
Abstract
The correlation between real-world clinical decisions and adherence to published treatment algorithms for problem bleeding episodes in patients with severe hemophilia and inhibitors and the resultant impact on clinical outcomes were assessed. Nine cases documenting treatment for problem bleeding episodes in patients with severe hemophilia and inhibitors were retrospectively reviewed. Adherence to treatment algorithms was rated on a scale of 1 to 5, 1 being no adherence and 5 being very high adherence. Adherence ratings >3 were assigned to 7 cases in which high adherence was associated with ≤4 days to achieve hemostatic control; hospitalization for ≤7 days was noted in 6 of these cases. In cases rated ≤3 (n = 2), time to hemostatic control ranged from 5 to 8 days and hospitalization duration ranged from 10 to 16 days. These findings suggest that adherence to treatment algorithms may be beneficial in treating problem bleeding events in patients with hemophilia and inhibitors.
Introduction
The development of inhibitors (alloantibodies against factor VIII [FVIII] or factor IX) is a serious complication in patients with severe hemophilia. Inadequate control or failure to prevent hemorrhages results in increased morbidity in patients with hemophilia and inhibitors as compared with those without inhibitors. Patients who have inhibitors are at increased risk of developing hemophilic arthropathy, which markedly decreases their quality of life, as evidenced by their decreased mobility, increased number of orthopedic procedures, and increased frequency of missed work or school days. 1,2
Bypassing therapy with activated prothrombin complex concentrate (aPCC, factor VIII inhibitor bypassing activity; Baxter Healthcare Corporation, Deerfield, IL, USA) or recombinant activated factor VII (rFVIIa, NovoSeven; Novo Nordisk Inc, Bagsvaerd, Denmark) is vital for hemostatic control in patients with severe hemophilia and high-titer inhibitors in the event of bleeding episodes and surgical procedures. Patients with high-titer inhibitors may experience bleeding that does not respond to initial therapy with bypassing agents. Such bleeding events are highly challenging from a treatment perspective. 3
In the absence of information to guide the clinical decision-making process for challenging bleeding episodes, an international panel of physicians with extensive experience in hemophilia treatment used a systematic approach to propose recommendations in the form of algorithms for the treatment of difficult to control life-threatening and non–life- or limb-threatening bleeding events in pediatric or adult patients with hemophilia who have high-titer inhibitors and in whom immune tolerance induction (ITI) has been unsuccessful. The algorithms specified decision-making time points that were based on the type of hemorrhage to assess treatment efficacy and to allow modifications in treatment in order to improve outcomes. 3 The algorithms were aimed at the optimization of timing of treatment decisions that might induce more efficient and rapid responses that lead to improved outcomes. A simulation model which was later developed to forecast the clinical and economic impact of adherence to the treatment algorithms predicted that adherence to the algorithms would lower bypassing therapy costs by reducing the uncontrolled and insufficiently effective consumption of bypassing agents. 4
To examine the benefit and utility of treatment algorithms in real-world clinical practice and to determine whether adherence to these algorithms led to outcomes similar to those that were predicted by the simulation model, panel members reconvened to evaluate treatment decisions in 9 cases of problem bleeding episodes in patients with severe hemophilia and high-titer inhibitors. The primary objectives were to retrospectively determine whether there was a correlation between adherence to treatment algorithms and patient outcomes and to assess the practical implementation of the algorithms. The secondary objective was to evaluate the economic impact of adherence to treatment algorithms. This case series report examines real-world experience in the management of problem bleeding episodes and the potential value of utilizing a treatment algorithm, and identifies modifications that might enhance the efficacy of these algorithms in clinical practice.
Methods
Patient Recruitment
Two members of the original panel who provided recommendations for the treatment of problem bleeding episodes in patients with severe hemophilia and high-titer inhibitors each collected eligible, consecutive cases of problem bleeding episodes that were documented at their respective treatment centers between 2000 and 2010. A total of 9 patient cases were presented to and subsequently evaluated by other members of the original panel at the Treatment Algorithm Case Series Roundtable Meeting held on September 19, 2011, in Chicago, Illinois.
Inclusion and Exclusion Criteria
Inclusion criteria comprised patients of all ages who were diagnosed with severe congenital hemophilia A or B, who had historical peak inhibitor titers >5 Bethesda units, and who had been judged to require bypassing agents for the management of bleeding. Eligible patients who had experienced a defined “problem bleeding episode” were enrolled after obtaining written informed consent (from the patient, parent, or legally authorized representative). Problem bleeding episodes were defined as muscle or joint bleeds, or intracranial hemorrhages requiring treatment in a hospital. Eligible patients had bleeding episodes deemed resistant to initial treatment with bypassing agents (administered either at home or at a clinic or hospital) or unresponsive to treatment within the first 24 hours. Exclusion criteria were the occurrence of ≥2 concurrent bleeding sites, participation in an interventional clinical study, receipt of porcine FVIII before receiving other bypassing therapy (because porcine FVIII was no longer available at the time the treatment algorithm was developed), postsurgical bleeding, and the presence of another congenital bleeding disorder. Patients eligible for ITI were also excluded. 3
Definitions of Terms
The onset of bleeding was defined as the first report of symptoms either at home or in the hospital. The date and time of hospital presentation represent the date and time when the patient was first assessed by the physician after the onset of bleeding.
