
Abstract
Background:
Current disseminated intravascular coagulation (DIC) criteria are insufficient for predicting mortality. Hemostatic endothelial molecular markers are useful for DIC diagnoses. We aimed to design new DIC criteria involving these markers based on the recently published Japanese Association for Acute Medicine (JAAM) DIC criteria, which exhibit higher sensitivity for mortality.
Materials and Methods:
Patients with severe sepsis or septic shock admitted to a tertiary referral hospital in Japan between September 2009 and November 2011 were included. Clinical data, including hemostatic endothelial molecular markers, were measured within 12 hours after admission. Receiver operating characteristic analyses were conducted for 8 candidate variables to identify the mortality-related markers. Then, we designed new unified criteria based on the JAAM DIC criteria and involving the identified optimal markers.
Results:
Of the 79 patients, 66 (83.5%) survived and 13 (16.5%) died. Protein C activity correlated best with mortality with a very high prognostic value (area under the curves [AUCs] = 0.850; P < .001), followed by plasminogen activator inhibitor 1 (AUC = 0.828; P < .001). The unified criteria, consisting of the JAAM DIC criteria plus these 2 markers, exhibited greater prognostic value for mortality (sensitivity, 84.6%; specificity, 80.3%). Moreover, DIC-positive patients using the unified criteria had significantly higher disease severity, as indicated by the Acute Physiology and Chronic Health Evaluation II and Sequential Organ Failure Assessment scores.
Conclusion:
Our unified criteria involving hemostatic endothelial molecular markers reflected not only mortality but also the severity of illness in patients with severe sepsis.
Introduction
Sepsis invariably leads to hemostatic abnormalities, which range from insignificant coagulopathy to disseminated intravascular coagulation (DIC). Among patients with severe sepsis, the mortality of patients without DIC is approximately 20% to 30%. This figure almost doubles (40%-45%) in patients with DIC, suggesting that complications related to DIC result in poorer outcomes in these patients. 1 –4 The DIC is characterized by the widespread formation of fibrin thrombosis, microvascular occlusion, and reduced oxygen delivery to cells and tissues, leading to multiple organ dysfunction syndrome. 5 Therefore, DIC associated with sepsis is a syndrome that should be diagnosed and treated early.
The initial definition and concept of DIC were based on the associated pathological states; however, there has been a gradual shift to clinical laboratory test-based definitions. Until now, 3 diagnostic criteria for DIC based on general coagulation tests and clinical symptoms have been widely used and reported to be useful: the DIC diagnostic criteria established by the Japanese Ministry of Health and Welfare (JMHW) 6 and the Japanese Association for Acute Medicine (JAAM) 7 in addition to the International Society of Thrombosis and Hemostasis (ISTH) overt-DIC diagnostic criteria. 8 However, there are limitations to these criteria. The JMHW DIC and ISTH overt-DIC criteria include a decrease in the fibrinogen level, which occurs relatively infrequently in septic DIC. The JAAM DIC diagnostic criteria, which include the systemic inflammatory response syndrome (SIRS) criteria, demonstrate better sensitivity, but not specificity, for septic DIC. Consequently, evidence of the ability of these criteria to accurately predict mortality in patients with DIC remains limited. Therefore, new diagnostic criteria with greater sensitivity and specificity and a subsequent ability to decrease mortality need to be established.
Hemostatic molecular markers such as thrombin antithrombin (TAT) complex and plasmin-α2 plasmin inhibitor complex are reported to be useful for the diagnosis of early phase DIC. 9,10 In the pathophysiology of sepsis-induced DIC, the endothelium plays a pivotal role in the hemostatic and fibrinolytic processes through the regulated synthesis and release of endothelial-derived proteins. 11 –13 In the present study, we prospectively evaluated the predictive value of these molecular markers for mortality in sepsis-induced DIC and the utility of modified JAAM DIC criteria that included additional significant molecular markers.
Materials and Methods
Study Sample
Data were collected from the Department of Emergency and Critical Care, Osaka General Medical Center, Japan, over a period of 26 months from September 2009 to November 2011 as part of the prospective observational study that evaluated the diagnostic value of maximal chemiluminescent intensity in patients with sepsis, the primary results of which have been reported by Kiguchi et al. 14 The inclusion criteria were severe sepsis or septic shock diagnosed on admission and age >18 years. Severe sepsis and septic shock were defined according to the definitions set by the American College of the Chest Physicians/Society of Critical Care Medicine consensus conference. 15 In addition, patients were included only when baseline routine and central laboratory data for DIC determination were available. The exclusion criterion was end-stage cancer. All patients were typically treated according to the Surviving Sepsis Campaign Guidelines, 16 and we also administered recombinant human thrombomodulin to treat patients with sepsis-induced DIC. We did not use antithrombin, immunoglobulin, and polymyxin B hemoperfusion as adjunctive therapy for severe sepsis/septic shock.
This study followed the principles of the Declaration of Helsinki, and the institutional review board at the Osaka General Medical Center approved the study. Informed consent was obtained from all patients or the next of kin if patients were unconscious.
Data Collection
Patients were followed up until hospital discharge or death. Data included age, gender, site of infection, C-reactive protein levels, the Acute Physiology and Chronic Health Evaluation (APACHE) II score, and the Sequential Organ Failure Assessment (SOFA) score. Multiple organ dysfunction syndrome (MODS) was defined as a SOFA score >12 points. 17
A whole-blood sample was collected within 12 hours of admission. Immediately after the blood sampling, we measured platelet counts, prothrombin time (PT), fibrinogen levels, fibrin/fibrinogen degradation products (FDPs),
The primary outcome was in-hospital mortality. We also evaluated intensive care unit (ICU)-specific outcomes including the number of ICU-free and ventilator-free days. Namely, we evaluated ventilator-free days as the number of days to day 28 that the patient achieved unassisted breathing, assuming that the patient survived to 28 days and did not require assisted breathing. Patients who did not survive to 28 days were assigned 0 ventilator-free days. The ICU-free days were evaluated in a similar manner.
