
Abstract
There is accumulating evidence that the coagulation system is involved in the process of fibrogenesis in chronic liver disease. Recent studies postulated a possible connection between plasmatic hypercoagulability and progression of fibrosis. The aim of the study was to investigate disorders of the coagulation system in patients with chronic hepatitis C having different extent of hepatic fibrosis well defined by liver histology. A total of 62 patients with chronic hepatitis C were recruited and categorized into 2 groups according to their histological fibrosis stage : mild/moderate fibrosis group (F0-F3 group, n = 30) and extensive fibrosis/cirrhosis group (F4-F6 group, n = 32). The control group consisted of 31 healthy individuals. The following hemostatic assays were evaluated: antithrombin III (AT), protein C (PC) activity, activated partial thromboplastin time, prothrombin time, plasma fibrinogen as well as conventional liver function test. The PC level exhibited a significant reduction in both patient groups when compared to the normal control group (89.25% ± 10.05% and 48.33% ± 15.86% vs 111.86 ± 10.90; P < .001 and P < .001). The PC was found to be the strongest associated factor to histological fibrosis stage (r = –.834; P < .0001). Univariate and multivariate analysis showed that AT (P = .003) and PC (P = .0001) were the most important factors associated with advanced fibrosis. The PC (P = .001) was found to be the only predictor of mild fibrosis. In conclusion, PC deficiency occurs in an early stage of liver fibrosis. The severity of deficiency is proportional to extent of fibrosis. The PC may have a key role in linking hypercoagulability with hepatic fibrogenesis in chronic liver disease.
Introduction
The development of hepatic fibrosis following chronic parenchymal injury is considered to be a complex disease, and there are several recognized factors influencing the process of fibrogenesis. 1 –4 Among them, the coagulation system appears to be particularly involved.
Advanced liver disease is commonly associated with variable coagulation disorders including marked decrease in procoagulant factors 5 –7 as well as their anticoagulant counterparts, namely, protein C (PC) and antithrombin III (AT), due to impaired synthesis. 8 –11 Despite the fact that cirrhosis is characterized by a prolongation of conventional coagulation tests, clinical observations have shown that these patients are not protected of thrombotic events. Moreover, recent in vitro studies have even shown a procoagulant imbalance in patients with cirrhosis. 12,13
Evidence suggests that a hypercoagulant state in advanced liver disease is linked to progression of fibrosis. These findings are supported by clinical studies showing an association between activated PC resistance and acquired PC deficiency and advanced liver fibrosis in patients with hepatitis C virus (HCV) infection. 14 –17 However, the exact link between coagulation and hepatic fibrogenesis is still unclear.
In the present study, we determined conventional coagulation screening tests including AT and PC anticoagulant activity in patients with chronic HCV infection and variable stage of fibrosis as confirmed by liver histology.
We aimed to prove whether disorders of the coagulation system could be observed at an early stage of liver disease in patients with chronic HCV infection as well as their possible association with the extent of hepatic fibrosis.
Materials and Methods
Study Patients
In the period from November 2007 to March 2013, we recruited 65 consecutive patients referred to the Department of Gastroenterology and Hepatology of the University Clinical Center Sarajevo for chronic hepatitis C infection. Patients included in the study signed formal informed consent. The study protocol was approved by the Institutional Ethics Committee of the University Clinical Center of Sarajevo.
All 65 patients had a percutaneous liver biopsy. Three individuals were excluded from the study due to inadequate liver specimens as defined previously on the basis of no portal tracts identified or small sample size.
The diagnosis of chronic viral hepatitis was based on biochemical tests and positive RNA polymerase chain reaction assays and confirmed by liver biopsy.
Exclusion criteria were as follows: previous antiviral or immunomodulatory therapy, hepatocellular carcinoma or other known malignancy, other chronic liver disease, history of portal vein thrombosis or deep venous thrombosis, and current anticoagulant therapy.