Hemostatic control was defined as 2 consecutive assessments of “improvement” or 2 consecutive decreases in the intensity of treatment, either by a decrease in dose or by a decrease in treatment frequency. Time to hemostatic control was the amount of time between hospital presentation and the time at which the criteria for hemostatic control were satisfied. Hemostatic control had not been attained if a “worsening” assessment was given within 48 hours after either of the aforementioned criteria (decrease in treatment intensity or 2 consecutive “improvement” assessments) had been fulfilled. Unresponsiveness to treatment was defined as a worsening or lack of improvement in the signs or symptoms of bleeding. Rebleeding was defined as a bleeding episode at the same site that occurred <48 hours after cessation of the first episode. The day of hospitalization was counted as day 1, the next hospitalization day was defined as >24 hours after admission, and each subsequent hospitalization day was defined as 24 hours thereafter. The day of admission was counted as a full day of hospitalization.
Outcome Measures
The primary outcome measure was the time taken to achieve hemostatic control. Secondary outcome measures were the total number of hospitalization days and the total amount of bypassing agent(s) used (in the hospital) for the treatment of the bleeding episode.
Evaluation of Adherence to Treatment Algorithms
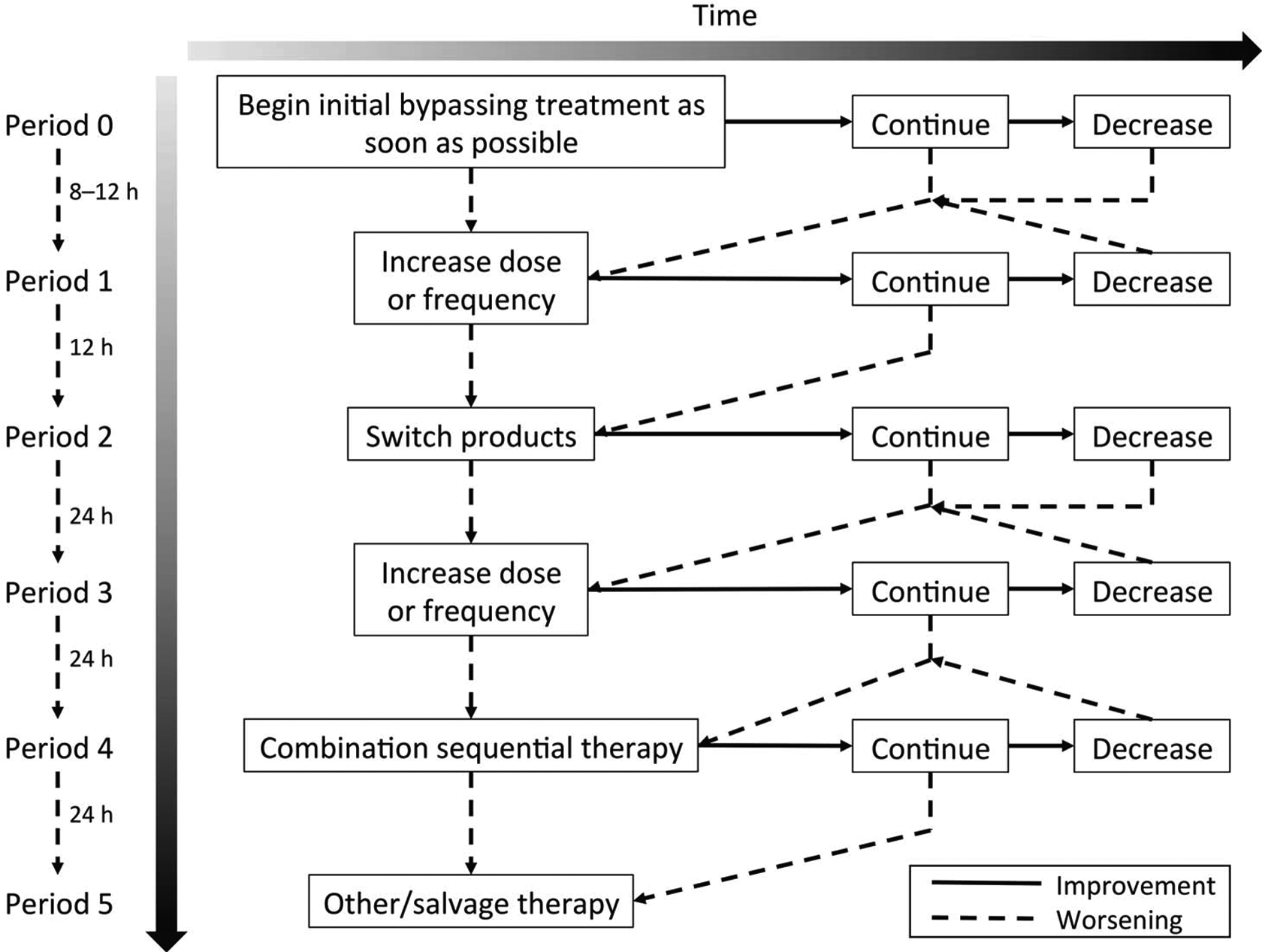
Adherence was evaluated using the previously published recommendations described in the algorithm for muscle hematomas. 3 The algorithm for muscle hematoma (Figure 1) was also used to evaluate the treatment of joint hemorrhages. Treatment decisions were defined as adherent if recommendations in the algorithms that pertained to evaluation intervals, changes in bypassing regimen or product, and the use of sequential therapy were appropriately followed in response to assessments of patient status. Evaluation intervals of 8 to 24 hours were recommended for muscle hematomas and joint hemorrhages, and evaluation intervals of 2 to 4 hours were recommended for intracranial hemorrhages. Decreases in treatment intensity were recommended after 2 consecutive assessments of improvement in patient status. Increases in treatment intensity could be made after a single assessment of worsening or lack of improvement in patient status. The use of sequential therapy with rFVIIa and aPCC was warranted only after high-dose monotherapy with each agent was unsuccessful. Treatment decisions were defined as nonadherent if they deviated from the recommendations indicated in the treatment algorithms. A rating system to evaluate adherence to the algorithm was developed on the basis of the clinical expertise of panel members. Adherence to the algorithm was rated subjectively on a scale from 1 to 5, where 1 signified no adherence, 2 signified low adherence, 3 signified moderate adherence, 4 signified high adherence, and 5 signified very high adherence. Adherence ratings were obtained from each panel member, and the mean adherence rating was calculated for each case.
