
Abstract
Few studies have assessed whether cases of asymptomatic pulmonary embolism (PE) in the early postoperative phase are subsegmental versus more proximal. In this study, we investigated whether asymptomatic PE occurring just after gynecologic surgery was subsegmental, and we examined the background characteristics of patients who experienced PE within 2 months postoperatively. All hospital records were reviewed, yielding a total of 2052 women who had undergone surgeries performed by the gynecologic oncology team between 2003 and 2013 in the National Kyushu Cancer Center. Asymptomatic and symptomatic postoperative PE cases diagnosed by multidetector computed tomography angiography or lung scan were identified; after excluding 2 cases of preoperative PE, there were 15 (0.73%) cases of postoperative PE among 2050 women. Of the 15 cases, 9 (60%) were diagnosed on postoperative day 1 or 2. Of the 9 women, 4 had no or minor symptoms/signs other than decreased oxygen saturation as measured by pulse oximetry (Sp
Introduction
In a previous study of patients who had undergone orthopedic surgery or had end-stage arteriosclerotic disease, only 4 of the 48 experienced symptoms suggestive of pulmonary embolism (PE); in general, asymptomatic PE is common.
1
Regarding gynecologic diseases, in a prior study involving women with ovarian cancer, PE was identified in 11.1% of the women prior to any treatment, and all of them were asymptomatic.
2
Following gynecologic surgeries, another study found that 35.6% of women diagnosed with postoperative PE were asymptomatic and had no signs except for a low oxygen saturation as measured by pulse oximetry (Sp
Multidetector computed tomography angiography (MDCTA) has a higher sensitivity for PE within the subsegmental pulmonary arteries compared with single detector computed tomography (CT) angiography, and the use of MDCTA has the potential to increase the rate of subsegmental PE diagnosis.
4
The risk profile and short-term clinical course of patients with symptomatic subsegmental PE appear to mimic those of patients with segmental or more proximal PE.
5
However, asymptomatic subsegmental PE may not be clinically relevant; in a previous study, the 3-month thromboembolic risk for patients with suspected PE who were left untreated was similar in those who underwent single CT and those who underwent multidetector CT pulmonary angiography.
