
Abstract
Background:
Warfarin, which is a widely used oral anticoagulant, has a narrow therapeutic window and requires regular international normalized ratio (INR) monitoring to maintain optimal anticoagulation. Recently, several portable coagulometers have been developed to measure INR levels.
Objective:
To compare the INR results obtained by a portable coagulometer (CoaguChek XS) and a standard laboratory method (STAGO STA-R).
Methods:
Overall, 433 consecutive patients (male: 191, median age: 61 [44-86] years) who were admitted to outpatient anticoagulation clinic were enrolled in this study. Each patient was tested for INR using portable CoaguChek XS and STAGO STA-R automatic laboratory coagulometer. Correlation between methods was assessed using the Pearson correlation test and Cohen κ test. Bland-Altman plot was used to identify mean difference and 95% limits of agreement.
Results:
The mean INR values for CoaguChek XS and STAGO STA-R were 2.54 ± 1.17 and 2.79 ± 1.39, respectively. There was a strong positive correlation between the 2 methods (r = .966; 95% confidence interval [CI]: 0.95-0.97, P < .001). The Bland-Altman analysis gave a mean difference of 0.26 ± 0.40 between the 2 methods, with a 95% limit of agreement of −0.54 to 1.05. In patients with INR values >5.0, there was only a moderate correlation (r = .676; 95% CI: 0.38-0.89, P = .002), and the mean difference of INR tended to increase as mean INR values increased. There was a high overall agreement between the 2 methods (κ = .751; 95% CI: 0.69-0.80; P < .001).
Conclusion:
There was good consistency between traditional laboratory testing and CoaguChek XS coagulometer, which provides rapid and reliable INR analysis.
Introduction
Vitamin K antagonists (VKAs), such as warfarin, have been the drugs of choice for oral anticoagulation for a long time. Their effectiveness was mostly demonstrated in primary and secondary prevention of systemic embolism in patients with heart valve prostheses and atrial fibrillation (AF) as well as the treatment of venous thromboembolism. 1,2 The anticoagulant effect of VKAs can be monitored by the prothrombin time or the international normalized ratio (INR).
Therapeutic success with the VKAs is highly dependent on the quality of dose management. The goal of therapy is to keep the patient within the predetermined therapeutic range, usually an INR of 2.0 to 3.0 for most indications or 2.5 to 3.5 for selected patients with mechanical heart valves or highly thrombogenic conditions. Time in therapeutic range is a principal determinant of clinical outcomes as shown in numerous clinical trials. 3
Warfarin has a narrow therapeutic window and therefore requires regular INR monitoring to ensure that a therapeutic level is maintained. 4 Due to the variable pharmacokinetic profile, its anticoagulation effect shows great interpatient and intrapatient variability closely related to genetic and environmental factors, 5 and there is a high potential for drug-drug and dietary interactions. 6 These factors can result in a poor INR control in “real-world” clinical practice.
In recent years, several portable coagulometers using capillary blood for INR analysis have been developed. These instruments, known as point of care (POC), have eliminated the need for whole blood collection and plasma separation by centrifugation and, thus, facilitate the monitoring of VKAs. 7 Although they were originally developed for home use, POC monitors have become very useful in hospital and outpatient clinics due to the practicality and speed in obtaining results. 8 However, there are limited studies in the literature regarding the consistency of their results with standard laboratory methods. 9
The objective of this study was to evaluate and compare the INR results obtained by a portable coagulometer device (CoaguChek XS) and a standard laboratory method (STAGO STA-R automatic coagulometer) in a large number of patients admitted to our outpatient anticoagulation clinic.
Materials and Methods
Study Population
A total of 433 consecutive patients with a median age of 61 years (range, 44–86), who were admitted to outpatient anticoagulation clinic of Kosuyolu Kartal Heart Training and Research Hospital, İstanbul, Turkey, for routine INR monitoring between March 2014 and April 2014 were enrolled in this study. The study population consisted of 191 males and 241 females who were on VKA therapy for various indications. Each patient gave informed consent to participate in this study, and the study was approved by the institutional review board.
Point-of-Care Procedure
The CoaguChek XS (Roche Diagnostics, Basel, Switzerland) system consists of a small and portable coagulometer and disposable test strips. It measures the INR in whole blood obtained by finger prick, using recombinant human thromboplastin, and has an international sensitivity index (ISI) value of 1.0. All measurements were performed simultaneously in the blood collection room when venous blood samples were taken for standard laboratory tests. About 0.01 cm3 blood at the end of capillary of finger was collected from all patients by the same physician and added into corresponding area on the dry reaction test strip and tested with a portable CoaguChek XS coagulometer.
Standard Laboratory Procedure
Blood samples were collected by a clean puncture of an antecubital vein in the blood collection room. Peripheral venous blood of about 3 cm3 was collected by laboratory staffs, and added into a blood collection tube containing 3.8% buffered sodium citrate. Then, the tubes were transferred to the laboratory where they were centrifuged at 2500 × g for 20 minutes at room temperature. The plasma obtained after centrifugation were analyzed with a STAGO STA-R (Diagnostica Stago, France) automatic coagulometer using STA-R Hepato Quick kit (Diagnostica Stago, SAS) with an ISI value of 0.91.
Statistical Analysis
Statistical analyses were performed using SPSS for Windows version 19.0 (SPSS Inc, Chicago, Illinois), and significance level was set as P < .05 in all statistical analyses. The variables were investigated with the use of analytical methods (Kolmogorov-Smirnov/Shapiro-Wilk tests) to determine whether they were normally distributed. Descriptive statistics were reported as mean with standard deviation for normally distributed continuous variables, median with minimum and maximum values for nonnormally distributed continuous variables, and as frequency with percentages for the categorical variables.
Correlation between methods was assessed using the Pearson correlation test. Bland-Altman plot was used to identify mean difference and 95% limits of agreement of the INR results between CoaguChek XS and STAGO STA-R. The overall correlation and difference were compared in a total of 433 measurements and were further compared in 4 INR ranges (INR < 2.0, 2.0 ≤ INR ≤ 3.5, INR > 3.5, and INR > 5.0).