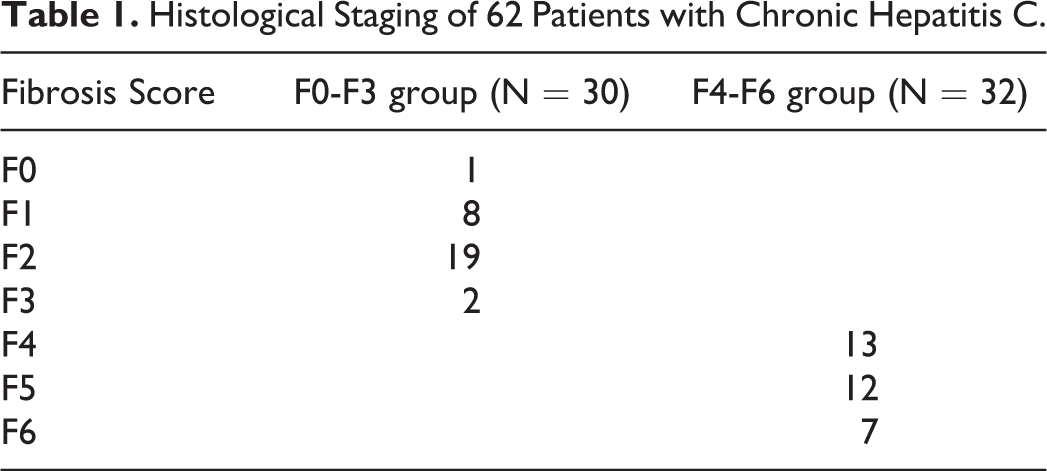
The patients were divided into 2 groups. The first group (F0-F3 group, n = 30, 15 men and 15 woman) included patients diagnosed with chronic viral hepatitis C and histological findings of mild/moderate fibrosis (Ishak fibrosis score F0, F1, F2, and F3). The second group (F4-F6 group, n = 32, 27 men and 5 woman) consisted of patients with extensive fibrosis or cirrhosis in the histological findings (Ishak fibrosis score F4, F5, and F6; Table 1).
Histological Staging of 62 Patients with Chronic Hepatitis C.
A control group consisting of 31 healthy individuals (17 men and 14 woman) with normal results of physical examination and laboratory blood findings was selected from the general public.
Men were significantly more common in the F4-F6 group (men 27 [84%] vs woman 5 [15.6%]), whereas gender distribution was not significantly different between the F0-F3 and the healthy control group.
The mean age at the time of the study was significantly higher in the F4-F6 patient group than in the F0-F3 group (median 49 years [range 28-65] vs 43 years [range 19-62]; Table 2).
Demographic and Biochemical Characteristics of Healthy Controls and Patients With Chronic Hepatitis C.a
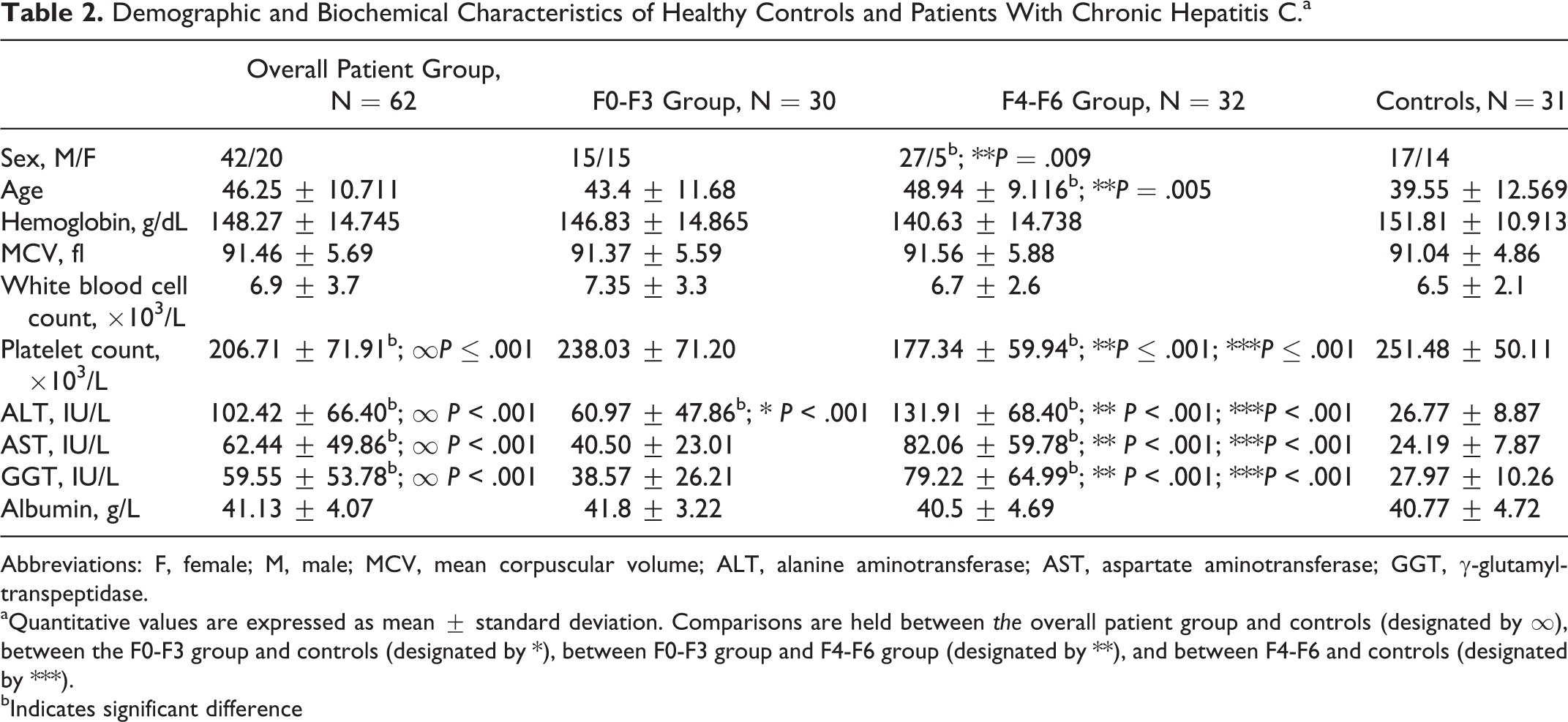
Abbreviations: F, female; M, male; MCV, mean corpuscular volume; ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, γ-glutamyl-transpeptidase.
aQuantitative values are expressed as mean ± standard deviation. Comparisons are held between the overall patient group and controls (designated by ∞), between the F0-F3 group and controls (designated by *), between F0-F3 group and F4-F6 group (designated by **), and between F4-F6 and controls (designated by ***).
