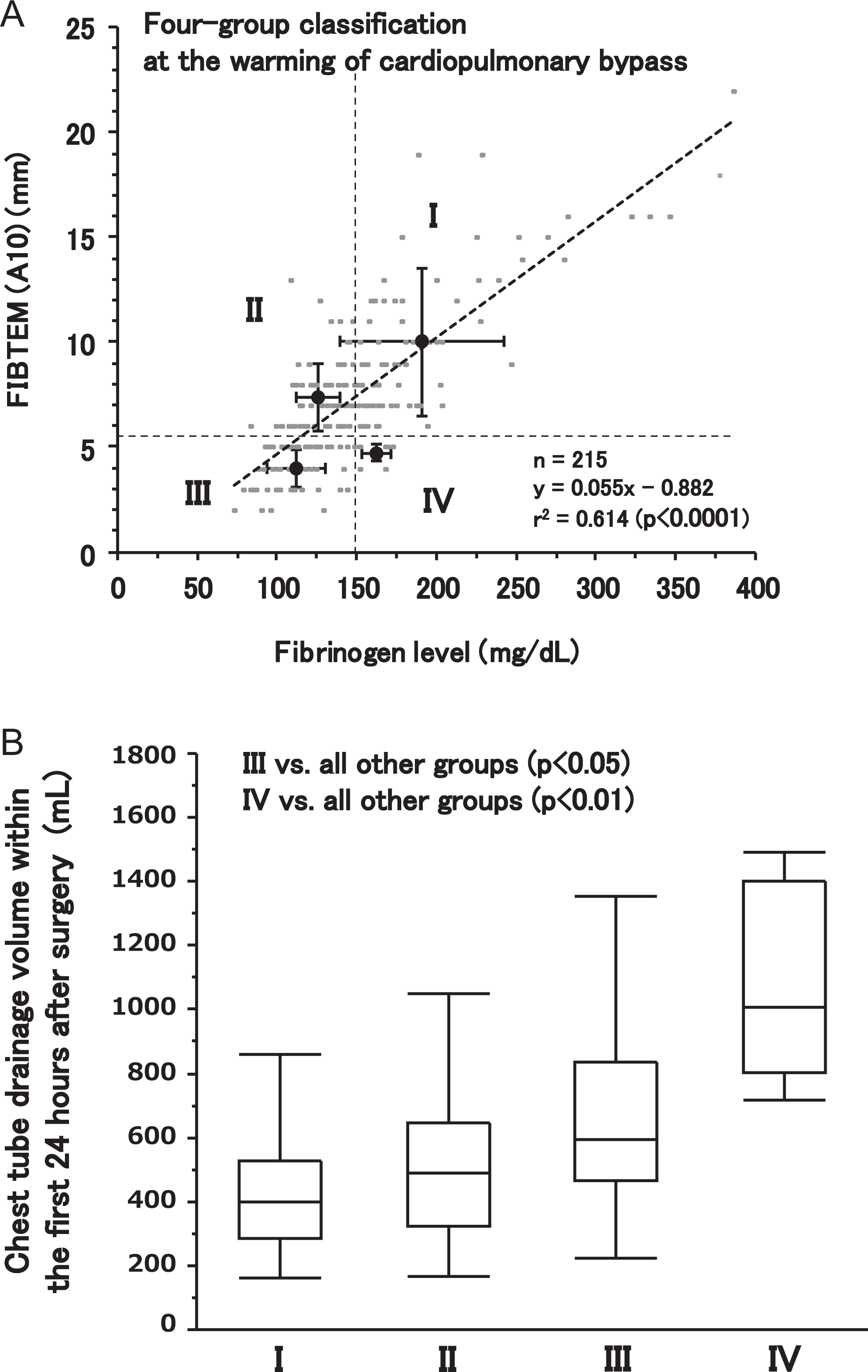
The 4-group classification and the chest tube drainage within the first 24 hours after surgery. A, The 4-group classification, divided by the fibrinogen level and FIBTEM (A10) value. In the linear correlation between fibrinogen level and FIBTEM (A10) value during cardiopulmonary bypass, the 4 groups are divided by a fibrinogen level of less than 150 mg/dL (ie, hypofibrinogenemia) and a FIBTEM (A10) value less than 6 mm (ie, low fibrin polymerization). B, Box plots of the chest tube drainage volume in the 4-group classification. The chest tube drainage within the first 24 hours after surgery is less in group I and group II than in group III (P < .05, vs all other groups) and group IV (which has the highest volume; P < .01, vs all other groups). FIBTEM (A10) indicates fibrinogen thromboelastometry value at 10 minutes.