Disseminated Intravascular Coagulation Scoring Systems
We calculated the JAAM DIC and ISTH overt-DIC scores. The JAAM DIC scoring system was published in 2005, it includes global coagulation tests and SIRS scores. 18
The ISTH overt-DIC definitions were adopted as proposed by Taylor et al, for platelet counts, PT, and fibrinogen level. 8 The FDP values were chosen as the fibrin-related marker and scored according to the cutoff levels and ranges recently published by Gando et al (no increase, moderate increase, and strong increase were defined as FDP values <10, 10-25, and >25 mg/L, respectively). 19
Statistical Analysis
Baseline characteristics are summarized as group medians with interquartile ranges for continuous variables and frequencies with percentages for categorical variables. Differences between groups were assessed using the Mann-Whitney U test and chi-square test or Fisher exact test, as appropriate.
To identify the markers that distinguished nonsurviving from surviving patients with sepsis, receiver operating characteristic (ROC) analyses were constructed for PT, fibrinogen, FDP,
Then, we established a new unified scoring system involving optimal markers as determined earlier and evaluated whether or not the predictive value of the JAAM DIC scoring system was improved by adding parameters through ROC analysis. The ROC analysis was also performed to assess the optimal weighting of protein C activity and PAI-1 in the JAAM DIC scoring system to yield maximal discrimination. The area under the curve (AUC) of this new unified scoring system was compared to the JAAM and ISTH overt-DIC scoring systems using the method by DeLong et al. 21 Finally, a Kaplan-Meier survival curve with the log-rank method was determined for survival analysis of the new DIC scoring system.
A P < .05 was set for statistical significance. Statistical analyses were conducted using SPSS v17.0 (IBM Corp., Armonk, New York) or SAS v.9.3 (SAS Institute Inc, Cary, North Carolina).
Results
Patient Characteristics
During the study period, 79 patients fulfilled the inclusion criteria. Baseline characteristics of the study population are shown in Table 1. All patients were admitted to the ICU via the emergency department. The origin of sepsis included the abdomen (n = 25, 31.6%), urinary tract (n = 23, 30.3%), soft tissue (n = 15, 19.0%), lung (n = 11, 13.9%), and others (n = 5, 6.3%).
Baseline Characteristics of the Study Sample Comprised of Patients With Severe Sepsis or Septic Shock Diagnosed on Admission.a
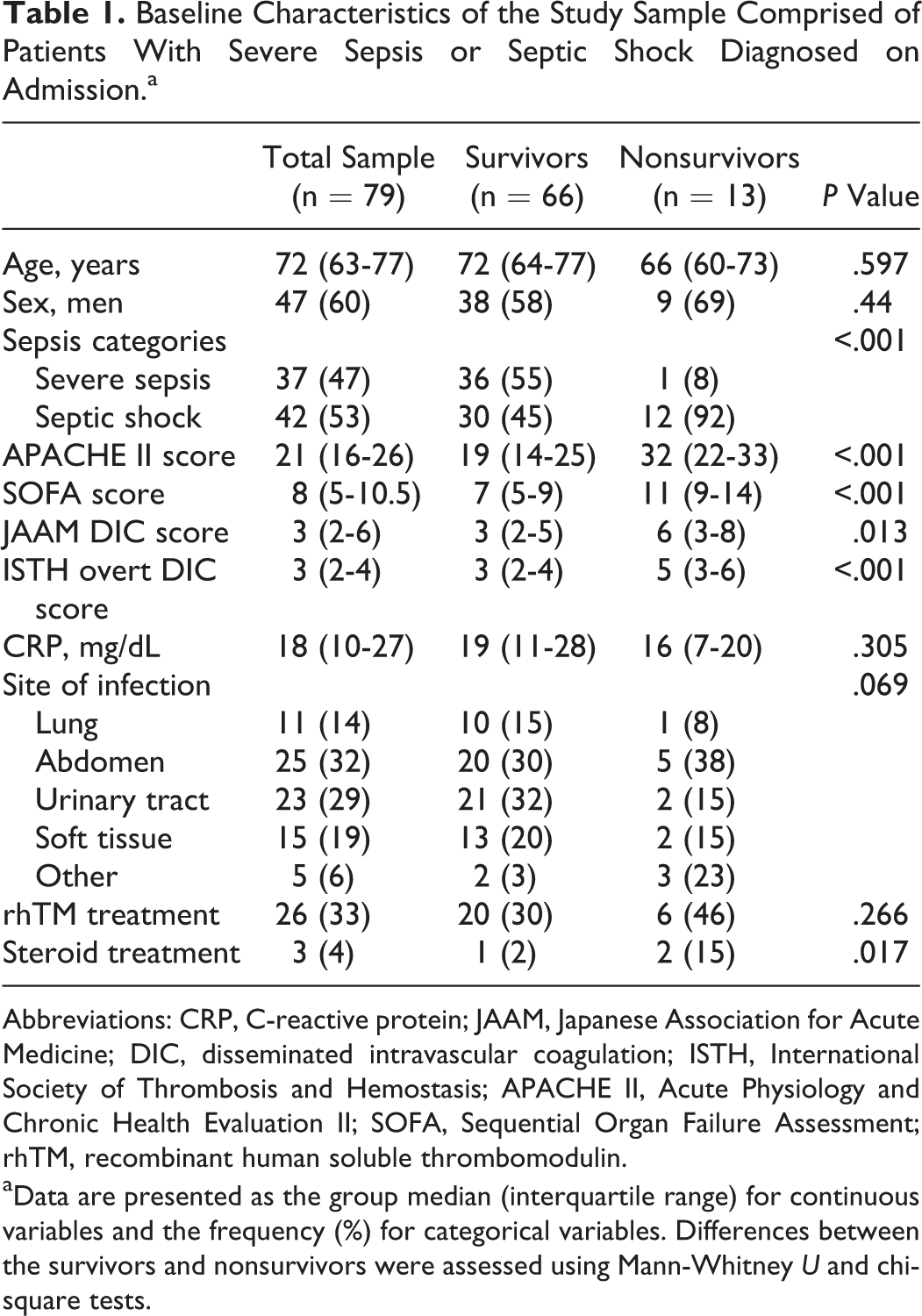
Abbreviations: CRP, C-reactive protein; JAAM, Japanese Association for Acute Medicine; DIC, disseminated intravascular coagulation; ISTH, International Society of Thrombosis and Hemostasis; APACHE II, Acute Physiology and Chronic Health Evaluation II; SOFA, Sequential Organ Failure Assessment; rhTM, recombinant human soluble thrombomodulin.
aData are presented as the group median (interquartile range) for continuous variables and the frequency (%) for categorical variables. Differences between the survivors and nonsurvivors were assessed using Mann-Whitney U and chi-square tests.