4
In our previous study, 51.1% of PE cases occurring after gynecologic surgeries were detected on postoperative days 1 and 2; 70.4% of patients were asymptomatic and had no signs except for a drop in Sp
Methods
Mechanical prophylaxis with/without medical prophylaxis was established in our department around June 2003; thereafter, PE cases have been recorded when reported by attending doctors, and we have created a digital database of PE cases. For this study, we reviewed the surgical database to identify women who had undergone surgery performed by the gynecologic oncology team through the Gynecology Service of the National Kyushu Cancer Center from June 2003 through December 2013. A total of 2052 women who had undergone laparotomy, laparoscopic surgery, vaginal surgery, or vulvar surgery were identified from this database. Women who had undergone conization, dilatation and curettage, or left supraclavicular lymph node biopsy were not included, and there were no PE cases in this population. Patients’ background characteristics, such as height, weight, operation time, blood loss, and concomitant diseases, were obtained from the digital database of the Department of Anesthesiology. Digital data for laboratory tests were available starting in March 2004, and digital Sp
A schematic illustration of the diagnostic protocol used for identifying postoperative PE is presented in Figure 1. The Sp
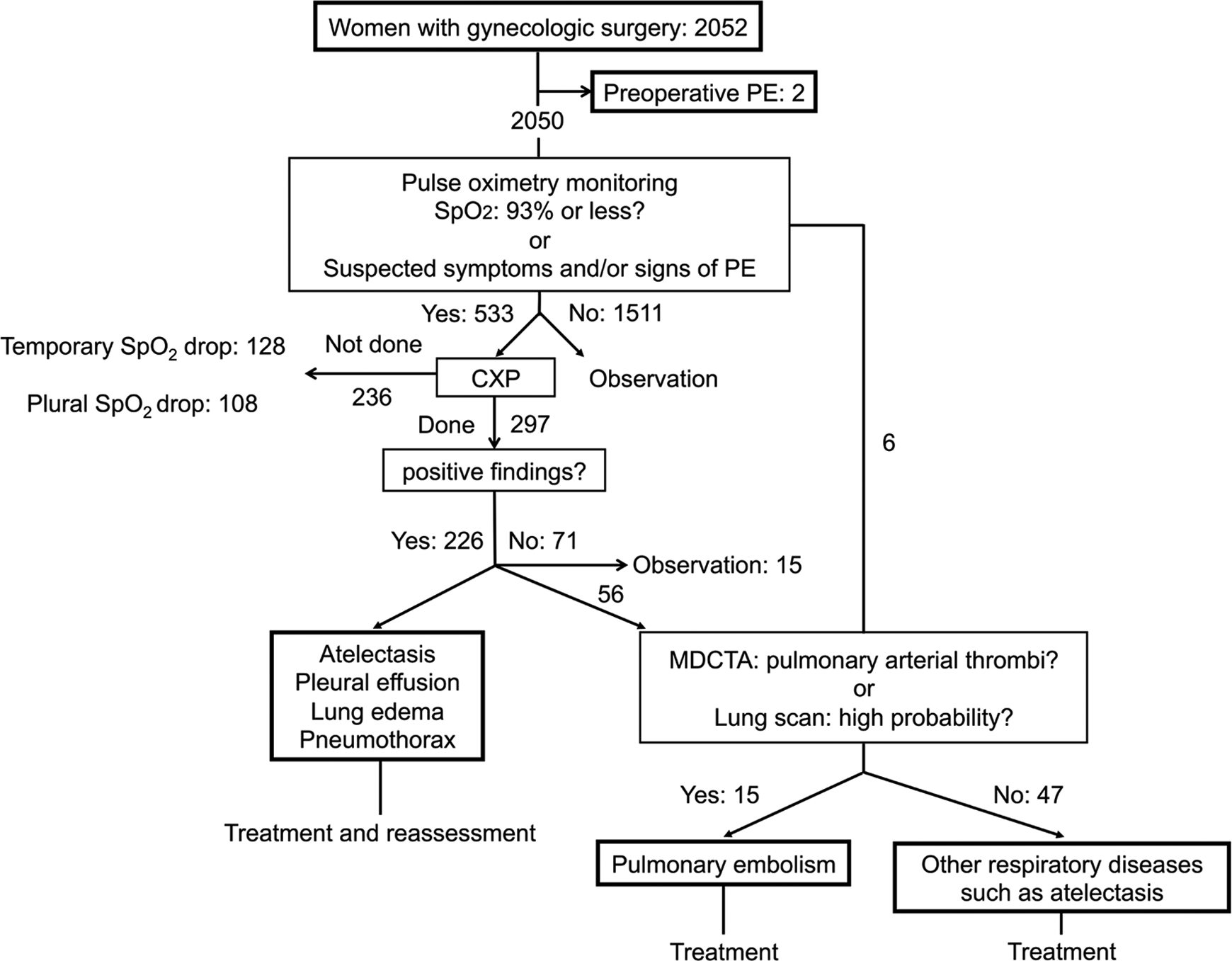
Schematic illustration of the diagnostic protocol for postoperative pulmonary embolism. When hypoxia (Sp
During the study period, 2052 patients were given graduated compression stockings (GCSs) and/or intermittent pneumatic compression (IPC) devices during and after surgery. The GCS and IPC were removed after complete ambulation. Most of the patients with malignant diseases and some of the patients with benign diseases were given low-molecular-weight heparin (LMWH; ie, dalteparin and/or enoxaparin) plus/minus fondaparinux after surgery. Five patients with preoperative deep vein thrombosis (DVT) above the calf received preoperative LMWH or unfractionated low-dose heparin. Under the Japanese health insurance system, LMWH use is usually restricted to malignant diseases in gynecological surgery.
