
Abstract
Dabigatran and rivaroxaban are novel nonvitamin K antagonist oral anticoagulants (NOACs) approved for thromboprophylaxis in atrial fibrillation (AF). In Turkey, like other countries, the efficacy of translation of the clinical trial results and current guideline recommendations into daily clinical practice is yet to be discovered. Using data from medical records of three tertiary care cardiology centers, we identified patients with nonvalvular AF on dabigatran or rivaroxaban treatment. Baseline characteristics and utilization trends were compared between dabigatran and rivaroxaban groups. Secondarily, clinical events including ischemic stroke and/or transient ischemic attack, systemic embolism, and bleeding were evaluated. Among 294 patients with AF included, dabigatran was utilized in 177 (60.2%) and rivaroxaban in 117 (39.8%). Overall, 76% of patients had received long-term warfarin therapy. The use of 110 mg twice a day (55.4%) was the prevailing strategy in dabigatran group, whereas in rivaroxaban group 20 mg every day (67.5%) was the preferred option. Of the patients, 37.3% had severe valvular disease in which mitral regurgitation was the predominant valve abnormality. Scores of CHADS2, CHA2DS2VASc, and HAS-BLED were similar in both the groups. Of the patients, 24% in dabigatran group and 13.7% in rivaroxaban group were prescribed the lower dose inappropriately. The two NOACs did not differ significantly in terms of clinical events. The results of this study indicate that in daily practice, the physicians’ behavior in utilizing the NOACs is shaped by the clinical trials and the guideline recommendations. On the other hand, in dose selection, this adherence is not of high quality.
Introduction
Patients with atrial fibrillation (AF) have a 5-fold increased risk of cardioembolic stroke compared to those in sinus rhythm, with a cardioembolic stroke resulting in approximately 20% of patients dying in the acute phase and 60% developing severe disability. 1,2 Anticoagulant therapy with vitamin K antagonists (VKAs), mainly with warfarin, can reduce the risk of stroke by at least 60% compared to placebo. 3 However, there are concerns with warfarin due to its narrow therapeutic window, numerous drug and food interactions, need for frequent monitoring of international normalized ratio (INR), and tailoring doses accordingly. 4 Despite all efforts, maintaining some patients within the desired INR levels, in other words achieving a time in therapeutic range (TTR) ≥70% as the guidelines recommend, is not possible. 5
NonVKA oral anticoagulants (NOACs) were developed to overcome the above-mentioned limitations of warfarin. These include dabigatran, an oral direct thrombin inhibitor, and rivaroxaban, apixaban, and edoxaban, oral factor Xa inhibitors. In the pivotal trials, RE-LY (The Randomized Evaluation of Long-Term Anticoagulation Therapy), ROCKET-AF (The Rivaroxaban Once Daily Oral Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation), ARISTOTLE (The Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation), and ENGAGE-AF TIMI 48 (edoxaban The Effective Anticoagulation with Factor Xa Next Generation in Atrial Fibrillation-Thrombolysis in Myocardial Infarction 48), the efficacy and safety of NOACs were tested against warfarin and found to be at least noninferior to warfarin. 6 –9
Eventually, they are strongly endorsed by the recent guidelines from the American College of Cardiology, the American Heart Association, the Heart Rhythm Society, and the European Society of Cardiology and European Heart Rhythm Association for use as an alternative to warfarin in the treatment of patients with nonvalvular AF for the risk reduction of stroke and systemic embolism. 5,10,11
All these drugs, except edoxaban, have been marketed extensively worldwide and are increasingly replacing warfarin in clinical practice. 12 The NOACs offer several advantages compared with warfarin, including rapid onset of action, fixed dosing, and no requirement for routine coagulation monitoring. In daily clinical practice, while these properties will make the usage of these drugs easier than warfarin, concern regarding the long-term safety and efficacy in various patient groups remains. In contemporary medicine although the results of clinical trials shed light to clinical practice, not all the patients in real-life are represented in those trials. Therefore, it is a challenge to learn the behaviors of physicians when using these new drugs in real-life setting.
Using data from the medical records of three centers, in this retrospective study, we primarily aim to investigate the characteristics of the patients in whom the physicians prefer to use NOACs, namely, dabigatran and rivaroxaban in daily clinical practice and physicians’ compliance with the relevant guidelines and clinical trials. Secondarily, clinical events including ischemic stroke and/or transient ischemic attack (TIA), systemic embolism, bleeding, and any adverse event that the patient or the physician linked with the NOACs were evaluated.