In a second phase, the quantitative data were categorized into 3 ranges: subtherapeutic, therapeutic, and supratherapeutic ranges. The definition of the ideal therapeutic range depended on the indication of oral anticoagulation. For patients with mechanical prostheses, the ideal range was between 2.5 and 3.5. For the other indications, the ideal range was between 2 and 3. Cohen κ value was used for assessing the degree of agreement between methods in guiding the clinical management (<0.4, poor; 0.4-0.75, fair to good; and >0.75, excellent). Concordance was defined when both of the paired INR results were within the therapeutic range or both were above the therapeutic range (supratherapeutic) or both were below the therapeutic range (subtherapeutic).
Results
The INR results were obtained from 433 consecutive patients who were on VKA therapy. The indications for oral anticoagulation with VKAs are listed in Table 1. The laboratory INR results ranged from 0.9 to 7.5 with a mean of 2.54 ± 1.17, and CoaguChek XS INR ranged from 0.9 to 8.0 with a mean of 2.79 ± 1.39 (Figure 1A and B). Pearson correlation coefficient (r) obtained by comparing INR levels of the 2 methods was 0.966 (P < .001; 95% CI: 0.95-0.97; Figure 2A). The mean INR difference between the 2 methods was 0.26 ± 0.40. The Bland-Altman plot illustrates the mean difference between the 2 methods, with POC exhibiting a mean bias of 0.26 and a 95% limit of agreement of −0.54 to 1.05. The mean difference in INR measurements tended to increase as mean INR values increased (Figure 2B). The agreement of INR measurements between CoaguChek XS and STA-R was further assessed according to the 3 INR categories (subtherapeutic, therapeutic, and supratherapeutic ranges). When the influence of INR measuring method on dose-management decisions was taken into consideration, total observed agreement (concordance) between the 2 methods was 84.3%. The INR measurements showed a difference (discordance) in dosing decision between the 2 methods in 68 (15.7%) patients (Table 2). The overall agreement was excellent (κ = .751; 95% CI: 0.69-0.80; P < .001; Table 3).
The List of Indications for Use of VKAs in Study Population.
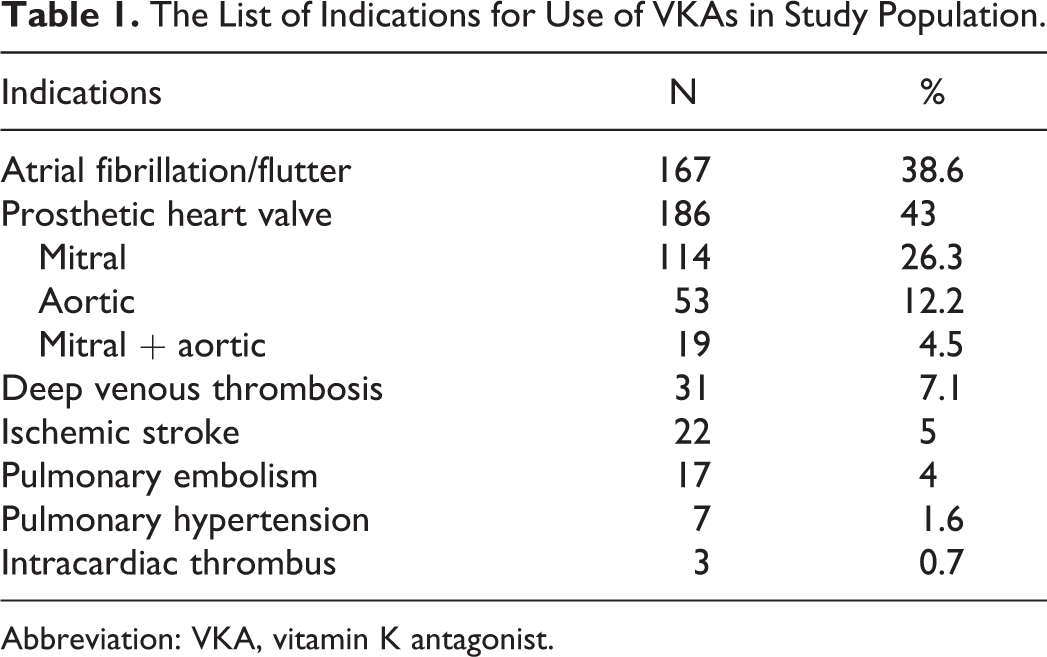
Abbreviation: VKA, vitamin K antagonist.