bIndicates significant difference
Laboratory Assays
Blood samples were obtained from each patient on the first day of admission to our department. Blood samples were collected by venipuncture directly into vacuum tubes containing trisodium citrate. The blood samples tubes were centrifuged at 2.000g for 15 minutes at room temperature. The assays were performed on fresh plasma or on aliquots, which were immediately stored at –70°C until analysis was performed.
Full blood count, including platelet count, albumin levels, and liver function tests (alanine aminotransferase [ALT], aspartate aminotransferase [AST], and γ-glutamyl-transpeptidase[GGT]) were performed using commercially available assays.
Coagulation screening tests included activated partial thromboplastin time (aPTT) and prothrombin time expressed as international normalized ratio (INR), which were performed by the conventional methods. Plasma fibrinogen was measured by the turbidimetric method of Clauss (Dade Fibrinogen Determination Reagents, Dade Behring, Marburg, Germany). Natural anticoagulants were analyzed using commercial reagent kits according to the manufacturer’s instructions: Activities of AT were determined by colorimetric assay (Berichrom AT III, Dade Behring, Marburg, Germany) and PC activity by kinetic testing (Berichrom C, Dade Behring, Marburg, Germany). Anticoagulant activity was expressed in percentage with a reference range of 75% to 125% for AT III and 70% to 140% for PC.