Preoperative Characteristics of the Patients in the 4-Group Classification.
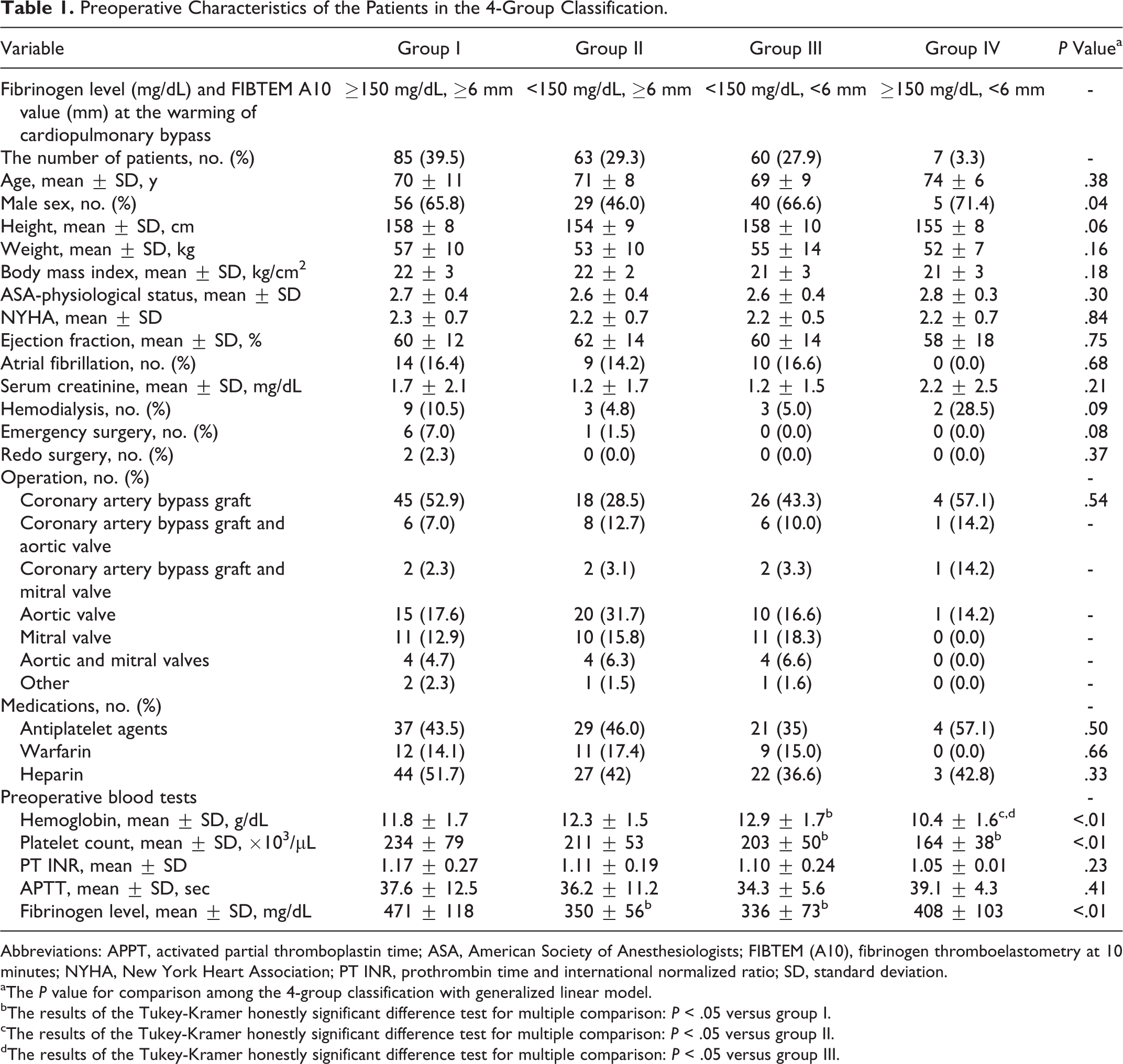
Abbreviations: APPT, activated partial thromboplastin time; ASA, American Society of Anesthesiologists; FIBTEM (A10), fibrinogen thromboelastometry at 10 minutes; NYHA, New York Heart Association; PT INR, prothrombin time and international normalized ratio; SD, standard deviation.