Results
Demographics and Baseline Characteristics
Patient demographic and baseline characteristics are shown in Table 1. Patients ranged in age from 14 to 36 years and had a diagnosis of severe hemophilia A with inhibitors. None of the patients had a history of nonresponse to bypassing agents.
Demographic and Baseline Characteristics.
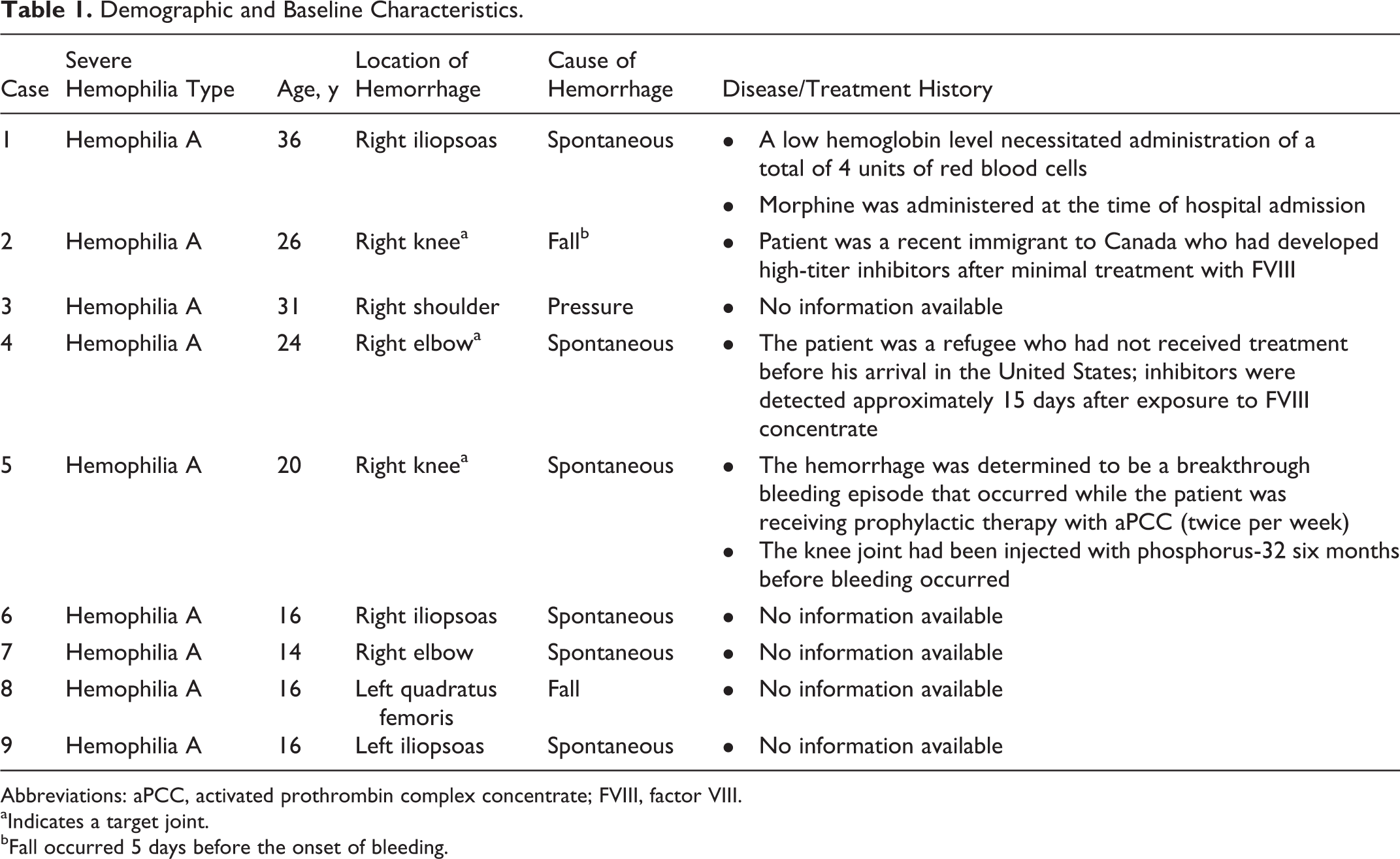
Abbreviations: aPCC, activated prothrombin complex concentrate; FVIII, factor VIII. aIndicates a target joint. bFall occurred 5 days before the onset of bleeding.
