
Abstract
We analyzed a cohort of 36 females with pregnancy loss. In addition to 11 patients with antiphospholipid antibody syndrome and 2 patients with congenital antithrombin (AT) or protein C deficiency, we identified 5 patients with low fibrinogen levels (median 110 mg/dL) prior to 10 weeks of gestation. Four of these 5 patients underwent a fibrinogen gene analysis, and all 4 were found to be heterozygotes for the α-fibrinogen (FGA) Thr321Ala polymorphism. One female without hypofibrinogenemia with a history of 8 pregnancy losses was found to be homozygous for the same polymorphism, and she also showed hypercoagulability without thrombosis. In conclusion, there was a relatively high frequency of pregnancy loss in the setting of hypofibrinogenemia and/or the FGA Thr312Ala polymorphism, and this may be an important risk factor for pregnancy loss and a hypercoagulable state in later pregnancy.
Keywords
Introduction
Pregnancy is characterized as a proinflammatory and hypercoagulable state, with miscarriage occurring in approximately 15% of pregnancies. In contrast, recurrent miscarriage is a rather rare condition with an estimated incidence of 1% to 3%. 1 Although genetic factors are the major causes of spontaneous miscarriage, they are less frequently associated with recurrent miscarriage. Although autoimmune-based recurrent miscarriage has been described, including primarily antiphospholipid antibody syndrome (APS), 2,3 the role of alloimmune mechanisms remains poorly understood. The current treatment of patients with APS during pregnancy includes heparin and aspirin, which prevent clot formation and subsequently improve live birth rates. Nevertheless, other obstetric morbidities remain high, especially in patients with a history of thrombotic events. 2 In addition to classical thrombotic placental events, other factors involving inflammation and complement activation appear to play a role in certain complications. However, the influence of parameters associated with congenital thrombophilia, such as abnormalities in antithrombin (AT), protein C (PC), or protein S (PS), 4 is controversial. 1
The α-fibrinogen (FGA) Thr312Ala 5 polymorphism occurs in a region important for factor XIII-dependent cross linking 6 and may therefore affect the clot structure or the degree of rigidity. Hypofibrinogenemia is caused by a variety of structural abnormalities in the fibrinogen molecule which result in a tendency toward bleeding and thrombosis as well as obstetric complications. The obstetric complications of hypofibrinogenemia include first-trimester pregnancy loss, hemorrhage, placental abruption, and thrombosis. 7,8 A significant association between FGA Thr312Ala and poststroke mortality was observed in patients with atrial fibrillation, with increased mortality in those possessing Ala312 versus those homozygous for Thr312. 9 This fibrinogen polymorphism is also associated with venous thromboembolism (VTE). 10
In this study, hemostatic abnormalities were examined in 36 pregnant females who experienced pregnancy loss, and gene analyses for fibrinogen were performed in 4 of 5 patients with hypofibrinogenemia.
Materials and Methods
Thirty-six women who had experienced pregnancy loss were examined at Mie University School of Medicine between January 1, 2007, and February 28, 2015. The median age (25%-75% tile) was 32.5 years (30.0-36.0 years), and the median number of abortions was 2.0 (1-3). There were 11 patients with APS, 2 patients with systematic lupus erythematosus, 1 patient with idiopathic thrombocytopenic purpura (ITP), 1 patient with Sjögren’s syndrome, 1 patient with congenital AT deficiency, 1 patient with congenital PC deficiency, and 1 patient with plasminogen deficiency (Table 1). The hemostatic abnormalities were also examined in 20 patients with ITP without pregnancy loss with a median age of 30.0 years (28.0-32.8 years). The diagnosis of APS was made according to the established criteria. 11 The fibrinogen level which was less than 150 mg/dL either before or in the very early phase of pregnancy in the patients without liver dysfunction or disseminated intravascular coagulation was considered to indicate a state of hypofibrinogenemia. The study protocol was approved by the Human Ethics Review Committee of the Mie University School of Medicine, and signed informed consent was obtained from each participant. The study was faithfully carried out in accordance with the principles of the Declaration of Helsinki.
