
Abstract
The aim of this study was to investigate the effects of different paclitaxel concentrations on platelet aggregation induced by adenosine diphosphate (ADP). This experiment involved platelet suspensions that were obtained from fasting morning blood specimens from healthy adult male volunteers aged 22 to 28 years. The effect of paclitaxel on platelet aggregation induced by ADP and the inhibition rate of platelet aggregation were calculated in 6 groups with varying concentrations of paclitaxel, respectively. The optimal incubation time and concentration of ADP were 10 minutes and 10 μmol/mL, respectively. When the concentration of paclitaxel increased, platelet aggregation induced by ADP increased accordingly. When the concentration of paclitaxel exceeded 0.1 ng/mL, the ability of ADP to induce platelet aggregation increased significantly with increasing paclitaxel concentrations. In all the 3 experimental groups, that is A, C, and AC groups, the ability to inhibit platelet aggregation was weakened as paclitaxel concentration increased. Paclitaxel can enhance platelet aggregation induced by ADP, and this ability was observed to increase as paclitaxel concentration increased. In conclusion, paclitaxel can reduce the ability of aspirin, clopidogrel, and aspirin combined with clopidogrel to inhibit platelet aggregation. Furthermore, the ability to inhibit platelet aggregation was weakened as paclitaxel concentration increased in all 3 experimental groups.
Introduction
Recently, percutaneous coronary intervention (PCI) has been the mainstream technique for the treatment of coronary heart disease. 1 It was determined that 468 000 patients used PCI in 2012, and about 750 000 stents were inserted. 2 The paclitaxel-eluting stent is a commonly used drug-eluting stent (DES) in clinics. 3 Paclitaxel is very suitable for the preparation of DES because it is fat soluble and likely to pass through the cell membrane. Furthermore, the paclitaxel dose used for antiproliferation of smooth muscle cells is much less than the dose required for antineoplastic drugs. 4 Approximately 90% of paclitaxel can remain in the high-polymer coating, but it is not clear whether the residual drugs are released slowly or retained within the polymer coating stent. Compared with bare metal stents, the total incidence of stent thrombosis (ST) in paclitaxel-eluting stents does not increase, but the incidence rate of late ST increases from 0.2% to 0.4% per year. 5 –8 According to recent studies, the formation of late ST after inserting a paclitaxel-eluting stent is associated with many factors. An important factor may be the premature discontinuation of the antiplatelet drug 9,10 because the adhesion, aggregation, and activation reactions of platelets are closely associated with the formation of the thrombus. 11,12
Aspirin and clopidogrel are 2 kinds of commonly used antiplatelet drugs in clinics. Aspirin can interdict the metabolism of arachidonic acid by inhibiting cyclooxygenase activation 13 and then reduce the generation of thromboxane A2 (TXA2). Thromboxane A2 has a strong role in accelerating platelet aggregation and blood vessel contraction, while prostaglandin I2 (PGI2) strongly inhibits platelet aggregation and vasodilation. Thromboxane A2 and PGI2 relatively balance and regulate the mechanism of normal hemostasis and thrombosis. Clopidogrel has a role in antiplatelet aggregation by inhibiting adenosine diphosphate (ADP)-inducing platelets. 14,15 However, the effects of paclitaxel on aspirin and clopidogrel for inhibiting platelet aggregation remain unclear. Therefore, the aim of this study was to explore the effects of different paclitaxel concentrations on aspirin and clopidogrel to inhibit platelet aggregation in vitro.
Materials and Methods
Collection and Preparation of Blood Specimens
Fasting venous blood specimens were collected during the morning from 3 healthy adult male volunteers aged 22 to 28 years (24 ± 1.4 years). The 3 volunteers had no chronic diseases and did not take any drugs that could affect their platelet function during the 2 weeks prior to the study. High-fat foods were avoided 1 day before blood sampling, and alcohol and wine were forbidden during the 12 hours prior to blood sampling. The collected blood specimens were immediately sealed and conserved at 15°C to 25°C. This study was conducted with approval from the Ethics Committee of Sichuan University, and written informed consent was obtained from all volunteers.