Histological Evaluation
Liver biopsy specimens were fixed in Bouin liquid, embedded in paraffin, and sections were stained in hematoxylin–eosin and Masson trichrome. Histological liver fibrosis was evaluated according to the classification system proposed by Ishak and colleagues. 18 The stage of fibrosis was assessed in 7 categories: F0 = no fibrosis, F1 = fibrous expansion of some portal areas, F2 = fibrous expansion of most portal areas, F3 = fibrous expansion of most portal areas with occasional portal to portal bridging, F4 = fibrous expansion of most portal areas with marked bridging, F5 = marked bridging with occasional nodules, and F6 = cirrhosis. Patients with extensive fibrosis or cirrhosis had F4, F5, or F6 scores and patients with no or limited fibrous expansion had F0, F1, F2 or F3 scores.
Statistical Analysis
Statistical analyses were carried out with SPSS (Version 16.0. Chicago, SPSS Inc). Descriptive and analytical statistics were applied using Student t test, analysis of variance, and Mann-Whitney U test to compare continuous variables between groups and chi-square test for categorical variables. Spearman rank correlation test was used to assess the strength of the relationship between continuous variables and histological staging. Univariate analysis was performed to identify variables associated with mild/extensive fibrosis, and multivariate analysis was performed using multiple regression models, where appropriate. A P value of <.05 was considered statistically significant for all tests.
Results
Histological fibrosis scores of 62 patients with chronic hepatitis C are presented in Table 1. The main characteristics of healthy controls (n = 31) and patients with chronic hepatitis C (n = 62) are presented in Table 2.
In patients with extensive fibrosis, mean platelet count was significantly lower (177.34 ± 59.94, P ≤ .001). Mean hemoglobin, mean corpuscular volume, and white blood cell counts showed no significant difference across all the study groups (Table 2).
Patients with extensive histological fibrosis had significantly higher levels of ALT, AST, and GGT (P < .001). At the same time, patients with mild/moderate fibrosis (F0-F3 patient group) only had significantly higher levels of ALT when compared to healthy controls (P < .001). Mean levels of AST and GGT did not show statistically significant difference. Albumin levels were not significantly different across all the groups (Table 2).
Analysis of Hemostatic Assays
The mean fibrinogen level showed no significant difference between the 2 groups of patients (3.17 ± 0.55 vs 3.11 ± 0.65 g/L; P = .78) in comparison with normal controls (3.21 ± 0.36 g/L; P = .48). A more prolonged aPTT (34.32 ± 4.24 vs 32.03 ± 2.73 seconds; P = .014) and INR (1.11% ± 0.12% vs 1.04% ± 0.10%; P = .047) was noted in patients with advanced fibrosis when compared to those with mild fibrosis stage. No significant prolongation of both INR and aPTT was noted in patients with mild fibrosis (F0-F3 group; Table 3).