Hospital Evaluation and Initial Bypassing Treatment
In all 9 cases, patients received bypassing therapy before hospital presentation, as noted in Table 2. Upon hospital admission, initial bypassing therapy with aPCC was administered in 2 cases and with rFVIIa in 7 cases. The longest duration of hospitalization (16 days) and the most deviations (3) from the treatment algorithm were documented in case 5.
Treatment of Problem Bleeding Episodes and Evaluation of Adherence to the Treatment Algorithm.
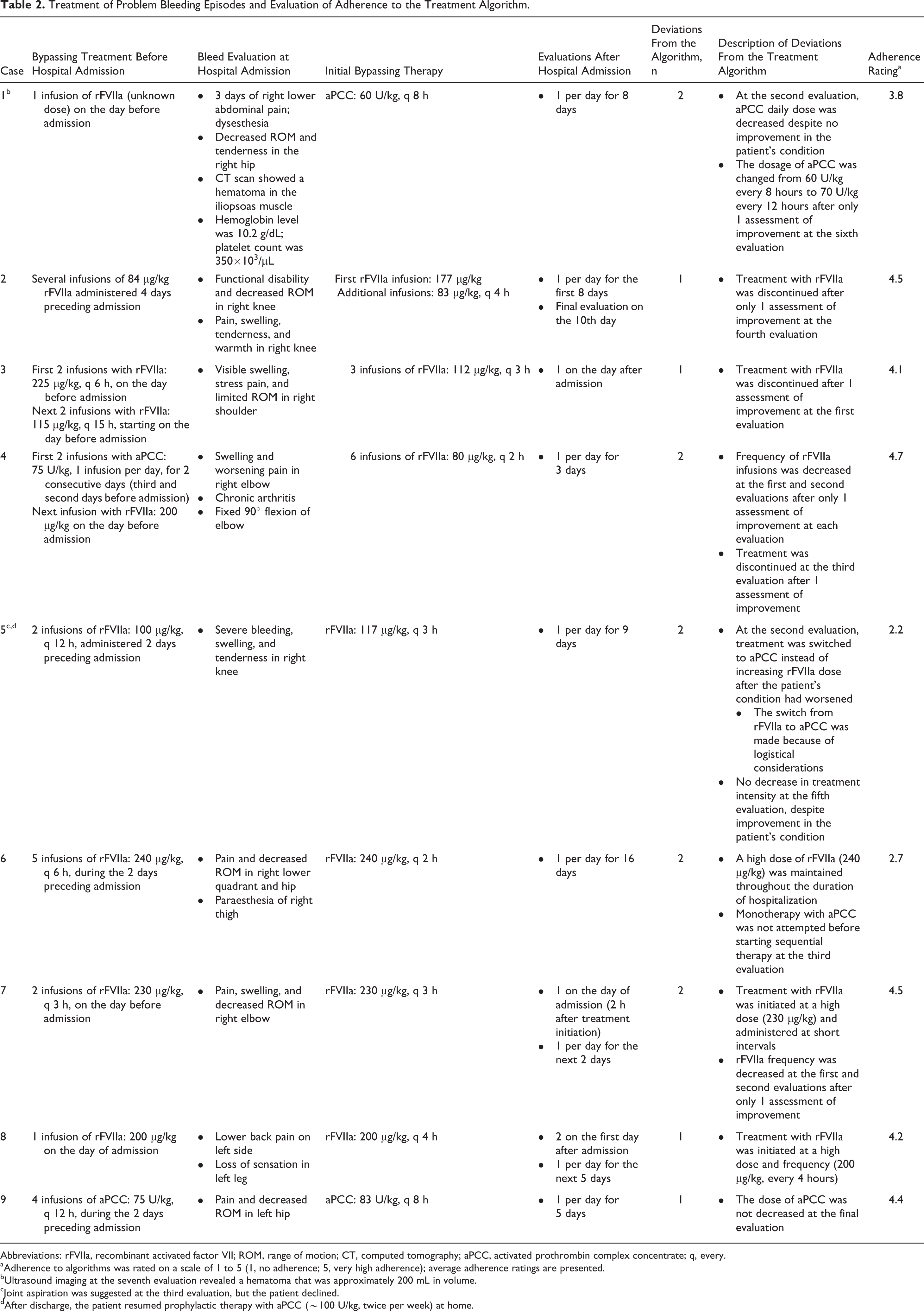
Abbreviations: rFVIIa, recombinant activated factor VII; ROM, range of motion; CT, computed tomography; aPCC, activated prothrombin complex concentrate; q, every.
aAdherence to algorithms was rated on a scale of 1 to 5 (1, no adherence; 5, very high adherence); average adherence ratings are presented.
bUltrasound imaging at the seventh evaluation revealed a hematoma that was approximately 200 mL in volume.
cJoint aspiration was suggested at the third evaluation, but the patient declined.
dAfter discharge, the patient resumed prophylactic therapy with aPCC (∼100 U/kg, twice per week) at home.