aThe P value for comparison among the 4-group classification with generalized linear model.
bThe results of the Tukey-Kramer honestly significant difference test for multiple comparison: P < .05 versus group I.
cThe results of the Tukey-Kramer honestly significant difference test for multiple comparison: P < .05 versus group II.
dThe results of the Tukey-Kramer honestly significant difference test for multiple comparison: P < .05 versus group III.
Intraoperative and Postoperative Characteristics of the Patients in the 4-Group Classification.
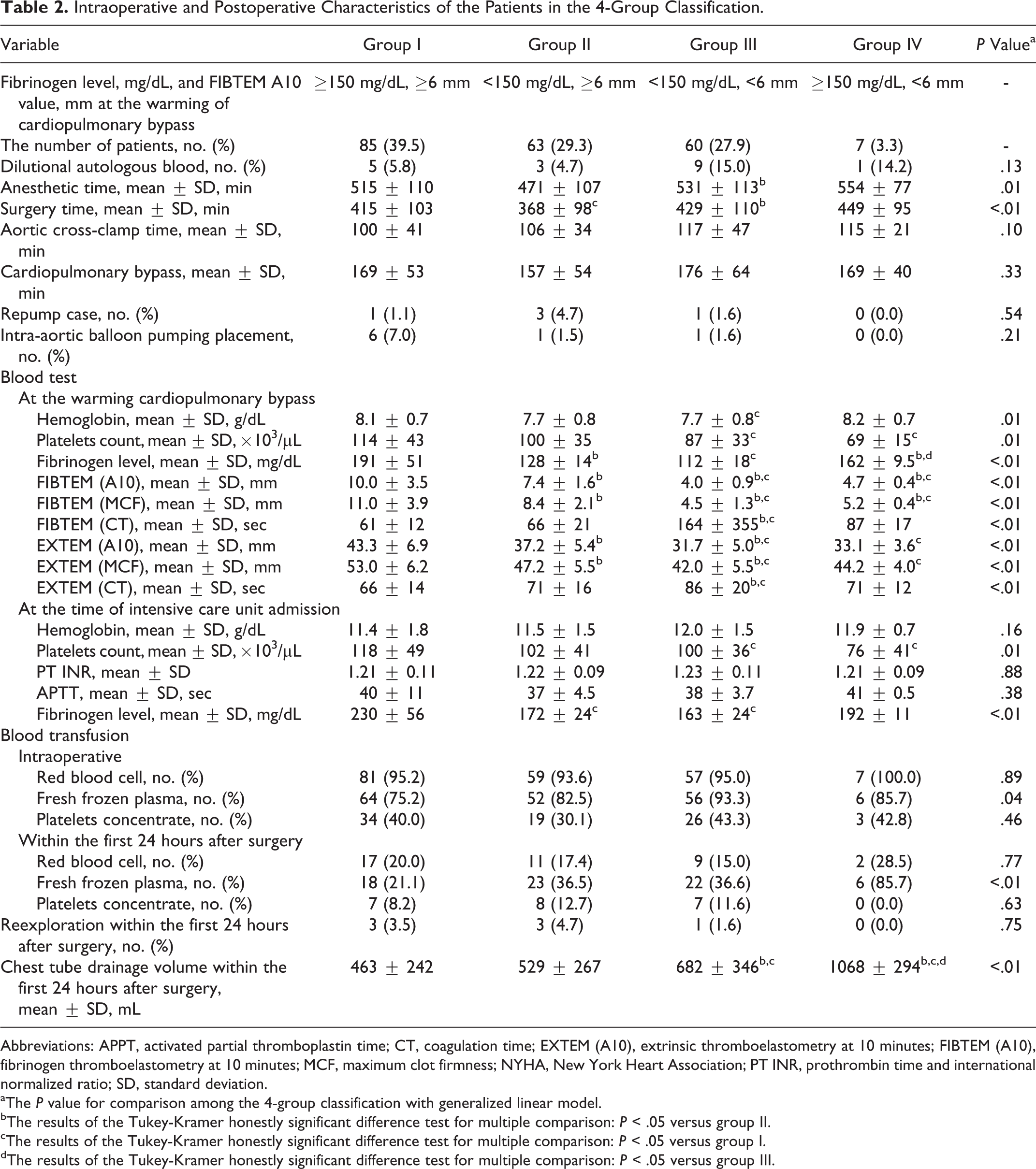
Abbreviations: APPT, activated partial thromboplastin time; CT, coagulation time; EXTEM (A10), extrinsic thromboelastometry at 10 minutes; FIBTEM (A10), fibrinogen thromboelastometry at 10 minutes; MCF, maximum clot firmness; NYHA, New York Heart Association; PT INR, prothrombin time and international normalized ratio; SD, standard deviation.
aThe P value for comparison among the 4-group classification with generalized linear model.
bThe results of the Tukey-Kramer honestly significant difference test for multiple comparison: P < .05 versus group II.
cThe results of the Tukey-Kramer honestly significant difference test for multiple comparison: P < .05 versus group I.
dThe results of the Tukey-Kramer honestly significant difference test for multiple comparison: P < .05 versus group III.
Postoperative Outcome