Of the 79 patients, 42 (53.1%) fulfilled the criteria for septic shock, 66 (83.5%) survived to discharge, and 13 (16.5%) died. There were no significant differences in age, gender, origin of sepsis, or CRP levels between survivors and nonsurvivors. The severity of illness, as indicated by the APACHE II and SOFA scores, was significantly higher in the nonsurvivors than in the survivors. In addition, both the JAAM DIC and ISTH overt-DIC scores were significantly higher in the nonsurvivors compared with the survivors.
Receiver Operating Characteristic Analysis of Biomarkers
The ROC analyses revealed that protein C activity and PAI-1 had excellent abilities to predict mortality (AUC = 0.850 and 0.828, respectively; Table 2 and Figure 1). The optimal cutoff point for PAI-1, as calculated using the Youden index, was 150 ng/mL. In addition, because the Youden index for protein C activity exhibited a bimodal distribution, we selected 2 optimal cutoff points (20% and 40%) for protein C activity.
Comparison of AUC for Prediction of Mortality in Patients With Severe Sepsis or Septic Shock.
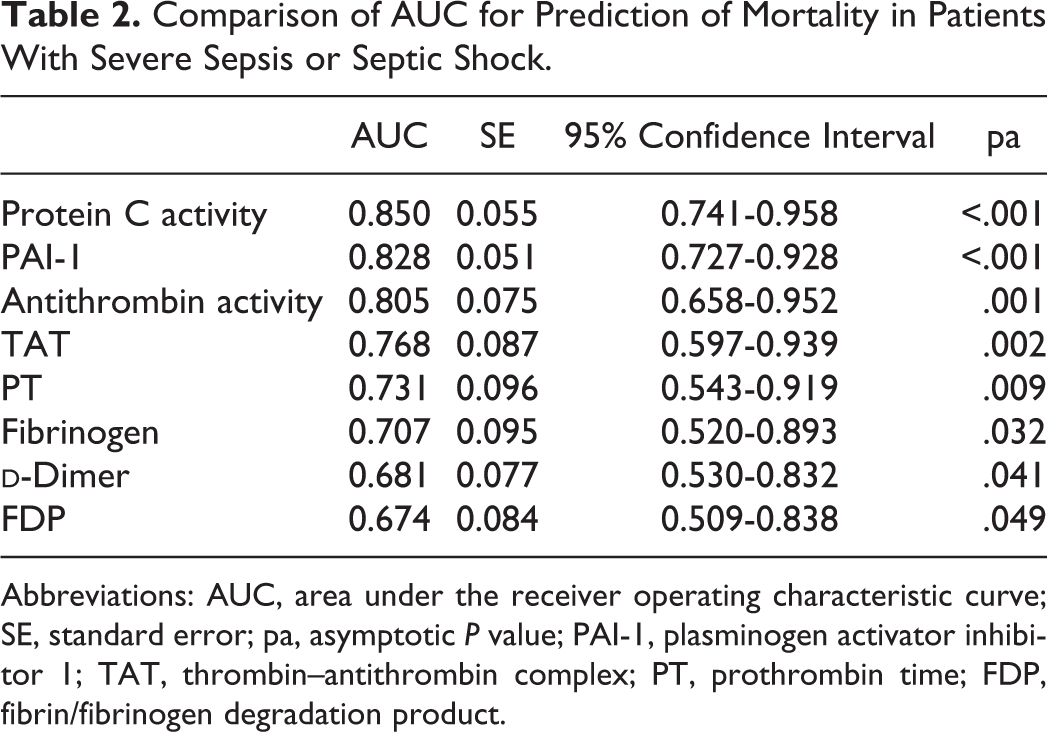
Abbreviations: AUC, area under the receiver operating characteristic curve; SE, standard error; pa, asymptotic P value; PAI-1, plasminogen activator inhibitor 1; TAT, thrombin–antithrombin complex; PT, prothrombin time; FDP, fibrin/fibrinogen degradation product.
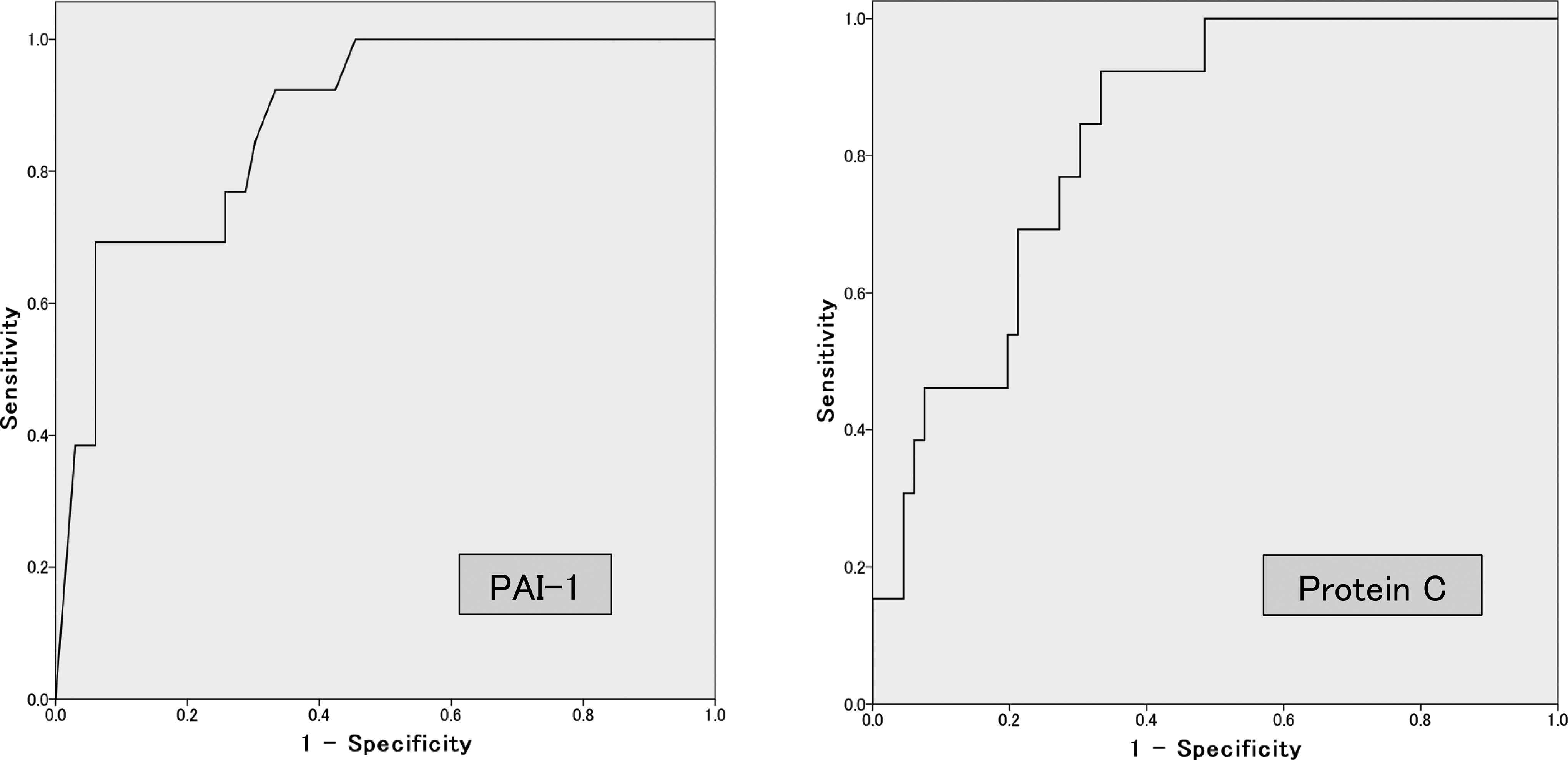