Patients’ background characteristics included age,
Patients’ Background Characteristics and Univariate Analysis.a
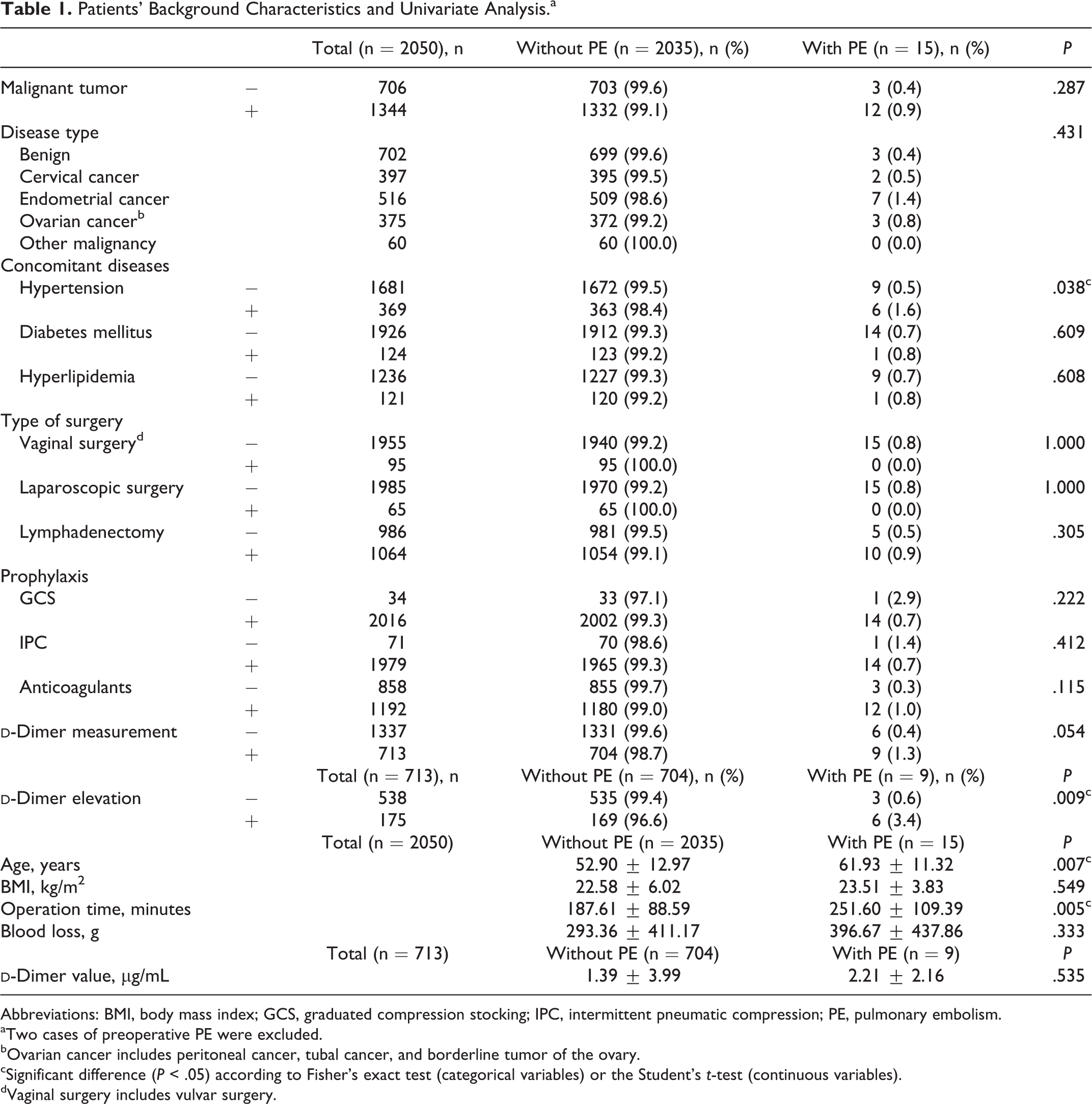
Abbreviations: BMI, body mass index; GCS, graduated compression stocking; IPC, intermittent pneumatic compression; PE, pulmonary embolism.
aTwo cases of preoperative PE were excluded.
bOvarian cancer includes peritoneal cancer, tubal cancer, and borderline tumor of the ovary.
cSignificant difference (P < .05) according to Fisher’s exact test (categorical variables) or the Student’s t-test (continuous variables).
dVaginal surgery includes vulvar surgery.