Adherence to Treatment Algorithms
The specific deviations from the treatment algorithm for each of the 9 cases are described in Table 2. Figure 2 depicts the average adherence rating for each case. Adherence ratings varied relative to the number and type of deviations from the algorithm. In case 1, the patient’s hemoglobin level remained low (6.2 g/L) until the third evaluation. Three days after discharge without prophylactic therapy, the patient was readmitted after experiencing worsening pain. Computed tomographic imaging confirmed the recurrence of bleeding, and additional bypassing therapy was administered. The patient subsequently began prophylactic therapy with aPCC (75 U/kg twice weekly).
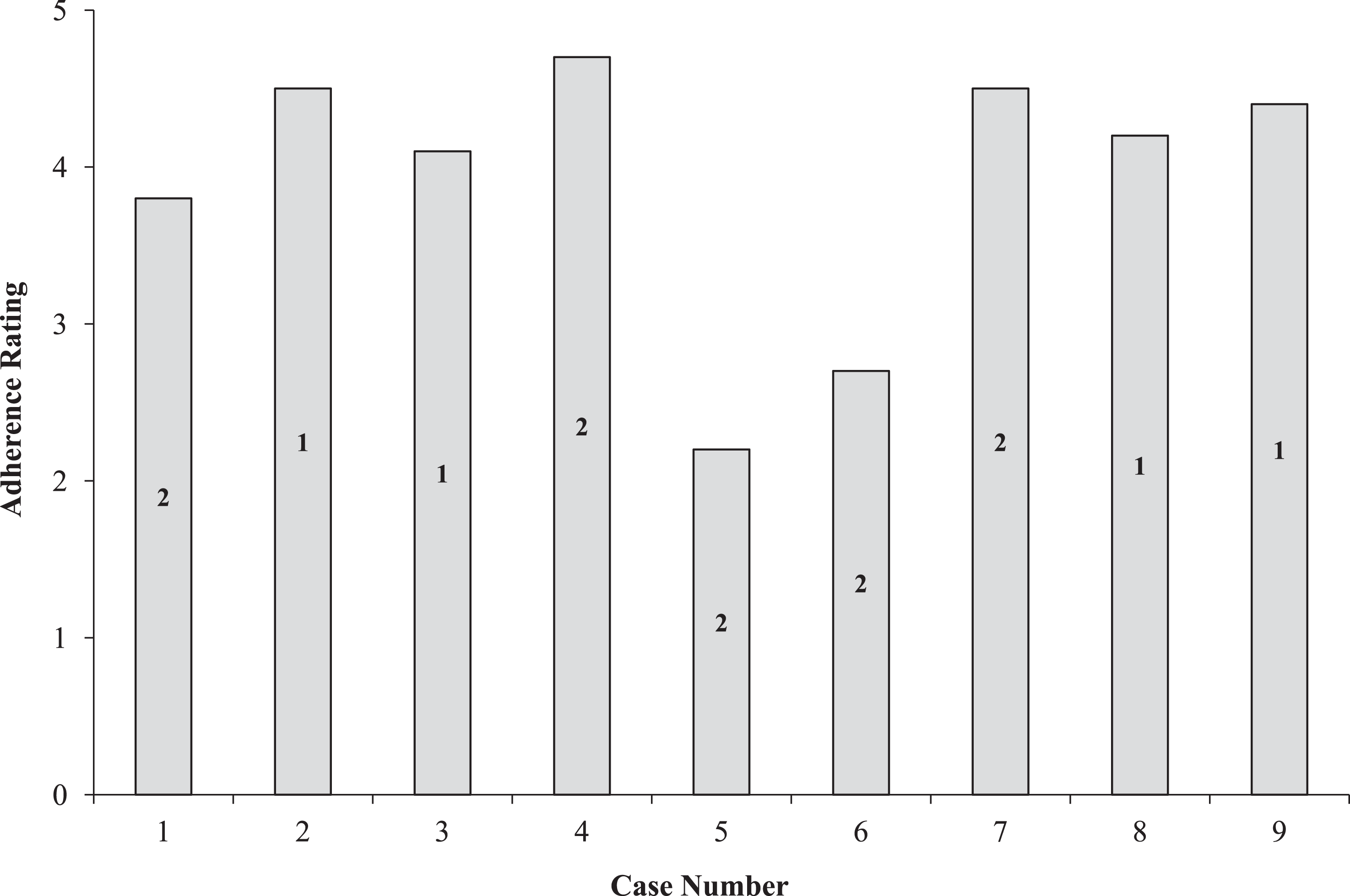
Adherence ratings by case. Numbers within the bars represent the number of deviations from the treatment algorithm.
Abrupt discontinuations in bypassing therapy were noted in cases 2, 3, and 4. However, in case 3, no further change in the patient’s condition was noted at the postdischarge follow-up visit. In case 4, pain in the right elbow had resolved and joint range of motion had returned to baseline at the time of discharge. The omission of key steps in the decision-making process that were observed in cases 5 and 6 resulted in lower adherence ratings than those in the other cases. In case 5, the switch from rFVIIa to aPCC was made because the need for frequent infusions posed challenges for the medical staff. In light of thromboembolic risk, the use of high-dose therapy with rFVIIa was a concern in cases 6, 7, and 8; in case 6, high doses of rFVIIa were used both as monotherapy and as part of a sequential therapy regimen with aPCC. In case 9, therapy with 75 U/kg aPCC every 12 hours was continued for 2 weeks after hospital discharge.