A total of 50 mL of blood was mixed with 3.8% sodium citrate (Sigma-Aldrich, Shanghai, China), and the solution was sealed and thoroughly mixed. Then, the mixed solution was centrifuged for 10 minutes at 1000 r/min (Heraeus, Germany), and the collected supernatant was platelet-rich plasma (PRP). The remaining blood was centrifuged for 10 minutes at 3000 r/min, and the collected supernatant was platelet-poor plasma (PPP).
The PRP (20 μL) was mixed to a 0.38 mL diluent of ammonium oxalate (Sigma-Aldrich, Shanghai, China); this solution was used to estimate platelet counts (the platelet counts were 250 to 300 × 109/L).
Determination of Platelet Aggregation Rate
Equal volumes of normal saline and 10 ng/mL paclitaxel (Sigma-Aldrich, Shanghai, China) were added to the platelet suspension liquid in the control and experimental groups, respectively. Platelet aggregation rates were determined after being induced by the same concentrations of ADP (3 μmol/mL) at different incubation times (ie, 1, 3, 5, 10, 15, 20, and 30 minutes), and the optimal incubation time was determined according to these results. Simultaneously, the maximum platelet aggregation rates were determined at different concentrations of ADP (ie, 1, 3, 5, 10, and 15 μmol/mL) under the same incubation time, the maximum rate of platelet aggregation was determined by intelligent blood agglutination instrument (TYXN-91, Shanghai Research Institute of Mechanical and Electrical Technology, Shanghai, China), and then the optimal concentration of ADP was determined.
Equal volumes of normal saline and different concentrations of paclitaxel were added to the platelet suspension liquid in the control and experimental groups, respectively. The following six experimental groups were formed according to the different concentrations of paclitaxel: P1 group (0.01 ng/mL), P2 group (0.1 ng/mL), P3 group (1 ng/mL), P4 group (10 ng/mL), P5 group (100 ng/mL), and P6 group (1000 ng/mL). Platelet aggregation rates were measured under the optimal incubation time and concentration of ADP.
In the 6 groups with different paclitaxel concentrations, we added equal volumes of 60 μmol/L aspirin (Sigma-Aldrich, Shanghai, China; group A), 10 μmol/L clopidogrel (Sigma-Aldrich, Shanghai, China; group C), aspirin combined with clopidogrel (group AC) in each experimental group and an equal volume of normal saline in the control group (group V). Platelet aggregation rates were further measured under the optimal incubation time and concentration of ADP.
Statistical Analysis
All statistical analyses were analyzed using the SPSS 17.0 software. 16 Pearson and Spearman rank correlation analyses were performed on data that were normally and nonnormally distributed, respectively. Data that were normally distributed were expressed as x̄ + s, and a paired t test analysis or independent t test was used to estimate the difference between the 2 groups. An analysis of variance (ANOVA) was used to compare differences among the 3 groups in the study and a pairwise comparison was performed using the Student-Newman-Keuls and least significant difference methods (α = .05).
Results
Effects of Paclitaxel on Platelet Aggregation Induced by ADP
The largest and smallest platelet aggregation values in the experimental (ie, paclitaxel) and control groups were detected at an incubation time of 10 minutes and 1 minute, respectively (P < .001). Higher levels of aggregation were detected at all incubation time points in the paclitaxel group compared with the control group (Figure 1). Therefore, the optimal incubation time was 10 minutes.