Methods
When this retrospective study was designed, dabigatran and rivaroxaban were the two NOACs that were approved by authorities and reimbursed by the major health insurance provider in Turkey. Therefore, only the data relevant to these two NOACs are extracted from the medical records. In order to examine the plurality of practice behavior, three tertiary care cardiology clinics in Turkey (Department of Cardiology, Istanbul University, Cerrahpasa Faculty of Medicine, Istanbul; Department of Cardiology, Sakarya University Faculty of Medicine, Sakarya; and Bakırkoy Dr Sadi Konuk Research And Training Hospital, Istanbul) took place in the study. Beginning from April 2012, 100 consecutive patients, aged ≥18 years with electrocardiographically documented paroxysmal or permanent nonvalvular AF and already on dabigatran or rivaroxaban treatment for at least 3 months, were recruited from each center. In order to reflect real-life clinical practice, there were no exclusion criteria. This study was approved by the ethics committee of Cerrahpasa Medical Faculty, which was the coordinating center.
The patients were identified from the electronic patients records. The date of the first prescription found in the records was assumed as the initiation date of dabigatran or rivaroxaban treatment. The clinical data were extracted from the cases’ outpatient clinic records. In addition to that, in order to assess the latest clinical status, researchers conducted an interview with all patients either by phone (75%) or during an outpatient clinic visit (25%) between June and November 2014. By this method, there were no dropouts. Patients’ demographics, prior use of warfarin, concomitant use of antiplatelet drugs, concomitant use of other drugs, prior stroke and/or TIA, systemic embolism, and bleeding history were documented. As recommended by the recent and relevant guidelines, renal function (creatinine clearance [CrCl]) was calculated by Cockroft-Gault formula. 13
Nonvalvular AF was defined as the presence of AF and the absence of severe mitral stenosis or prosthetic heart valves. Patients with other types of valvular disease were specified according to echocardiography report, which was performed before initiation of NOACs. Severe valvular disease (SVD) was defined as any valvular disease classified as at least moderate to severe in echocardiography report.
The risk scores used in this study to estimate the annual stroke risk in patients with nonvalvular AF were the “CHADS2” (congestive heart failure, hypertension, age ≥75 years, diabetes mellitus are each assigned 1 point and previous stroke or TIA is assigned 2 points) 14 and “CHA2DS2VASc” scores (congestive heart failure, hypertension, age 65 to 74 years, diabetes mellitus, female sex, and vascular disease are each assigned 1 point and prior stroke or TIA or thromboembolism and ≥75 years are assigned 2 points). 15 For the calculation of bleeding risk the HAS-BLED score (hypertension, renal or liver disease, stroke, bleeding, labile INR, an age of 65 years or older, and the use of medications or alcohol are each assigned 1 point) was used. 16
The primary aim of this study was to gain detailed insight into the characteristics of the patients in whom the physicians prefer to use dabigatran or rivaroxaban in daily clinical practice and physicians’ compliance with the relevant guidelines and clinical trials. Secondarily, ischemic stroke and/or TIA, systemic embolism, and bleeding were queried as clinical events. Bleeding events were categorized as major or minor hemorrhage. Intracranial bleeding and bleeding requiring transfusion were accepted as major bleedings. All other bleedings were considered as minor. Because of the retrospective nature of the study for the estimation of adherence to medications, pill counting was not possible. Therefore, this was evaluated according to patients’ self-reporting.
Statistics
A statistical software package (SPSS 16; Chicago, Illinois) was used to perform all analyses. Continuous variables were summarized as mean ± standard deviation or as median with range as appropriate, and categorical variables as the number of patients and percentage. The baseline characteristics were compared using the chi-square test for categorical variables and the Mann-Whitney U test for continuous variables. A P value of less than .05 was considered significant.
Results
Although 300 patients from three centers were enrolled initially, 6 patients were excluded because the indication for NOAC was other than AF. Therefore we analyzed the data of 294 patients as the study population. The first prescription of dabigatran was on April 1, 2012, and rivaroxaban was on January 16, 2013. The median duration of the elapsed time since the commencement of the NOACs was 336 days (range 91; 583) in dabigatran group and 280 days (range 108; 383) in rivaroxaban group (P < .001). There were 5 deaths from any cause reported (3 patients in dabigatran group and 2 patients in rivaroxaban group).