Receiver operating characteristic (ROC) curves for protein C activity and plasminogen activator inhibitor 1 (PAI-1) as predictors of mortality in patients with severe sepsis or septic shock.
A New Unified DIC Scoring System
Owing to the predictive abilities for mortality of the 2 molecular markers, the PAI-1 (>150 ng/mL = 0 points and <150 ng/mL = 3 points) and protein C activity (>40% = 0 points, 20%-40% = 1 point, and <20% = 3 points) components were then added to the JAAM DIC scoring system, and we constructed a new unified scoring system (Table 3).
The Unified Criteria Based on the JAAM DIC Criteria, With Protein C Activity and PAI-1 Components Added Based on Our Analysis.
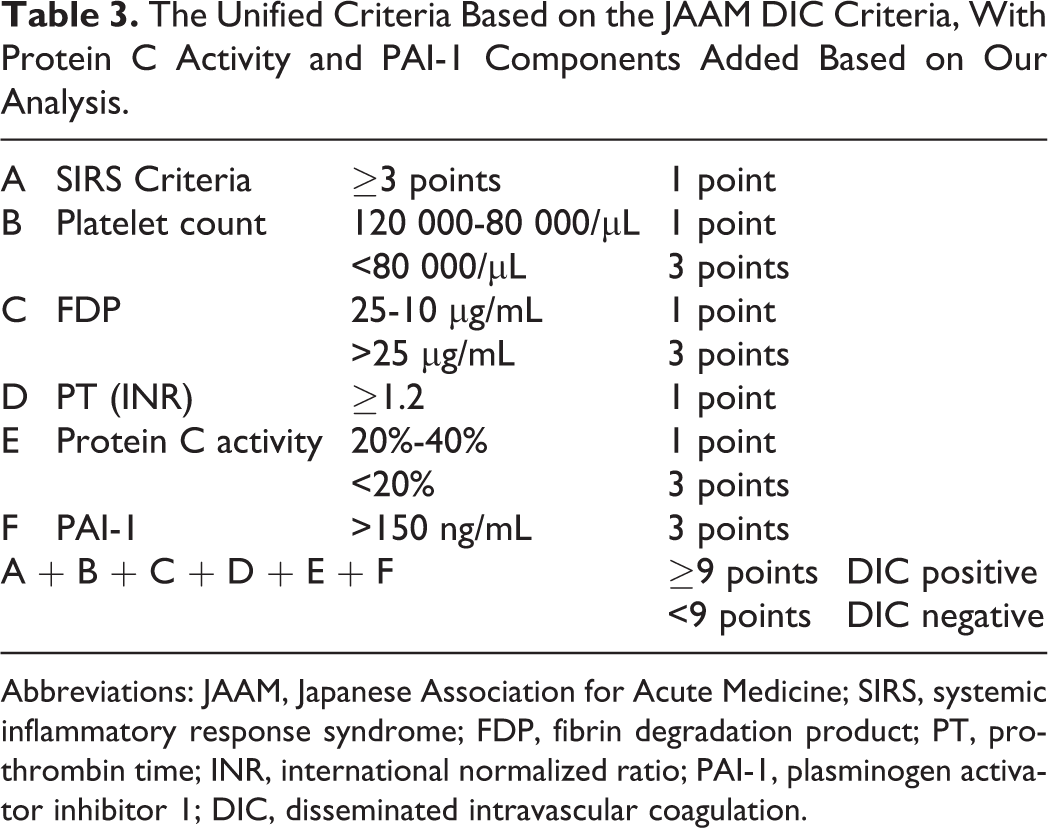
Abbreviations: JAAM, Japanese Association for Acute Medicine; SIRS, systemic inflammatory response syndrome; FDP, fibrin degradation product; PT, prothrombin time; INR, international normalized ratio; PAI-1, plasminogen activator inhibitor 1; DIC, disseminated intravascular coagulation.
Figure 2 shows the ROC curves of the JAAM DIC, ISTH overt-DIC, and unified DIC scoring systems for predicting hospital mortality. The AUC for the unified scoring system was 0.864 (95% confidence interval [CI] 0.737-0.991), which was superior to that of the JAAM (AUC, 0.717; 95% CI 0.555-0.879; P < .001), as shown in Table 4. The calculated Youden index resulted in an optimal cutoff point for the unified scoring system of 9 points. At this cutoff, the sensitivity for mortality was 84.6%, and the specificity was 80.3% (Table 5).