The chest tube drainage within the first 24 hours after surgery in group I (463 ± 242 mL) and in group II (529 ± 267 mL) was less than the volume in group III (682 ± 346 mL, P < .05, vs all other groups) and group IV (which was the greatest at 1068 ± 294 mL; P < .01, vs all other groups; Figure 1B). The cardiopulmonary bypass time was longer in patients with a postoperative drainage volume greater than the third quartile in group I (205 ± 58 vs 159 ± 47 minutes, P < .01) and group II (188 ± 61 vs 148 ± 48 minutes, P = .01). This did not occur in group III (174 ± 44 vs 177 ± 70 minutes, P = .89). However, patients in group III with a postoperative drainage volume greater than the third quartile were more likely to have received preoperative warfarin (P = .02) and hemodialysis (P = .01).
Multivariate logistic regression analysis after adjustment showed that the risk of chest tube drainage of greater than 500 mL within the first 24 hours after surgery (using group I as the reference) was increased in group II (adjusted odds ratio [AOR], 3.3; 95% confidence interval [CI], 1.5-7.4; P < .01) and group III (AOR, 8.5; 95% CI, 3.5-21.7; P < .01) with an area under the curve of 0.79. The risk of postoperative chest tube drainage greater than 1000 mL (using group I as the reference) was increased in group III (AOR, 4.0; 95% CI, 1.1-17.3; P = .03) and group IV (AOR, 23.1; 95% CI, 3.2-201.0; P < .01) with an area under the curve of 0.78.
Intraoperative and postoperative requirements of fresh frozen plasma was increased (listed in increasing order) in groups I, II, III, and IV (P < .05), and perioperative transfusion of fresh frozen plasma was increased in group I (545 ± 46 mL), group II (716 ± 54 mL), group III (807 ± 55 mL; P < .01, vs group I), and group IV (1200 ± 162 mL; P < .05, vs groups I and II).