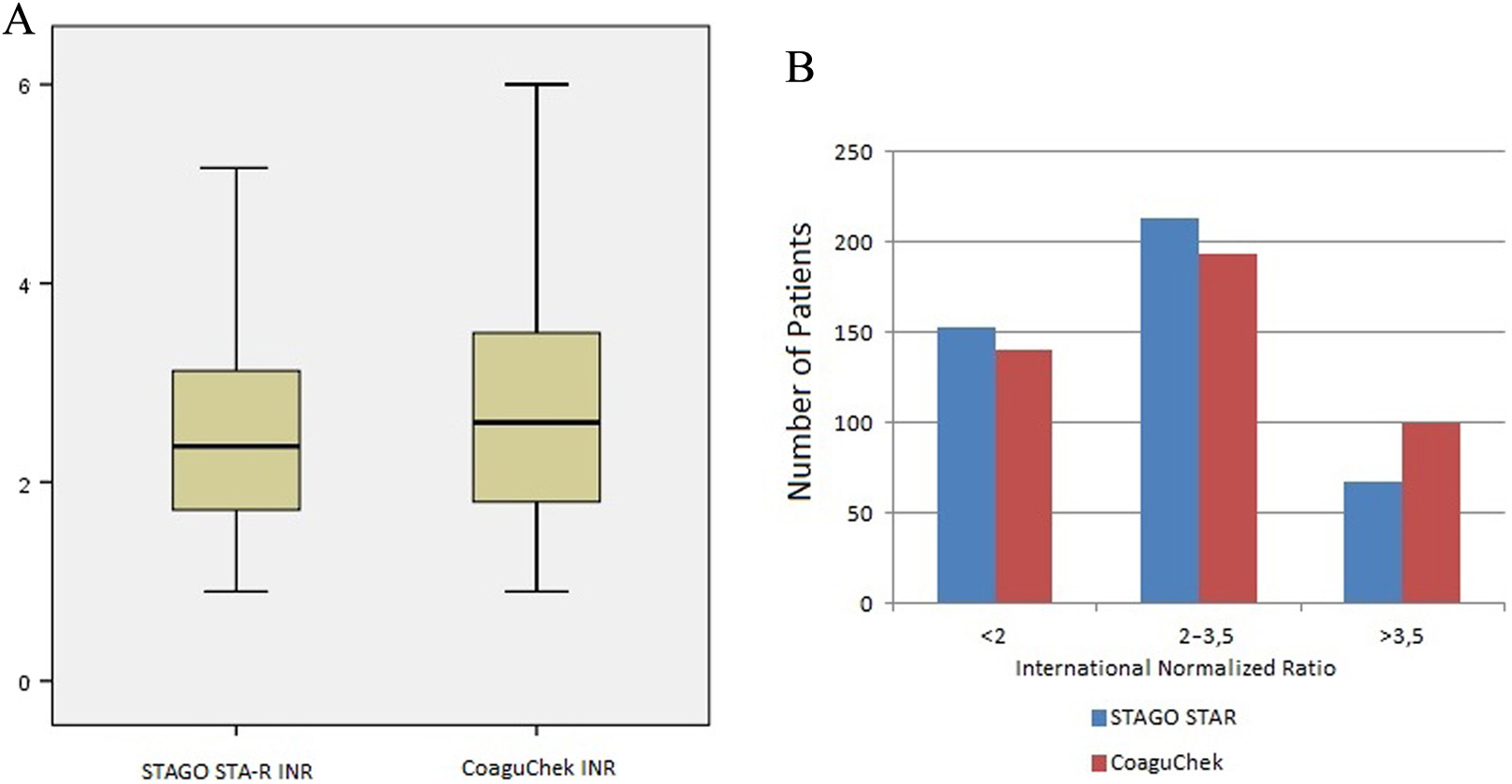
The box plot (A) and simple bar (B) graphs illustrating the distribution of the international normalized ratio values obtained by portable CoaguChek XS and laboratory STAGO STA-R coagulometers.
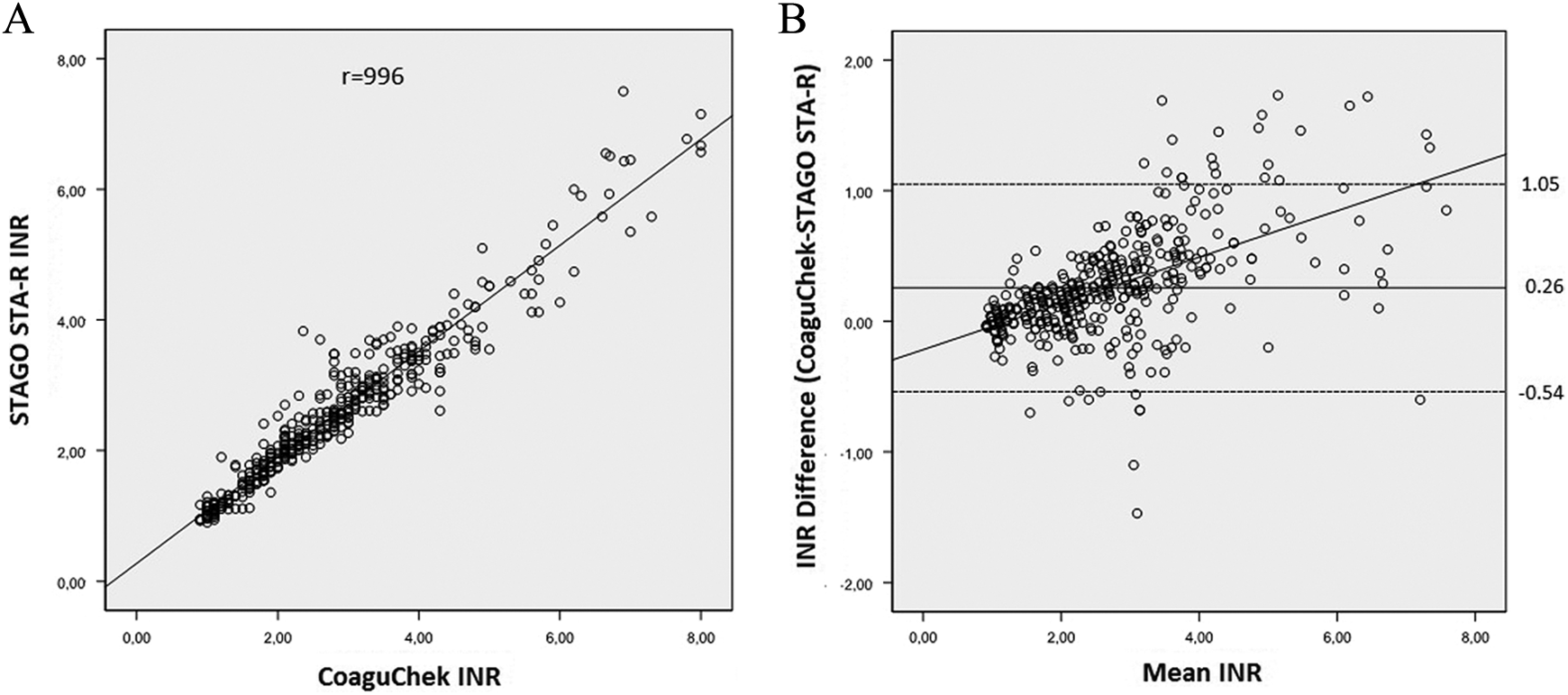
The scatter plot graph illustrating the strong correlation between the international normalized ratio (INR) values obtained by portable CoaguChek XS and laboratory STAGO STA-R coagulometers (A). The Bland-Altman diagram showing the magnitude of the difference between the INR values obtained by the laboratory and CoaguChek XS. The solid line represents the mean difference and the dashed lines represent the lower (−1.96 standard deviation [SD]) and upper limits (+1.96 SD) of agreement. The mean difference in INR measurements tends to increase as the mean INR values increases (B). (The mean INR was calculated by adding the CoaguChek XS to the laboratory INR values and then dividing the sum by 2.)