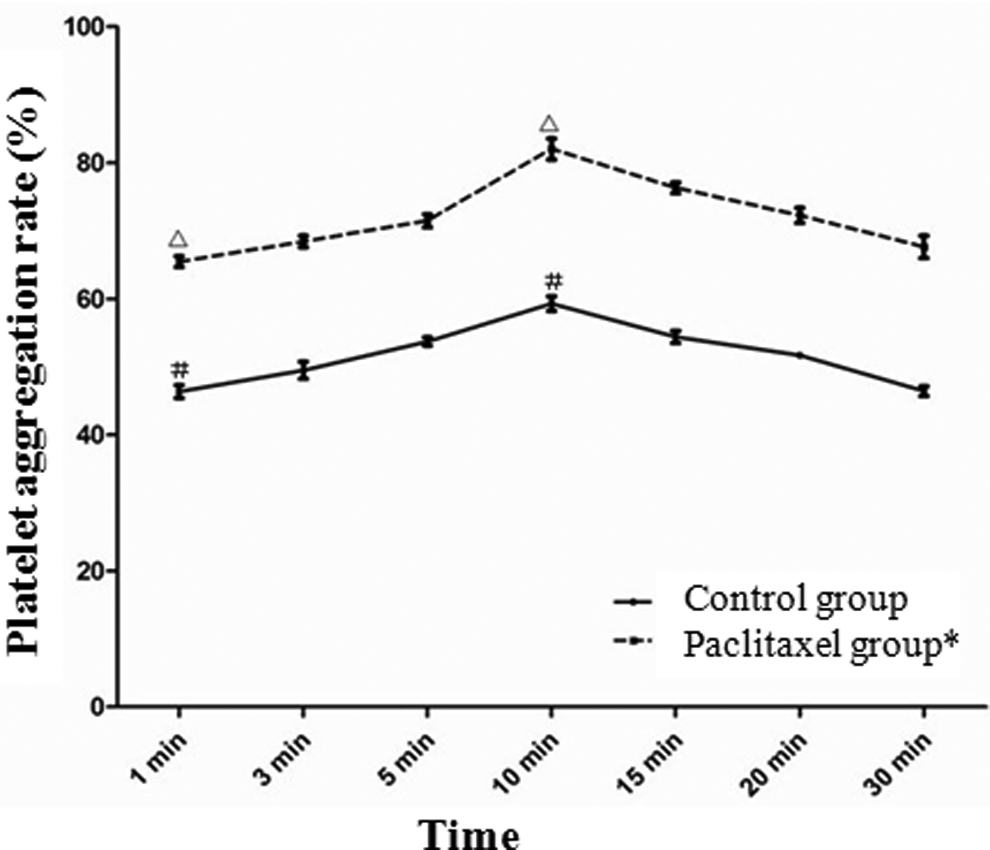
Platelet aggregation rates (%) in different incubation time points. * indicates that significant difference was detected between paclitaxel and control groups in different incubation time points (P < .001). ▵ indicates that significant difference was detected between paclitaxel groups when incubation times were 10 minutes and 1 minutes, respectively (P < .001). # indicates that significant difference was detected between control groups when incubation times were 10 minutes and 1 minutes, respectively (P < .001).
With increasing ADP concentrations, the largest and smallest platelet aggregation values in both the paclitaxel and the control groups were detected when the ADP concentration was 10 μmol/mL and 1 μmol/mL, respectively, at an incubation time of 10 minutes. Different aggregation values were detected when the ADP concentrations were 10 μmol/mL and 1 μmol/mL, respectively (P < .001, Figure 2), and 10 μmol/mL was selected as the optimal ADP concentration.
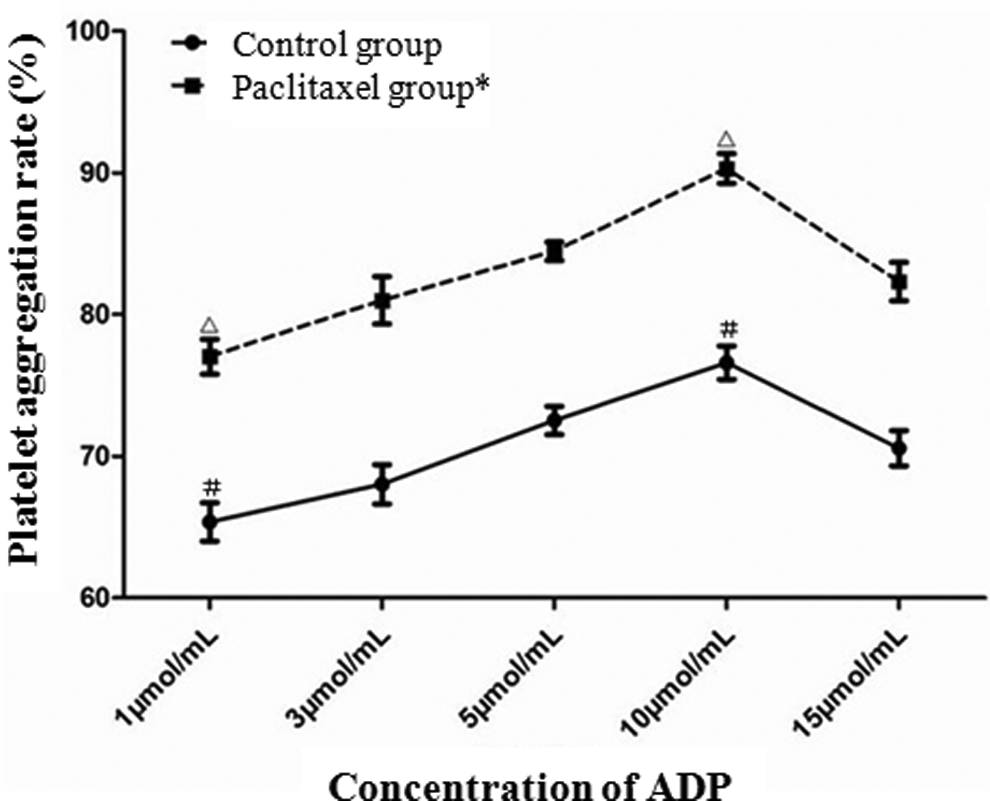