Baseline Characteristics
Baseline characteristics of the patients for the whole cohort and according to the NOAC (dabigatran or rivaroxaban) they use are presented in Table 1. There was a female predominance in our cohort. Age, sex, CHA2DS2VASc, CHADS2, or HAS-BLED scores were not different between the groups. However, while diabetes mellitus was more prevalent in dabigatran group (P = .007), heart failure was more frequent in patients treated with rivaroxaban (P = .053). The review of the medical records revealed that 3 patients (1%) had no indication for any NOAC (CHA2DS2VASc = 0). Within the groups, the rates of prior stroke and/or TIA, systemic embolism or bleeding were almost identical. The renal function of the whole cohort was fair but CrCl was significantly lower in rivaroxaban group than dabigatran group. Although in the whole cohort, 76% of the patients are switched to NOACs from warfarin, this rate in rivaroxaban group exceeds dabigatran group significantly (P < .001) by 21%. Dual antithrombotic treatment was not rare, and it was even more frequent in patients using rivaroxaban. Considering the most uncomfortable side effect of dabigatran, it was not a surprise to find an almost 6-fold (P < .001) higher rate of proton pump inhibitor treatment in the group using dabigatran.
Characteristics of the Patients.a
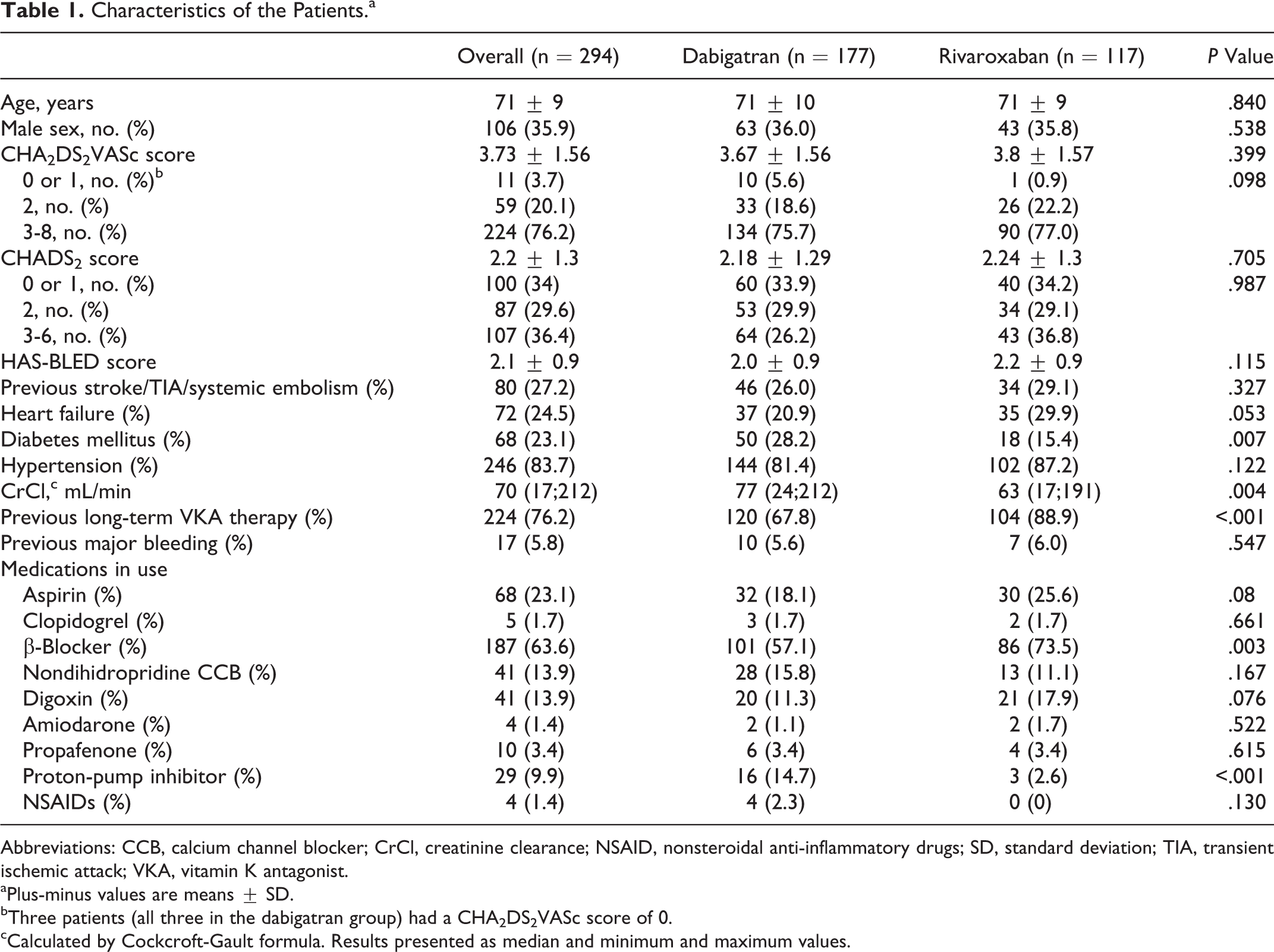
Abbreviations: CCB, calcium channel blocker; CrCl, creatinine clearance; NSAID, nonsteroidal anti-inflammatory drugs; SD, standard deviation; TIA, transient ischemic attack; VKA, vitamin K antagonist.