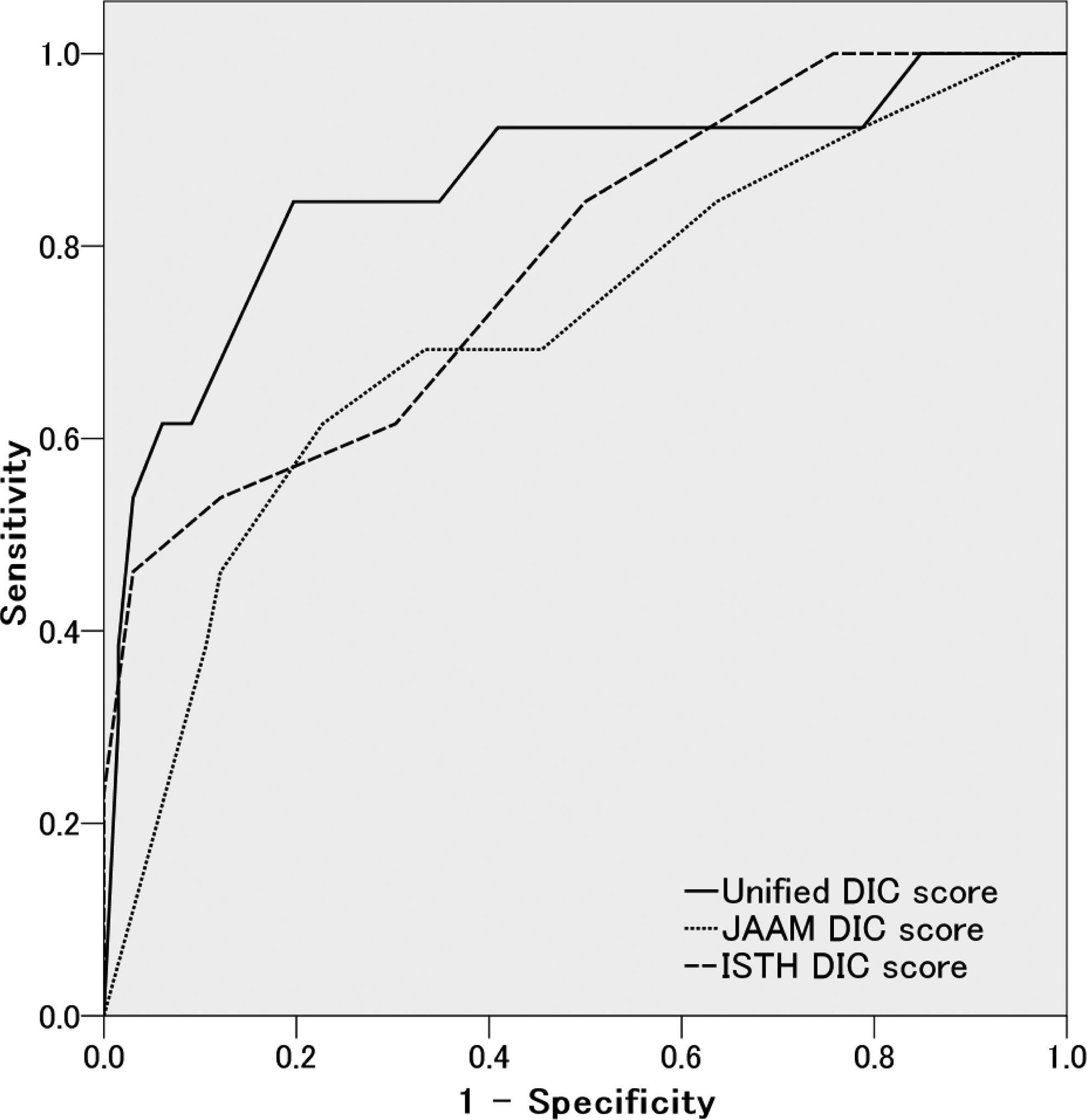
Receiver operating characteristics (ROC) curves for each disseminated intravascular coagulation (DIC) scoring system, measuring the ability to predict mortality in patients with severe sepsis or septic shock. The solid line represents the unified scoring system, the dashed line represents the Japanese Association for Acute Medicine (JAAM) DIC scoring system, and the dotted line represents the International Society of Thrombosis and Hemostasis (ISTH) DIC scoring system.
Comparison of the AUC for the Ability of Each DIC Scoring System to Predict Mortality in Patients With Severe Sepsis or Septic Shock.
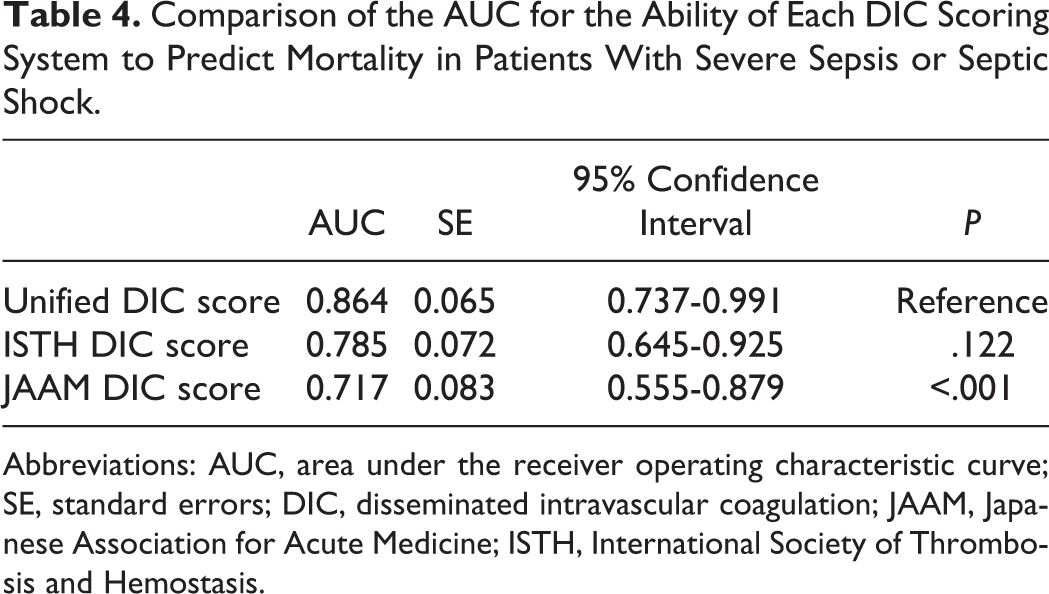
Abbreviations: AUC, area under the receiver operating characteristic curve; SE, standard errors; DIC, disseminated intravascular coagulation; JAAM, Japanese Association for Acute Medicine; ISTH, International Society of Thrombosis and Hemostasis.