Patients With Pregnancy Loss.
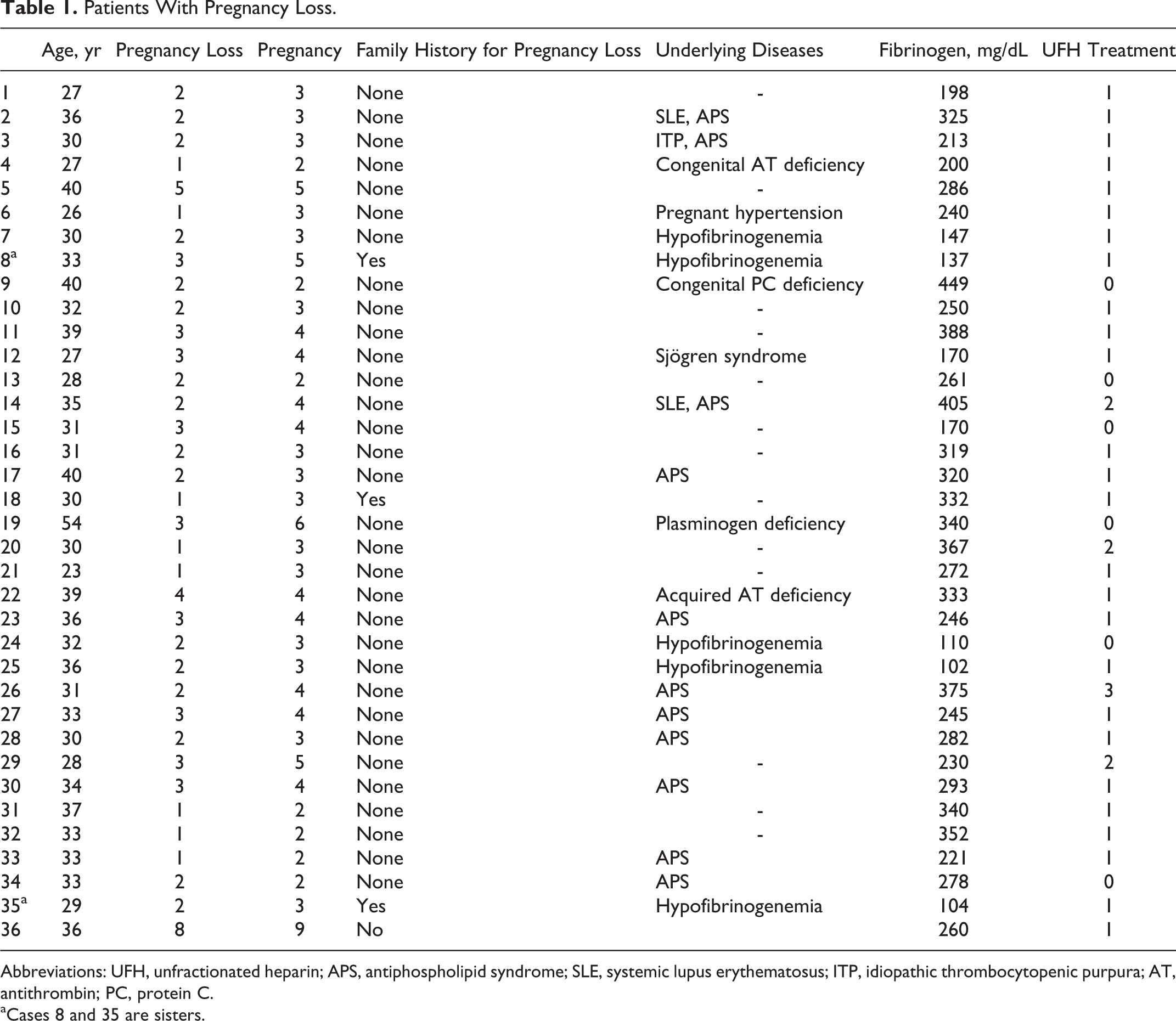
Abbreviations: UFH, unfractionated heparin; APS, antiphospholipid syndrome; SLE, systemic lupus erythematosus; ITP, idiopathic thrombocytopenic purpura; AT, antithrombin; PC, protein C.
aCases 8 and 35 are sisters.