Patients with cervical cancer underwent radical hysterectomy and pelvic lymphadenectomy with/without bilateral salpingo-oophorectomy and with/without para-aortic lymphadenectomy. Patients with endometrial cancer underwent total abdominal hysterectomy and bilateral salpingo-oophorectomy, with/without pelvic and para-aortic lymphadenectomy. Some patients with endometrial cancer, such as women with serous adenocarcinoma, underwent omentectomy with/without appendectomy. Patients with ovarian cancer, including those with peritoneal cancer, tubal cancer, and borderline tumor of the ovary, underwent total abdominal hysterectomy, bilateral salpingo-oophorectomy, omentectomy, and appendectomy, with/without pelvic lymphadenectomy and para-aortic lymphadenectomy and with/without resection of disseminated lesions. Patients with vulvar cancer underwent radical vulvectomy or radical local excision of the vulvar tumor with/without inguinal lymphadenectomy. Patients with vaginal cancer underwent the same procedures as patients with cervical cancer. Patients with uterine sarcoma underwent total abdominal hysterectomy and bilateral salpingo-oophorectomy with/without lymph node sampling and with/without resection of disseminated tumors. Some women with microinvasive cancer, small-sized cancer, serious concomitant diseases, and obesity—as well as women hoping to become pregnant in the future—underwent more minimal procedures. The lymphadenectomy rate among women with malignant diseases was 79.2% (1064 of 1344), which was calculated using the data in Table 1.
Compression ultrasonography (CUS) of the lower limbs has been available since November 2006 in the Department of Clinical Laboratory Medicine at National Kyushu Cancer Center. Before this date, attending doctors in our department were instructed to avoid using IPC among patients with a high preoperative
Statistical Analysis
Student’s t-test was used for univariate analysis of continuous variables, Fisher’s exact test was used for univariate analysis of categorical variables, and multiple logistic regression was used for multivariate analysis. P-values less than .05 were considered to be significant. Dr SPSS II software, version 11.0.1 (SPSS Japan, Tokyo, Japan) was used for analyses.
Results
Follow-Up Period and Exclusion of Preoperative PE
Among the 2052 women who underwent surgeries from June 2003 to December 2013, the median follow-up period was 902 days (range, 5-4217 days) and the median hospitalization duration was 16 days (range, 2-249 days). Of these patients, 2 women with International Federation of Gynecology and Obstetrics (FIGO) stage IIIC and IC1 ovarian cancer were diagnosed with preoperative PE by MDCTA. The subtype was clear cell adenocarcinoma in both cases. Their Sp
Identification of Decreased Spo
2 (≤93%) and Suspected Symptoms/Signs of PE
Using the diagnostic protocol outlined in Figure 1, 15 (0.73%) cases of postoperative PE were identified among the 2050 women remaining after exclusion of the 2 with preoperative PE (Figure 1). There were 6 women who underwent MDCTA without chest X-ray photography (CXP), and PE was not detected among them (Figure 1). Their low Sp
Symptoms and Signs Associated With Postoperative PE
The 15 cases of postoperative PE are listed in Table 2. Of the 15 cases, 4 were diagnosed by lung scan, and the rest were diagnosed by MDCTA (Table 2). Patients’ primary diseases were as follows: 7 cases of endometrial cancer, 3 cases of ovarian cancer, 2 cases of cervical cancer, and 3 cases of benign disease (Tables 1 and 2).
Postoperative Pulmonary Embolism Cases During the Study Period.