Correlation Between Each Cutoff Point of the Unified Scoring System and Mortality.a
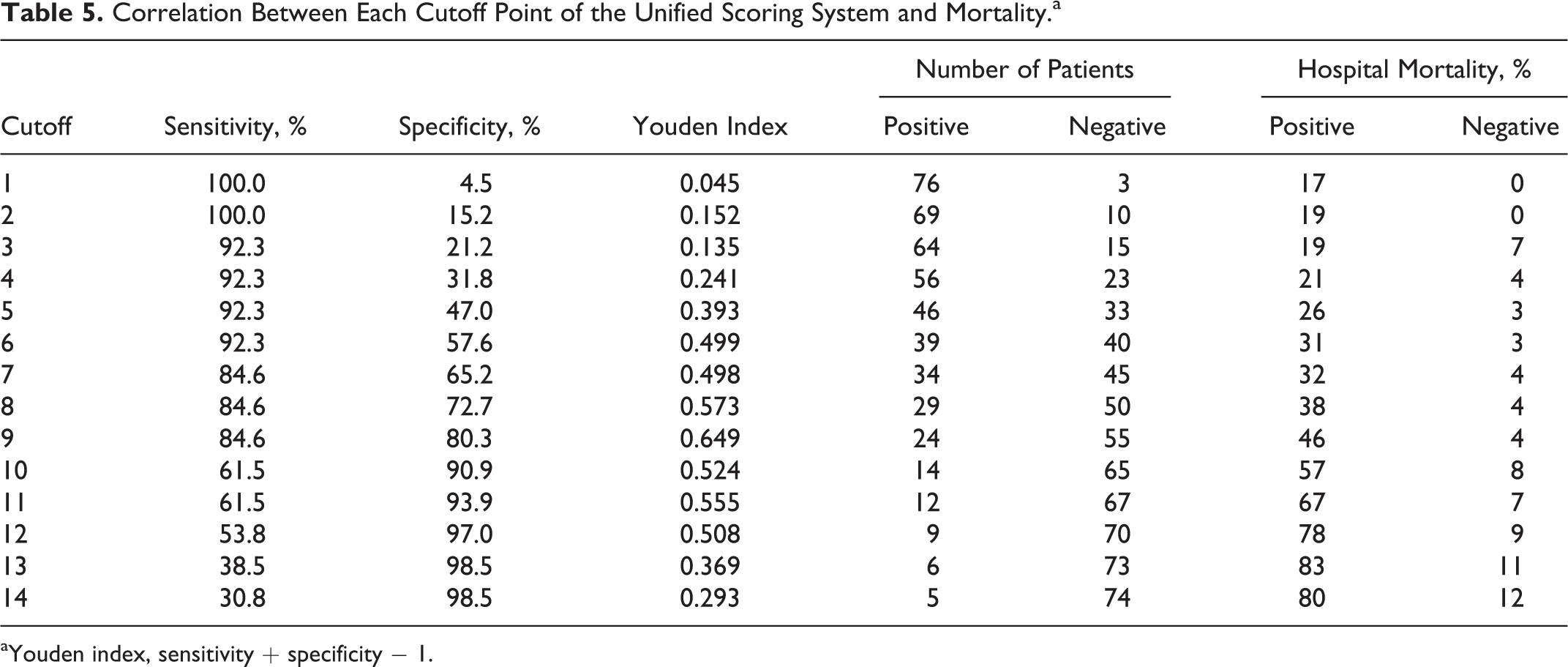
aYouden index, sensitivity + specificity − 1.
Survival Analysis
In this sample, 24 patients were DIC positive using the unified criteria (Table 6). There were no significant differences in age, gender, or CRP between the DIC-positive and DIC-negative patients. The mortality and severity of illness, as indicated by the APACHE II and SOFA scores, were significantly higher in the DIC-positive patients. The survival curves derived using the Kaplan-Meier method demonstrated that the survival rate of the DIC-positive patients was significantly lower than that of the DIC-negative patients (log rank test, P < .001) as shown in Figure 3.