The level of lupus anticoagulant (LA) was measured using diluted Russell viper venom time based on a LA test, the “Guardipore” (Medical and Biological Laboratories CO, LTD [MBL], Nagoya, Japan). The titers of anticardiolipin immunoglobulin G (IgG) antibodies (aCL-IgG) and anticardiolipin β2-GPI complex antibodies were measured according to an enzyme-linked immunosorbent assay using an MESACUP cardiolipin IgG test (MBL) and anti-CL β2GPI kit Yamasa enzyme immunoassay (Yamasa Shoyu Co, Tyoushi, Japan). 12 The concentration of fibrinogen was measured by thrombin time method using a datafi fibrinogen kit (Sysmex, Kobe, Japan), a turbidimetric immunoassay (TIA) using a N-assay TIA Fib kit (Nittobo, Koriyama, Japan), and the heat precipitation method. 11,13
A gene analyses of all 3 fibrinogen genes (FGA, β-, and γ-fibrinogen, respectively) was performed using the cycle sequencing method. Genomic DNA was prepared from peripheral blood leukocytes using a QIAamp DNA Blood Mini Kit (QIAGEN, Tokyo, Japan) according to the manufacturer’s instructions. Each exon, including the exon–intron boundary of the gene, was amplified from genomic DNA via polymerase chain reaction (PCR). The PCR products were directly sequenced using a Big-Dye Terminator Cycle Sequencing Kit and a 310 or 3130 Genetic Analyzer (Applied Biosystems, Foster City, California).
Statistical Analysis