Bypassing Agent Consumption
The quantities of bypassing agents used for hemostatic control are shown in Figure 3. For the 7 cases with average adherence ratings >3 (range, 3.8-4.7), the mean cumulative aPCC dose per patient was 908.7 ± 201.7 U/kg and the mean cumulative rFVIIa dose per patient was 1536.4 ± 1113.2 μg/kg. Relative to cases with high average adherence ratings, the 2 cases (cases 5 and 6) with low average adherence ratings (2.2-2.7) required higher cumulative doses of bypassing therapy and the use of both agents for hemostatic control. The cumulative doses of aPCC and rFVIIa for case 5 were 1456 U/kg and 1989 μg/kg, respectively; the cumulative doses of aPCC and rFVIIa for case 6 were 156 U/kg and 10080 μg/kg, respectively.
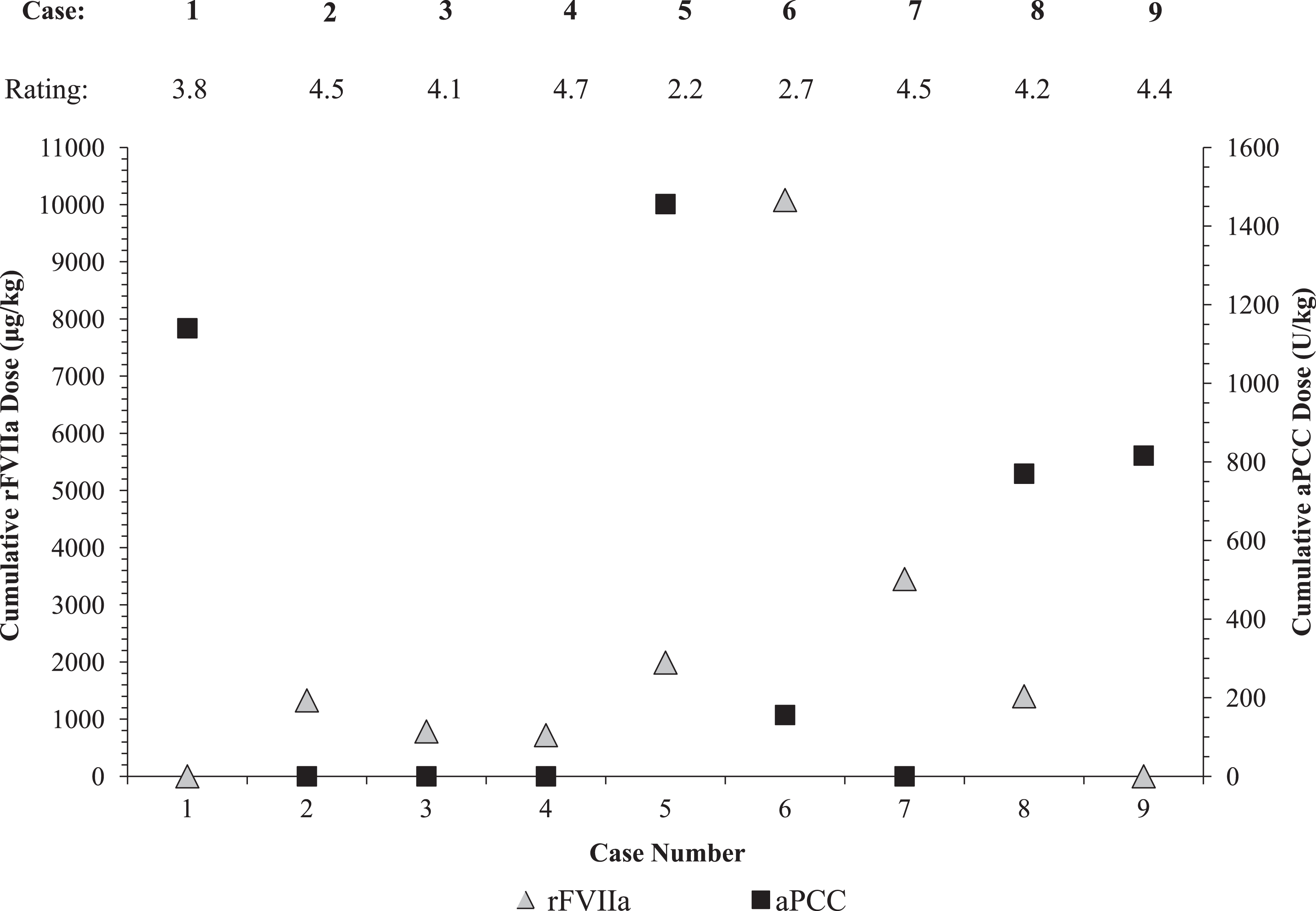
Relationship between adherence ratings and bypassing agent consumption. rFVIIa indicates recombinant activated factor VII; aPCC, activated prothrombin complex concentrate.