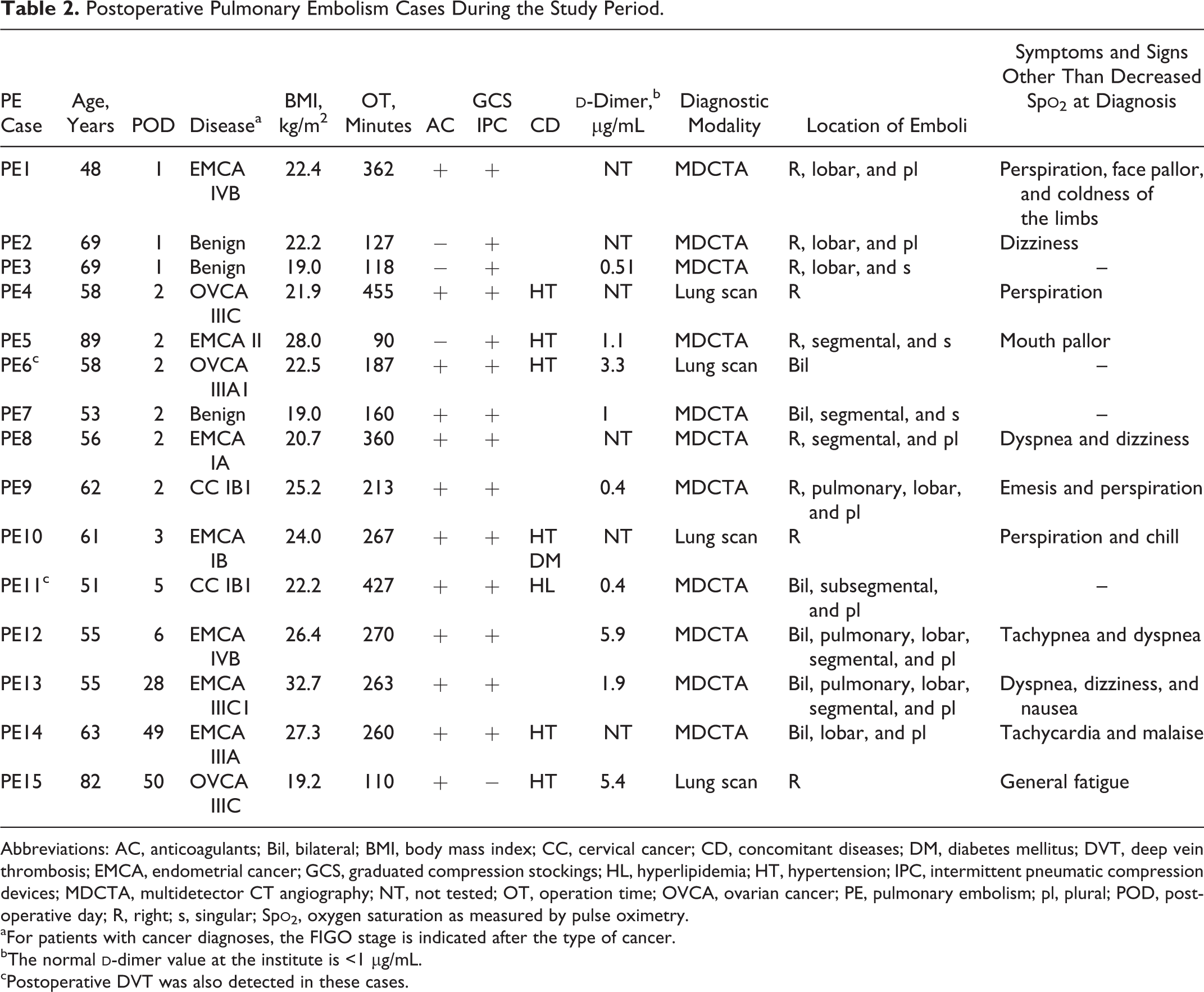
Abbreviations: AC, anticoagulants; Bil, bilateral; BMI, body mass index; CC, cervical cancer; CD, concomitant diseases; DM, diabetes mellitus; DVT, deep vein thrombosis; EMCA, endometrial cancer; GCS, graduated compression stockings; HL, hyperlipidemia; HT, hypertension; IPC, intermittent pneumatic compression devices; MDCTA, multidetector CT angiography; NT, not tested; OT, operation time; OVCA, ovarian cancer; PE, pulmonary embolism; pl, plural; POD, postoperative day; R, right; s, singular; Sp
aFor patients with cancer diagnoses, the FIGO stage is indicated after the type of cancer.
bThe normal
cPostoperative DVT was also detected in these cases.