Accuracy Criteria and the Corresponding Results of Comparison.
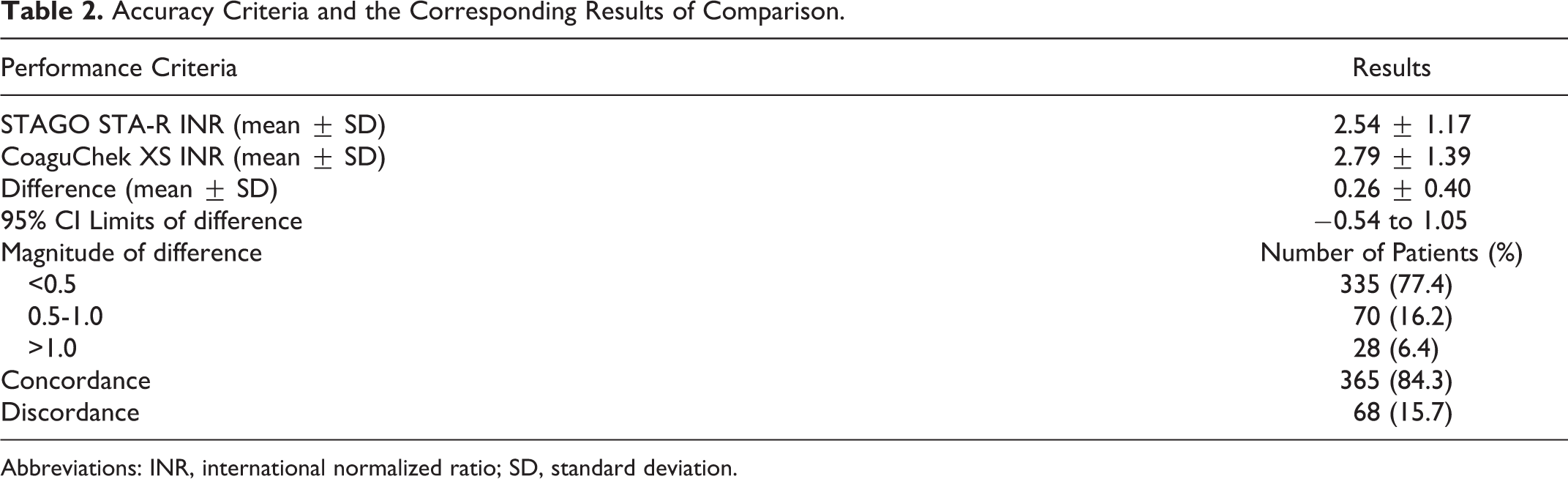
Abbreviations: INR, international normalized ratio; SD, standard deviation.
Agreement of INR measurements between CoaguChek XS and STAGO STA-R.a
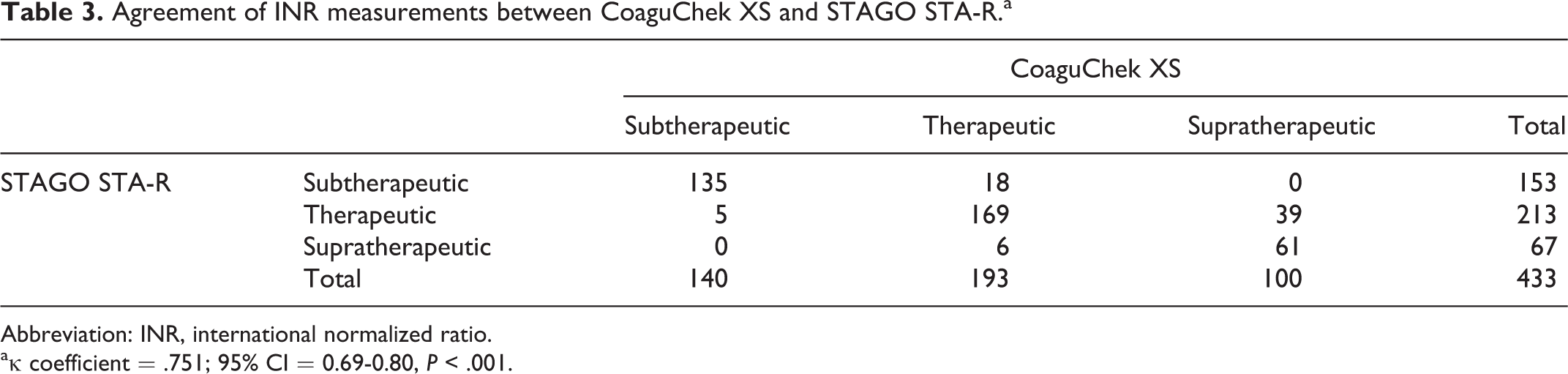
Abbreviation: INR, international normalized ratio.
aκ coefficient = .751; 95% CI = 0.69-0.80, P < .001.
Patients were grouped according to the indications for VKA as AF group (n = 167), protahetic heart valve group (n = 186), and the others (n = 80). There was no difference in terms of Pearson correlation coefficients (r) in these groups: .957 (95% CI: 0.94-0.97, P < .001); 0.969 (95% CI: 0.95-0.98, P < .001), and 0.978 (95% CI: 0.96-0.98, P < .001), respectively.
Pearson correlation coefficients (r) obtained at INR < 2.0, 2.0 ≤ INR ≤ 3.5, and INR > 3.5 ranges were 0.919 (95% CI: 0.87-0.95, P < .001), 0.820 (95% CI: 0.76-0.86, P < .001), and 0.880 (95% CI: 0.82-0.92, P < .001), respectively (Table 4 and Figures 3A, 4A, and 5A). On the other hand, the mean differences in the INR measurements in subgroups were 0.06 ± 0.16, 0.30 ± 0.36, and 0.56 ± 0.63, respectively (Figures 3B, 4B, and 5B). The 95% CI of the differences in these 3 subgroups were −0.25 to 0.373, −0.41 to 1.01, and −0.67 to 1.79, respectively (Table 5). In 18 patients whose laboratory INR values were >5.0, there was only a moderate correlation between the 2 methods (r = .676; 95% CI: 0.38-0.89, P = .002), and the mean difference in this subgroup was 0.66 ± 0.62 (Figure 6A and B) with a 95% CI of −0.54 to 1.88.