Fibrinogen Level or FIBTEM (A10) Alone
We observed that 92.8% of all patients who had a fibrinogen level less than 300 mg/dL before cardiopulmonary bypass were classified in group II, III, or IV at the warming of cardiopulmonary bypass (P < .01). Postoperative chest tube drainage was greater in patients with a fibrinogen level less than 150 mg/dL (604 ± 316 vs 510 ± 294 mL, P = .03) and with FIBTEM (A10) less than 6 mm (723 ± 359 vs 491 ± 254 mL, P < .01) during cardiopulmonary bypass. The perioperative requirement for fresh frozen plasma was greater in patients with a fibrinogen level less than 150 mg/dL (92.6% vs 81.5%, P = .01) and with FIBTEM (A10) less than 6 mm (95.5% vs 84.4%, P = .02) during cardiopulmonary bypass.
Figure 2 shows the relationship between the fibrinogen level or FIBTEM (A10) value during cardiopulmonary bypass and the postoperative chest tube drainage in all patients, based on the 4-group classification. The fibrinogen level was similar between groups I and IV (P = .14) or between groups II and III (P = .06; Figure 2A). The FIBTEM (A10) value was similar between groups III and IV (P = .91; Figure 2B).
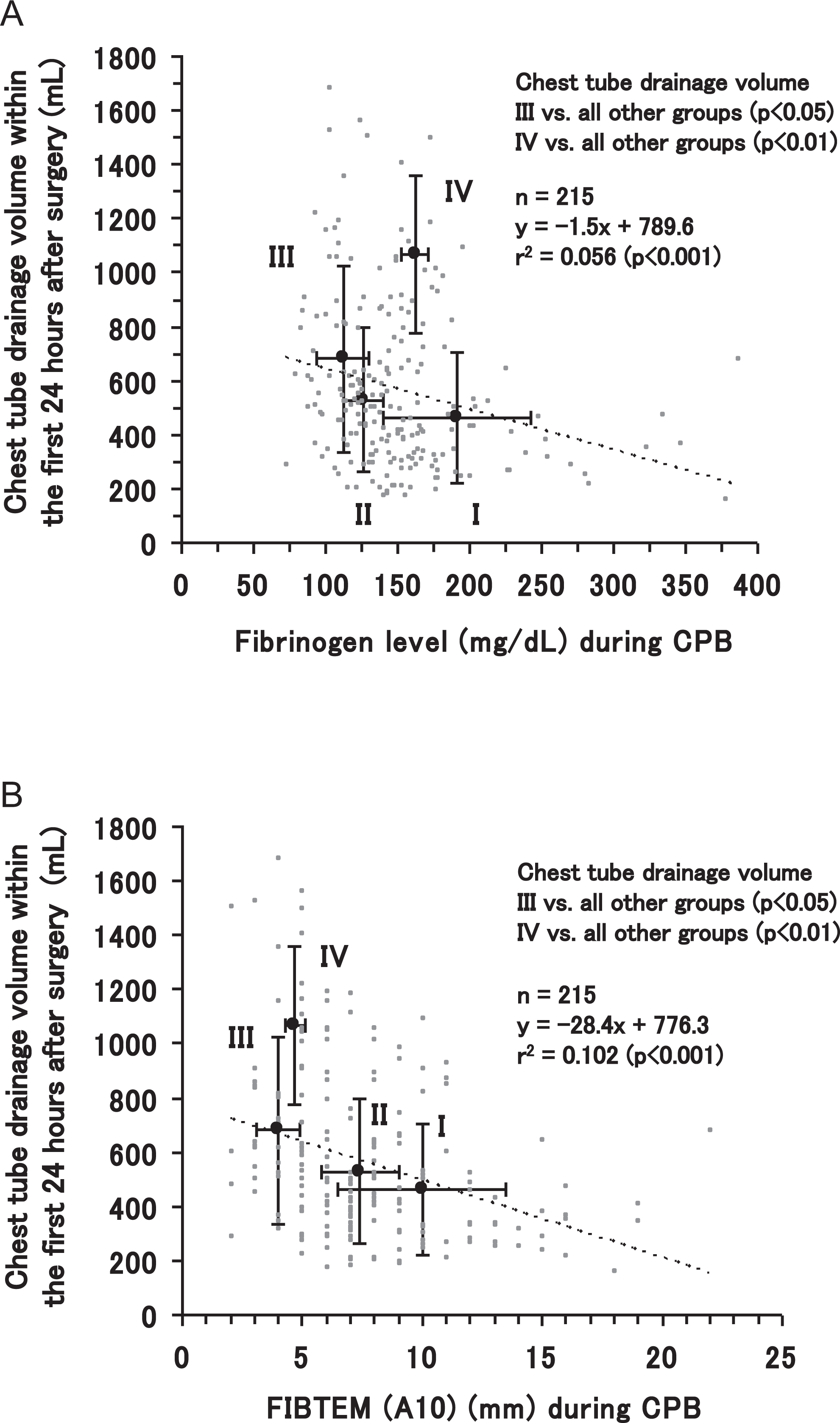
The relationship between the fibrinogen level or FIBTEM (A10) and the chest tube drainage volume. A, The relationship between the fibrinogen level and the chest tube drainage volume. In the relationship between the fibrinogen level and chest tube drainage within the first 24 hours after surgery, the fibrinogen level is similar between groups I and IV (P = .14) or between groups II and III (P = .06) in the 4-group classification. B, The relationship between the FIBTEM (A10) value and the chest tube drainage volume. In the relationship between the FIBTEM (A10) value and the chest tube drainage within the first 24 hours after surgery, the FIBTEM (A10) value is similar between groups III and IV (P = .91) in the 4-group classification. CPB indicates cardiopulmonary bypass; FIBTEM (A10), fibrinogen thromboelastometry value at 10 minutes.