aPlus-minus values are means ± SD.
bThree patients (all three in the dabigatran group) had a CHA2DS2VASc score of 0.
cCalculated by Cockcroft-Gault formula. Results presented as median and minimum and maximum values.
Concomitant Valvular Disease
The echocardiography findings were available in 217 (74%) patients in whom 81 (37.3%) had SVD (Table 2). Mitral regurgitation dominated (33%) the SVD, followed by aortic stenosis (3.7%) and regurgitation (3.2%). Although the aortic valvular abnormalities were not different between the groups, mitral regurgitation was significantly (P < .001) more prevalent in patients using rivaroxaban. One patient not displayed in the table, had mild mitral stenosis.
Type of Valvular Disease in Patients Assessed as Having SVD.
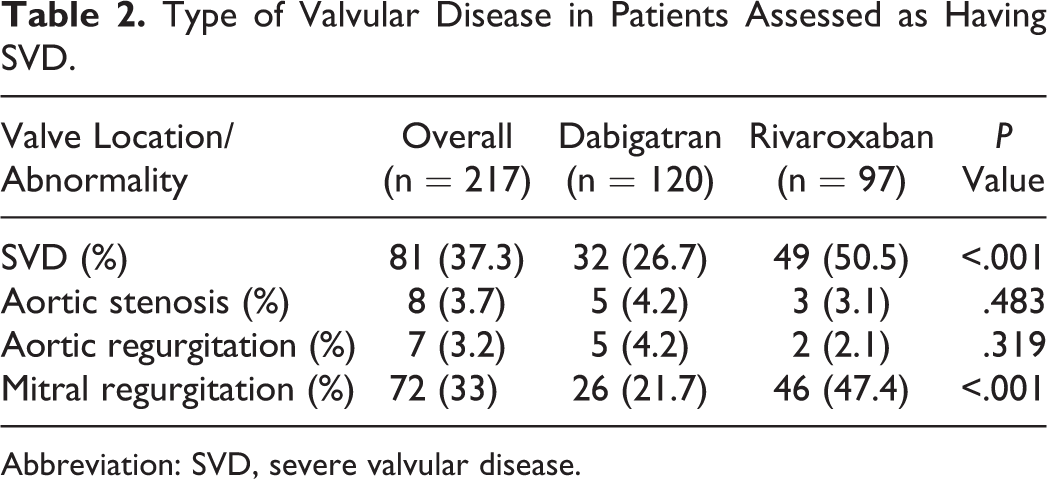
Abbreviation: SVD, severe valvular disease.
Dosing
Dosing regimens for both drugs, stratified by age and CrCl are shown in Figures 1 and 2. The use of 110 mg twice a day (55.4%) was the prevailing regimen in the dabigatran group, whereas in rivaroxaban group 20 mg every day (67.5%) was the preferred option for anticoagulation. Despite the recommendations of the current guidelines in favor of 150 mg twice a day, 24% of patients younger than 80 years, with preserved renal function (CrCl > 50) and HAS-BLED score <3, were prescribed dabigatran 110 mg twice a day. Under similar circumstances, 13.7% patients in the rivaroxaban group received 15 mg every day.