The Summary of the Correlation Analysis Between the 2 Methods in Total and Subgroups.
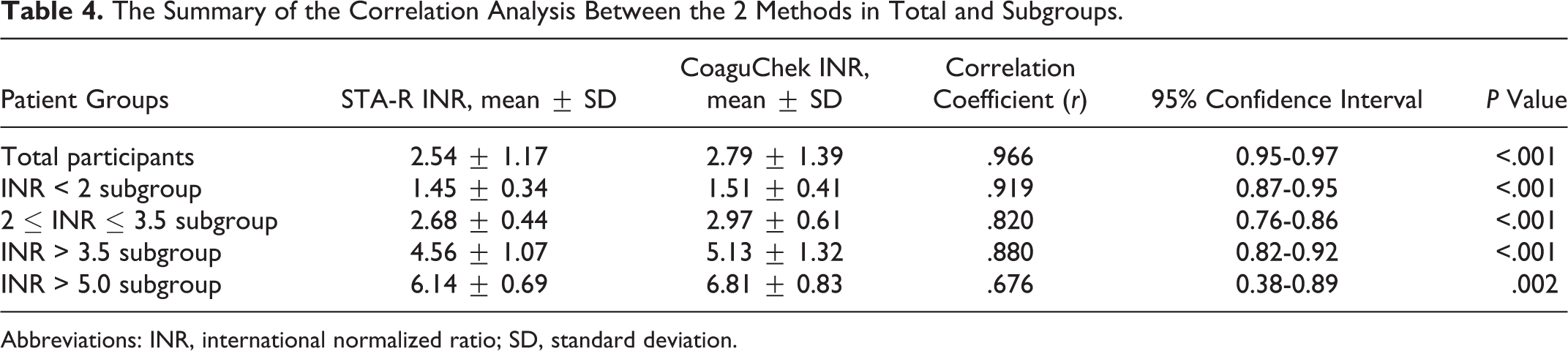
Abbreviations: INR, international normalized ratio; SD, standard deviation.
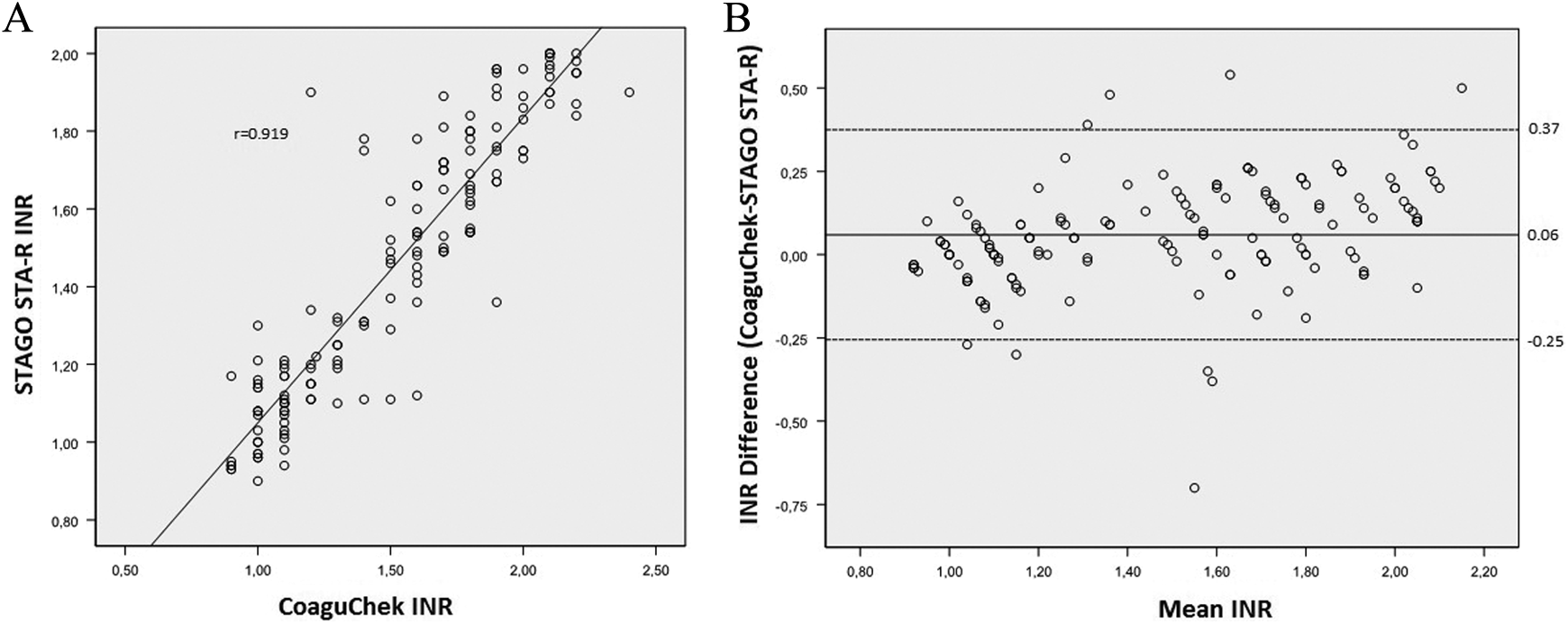
Comparison of international normalized ratio (INR) measurements between the 2 methods by scatter plot (A) and Bland-Altman diagram (B) in the INR range of <2.0 in 153 patients.