Results and Comparison of Hemostatic Assays in Patients With Chronic Liver Disease and Controls.a
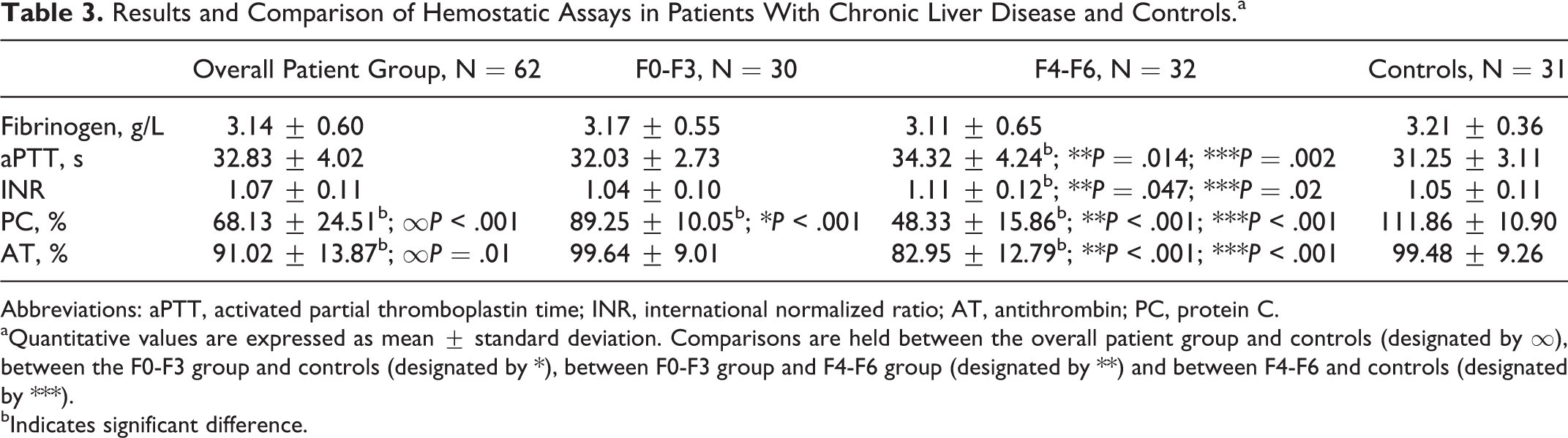
Abbreviations: aPTT, activated partial thromboplastin time; INR, international normalized ratio; AT, antithrombin; PC, protein C.
aQuantitative values are expressed as mean ± standard deviation. Comparisons are held between the overall patient group and controls (designated by ∞), between the F0-F3 group and controls (designated by *), between F0-F3 group and F4-F6 group (designated by **) and between F4-F6 and controls (designated by ***).
bIndicates significant difference.
The mean level of AT showed significant reduction in patients with extensive fibrosis (82.95% ± 12.79%) in comparison to mean level of patients with mild fibrosis (99.02% ± 13.87%; P < .001) and mean normal control level (99.48% ± 9.26%; P < .001). However, there was no significant decrease in AT levels in the F0-F3 group with mild liver fibrosis (99.64% ± 9.01%; P = .66).
At the same time, mean PC level exhibited a significant reduction in both patient groups when compared to normal control group (89.25% ± 10.05% and 48.33% ± 15.86% vs 111.86 ± 10.90; P < .001 and P < .001; Table 3). It is interesting to note that in patients with early stage of fibrosis, only PC levels showed significant decrease in comparison to the healthy control group.
Correlations Between Hemostatic Parameters, Liver Function Tests, and Histological Staging
Spearman test demonstrated significant correlations between AT level and fibrosis stage (r = –.615, P < .001) and PC level and fibrosis stage (r = –.834; P < .0001). Spearman test also yielded positive correlations between INR (r = .311; P = .014), aPTT (r = .398; P = .001), ALT (r = .538; P = .0001), AST (r = .481; P = .0001), GGT (r = .410; P = .001), and stage of fibrosis. Among these variables, PC was found to be the strongest associated factor to histological fibrosis stage. On the other hand, levels of albumin and fibrinogen were not correlated with fibrosis stage (P > .05; Table 4).