Of the 15, 9 (60%) postoperative PE cases were diagnosed on postoperative day 1 or 2 (Table 2). Of the 9 women, 3 had no symptoms or signs except for decreased Sp
The cases with a late onset (PE13, PE14, and PE15) were diagnosed during the postoperative chemotherapy period, and they all showed symptoms and signs that were relatively easy to detect (Table 2). There were no recurrent, massive, 10,11 or fatal postoperative PE cases from June 2003 through December 2013.
Characteristics of the 15 Women With PE
The BMI, operation time, concomitant diseases, and prophylaxes are shown in Table 2. For patients with malignant disease, the FIGO stage is also indicated. Of the 3 patients with ovarian cancer, the subtype was serous adenocarcinoma in 2 cases and endometrioid adenocarcinoma in 1 case. Six women received IPC without preoperative
Locations of Postoperative Pulmonary Emboli
The locations of the emboli detected in the 11 postoperative PE cases diagnosed by MDCTA are indicated in Table 2. In all, 7 cases were diagnosed on postoperative days 1 and 2, and the remaining 4 cases were diagnosed thereafter. Among the cases diagnosed on postoperative days 1 and 2, the 3 women who were asymptomatic or had minor symptoms (PE3, PE5, and PE7) had emboli located in the segmental or lobar arteries (Table 2 and Figure 2A, B, and C). Four symptomatic women had emboli in the segmental arteries or more proximal (PE1, PE2, PE8, and PE9; Table 2). Two of the symptomatic cases (PE2 and PE9) are shown in Figure 2D and E.
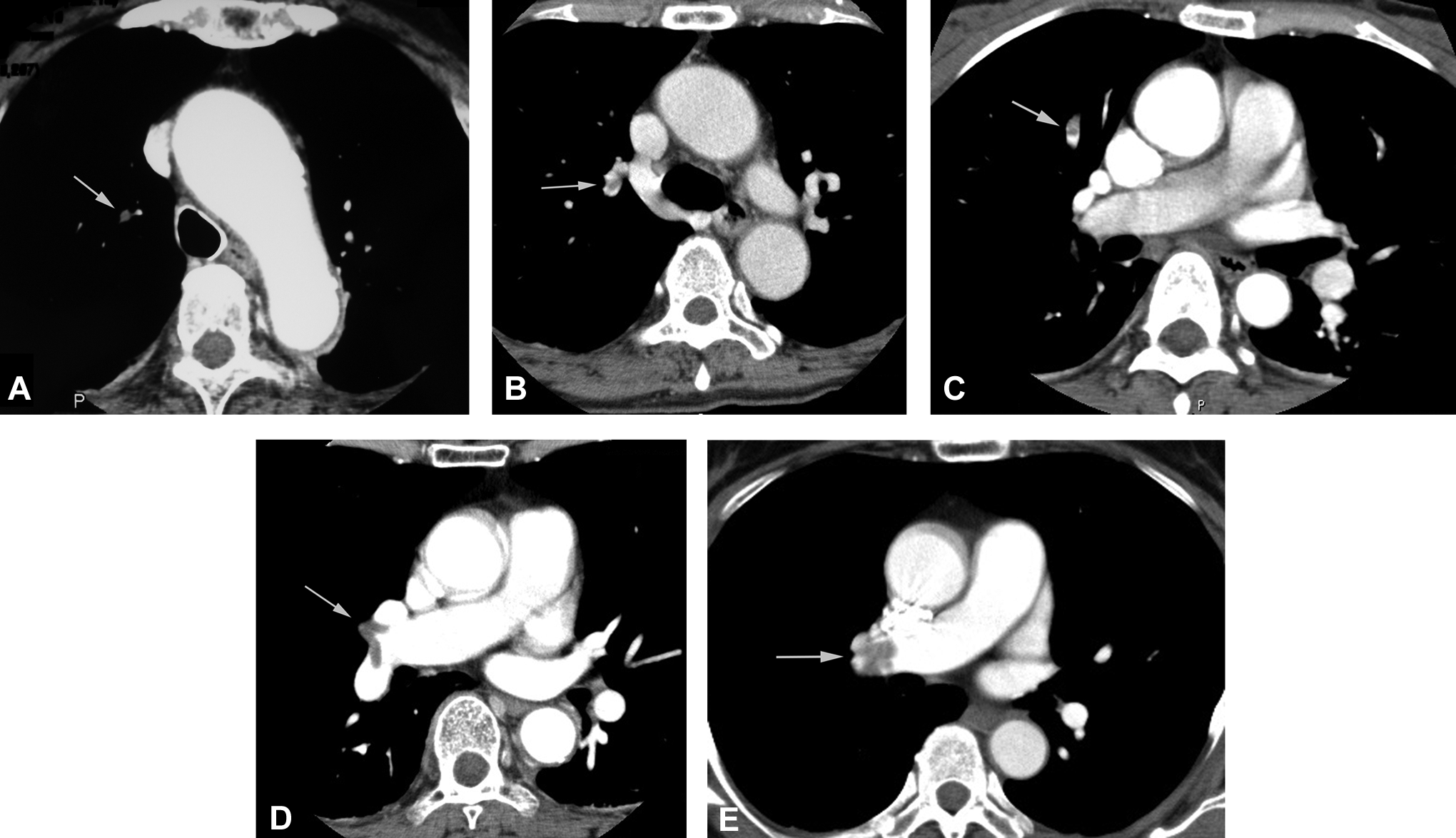
The CT angiography imaging of pulmonary emboli detected on postoperative days 1 and 2. The CT angiography shows several emboli (arrows). A, Illustrates an embolus associated with minor symptoms (PE5). B and C, Represent asymptomatic cases (PE3 and PE7). D and E, Represent symptomatic cases (PE2 and PE9). A, An embolus is shown in the right segmental artery. B, An embolus is shown in the right lobar artery. C, An embolus is shown in the right segmental artery. D, Emboli are shown in the right lobar arteries. E, An embolus is shown in the right pulmonary artery. CT indicates computed tomography; PE, pulmonary embolism.