Comparison of the Characteristics Between the DIC and Non-DIC Patients Diagnosed With the Unified Criteria.a
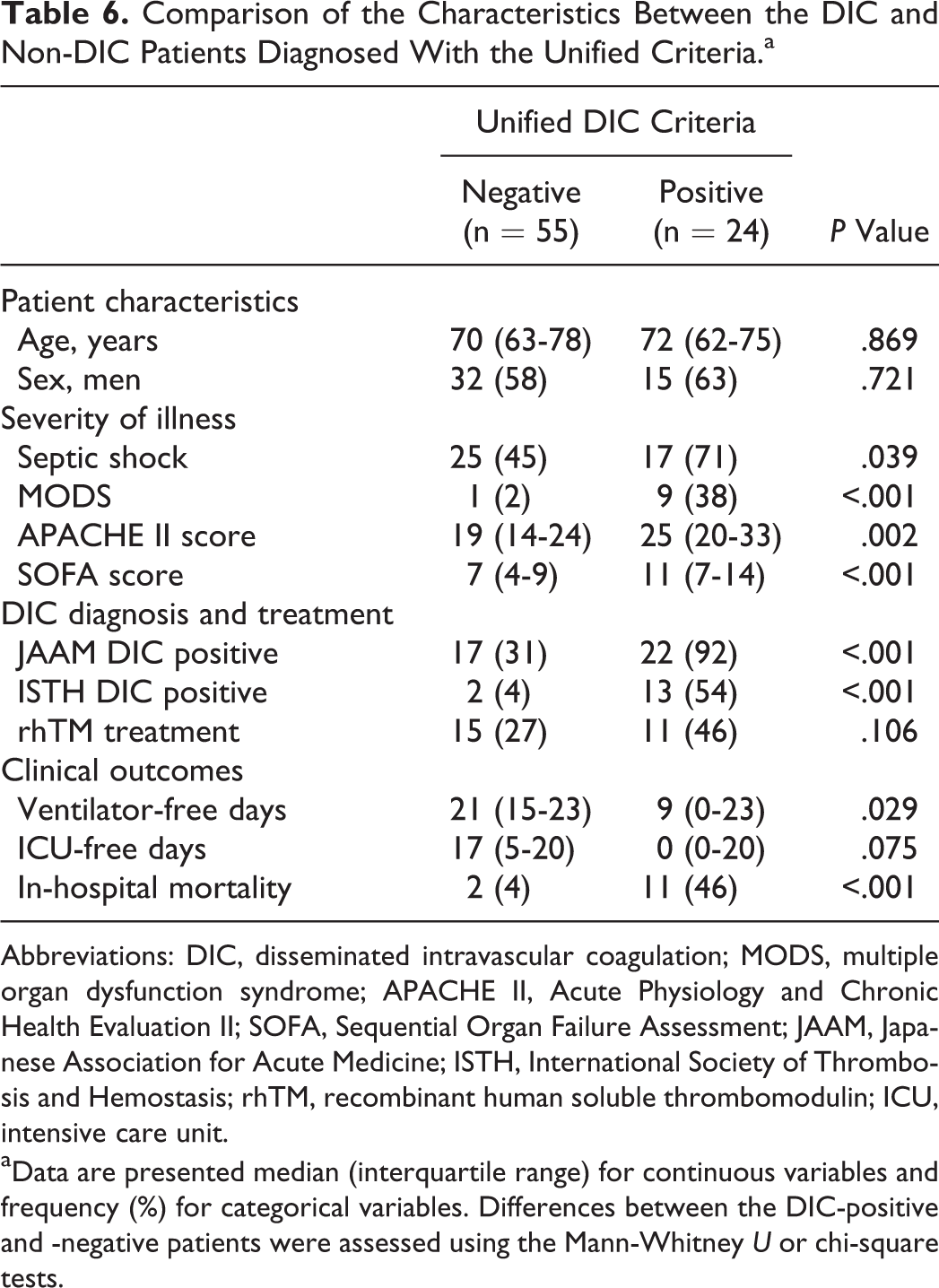
Abbreviations: DIC, disseminated intravascular coagulation; MODS, multiple organ dysfunction syndrome; APACHE II, Acute Physiology and Chronic Health Evaluation II; SOFA, Sequential Organ Failure Assessment; JAAM, Japanese Association for Acute Medicine; ISTH, International Society of Thrombosis and Hemostasis; rhTM, recombinant human soluble thrombomodulin; ICU, intensive care unit.
aData are presented median (interquartile range) for continuous variables and frequency (%) for categorical variables. Differences between the DIC-positive and -negative patients were assessed using the Mann-Whitney U or chi-square tests.
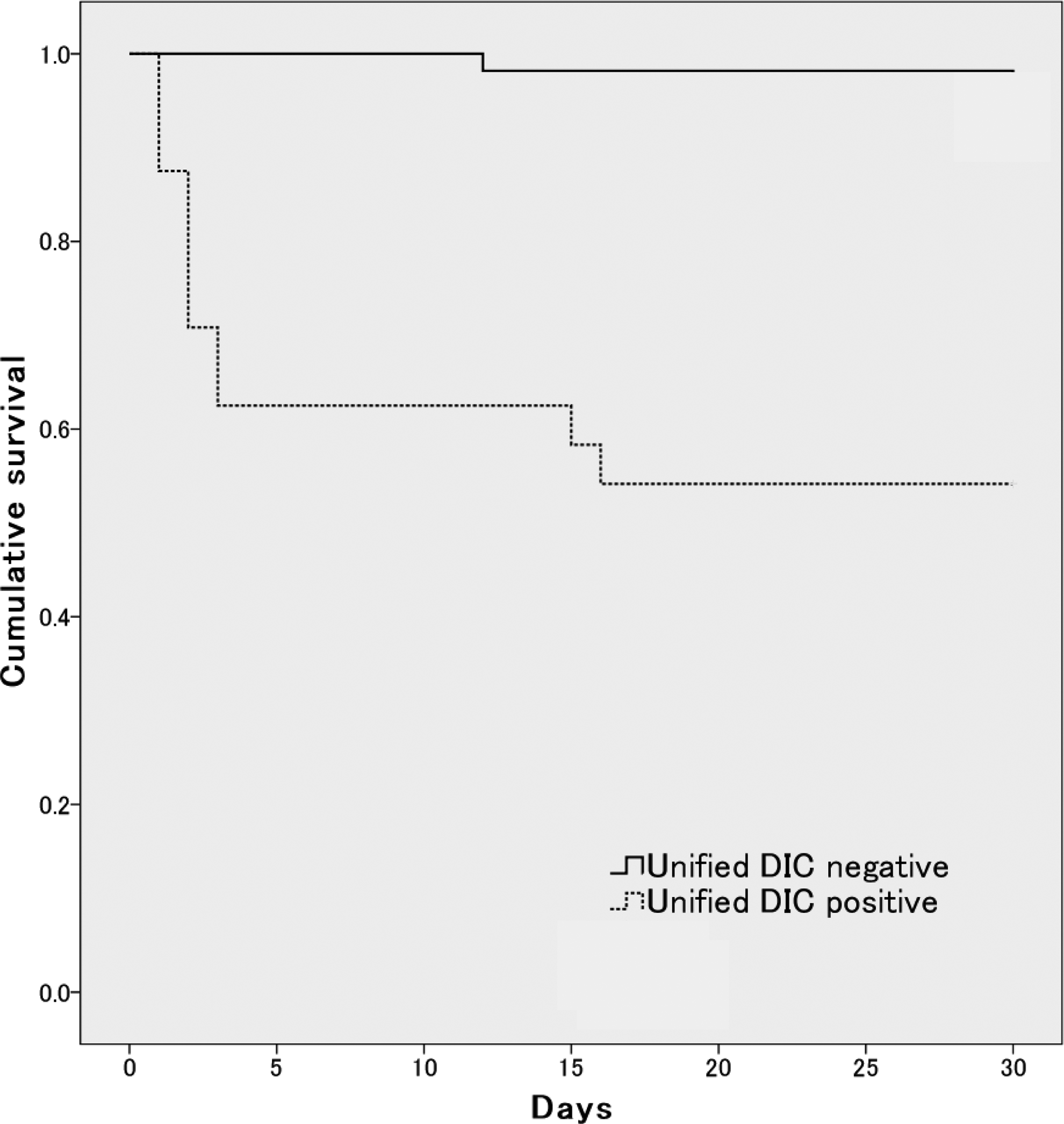
Kaplan-Meier survival curves for patients with disseminated intravascular coagulation (DIC) and non-DIC patients determined using the unified criteria that was developed using this study sample, based on the Japanese Association for Acute Medicine (JAAM) criteria. The solid line represents the non-DIC patients, and the dotted line represents the DIC patients. The DIC patients had significantly higher mortality (log rank test, P < .001).