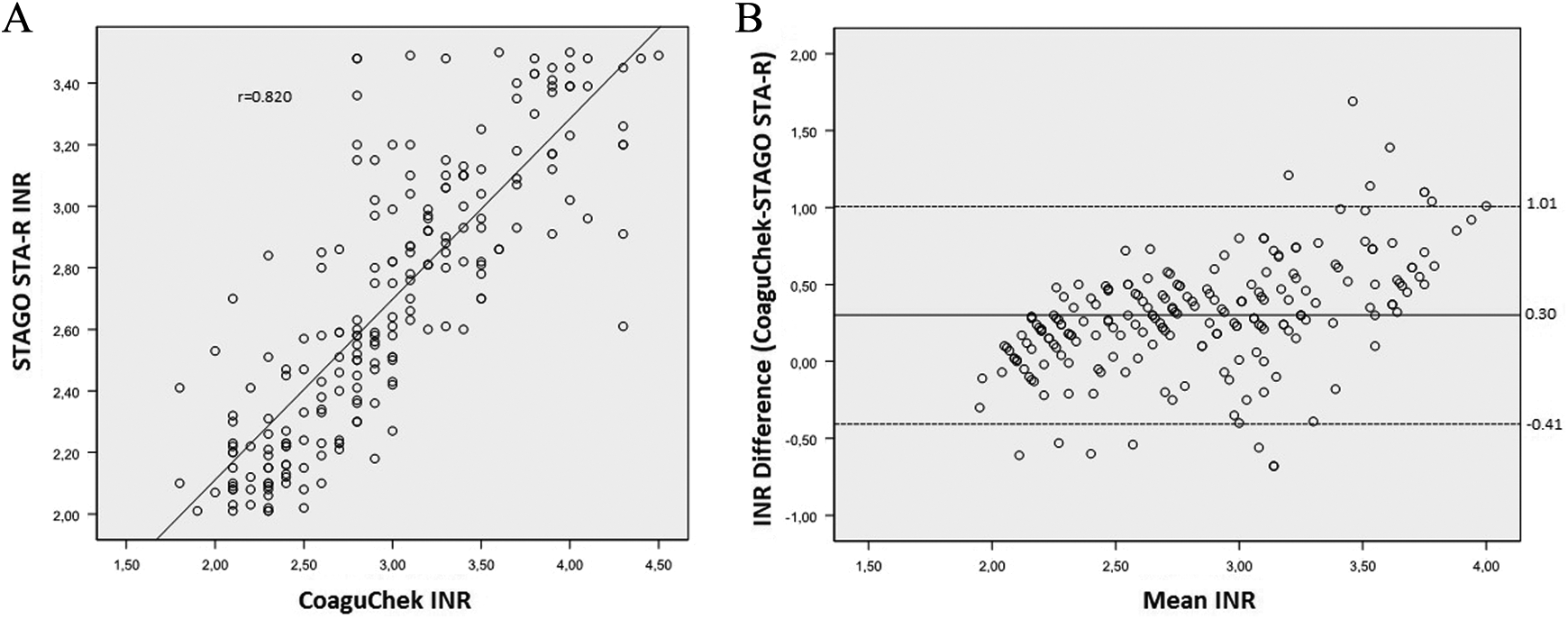
Comparison of international normalized ratio (INR) measurements between the 2 methods by scatter plot (A) and Bland-Altman diagram (B) in the INR range of 2.0 to 3.5 in 213 patients.
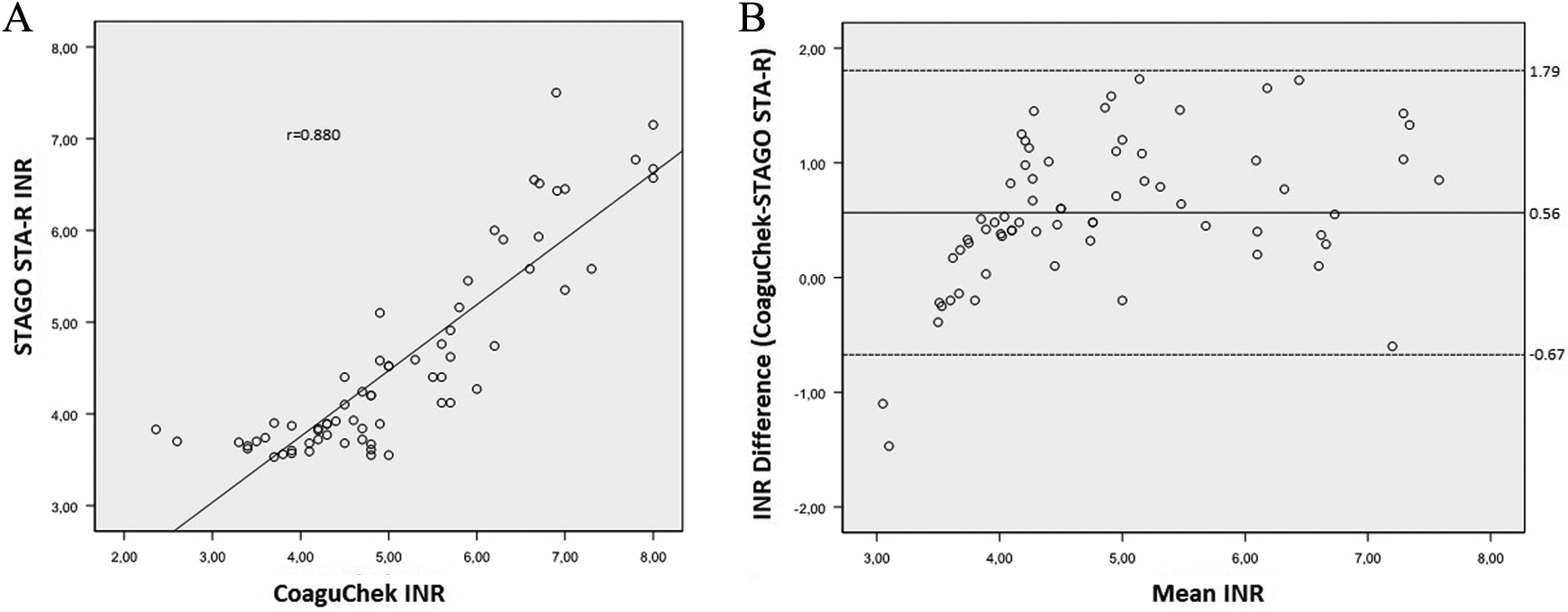
Comparison of international normalized ratio (INR) measurements between the 2 methods by scatter plot (A) and Bland-Altman diagram (B) in the INR range of >3.5 in 67 patients.