Platelet aggregation rates (%) in different concentrations of adenosine diphosphate (ADP). * indicates that significant difference was detected between paclitaxel and control groups in different concentrations of ADP (P < .001). ▵ indicates that significant difference was detected between paclitaxel groups when concentrations of ADP were 10 μmol/mL and 1 μmol/mL, respectively (P < .001). # indicates that significant difference was detected between control groups when concentrations of ADP were 10 μmol/mL and 1 μmol/mL, respectively (P < .001).
Under optimal experimental conditions, platelet aggregation induced by ADP and the promoting ratio of platelet aggregation increased as the paclitaxel concentrations increased. When the paclitaxel concentration exceeded 1 ng/mL, the platelet aggregative ability was rapidly increased with the paclitaxel concentration (Figure 3).
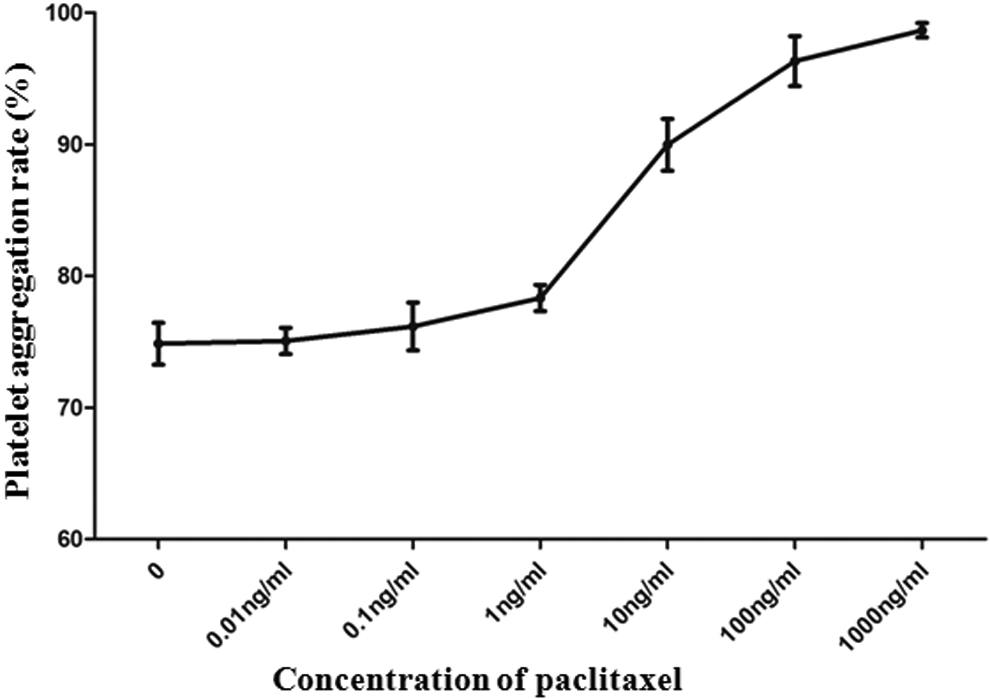
Platelet aggregation rates (%) induced by adenosine diphosphate (ADP) treated by different concentrations of paclitaxel.