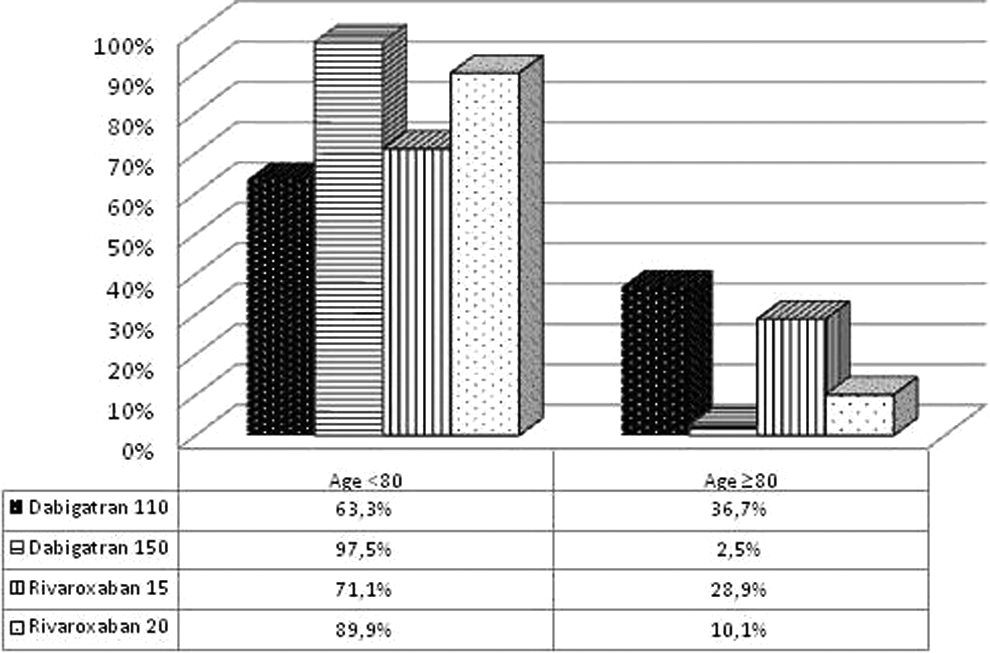
Dosing regimens for dabigatran and rivaroxaban, stratified by age.
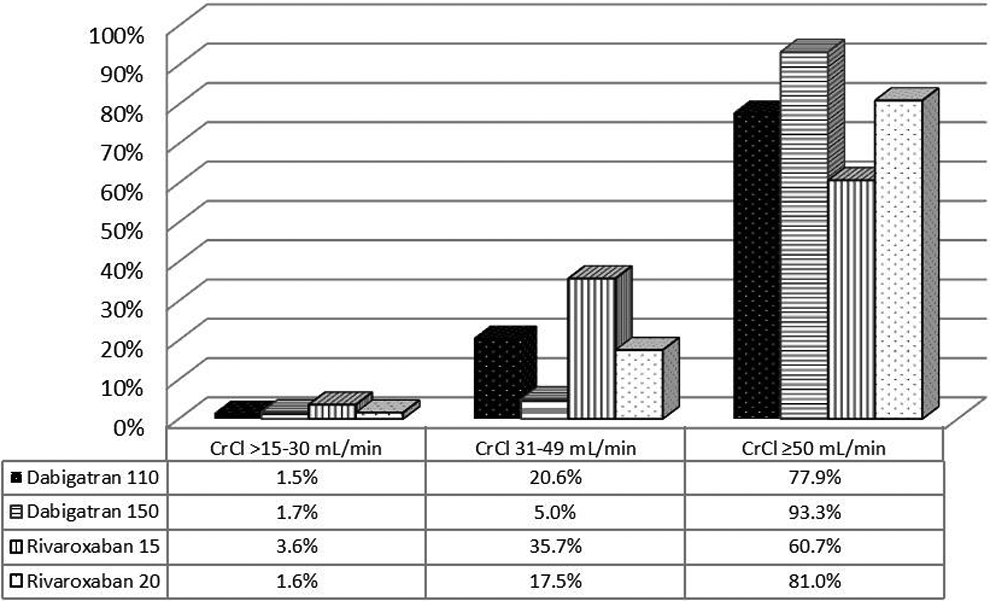
Dosing regimens for dabigatran and rivaroxaban, stratified by creatinine clearance (CrCl).
Clinical and Adverse Events
Clinical and adverse events are presented in Table 3. The rate of stroke, TIA, or systemic embolism was similar within both NOAC groups. Major or minor bleedings were not significantly different between the groups. Of the 6 major bleedings, 5 were gastrointestinal and 1 in a patient on rivaroxaban, was intramuscular. There was no intracranial bleeding. As expected, the rate of dyspepsia was higher among those treated with dabigatran compared to those treated with rivaroxaban (11.3% dabigatran vs 1.7% rivaroxaban). As compared with the 110 mg dose of dabigatran, the 150 mg dose of dabigatran was associated with a trend toward a higher rate of dyspepsia although this was nonsignificant (8.2% with 110 mg vs 15.2% with 150 mg dose, P = .110).
Clinical and Adverse Events According to Treatment Groups.