Among the cases diagnosed on or after postoperative day 3, 3 symptomatic women had emboli located in the pulmonary, lobar, and/or segmental arteries (PE12, PE13, and PE14; Table 2). One woman without symptoms had subsegmental PE (PE11; Table 2).
Univariate Analysis of the Patients’ Background Characteristics
Univariate analysis of suspected factors was performed for postoperative PE cases (Table 1). Statistically significant factors were hypertension, preoperative
Age, Operation Time, Anticoagulant Use, and Preoperative d -Dimer Evaluation in Women With Malignant and Benign Diseases
The presence of a malignant tumor (as the operative indication during the study period) was not a significant factor in univariate analysis (P = .287; Table 1). The mean age of women with malignant diseases was 53.93 ± 12.61 years and that of women with benign diseases was 51.11 ± 13.46 years (P < .001). The operation time was 216.01 ± 90.25 minutes for women with malignant diseases and 134.91 ± 55.95 minutes for women with benign diseases (P < .001). Women with malignant diseases had more harmful factors in addition to malignancy itself than women with benign diseases. However, regarding thromboembolic prophylaxis, anticoagulants were administered to 1109 (82.5%) of the 1344 women with malignant diseases and 83 (11.8%) of the 706 women with benign diseases; the difference was statistically significant (P < .0001). Preoperative
Multivariate Analysis of the Factors Identified as Significant in Univariate Analyses
The 4 variables significantly associated with postoperative PE based on univariate analysis were evaluated using multiple logistic regression (Table 3). Multivariate analysis demonstrated that preoperative
Multivariate Analysis of the Variables Influencing Pulmonary Embolism Incidence.