Effects of Paclitaxel on Aspirin and Clopidogrel to Inhibit Platelet Aggregation
As the paclitaxel concentrations increased, the ability to inhibit platelet aggregation weakened and the inhibition ratio was also reduced (Tables 1 and 2). Clopidogrel also had similar characteristics. When the paclitaxel concentration was 0.01 to 1 ng/mL, the ability to inhibit platelet aggregation was the strongest in both paclitaxel and clopidogrel. However, when the concentration of paclitaxel exceeded 1 ng/mL, the ability to inhibit platelet aggregation was significantly weakened as paclitaxel concentrations increased; a significant difference was observed between groups A and V (P = .003) and groups C and V (P < .05).
Platelet Aggregation Rates (%) Induced by ADP in Different Concentrations of Paclitaxel Added Aspirin.

Abbreviation: ADP, adenosine diphosphate.
aIndicates that significant statistical difference can be detected between A and V groups (P = .003 < .05).
Inhibition of Platelet Aggregation Rates (%) induced by ADP in Different Concentrations of Paclitaxel Added Aspirin.

Abbreviation: ADP, adenosine diphosphate.
The ability of aspirin combined with clopidogrel to inhibit platelet aggregation was weakened as paclitaxel concentrations increased, and inhibition ratios were also reduced (Table 3 and Figure 4). The inhibition ability was strongest at a paclitaxel concentration of 0.01 to 1 ng/mL. However, the ability of combined aspirin and clopidogrel to inhibit platelet aggregation as paclitaxel concentrations increased was significantly weakened at a paclitaxel concentration >1 ng/mL. A significant difference could be detected between the groups AC and V (P = .009).
Platelet Aggregation Rates (%) Induced by ADP in Different Concentrations of Paclitaxel Added Aspirin Combined With Clopidogrel.

Abbreviation: ADP, adenosine diphosphate.
aIndicates that significant statistical difference can be detected between AC and V groups (P = .009 < .05).
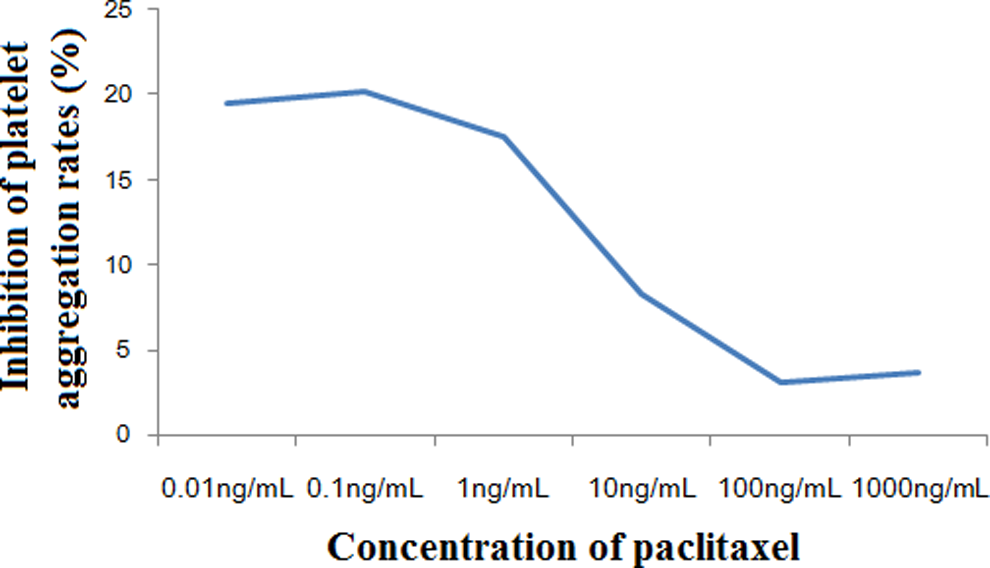
Inhibition of platelet aggregation rates (%) induced by adenosine diphosphate (ADP) in different concentrations of paclitaxel added aspirin combined with clopidogrel.