Spearman Rank Correlation Test of Liver Fibrosis Stage on Hemostatic and Liver Function Tests in Patients With Chronic Viral Hepatitis C.a
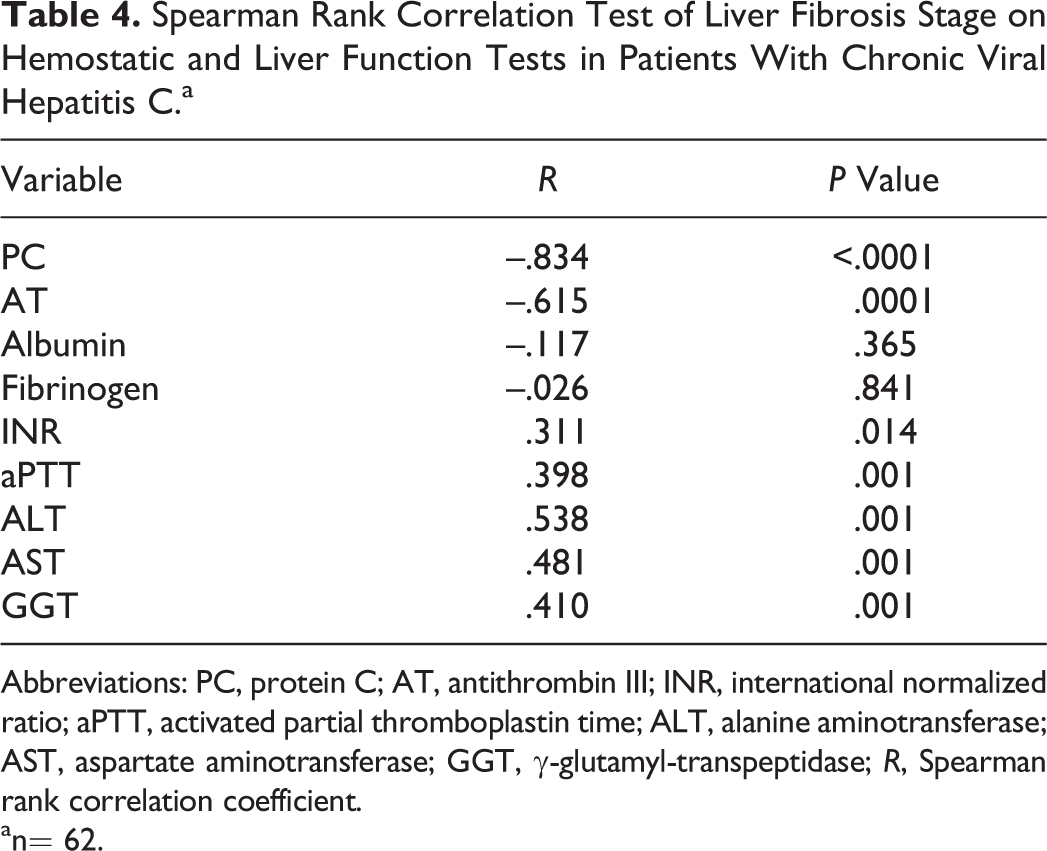
Abbreviations: PC, protein C; AT, antithrombin III; INR, international normalized ratio; aPTT, activated partial thromboplastin time; ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, γ-glutamyl-transpeptidase; R, Spearman rank correlation coefficient.
an= 62.
Univariate and Multivariate Analyses
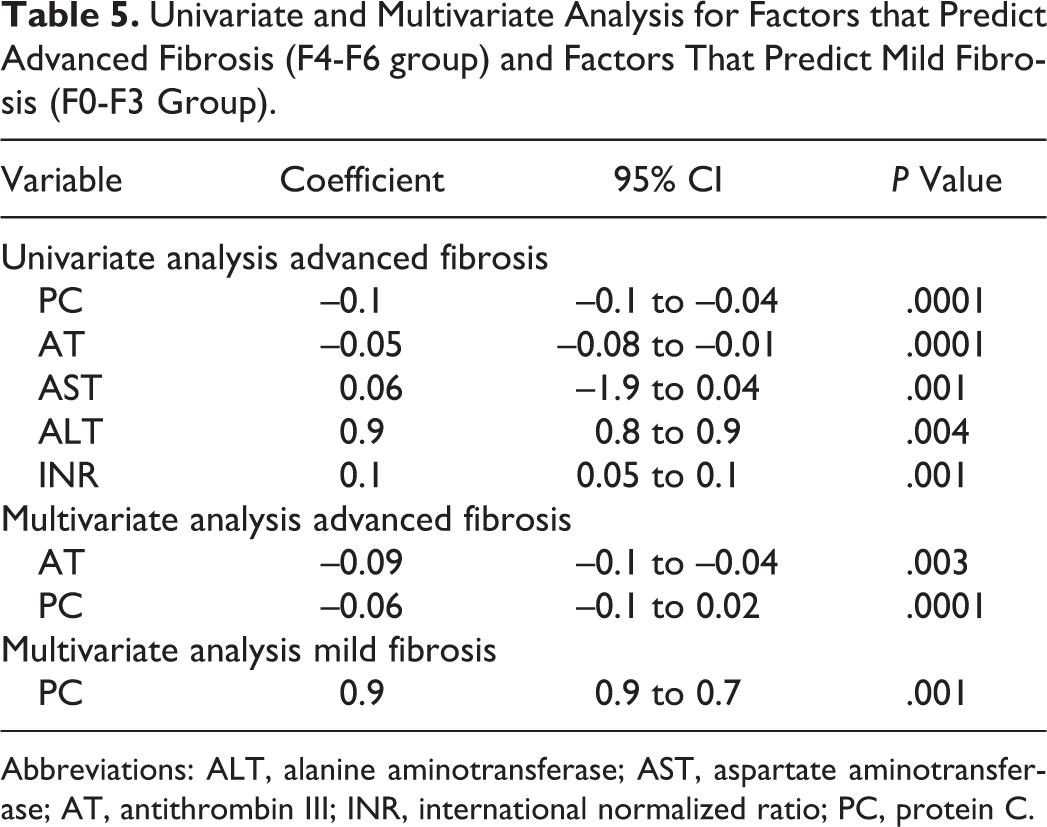
Independent variables predicted to be in the F4-F6 group were found to be PC, AT, AST, ALT, GGT, and INR (P < .05). Among these variables, AT and PC were found to be the strongest associated factors in the full multiple regression model (P = .003 and P = .0001). The only independent variable predicted to be in the F0-F3 group was found to be PC (P = .001; Table 5).
Univariate and Multivariate Analysis for Factors that Predict Advanced Fibrosis (F4-F6 group) and Factors That Predict Mild Fibrosis (F0-F3 Group).
Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase; AT, antithrombin III; INR, international normalized ratio; PC, protein C.
Discussion
In the current study, we extended the findings of previous studies of decreased natural anticoagulant levels in chronic liver disease and evaluated their association with the extent of hepatic fibrosis well defined by liver histology. We only investigated patients with chronic hepatitis C infection in order to constitute a homogenous population in which the varying degrees of fibrosis are easily assessed.