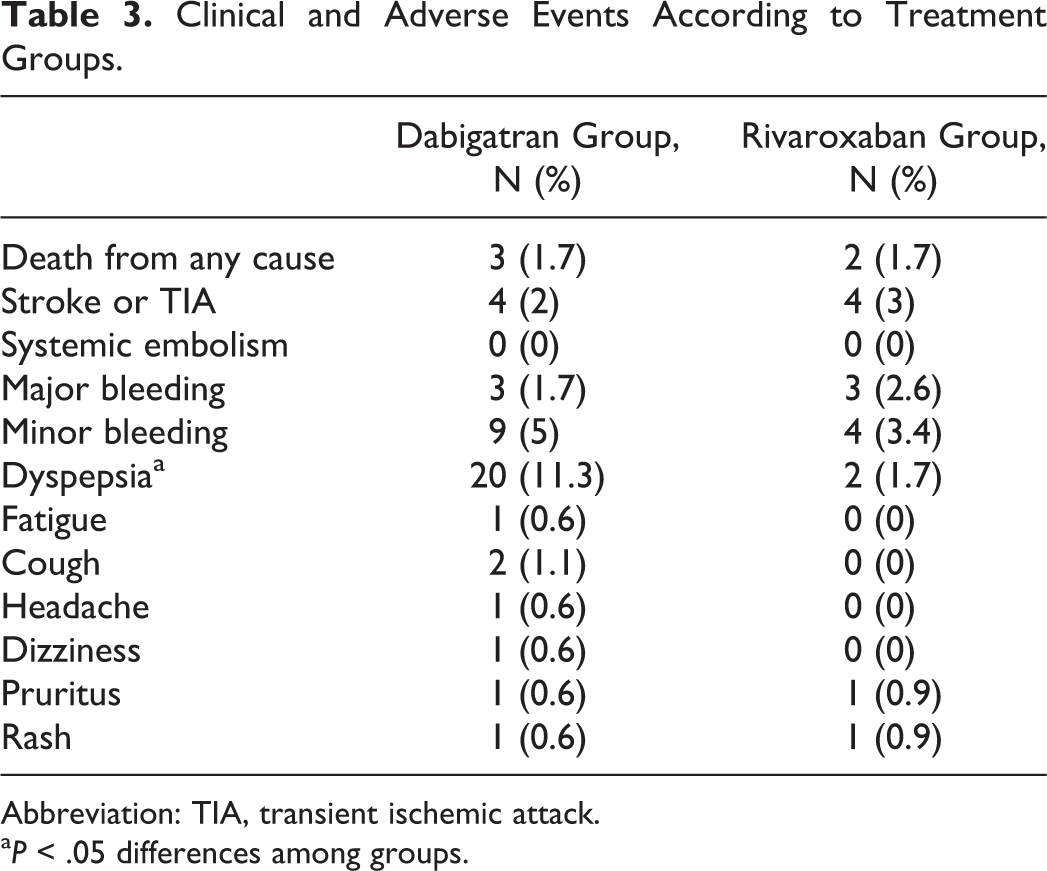
Abbreviation: TIA, transient ischemic attack.
a P < .05 differences among groups.
In our study cohort, NOACs were discontinued permanently in 42 (14.3%) patients. As compared with rivaroxaban group (11 patients; 9.4%), treatment discontinuation rate was significantly higher (31 [17.5%] patients in dabigatran group [P = .036]). When 110 and 150 mg doses of dabigatran were compared there was a trend toward increased rate of discontinuation (13.3% vs 22.8%, respectively; P = .073) in the higher dose. In half of these patients the reason for discontinuation was due to the aforementioned side effects. The most frequent adverse effects leading to discontinuation of dabigatran were bleeding and gastrointestinal discomfort. Six patients intentionally stopped NOAC therapy within 1 month after prescription. Other reasons for discontinuation were inappropriate counseling by the physicians (10 patients) and physician’s decision to switch to warfarin after percutaneous coronary intervention (2 patients).
According to patients’ self-reports, there was a 15.1% poor adherence in dabigatran group and 20.8% in rivaroxaban group. The patterns of poor adherence were as follows: (1) omission of doses and (2) taking only 1 dose a day for dabigatran (intentionally or because of inappropriate counselling by clinician).
Discussions
To the best of our knowledge, this is the first study to include two NOACs in almost equal proportions and which investigates the utilization patterns of NOACs in patients with nonvalvular AF in a real-life setting. Every 3 of 4 patients on NOACs are switched from prior warfarin treatment is the first major finding that has to be mentioned. Second, the NOAC (OAC) indication is highly in concordance with the relevant current guideline recommendations; however, the adherence to the guidelines disappears when choosing the proper NOAC dose, especially in dabigatran. Our third finding is that, since the baseline characteristics are mostly similar, no determinant is identified that affects the physician’s preference for choosing either NOAC. Finding number four is that the presence of SVD, other than severe mitral stenosis and prosthetic valves, does not affect the utilization of NOACs. And finally both drugs have similar efficacy and safety; however, gastrointestinal discomfort seems to be an important side effect of dabigatran.