The platelet aggregation rates in groups A, C, and AC were gradually increased as the paclitaxel concentration increased from 0.01 to 1000 ng/mL (Figure 5). No significant difference in the aggregation rates was detected among the 3 groups (F = 0.099, P = .906). A significant difference was detected among the 3 groups at a paclitaxel concentration of 0.01 to 1 ng/mL when the paclitaxel concentrations were divided into 2 intervals (ie, 0.01 to 1 ng/mL and 10 to 1000 ng/mL). According to the pairwise comparison, there was no significant difference in the platelet aggregation rate between groups A and C; however, there was a significant difference between groups AC and A and groups AC and C (F = 9.064 and P = .015). No significant difference was detected among the 3 groups at the paclitaxel concentration interval of 10 to 1000 ng/mL (F = 0.033, P = .967).
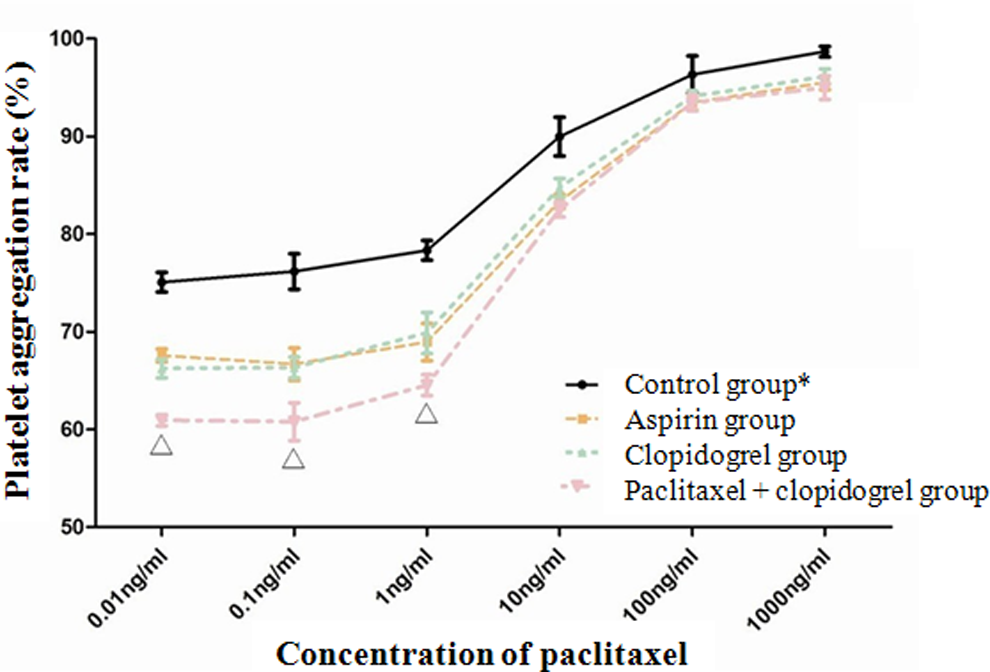
Platelet aggregation rates (%) in each group under different concentrations of paclitaxel. * indicates that significant difference was detected between control group and other 3 experimental groups in different concentrations of paclitaxel (P < .05). ▵ indicates that significant difference was detected among 3 groups when concentrations of paclitaxel were 0.01, 0.1, and 1 ng/mL, respectively (P < .05).
Discussion
Platelet aggregation is one of the most important clinical factors in hemostasis and thrombosis. 17,18 Platelet aggregation induced by ADP is reversible under a lower ADP concentration (<3 μmol/mL), which is the early gathered wave that can lead to ADP release and generate the second gathered wave. Platelet aggregation is irreversible under high ADP concentrations (>3 μmol/mL), which leads to all the platelets responding to exogenous ADP and immediately achieving the single gathered wave. 19 The optimal ADP concentration selected in this study was 10 μmol/mL, which was similar to the most commonly and clinically used range of ADP concentrations (5-20 μmol/mL). 20
According to previous animal experiments, the concentrations of paclitaxel in the blood plasma were 0.03 ± 0.04 μg/mL (after 6 hours) and 0.002 ± 0.003 μg/mL (after 24 hours) following the placement of a paclitaxel-eluting stent in a rabbit iliac artery. However, paclitaxel levels were not detected in the plasma after 72 hours and in 7 days. 21 According to these results, the paclitaxel concentration in the stent was higher than the blood paclitaxel concentration in systemic circulation. Therefore, the selected concentration of paclitaxel was from 0.01 to 1000 ng/mL in this study, which can better simulate the drug concentration in the internal paclitaxel stents.