Stratification for Plasma Transfusion
After we applied the 4-group classification to stratify the starting amount of fresh frozen plasma, we observed the reduction in the intraoperative transfusion of red blood cell concentrates (1264 ± 787 vs 1616 ± 603 mL, P < .01), fresh frozen plasma (450 ± 348 vs 587 ± 346 mL, P < .01), platelet concentrates (81 ± 150 vs 175 ± 207 mL, P < .01), and all blood products by 24.5% (1795 ± 1121 vs 2380 ± 915 mL, P < .01).
Discussion
The 4-group classification, based on a fibrinogen level less than 150 mg/dL (ie, hypofibrinogenemia) and FIBTEM (A10) value less than 6 mm (ie, low fibrin polymerization) during cardiopulmonary bypass in cardiac surgery, is associated with the postoperative chest tube drainage volume, which is increased (listed in increasing order) in group I (ie, fibrinogen level of ≥150 mg/dL and FIBTEM [A10] value of ≥6 mm), group II (ie, only hypofibrinogenemia), group III (ie, hypofibrinogenemia and low fibrin polymerization), and group IV (ie, only low fibrin polymerization). After we stratified the transfusion volume of fresh frozen plasma according to the 4-group classification, we observed a reduction in the total amount of perioperative blood transfusion.
Fibrinogen Level
Restoring the fibrinogen level may be a priority for effective hemostasis in perioperative bleeding. The recent European guidelines recommend fibrinogen target levels of 150 to 200 mg/dL for hemostasis in perioperative bleeding, which is higher than the level of 80 to100 mg/dL that was recommended before 2009. 10 In the present study, patients who had a fibrinogen level less than 150 mg/dL during cardiopulmonary bypass had greater postoperative bleeding and perioperative transfusion of fresh frozen plasma. Fibrinogen levels of greater than 180 mg/dL were required for stable hemostasis after surgery. These observations indicate the importance of normalizing the fibrinogen level for perioperative hemostasis.