In the current report, the plasma levels of natural anticoagulants PC and AT exhibited significant reduction in patients with advanced fibrosis. This is usually considered to be the case in established cirrhosis where natural anticoagulants decrease in parallel with procoagulant factors. 19,20 However, patients with clinical signs of cirrhosis were excluded from our study, and only 11% of the included patients had a fibrosis score 6, corresponding to the histological cirrhotic stage. It was interesting to notice that in patients with chronic hepatitis C and at early stage of fibrosis (F0-F3), PC levels exhibited significant reduction in comparison to healthy controls. Although 93% of this group of patients had F2 or below, fibrotic stage PC deficiency was observed. All other analyzed hemostatic assays did not show any significant fluctuation in this group of patients. These findings support the hypothesis of plasmatic hypercoagulability in chronic liver disease as postulated in recent in vitro 12,13 and clinical 21 studies. Furthermore, our data implicate an onset of plasmatic procoagulant imbalance at an early stage of fibrosis.
In our study, PC decreased with severity of fibrosis, reaching median values below 50% in the F4-F6 group. Tripodi et al 22 reported median plasmatic PC levels close to 40% in patients with cirrhosis with a high index of procoagulant imbalance detected in vitro with thrombin generation tests. The authors showed that the prothrombotic state was reduced after adding purified PC, giving evidence that low PC levels was one of the main factors that contributes to procoagulant imbalance in patients with cirrhosis.