After the approval of NOACs by the authorities, some registries especially from the Nordic Countries have been published to reflect the real-life experience with these novel oral anticoagulants. 12,17,18 However, when read thoroughly it will be easily noted that overwhelmingly dabigatran is the NOAC that is evaluated in these publications. As dabigatran is the first NOAC licensed, this is an expected and acceptable situation. On the other hand, sufficient time has elapsed since the appearance of rivaroxaban in the market. Therefore, by including both drugs and finding a 40% utilization of rivaroxaban among NOACs, this study reflects the real-life clinical experience and gives the opportunity to estimate the utilization patterns of NOACs and make a comparison between them.
For oral anticoagulation, current European guideline recommends the initiation of an NOAC, instead of warfarin, in patients with nonvalvular AF. The findings of this report indicate that this is not the case in real life. Seventy-six percent of the whole cohort is switched to NOACs from warfarin treatment. This is primarily due to the current reimbursement policy in Turkey that asks for at least 2 months trial and proof of failure (>60% of TTR) of warfarin treatment. It is out of the scope of this study to discuss the economic aspects of this policy but from a medical point of view, in a country with 45% TTR with warfarin therapy 19,20 not initiating NOAC therapy in anticoagulant naive patients might be a loss of time. Supporting this argument, an article from Turkey, which shows that anticoagulants are not prescribed to 60% of the patients with nonvalvular AF although they have a mean CHA2DS2VASc score of 3.32, is recently published. 21 Besides others, the complex nature of warfarin was held responsible for the underutilization of anticoagulants. No explanation is found for the higher rates of prior warfarin treatment in the rivaroxaban group. This might be due to play of chance.
Both the CHADS2 and CHA2DS2VASc mean scores of the whole cohort and two NOAC groups indicate that physicians’ decision of prescribing OAC treatment is almost completely in concordance with the current guidelines. In our cohort we observed a higher mean CHADS2 score than the mean scores of the recently published registries. 12,17,22 The most probable explanation for this difference is that this study was conducted in three referral tertiary centers, and an average patient to be enrolled in these centers would have a higher stroke risk than a typical patient in a nationwide registry. For the same reason, a similar diversity is seen in the mean CHA2DS2VASc score, as well. Overall, the mean CHA2DS2VASc score of our cohort is almost one point higher than the mean score of the very recently published Danish registry. 12
In spite of the difference in mean CHADS2 scores of the study populations of RE-LY and ROCKET-AF trials, the current guidelines do not specify any risk level that dabigatran or rivaroxaban would be more beneficial. When the mean CHADS2 score of this cohort driven from real-life experience is compared with the mean CHADS2 scores of the study populations of the above-mentioned randomized controlled trials, it is found that it is similar to RE-LY trial (2.1 ± 1.1). Due to the inclusion criteria, this score is strikingly higher in ROCKET-AF trial (3.5 ± 0.95) than our results. This finding is a proof that, since in the present study the mean CHADS2 scores of both NOAC groups are similar, while choosing one of the two novel anticoagulants the physicians adhere to the recommendations of the guidelines, rather than the individual trials. If it was the opposite we would have found a higher mean CHADS2 score in the rivaroxaban group.
In RE-LY trial, dabigatran 110 mg twice a day, with the same inclusion criteria with others, was one of the three randomization arms, and this arm included equal number of patients as the others. The results indicate that this dose is noninferior to warfarin in terms of efficacy but with significantly less bleeding rate is safer than warfarin. Dabigatran 150 mg twice a day is more effective in reducing thromboembolic events than warfarin with a similar safety profile. In ROCKET-AF, the dose of rivaroxaban was 20 mg every day and it was reduced to 15 mg every day when the patient’s CrCl was 30 to 49 mL/min. In other words the patients using rivaroxaban 15 mg are a subgroup (21%) rather than a randomization arm. In terms of efficacy, both doses of rivaroxaban were noninferior to warfarin. This brief summary of the studies are given here because, in real-life setting, this is what we found to determine the physicians’ behavior in selecting the dose of NOACs instead of the dose recommendations of the current guidelines. In order not to sacrifice the efficacy benefit, guidelines point the higher doses of both NOACs as the dose of choice. According to these documents the reduced doses are appropriate in only specified (age >80, CrCl 30-49 mL/min, HAS-BLED ≥3) patient groups. However in dabigatran dosing, what we observed in real-life practice is quite different from the guidelines but in a way in accordance with the results of RE-LY trial. Utilizing the lower dose in a quarter of patients in dabigatran group in the present real-life cohort, who do not need dose reduction according to guidelines, proves that substantial number of physicians prefer to stay in the safer side instead of choosing the more effective higher dose. And this can be rationalized by the evidence supplied by dabigatran 110 mg twice a day as a study arm. For rivaroxaban, the patient specifications of the trial and the guidelines for the reduced dose are almost overlapping. Therefore, it would not be wrong to expect a real-life practice in accordance. However what we found is slightly different. Above 10% of patients, who do not need dose reduction according to guidelines, are on rivaroxaban 15 mg every day. Utilizing an inappropriate reduced dose to one-third of the patients with nonvalvular AF with a high annual risk of stroke is a worrying pattern of practice.