The data are expressed as the median and 25th to 75th percentiles. Differences between the groups were examined for significance using the McNemar test. A P value of less than .05 was considered to indicate a significant difference. All statistical analyses were performed using the Stat flex, version 6, software package (Artec Co Ltd, Osaka, Japan).
Results
There were 11 patients with APS who had experienced pregnancy loss. Ten of the 11 patients with APS were pregnant and received treatment with aspirin and unfractionated heparin (UFH), and all patients either had a healthy baby or maintained a normal pregnancy (Table 1). Although no relationships between positive findings for antiphospholipid antibody (aPL) and the number of pregnancy losses were observed, the patients triple positive results for aPL-developed thrombosis (Table 2). In 35 cases, the pregnant females were treated with UFH because of elevation in
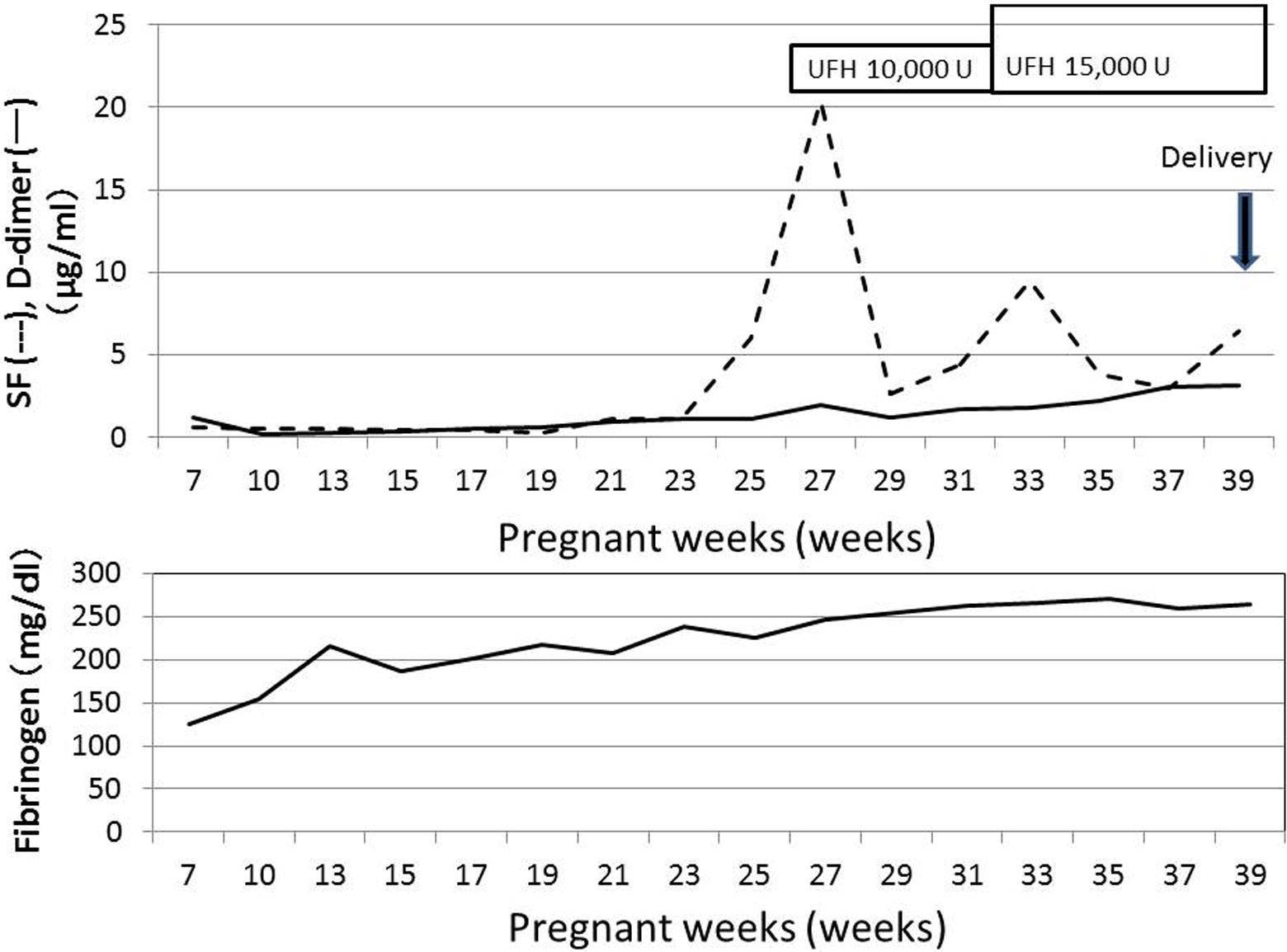
Plasma levels of SF,
Antiphospholipid Antibodies.
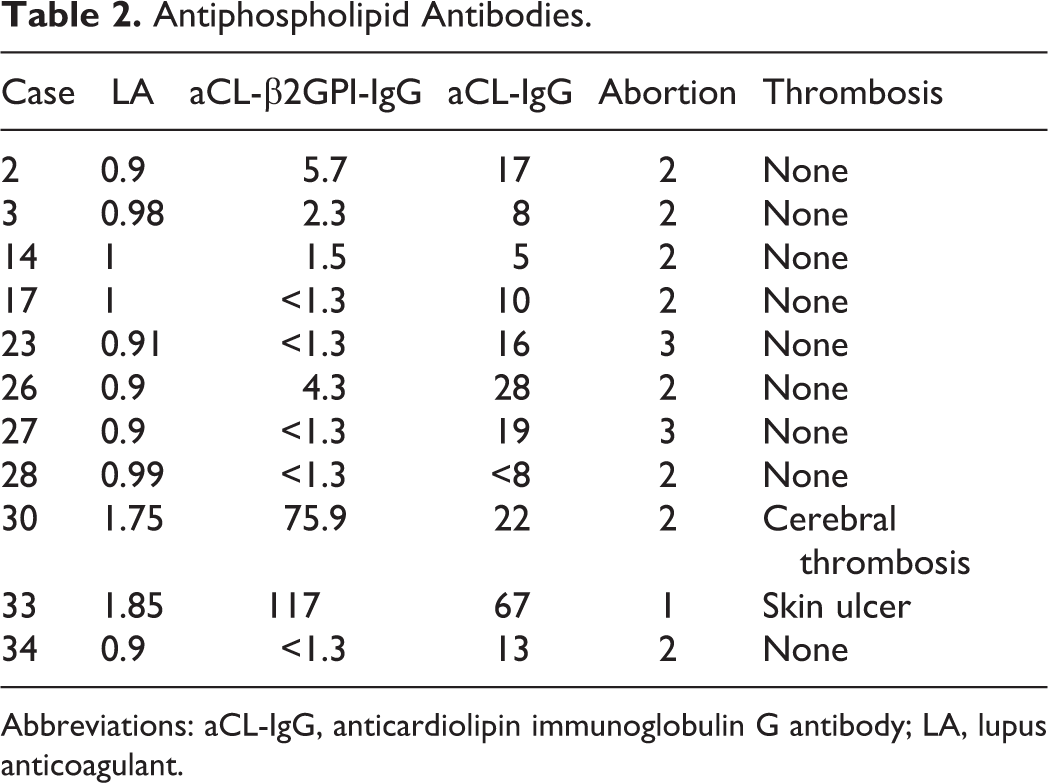
Abbreviations: aCL-IgG, anticardiolipin immunoglobulin G antibody; LA, lupus anticoagulant.
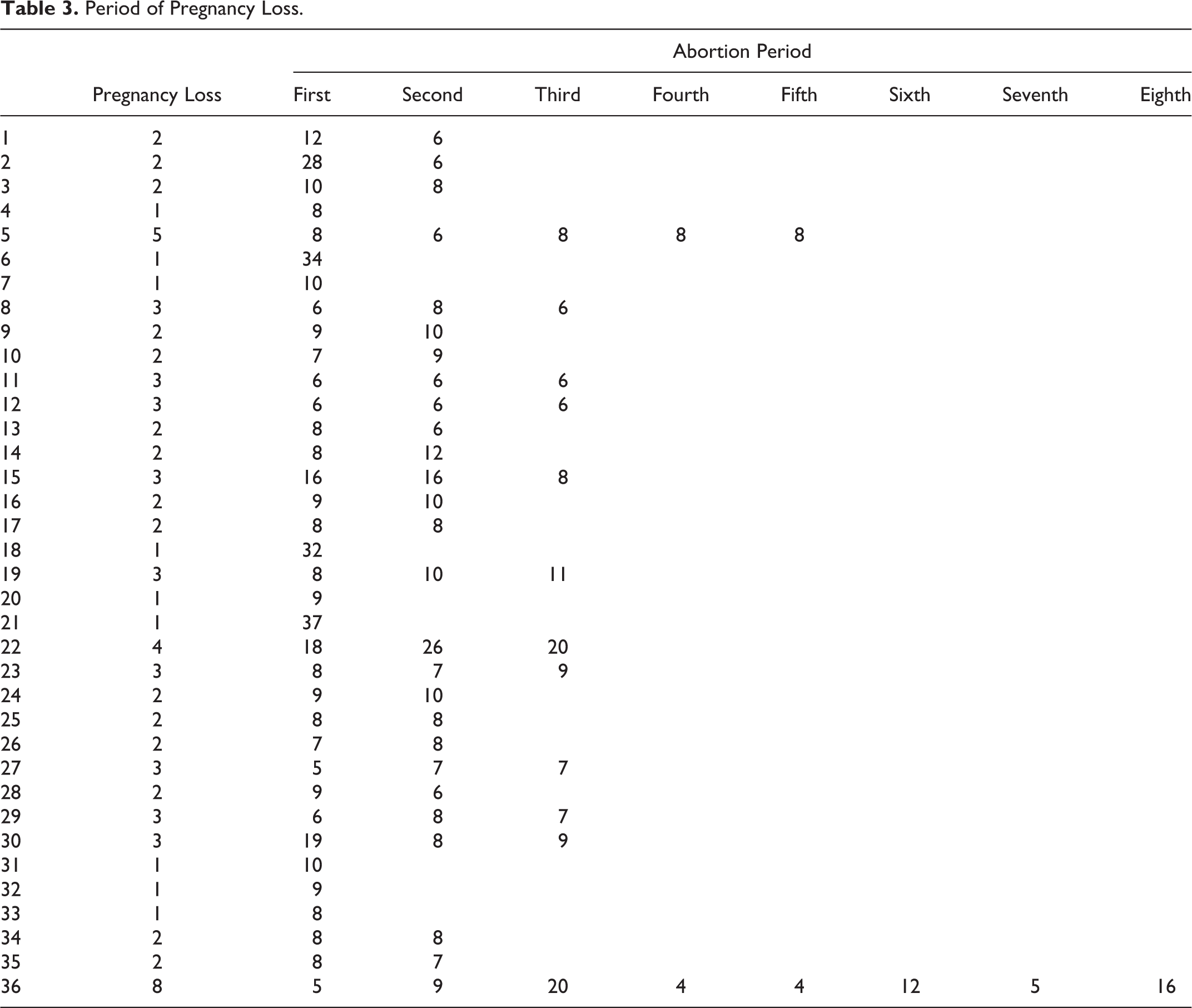
Period of Pregnancy Loss.
Patients With Hypofibrinogenemia and Case 36.
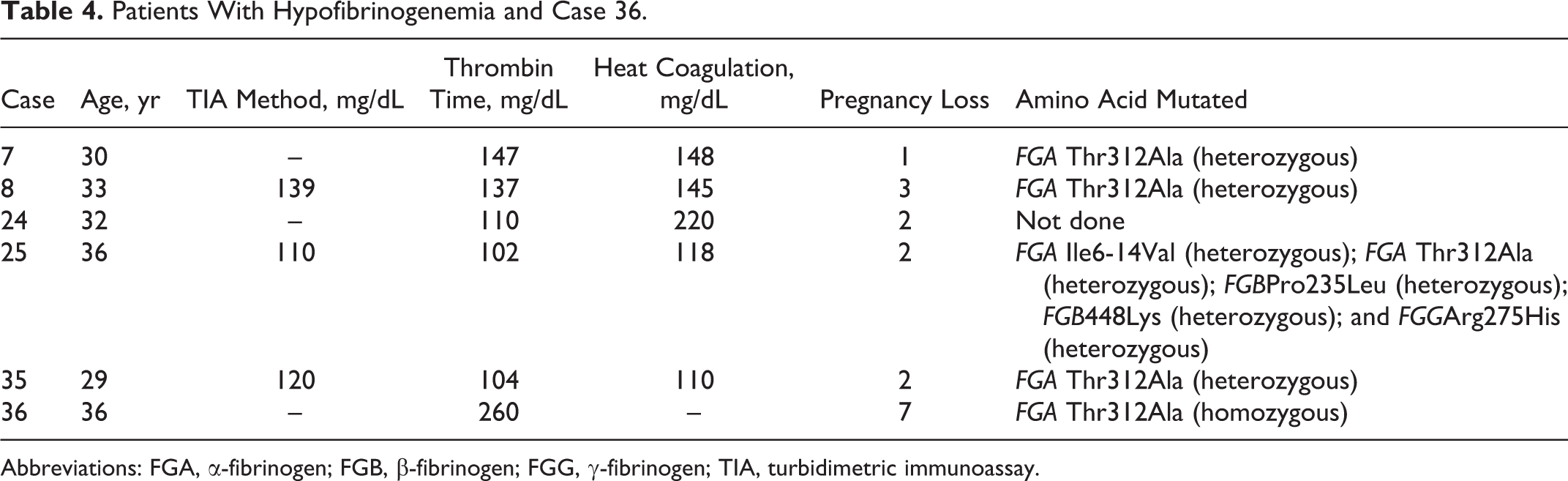
Abbreviations: FGA, α-fibrinogen; FGB, β-fibrinogen; FGG, γ-fibrinogen; TIA, turbidimetric immunoassay.