Our results of significant PC deficiency in all patient groups point to the concept that chronic liver disease possesses a procoagulant imbalance due to reduced PC.
The fact that AT, a sensitive indicator of liver impairment, 10,23 did not significantly differ between mild fibrosis and controls highlights the decrease in PC level as the earliest of the coagulation system in chronic liver disease, as suggested by a few previous reports. 24,25
More important was the finding that PC levels were inversely correlated with the extent of fibrosis showing the strongest association among all tested variables.
These data are in agreement with the previous studies that reported an association of extensive fibrosis with PC deficiency, along with other thrombotic risk factors, in patients with hepatitis C. 16,17 The role of coagulation in fibrogenesis has been supported by animal studies showing accelerated fibrosis progression in mice carrying the factor V Leiden (FVL) mutation. 26,27 Wright et al reported an association of FVL mutation with a 3.28-fold increased risk of rapid fibrosis progression in patients with hepatitis C. 28 This finding has been confirmed in a second cohort, 29 and a similar tendency has been demonstrated in patients with PC deficiency, increased FVIII expression, and hyperhomocysteinemia. 16
In our univariate and multivariate analyses, when healthy controls were compared to patients with extensive fibrosis, the strongest associated factor that emerged was PC. Furthermore, when healthy controls were compared to patients with mild fibrosis (F0-F3 group), PC was the only significantly associated variable. To our knowledge, this feature has not been described before. Our data strongly supports the connection between hypercoagulability, represented as PC deficiency, and progression of fibrosis.
Protein C deficiency observed in our study is likely to result from acquired defect, since in the healthy population, the prevalence of heterozygous deficiency is estimated at 0.2%. 30 Our hypothesis was that the most plausible mechanism for the significant decline in PC in our findings appears to be decreased liver synthesis due to liver fibrosis following chronic parenchymal damage in patients infected with hepatitis C virus.
The observed decrease in platelet count in patients with extensive fibrosis is a common feature in chronic advanced liver disease, 31,32 and it is universally agreed that multiple pathogenetic mechanisms that are complementary and often act in concert are involved. 33 In HCV-induced chronic liver disease, the main cause of thrombocytopenia could be attributed to sequestration as a result of hypersplenism secondary to portal hypertension and splenomegaly, bone marrow suppression by HCV, and impaired thrombopoietin production resulting from hepatocellular damage. 33
Although our data showed the evidence of a plasmatic procoagulant state, none of the patients included in our study had signs of venous thromboembolism or portal vein thrombosis. In a large population-based study, patients with liver disease were shown to have an increased risk of development of venous thrombosis compared with healthy persons. 34 Hypercoagulability could explain the occurrence of thrombotic complications, but according to Virchow triad, hemodynamic changes and a damaged vasculature may also play a role in the development of venous thrombosis. In patients with chronic liver disease, both processes may be present to enhance risk of thrombosis. 35 However, the observation that inherited thrombophilia, in particular the prothrombin G20210A mutation, enhances the risk of portal vein thrombosis in patients with cirrhosis suggests that hypercoagulability may play a role as well. 36
The main link between hypercoagulability and hepatic fibrogenesis is still being investigated giving strong evidence to the hypothesis that an increase in thrombin generation within the circulation directly activates stellate cell triggering fibrosis progression. 37 –39 This model is supported by studies showing that thrombin-mediated cell signaling is directly involved in modulating fibrogenesis. 38,40,41 One could assume that in PC deficiency, the progression of fibrosis could be modulated via an increased thrombin generation. However, if this is true, what occurs in vivo remains to be clarified.
Conclusion
The observed association between PC levels and histological staging supports the hypothesis of linking hypercoagulability with hepatic fibrogenesis. Protein C deficiency occurs in an early stage of chronic liver disease and may have a crucial role in the progress of fibrosis. Further clinical studies are warranted to establish the clinical consequences of a plasmatic hypercoagulant state in chronic liver disease and to study other associated factors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.