No basic characteristic is identified as a determinant of physicians’ preference to choose a NOAC of the two, except for the renal function. In rivaroxaban group, the CrCl is significantly lower than the dabigatran group. Considering the elimination routes of the two NOACs, the physicians’ tendency of utilizing rivaroxaban in patients with poorer kidney function seems reasonable.
In the European guideline, valvular AF is defined as AF due to rheumatic valvular disease (predominantly mitral stenosis) and prosthetic heart valves. Considering the spectrum of valvular diseases this caused confusion in practice. The most recent American Heart Association/American College of Cardiology guideline overcomes this confusion by clearly defining the patients with valvular disease that NOACs are contraindicated. 23 However, in the time interval that this study was conducted, the only contemporary guideline was the European one. 5 That is the reason why we aimed to find out the physicians’ real-life choices in patients with nonrheumatic valvular diseases. In patients who had a recent echocardiography report in their records, mitral regurgitation was the most prevalent abnormality and 37.3% had SVD. In dabigatran group, this was lower and this is understandable because SVD was among the exclusion criteria in RE-LY trial. On the other hand, ROCKET-AF trial included patients with SVD (14%), and this might encourage physicians to utilize rivaroxaban more frequently in those patients. Utilization of both NOACs in patients with SVD in this real-life practice indicates that even the confusing definition of the European guideline is correctly interpreted by the physicians.
To investigate the efficacy and safety of NOACs in real-life setting was not the primary aim of this study. Thromboembolic event rate in this cohort is quite similar to the event rate of the Danish registry. In both treatment arms, major bleeding rates were lower than the bleeding rates seen in the relevant clinical trials. The major bleeding rate in dabigatran group of this study was similar to the rate of corresponding complication in Danish registry. The most frequent side effect of NOACs was dyspepsia and it is seen in dabigatran treatment arm. The rate of this side effect is similar to the RE-LY trial but interestingly in the real-life report from three centers from Sweden this complication is almost 50% less. Nevertheless, in both clinical trials and real-life setting, this side effect stays as the major cause of permanent discontinuation of dabigatran treatment. The permanent discontinuation especially in the dabigatran arm of this study is higher than the other registries and the RE-LY trial. Considering this with the high nonadherence rates, the only explanation that comes to mind is the poor counseling by the physicians, especially due to lack of sufficient time.
Limitations
Certain limitations of the present study need to be acknowledged, including the limited sample size and the short duration of follow-up period and retrospective nature. Data are derived from three tertiary centers; therefore, sampling bias may exist and the results may not represent the nationwide practice. However, since a database or nationwide AF registry currently does not exist, the results of this study will reflect some sort of real-life patterns of utilization of NOACs. A missing apixaban arm might be considered as another limitation, but it has to be noted that this NOAC is approved and reimbursed recently, which did not give us the opportunity to accumulate sufficient experience. The comparison of the efficacy and safety end points in dabigatran and rivaroxaban groups were the not primary aim of the study because of the limitations mentioned above.
Conclusions
This is the first study that investigates how the evidence from clinical trials and guideline recommendations related with NOACs are translated into real-life practice in Turkey. Universally, it is one of the first real-life clinical data sets including both dabigatran and rivaroxaban in almost equal proportions. The results of the present study indicate that, for initiation of NOAC therapy, the physicians’ adherence to the guidelines and interpretation of contemporary evidences are well. If they have solid evidence, by choosing the lower dose of dabigatran, for the sake of safety, they may sacrifice efficacy. The clinical and adverse events observed in this study were in accordance with the results of clinical trials and other published registries. Nonetheless, in order to evaluate the long-term efficacy and safety of these novel drugs, complimentary to randomized controlled trials, data from well-designed registries, including the new NOACs, are needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.