Discussion
Although the DIC subcommittee of the Scientific Standardized Committee in the ISTH has emphasized that vascular endothelial cell injury is involved in the pathogenesis of DIC, 8 scoring systems based on the current and widely used diagnostic criteria do not reflect vascular endothelial cell injury. The results of the present study provide evidence that protein C activity and PAI-1, which are hemostatic endothelial molecular markers, were predictive of mortality in severe sepsis, and the unified DIC scoring system involving these molecular markers exhibited excellent prognostic value in patients with severe sepsis.
According to the ROC analysis, of the measured hemostatic molecular markers, protein C activity and PAI-1 were the best predictors of mortality, with very high prognostic values (AUCs = 0.850 and 0.828, respectively), followed by the other hemostatic molecular markers such as antithrombin activity and TAT. Conversely, the global coagulation markers were inferior to these hemostatic endothelial molecular markers in their abilities to predict mortality. Previous studies have indicated that changes in hemostatic molecular markers often occur in patients with organ dysfunction. 9 –12,22,23 Similarly, the present results clearly demonstrate that vascular endothelial cell injury is predictive of the outcome in sepsis-induced DIC.
In 2001, the ISTH proposed a set of nonovert-DIC diagnostic criteria that included some of the hemostatic endothelial molecular markers; however, the cutoff for each item in these criteria had not been defined. 8 Therefore, several modified versions of the nonovert-DIC diagnostic criteria have been proposed. 24,25 Wada et al reported that their modified nonovert-DIC diagnostic criteria, which removed the points for a negative change in the global coagulation test and added points for antithrombin activity and the fibrin monomer complex or TAT, had better sensitivity and specificity. However, the sensitivity and specificity for mortality were 86.2% and 32.8%, respectively, which were similar to those for the JAAM DIC criteria (80.0% and 33.2%, respectively 26 ) that were established to diagnose early phase septic DIC. The unified JAAM scoring system developed in the present study demonstrated greater sensitivity and specificity (84.6% and 80.3%, respectively) than both of these earlier criteria. Furthermore, the ROC analysis resulted in an AUC for the unified scoring system of 0.864, which was also superior to that of the JAAM DIC criteria.
There are several potential reasons for the superior performance of the newly developed unified scoring system. First, the clinical characteristics of the patients varied depending on the type of DIC and underlying disease in the previous studies, while the present study included only patients with severe sepsis; the unified scoring system was based on the JAAM DIC criteria, which was specifically established to diagnose the early phase of septic DIC. Second, PAI-1 is a key indicator of fibrinolysis suppression, which is an important factor in the pathogenesis of sepsis and may predispose patients with severe sepsis to poorer outcomes. 27,28 To the best of our knowledge, no previous DIC criteria included PAI-1; however, the use of PAI-1 is the most logical modification considering the widely accepted role of PAI-1 in sepsis.
In the present study, the DIC-positive patients, as identified using our unified criteria, scored higher on the APACHE II and SOFA and had higher rates of mortality, MODS, and septic shock compared to the DIC-negative patients. These results support those of a previous study using the JAAM criteria, in which Gando et al reported that patients with DIC had more severe illness than patients without DIC. 19 The newly developed unified criteria not only predicted mortality but also reflected the severity of illness in patients with septic DIC. In addition, the unified criteria performed significantly better in terms of specificity for mortality than did the JAAM DIC criteria, on which the unified criteria were based. Although there is no universal consensus regarding the management of sepsis-induced DIC, previous studies have suggested that the ideal management of DIC requires early additional supportive treatment that specifically targets the coagulation disorder. 29 However, as the diagnosis and treatment of DIC in this study were not based on the unified DIC criteria, we cannot comment on the usefulness of the unified criteria for DIC treatment. Nevertheless, as we found that the unified criteria enabled the successful diagnosis of patients who were at high-risk of death due to sepsis-induced DIC, our unified DIC criteria may be useful in the clinical decision making for early initiation of DIC treatment.
Despite the utility of our unified scoring system, this study has certain limitations. First, the single-center design resulted in a relatively small sample size, which may have influenced the findings of this study. Second, to investigate the utility of the unified scoring system using a single population, only internal validation was performed. Therefore, we are planning a prospective external validation to verify the utility of the unified scoring system. Third, measurement of the hemostatic endothelial molecular markers is costly and occurs only in specialized laboratories; therefore, the widespread implementation of our unified scoring system in clinical practice may not be feasible.
Conclusion
We demonstrated that protein C activity and PAI-1 were predictive of mortality in patients with severe sepsis. Moreover, the addition of these molecular markers to the JAAM DIC criteria, which resulted in a new unified DIC scoring system, resulted in greater prognostic value than the JAAM DIC alone in patients with severe sepsis. Further clinical investigations are necessary to verify the utility of this new unified scoring system.
Footnotes
Authors’ Note
Y. Umemura participated in the study design, data collection, and interpretation and drafted the manuscript. K. Yamakawa conceived and designed this study, and critically appraised the manuscript. T. Kiguchi and Y. Yoshikawa participated in study design and data collection. H. Ogura and T. Shimazu participated in the data interpretation. T. Hamasaki performed the statistical analysis and helped to draft the manuscript. S. Fujimi had a major impact on the interpretation of data and critical appraisal of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.