Fibrin Polymerization
Rotational thromboelastometry quickly distinguishes hypofibrinogenemia from thrombocytopenia, and it sensitively reflects the need for fibrinogen replacement in bleeding. In addition, analysis using thromboelastometry reduces the perioperative costs of blood and coagulation products by the early detection of a coagulation disorder in cardiac surgery. 11 The application of a ROTEM-guided transfusion strategy may reduce the amount of bleeding in patients with severe bleeding. 12 In the present study, patients who had FIBTEM (A10) values less than 6 mm during cardiopulmonary bypass had 1.4-fold postoperative bleeding and greater number of perioperative transfusions of fresh frozen plasma. These observations indicate a close association between a disturbance in fibrin polymerization and perioperative bleeding.
Four-Group Classification
To our knowledge, previous studies have not examined the 4-group classification as an indicator of perioperative bleeding and blood transfusions. The fibrinogen level itself may have a limited ability to distinguish between patients who have different postoperative bleeding outcomes. This is presumably because the fibrinogen level does not directly reflect the strength of the fibrin polymer that forms the mesh of branched fibers in blood clots and has unique structural and mechanical properties of clots at the network, fiber, and molecular levels. 13 In the present study, the patients in group IV had impaired fibrin polymerization in spite of a fibrinogen level of 150 mg/dL or greater. This finding was presumably because of a vulnerable fibrin network and hyperfibrinolytic state. To reduce postoperative bleeding, more effective fibrinogen replacement by a fibrinogen concentrate or cryoprecipitate may be preferable in patients who have deteriorated fibrin polymerization, despite a reasonable fibrinogen level. 4
Timing of Assessment
Assessing coagulation during cardiopulmonary bypass may allow early estimation of hemostatic impairment after the bypass procedure. A previous study showed similar fibrinogen level measurements shortly before weaning from cardiopulmonary bypass and after the bypass. 14 A preoperative fibrinogen level less than 250 mg/dL is independently associated with increased postoperative bleeding. 15 We observed that 90% of the patients who had a fibrinogen level less than 300 mg/dL before cardiopulmonary bypass had hypofibrinogenemia and/or low fibrin polymerization during the bypass. The recent dry-hematology (DRIHEMATO) method is currently available for an accurate and rapid determination of fibrinogen level in the whole blood. 16 Early evaluation of the fibrinogen level and fibrin polymerization may be helpful to identify patients who are at risk of postoperative bleeding.
Stratification for Transfusion
The transfusion algorithms with a point-of-care coagulation test reduce transfusion requirements and blood loss in cardiac surgery. 11,12,17 In the present study, we observed reduced intraoperative requirements of all blood products after we stratified the starting amount of fresh frozen plasma, based on the 4-group classification during cardiopulmonary bypass. This was presumably because we recognized fibrinogen replacement by fresh frozen plasma as a priority in blood transfusion, and because the 4-group classification reflected the necessary amount of fresh frozen plasma for effective hemostasis.
Limitations
There are some limitations in the present study. First, this was a retrospective study that obtained data from a routine clinical procedure. Therefore, it should be prospectively confirmed whether the combined evaluation of the fibrinogen level and fibrin polymerization improves the quality of perioperative blood transfusion. Second, postoperative bleeding outcome is not regulated only by the fibrinogen level and fibrin polymerization in cardiac surgery. In this study, there was an intragroup dispersion in postoperative bleeding that was attributable to the duration of cardiopulmonary bypass in groups I and II and attributable to the preoperative administration of warfarin or hemodialysis in group III. We could not exclude the possibility that postoperative blood transfusion influenced the bleeding outcome. Hence, the amount of blood transfusion should be adjusted in accordance with the patient profiles, procedures, and perioperative status.
Conclusion
The 4-group classification, which is based on the combined evaluation of fibrinogen level and fibrin polymerization during cardiopulmonary bypass, may be a useful indicator for postoperative bleeding and may improve the quality of perioperative blood transfusion in cardiac surgery.
Footnotes
Authors’ Note
Mutsuhito Kikura had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. SK, YS, TS, and MK designed and conducted the study, analyzed the data, wrote the article, and approved the final article. TK and SS helped to design the study, reviewed the analysis and the results of the data, and approved the final article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.