There were no cases of hypofibrinogenemia, APS, AT deficiency, or PC deficiency among the 20 pregnant females with ITP without pregnancy loss, and the frequency of combination treatment with hypofibrinogenemia and FGA Thr312Ala was significantly higher (P < .001) in the females with pregnancy loss than in the pregnant females with ITP without pregnancy loss.
According to an analysis of the frequency of FGA Thr312Ala, 13 (86.7%) of 15 patients had pregnancy loss, 20 (83.3%) of 24 patients had deep vein thrombosis (DVT), and 40 (81.6%) of 49 patients had prosthetic valves.
Discussion
In this study, 11 patients exhibited APS, suggesting that APS is one of the most important causes of recurrent miscarriage. A causative relationship between aPLs and recurrent early miscarriage (prior to 10 weeks of gestation) is supported by many studies, 14 and treatment with heparin and low-dose aspirin is associated with favorable pregnancy outcomes. 15 In the current study, UFH therapy was associated with a favorable pregnancy outcome in 34 of 35 cases, including 2 cases who have successfully maintained their pregnancy after UFH treatment. These findings suggest that the status of aPL is not related to the frequency of abortion, but triple positive finding for aPL is associated with thrombosis. Abnormal AT or PC levels have also been suggested to correlate with thrombosis but not directly with pregnancy loss. The findings of 5 pregnant females in 4 families with hypofibrinogenemia among 36 pregnant females who experienced pregnancy loss indicate a markedly high frequency. All 5 patients had pregnancy loss before 10 weeks of gestation. Although these patients were not treated with fibrinogen concentrate, fibrinogen concentrate may be recommended for females with a fibrinogen level of less than 150 mg in very early phase of pregnancy. In addition, UFH should not be administrated to pregnant women with a fibrinogen level of less than 150 mg/dL. Although the relationship between a heterozygous status for afibrinogenemia and pregnancy loss has not been reported, the relationship combination of hypofibrinogenemia and heterozygous of FGA Thr312Ala with pregnancy loss has not been clarified. Because the plasma fibrinogen level increases in pregnancy, it is difficult to diagnose hypofibrinogenemia in pregnant females.
In the gene analyses of 4 patients with hypofibrinogenemia, all patients were found to have a heterozygous of FGA Thr312Ala. One female with homozygous FGA Thr312Ala experienced pregnancy loss 7 times. These findings suggest that more than 2 abnormalities of fibrinogen may make it difficult to maintain the placenta in a good condition.
This fibrinogen polymorphism has been reported to be a strong risk factor, such as intracerebral hemorrhage, 16 chronic thromboembolic pulmonary hypertension, 17 and VTE 18 as well as myocardial infarction and ischemic stroke. 19 In Japan, FGA Thr312Ala in cases involving pregnancy loss is rarely reported. The frequency of FGA Thr312Ala polymorphism was reported to be 46.5% in Japanese 20 and 29.9% in Europeans. 21 According to the findings of our study, this frequency was high in patients with pregnancy loss, those with DVT, and those with prosthetic valves. Complications with FGA Thr312Ala and hypofibrinogenemia were observed in all 4 patients who had pregnancy loss, thus suggesting that such complications may be closely associated with pregnancy loss.
The patients in cases 8 and 35 were sisters, both of whom experienced pregnancy loss in the early period of pregnancy and consequently received UFH treatment for hypercoagulability in later pregnancies. In addition, both patients experienced a normal delivery after receiving treatment with UFH, suggesting that this fibrinogen abnormality may cause both bleeding tendency and thrombosis.
In conclusion, the frequency of complications with FGA Thr312Ala and hypofibrinogenemia is relatively high, and such complications may be associated with pregnancy loss in early pregnancy and hypercoagulability in later pregnancy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a Grant-in-Aid from the Ministry of Health, Labour and Welfare of Japan for Blood Coagulation Abnormalities and the Ministry of Education, Culture, Sports, Science and Technology of Japan.