Time to Hemostatic Control and Duration of Hospitalization
The effect of adherence to algorithms on the time to achieve hemostasis and the duration of hospitalization are shown in Figure 4. Hemostasis was achieved in ≤4 days in 7 cases, all of which had average adherence ratings ranging from 3.8 to 4.7; hemostasis was achieved within 2 days in 2 of these cases and within 1 day in 4 of these cases (Figure 4A). Hospitalization for ≤7 days occurred in 6 cases, all of which had average adherence ratings >3, and 5 of these 6 cases had ≤6 days of hospitalization (Figure 4B). Hospitalization for ≤4 days was noted in 3 of these 5 cases, all of which had average adherence ratings >4.
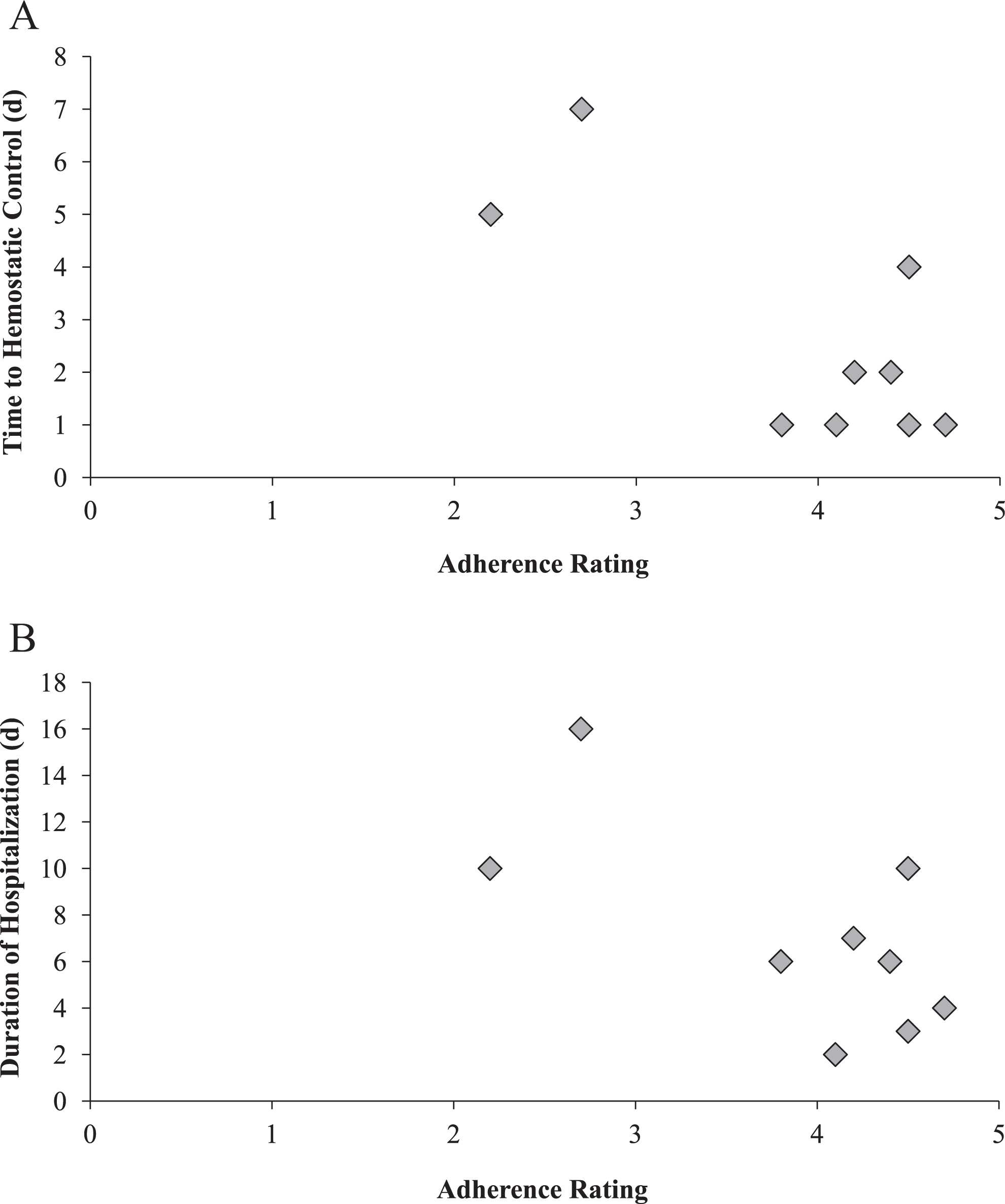
Effect of adherence to algorithm on time to achieve hemostasis and the duration of hospitalization. A, Relationship between adherence rating and time to hemostatic control. B, Relationship between adherence rating and duration of hospitalization.
Discussion
In the absence of evidence-based studies examining therapies for problem bleeding episodes in patients with severe hemophilia and inhibitors, treatment algorithms are valuable tools that may guide physicians in their treatment decisions. The 9 cases presented in this report suggest that adherence to a structured treatment algorithm may be beneficial with respect to clinical outcomes and treatment cost.