We found that the ability of platelet aggregation rate to induce platelet aggregation increased as the paclitaxel concentration increased, and a rank correlation was detected between them (P < .001). When the paclitaxel concentration was >0.1 ng/mL, the ability of platelet aggregation rate to induce platelet aggregation rapidly increased as the paclitaxel concentration increased. The main reason for this may be that platelet aggregation was induced, and ST formation was promoted because of increased paclitaxel concentrations in the stent. Stahli et al 22 reported that paclitaxel can promote the expression of tissue factor through the activation of c-Jun NH2-terminal kinase and increase the expression of plasminogen activator inhibitor type-I in human coronary artery endothelial cells. 23 These factors may induce or promote the formation of ST. According to our findings, selecting a stent with a lower paclitaxel concentration (<1 ng/mL), as a method of artificial control, may contribute to an improvement in late ST.
Current handbooks recommend a daily dose of 75 to 325mg for oral aspirin and 75 mg for oral clopidogrel. 24 Plasma concentrations of aspirin and clopidogrel in those undergoing long-term oral treatments are 60 to 85 μmol/mL and 10 to 19 μmol/mL, respectively. 17 According to in vitro experiments, it has been proven that platelet aggregation induced by collagen can be inhibited and TXA2 generation can be reduced when the aspirin or clopidogrel concentration is 60 μmol/mL or 10 μmol/mL, respectively. 14 In this study, the selected concentration of aspirin and clopidogrel was 60 μmol/mL and 10 μmol/mL, respectively.
A combined drug treatment is most commonly used for the clinical treatment of antiplatelet aggregation. 25,26 Compared to the independent use of aspirin or clopidogrel, a lower platelet aggregation rate can be detected when the combination of aspirin and clopidogrel was used at the same paclitaxel concentration. Although no significant differences of platelet aggregation rate were observed among the 3 groups using ANOVA (P > .05), a significant difference was found in the ADP concentration interval of 0.01 to 1 ng/mL (P < .05) but not 10 to 1000 ng/mL (P > .05). According to these findings, the higher the paclitaxel concentration, the smaller the effect of the combined aspirin and clopidogrel treatment on inhibiting platelet aggregation. Simultaneously, dual antiplatelet therapy contributes to the inhibition of ST formation by acting on different targets.
Some patients have different reactions for the same dose of clopidogrel in clinic, and even part patients have no reactions, which are named clopidogrel resistance. The mechanism of clopidogrel resistance is still not clear, and it may be derived from combination of multiple internal and external factors. Gene polymorphism is reported as a major internal factor and also including other factors, such as increased release of ADP and upregulation of other platelet aggregation approaches (collagen, thrombin, d-thromboxane, etc). External factors are associated with clinical practice, including interaction between drugs, insufficient dose of drug, inappropriate indications or drug delivery way, and patients with poor compliance. 27 –29 Whether placing paclitaxel-eluting stent is a influencing factor that can lead to different reactions for clopidogrel? Moreover, drug-eluting balloons has been applied in clinic, and some select paclitaxel as eluted drug. Whether these devices may influence effects of clopidogrel? All of these problems are worthy of our thinking and further research.
In summary, paclitaxel can enhance platelet aggregation induced by ADP, and this ability was observed to increase as paclitaxel concentration increased. Furthermore, paclitaxel can reduce the ability of aspirin, clopidogrel, and aspirin combined with clopidogrel to inhibit platelet aggregation.
Footnotes
Authors’ Note
Shu Zhang and Changli Sun contributed equally to this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by science and technology support plan of Sichuan Science and Technology Agency (No. 2014SZ0004-2).