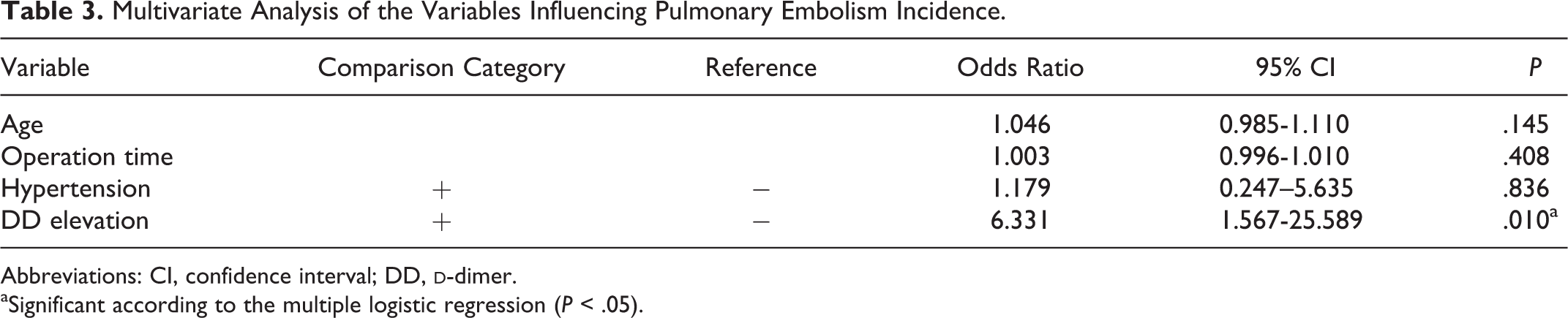
Abbreviations: CI, confidence interval; DD,
aSignificant according to the multiple logistic regression (P < .05).
d -Dimer Measurement and CUS Performance
The
Of the 2050 women included in the analysis, 15 were diagnosed with preoperative DVT; they all underwent CUS because of high
Use of IPC Devices Among Women With High d -Dimer Levels
Of the 124 women, 21 (16.9%) with high
Discussion
The identification of asymptomatic PE cases just after surgery might not be clinically important if most of these emboli tended to be subsegmental, because patients with subsegmental PE can have a favorable clinical outcome even without receiving anticoagulant therapy. 4 However, in the present study, 3 of the 4 patients who were asymptomatic or had minor symptoms when diagnosed with PE on postoperative days 1 and 2 had emboli in the segmental or more proximal arteries. Thus, diagnosing very early postoperative PE appears to be clinically relevant.
Plasma
Arterial blood gas oxygen saturation levels have low sensitivity and specificity for PE diagnosis and are incorporated in neither the Wells score nor the revised Geneva score.
6
Consequently, arterial blood gas saturation should not be routinely used to exclude PE.
6
One of the reasons for this is that PE does not necessarily cause hypoxia. In a previous study, hypoxia was present in only 35% of PE cases.
14
A high plasma
Cancer is one of the major risk factors for PE.
6,16
In our previous study, which included the period before methodical prophylaxis was established, the overall incidence of postoperative PE was 2.14%; according to univariate analysis, the incidence was higher in women with malignant diseases than in women with benign diseases.
3
However, in the present study, the incidence of postoperative PE did not statistically differ between women with malignant diseases and those with benign diseases, although the mean age was significantly older and the mean operation time was significantly longer among women with malignant diseases. The rate of anticoagulant use and the rate of
Among women who underwent vaginal or vulvar surgery, there were no cases of postoperative PE, although the type of surgery was not identified as a statistically significant factor. Opening the abdominal cavity and packing off the intestines may impede blood flow in the vena cava, potentially promoting more venous stasis than that which occurs in association with vaginal procedures. 17
A strength of the present study was its focus on very early, asymptomatic postoperative PE. Our study does have several limitations. First, 108 of the 553 patients who had several episodes of low Sp
In conclusion, patients who were asymptomatic or had minor symptoms at PE diagnosis on postoperative days 1 and 2 had emboli in the segmental or more proximal arteries. Identifying asymptomatic PE in the early postoperative period may be clinically significant because most of these emboli are proximal to the subsegmental arteries.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants-in-aid for cancer research from the Ministry of Health, Labour and Welfare (nos. 11-1 and l5-6) of Japan.