Findings from this case series are in agreement with the predictions of the simulation model. 4 In 7 of the 9 cases, close adherence (ie, adherence rating >3) to treatment algorithms was associated with shortened time to hemostatic control and shortened duration of hospitalization. It should be emphasized, however, that the types of hemorrhages varied, rendering comparison of hospitalization duration difficult between cases. Two cases (cases 5 and 6), which had low adherence ratings, had the highest levels of bypassing agents, and both bypassing agents were required for hemostatic control in each case. Case 6 had the longest duration of hospitalization (16 days) and was the only case in which combination sequential therapy with aPCC and rFVIIa was used. In both of these cases, the low adherence ratings reflected the omissions of key steps in the algorithm that were considered more serious deviations than those reported in the other cases.
Absence of recommended treatment, nonrecommended changes in treatment intensity, or abrupt discontinuation of bypassing therapy occurred in 8 cases. Repeated use of high-dose therapy during the treatment period was observed in 3 cases. Switching bypassing agents for convenience, noted in 1 case as a deviation from the algorithm, may be perceived as a reasonable clinical decision under some circumstances. Sequential therapy without attempting monotherapy with the alternate bypassing agent was observed in 1 case.
Combination sequential therapy, used in 1 of the 9 cases (muscle hematoma), has been shown to be effective for treating problem bleeding episodes in patients with severe hemophilia and inhibitors 5 because of the synergistic effect of aPCC and rFVIIa. 6 Although reports from 2 studies demonstrated that sequential therapy with rFVIIa and aPCC can be safely administered in this patient population using appropriate doses and dosing frequency, 7,8 a recent meta-analysis reported thrombotic complications in 13% (5 of 40) of patients with severe hemophilia and inhibitors who received combination sequential therapy. 9 Recommendations for the safe use of combination sequential therapy include a “washout” period or a minimum interval of 6 hours between products to minimize the risk of thrombosis. 10,11
Another critical aspect of bypassing therapy noted among these cases was the use of high-dose regimens administered at very short intervals. High-dose (>200 μg/kg) infusions of rFVIIa were administered at 2- and 4-hour intervals in 3 of the 9 cases that were evaluated. Administration of high-dose rFVIIa infusions at frequent intervals may raise the risk of thromboembolic events. 12 Typically, doses of 90 μg/kg rFVIIa are recommended for high-frequency regimens; however, single, high-dose boluses ranging from 270 to 346 μg/kg rFVIIa have been used with good efficacy and no thrombotic complications. 13 –15 Caution is also required when administering high doses of aPCC (≥100 U/kg per infusion), as it is recommended that doses should not exceed 200 U/kg/d. 16 Patients receiving individual aPCC doses of 100 U/kg require careful monitoring for the possible development of disseminated intravascular coagulation or acute coronary ischemia. 16
Findings from this case series also highlight the need for changes to the algorithms to better treat and monitor problem bleeding events in patients with hemophilia and inhibitors. Suggested modifications include incorporation of guidelines for bypassing agent dose and dosing frequency, provision of separate treatment recommendations for joint hemorrhages in target versus non-target joints, inclusion of guidelines to monitor improvement and stabilization of the patient’s condition, specification of evaluation intervals when improvement is noted, a clear definition of stable status, and permission to switch bypassing agents under extenuating circumstances (eg, lack of immediate availability of the previously used bypassing agent). Furthermore, the requirement of 2 consecutive improvements before initiation of a change in therapy may not be feasible in the clinical setting; in the treating physician’s clinical judgment, a single, yet clinically meaningful, improvement may suffice. Finally, specifying the severity of specific deviations from the algorithm may assist with the clinical decision-making process.
The retrospective nature of this case series analysis restricted the investigation of additional factors that may have contributed to patient outcomes, and documentation of evaluations may have been incomplete in some cases. The small number and varied nature of cases analyzed prevented statistical assessment of aspects pertaining to the efficacy of adherence to treatment algorithms. A larger scale study is required to unequivocally establish the efficacy of these algorithms. Adherence ratings were subjective and made by a small number of individuals, all of whom were involved in the development of the algorithms, which may have biased the evaluation. The suggested modifications may further strengthen the utility of treatment algorithms in clinical practice.
Footnotes
Author Contributions
Dr Guy Young and Dr Jerome Teitel provided patient cases, and contributed to the study design, data analysis, and case evaluation. Dr Cindy Leissinger, Dr Roseline d’Oiron, and Dr Erik Berntorp contributed to the data analysis and case evaluation. All authors provided critical comment and final approval of the article. Editorial support for this article was provided by MedLogix Communications, LLC, and was paid for by Baxter Healthcare Corporation.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Guy Young receives consultancy fees and honoraria for speaking engagements from Baxter and Novo Nordisk. Dr Jerome Teitel is a consultant and serves on advisory and data safety monitoring boards for Baxter, Bayer, CSL Behring, and Pfizer. Dr Cindy Leissinger receives grant funding from Baxter and Novo Nordisk and serves as a paid consultant and advisory board member for Baxter and Novo Nordisk. Dr Roseline d’Oiron received fees and honoraria from Baxter, Novo Nordisk, Bayer, Pfizer, Sobi, and CSL Behring for attending advisory boards, consultancy, or speaking at symposia. Dr Erik Berntorp serves on advisory boards for Baxter and Novo Nordisk and receives research grants from Baxter and lecture fees from Baxter and Novo Nordisk.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by an unrestricted educational grant from Baxter Healthcare Corporation.