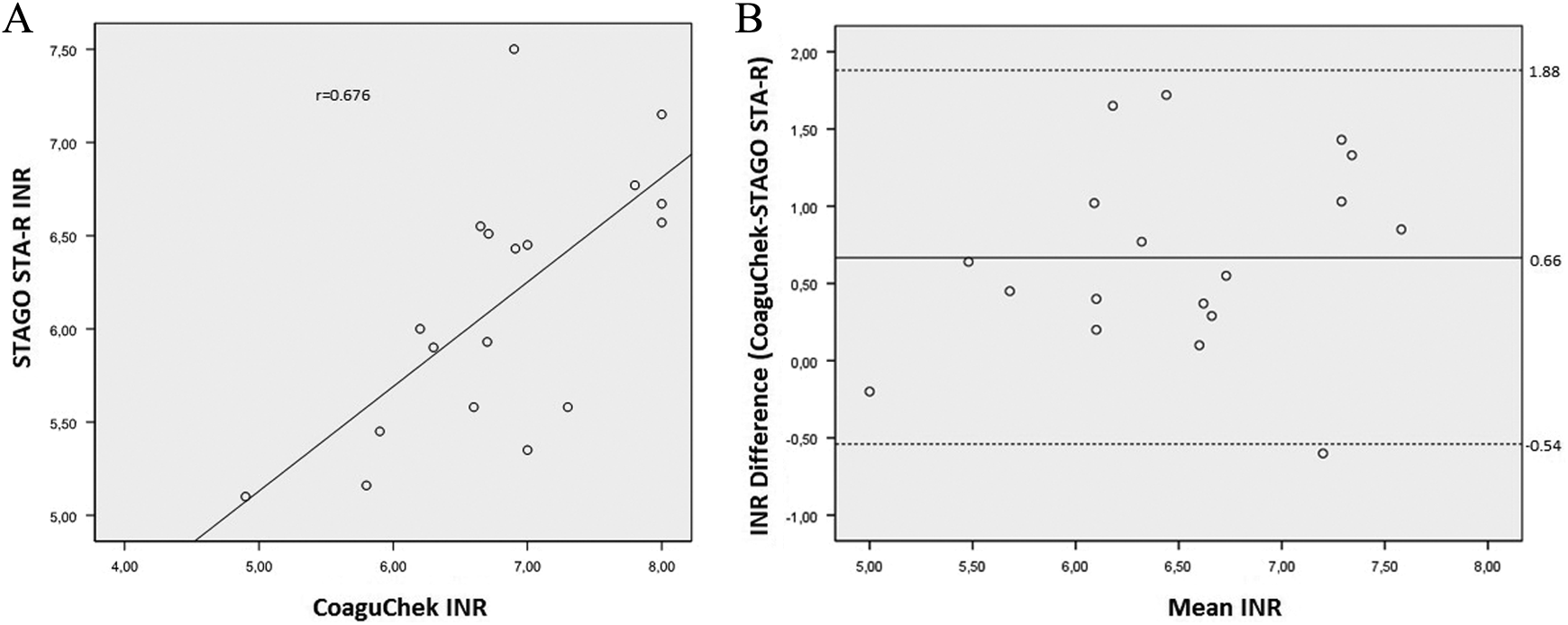
Comparison of international normalized ratio (INR) measurements between the 2 methods by scatter plot (A) and Bland-Altman diagram (B) in the INR range of >5 in 18 patients.
The Summary of Accuracy Analysis Between the 2 Methods.
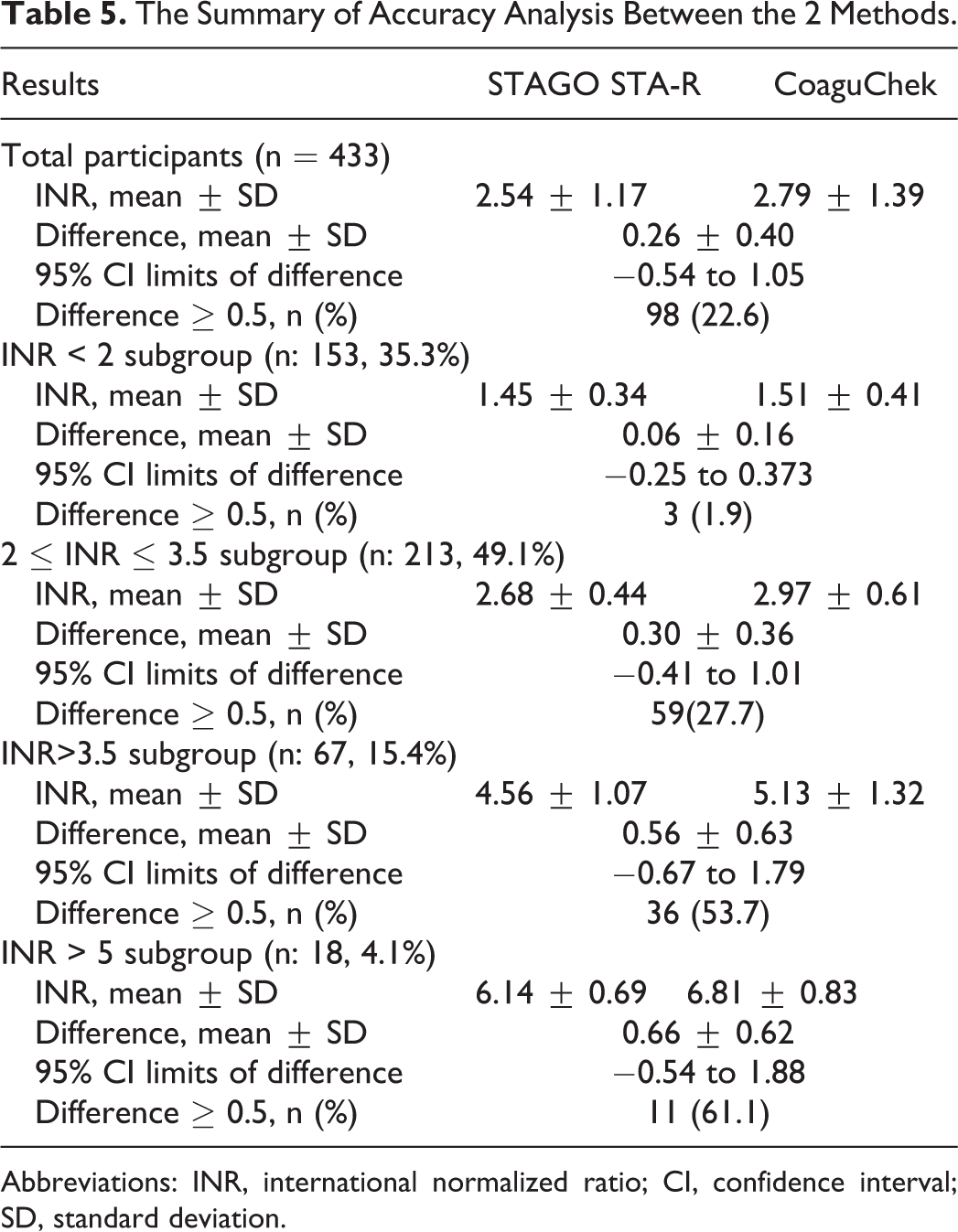
Abbreviations: INR, international normalized ratio; CI, confidence interval; SD, standard deviation.
The absolute differences between the POC and the laboratory results were <0.5 INR units in 335 (77.4%) and ≥0.5 INR units in 98 (22.6%) patients (Table 2). The prevalance of the patients with an absolute INR difference ≥0.5 tended to increase in subgroups as the INR range increased: 3 (1.9%), 59 (27.7%), 36 (53.7%), and 11(61.1%), respectively (Table 5).
Discussion
This monocentric observational study enrolling 433 patients on warfarin therapy showed that INR results of portable CoaguChek XS coagulometer correlated well with traditional laboratory testing (STAGO STAR) in multiple clinical settings. CoaguChek XS coagulometer provides rapid and reliable INR analysis for clinical management of the patients who are on VKA therapy.
Oral anticoagulants are widely used for the treatment of cardiovascular diseases, such as AF/flutter, valvular heart disease, and venous/arterial thromboembolism. Although novel oral anticoagulants provide successful prevention of thromboembolism in patients with nonvalvular AF and venous thromboembolism, VKA is still necessary for many patients, particularly for those with rheumatic heart diseases and prosthetic valves. Although the number of patients receiving VKA has consistently increased, the therapeutic success is highly dependent on the requirements to maintain the INR within a narrow target range, which includes frequent testing and appropriate dose adjustments. The risk of hemorrhagic and thromboembolic complications associated with the use of VKAs renders the routine INR monitoring mandatory for patient safety. Oral anticoagulation therapy should be managed in a systematic and coordinated fashion, incorporating patient education, systematic INR testing, followup, and good patient communication of results and compliance for dose adjustments.
Classical laboratory methods for INR testing analyze plasma samples and need whole blood collection and plasma separation by centrifugation, which requires a considerable amount of time and work load. Portable coagulometers are increasingly being used in general practice by primary healthcare providers and by patients in home settings and have the potential to improve management of anticoagulation therapy. The sample size required for these POC devices is much smaller (10 µL) and easier to obtain as compared with standard methods. Another advantage of the POC devices is the immediate availability of results, which enhances clinical decision making and therapeutic monitoring. Patients can have their test result managed by their health care provider (patient self-testing), or they can interpret their INR result and adjust their own dose of anticoagulant accordingly (patient self-management). Previous systematic reviews showed that self-monitoring is a safe intervention, which gives rise to significant reduction in thromboembolic events while reducing the risk of death. Additionally, patients spend more time in the therapeutic range of INR than they would without self-monitoring. 10 –12 However, there have been several documented limitations regarding the accuracy of these devices, including differences compared with a standard plasma-based laboratory method, especially in supretherapeutic INR ranges. 13
We have compared the INR results of the CoaguChek XS coagulometer and a standard laboratory method (STAGO STA-R) in the current study, and there was a considerably high correlation between the 2 methods. However, we observed that the mean difference of INR measurements tended to increase as the mean INR values increased. This observation led us to evaluate the performance of CoaguChek XS in 18 patients who had INR values >5.0. There was only a moderate correlation between the 2 methods in this subgroup. Similar findings were observed in a study carried out by Donaldson et al which demonstrated that the greater the INR value, the lower the correlation was detected between the methods studied. 14 The clinical impact of the increasing discrepancy between the methods in patients with supratherapeutic INR is unknown, however it may be necessary to double check the results with the laboratory findings in patients with INR values >5.0.
Although numerical differences may occur in the INR results between both the methods, these may not be clinically significant. It is important to evaluate whether there would be a change in the treatment, meaning a modification in the oral anticoagulant dose. Several studies suggest that both methods can be considered comparable as long as both INRs are within the therapeutic range or if both present a maximum difference of 0.5 INR units, regardless of the oral anticoagulation level. 15,16 Our study demonstrated that the mean difference of INR obtained by CoaguChek XS compared to the standard laboratory testing was of 0.26 INR units.
In addition to the statistical evaluation of the correlation between the methods, it is important to analyze the clinical agreement between the results generated by both methods. So the data were also categorized according to therapeutic levels and the 2 methods were compared for consistency by κ analysis. In our study, the clinical agreement was excellent with a concordance of 84.3% . It is noteworthy that in none of the cases the disagreement between the methods would lead to an antagonistic behavior (dose elevation vs dose reduction or vice versa).
Limitations
The only limitation of the present study was that all INR measurements with CoaguChek XS coagulometer were performed by an experienced physician; however, in real practice patients measure their INR by their own.
Conclusion
The determination of INR using the CoaguChek XS device is very satisfactory compared with the standard laboratory (STAGO STA-R) method. In our experience, the CoaguChek XS coagulometer has the potential to significantly optimize the routine INR monitoring of patients who are on oral anticoagulation with VKA.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors report nonfinancial support from Roche Diagnostics Turkey A.Ş. during the conduct of the study. Roche Diagnostics Turkey A.Ş. has supported CoaguChek XS strips used in this study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.