
Abstract
Venous thromboembolism (VTE) is the most common preventable cause of hospital death; the burden of VTE includes the management of the acute event (deep vein thrombosis [DVT]/pulmonary embolism) and the chronic subsequents such as postthrombotic syndrome and recurrent DVT. All experts agree that despite the abundance of knowledge available on VTE and how to prevent it, it is still underused, and since the first step in prophylaxis is to identify those who are at high risk of VTE, several risk assessment models have been developed to identify these patients and provide appropriate prophylaxis. In our study, the institutional guideline in a tertiary educational hospital is the Caprini score (2006), a comparison was conducted between the institutional guideline and the American College of Chest Physicians guideline (ACCP ninth edition [ACCP-9]) in terms of the degree of agreement of the actual prophylaxis with the institutional guideline and the ACCP-9 and the differences in risk levels. The concordance with the ACCP-9 guideline was higher than with the institutional guideline, specifically in those patients receiving prophylaxis, and there was an overestimation of the risk levels in the institutional guideline, especially in medical patients. The replacement of the existing Caprini-2006 with the ACCP-9 is prudent, since it agrees with the physicians’ clinical judgment and may result in reduced use of pharmacologic prophylaxis which could lead to lower costs and fewer adverse effects.
Keywords
Introduction
Venous thromboembolism (VTE) is the formation of a clot within the veins of either the lungs leading to pulmonary embolism (PE) or the legs leading to deep vein thrombosis (DVT). 1 In most cases, DVT starts in the calf, and it rarely causes symptoms if it is confined to the calf. However, if the initiating prothrombotic stimulus is severe, it will extend to affect the proximal veins and may eventually cause PE. Postthrombotic syndrome within 5 years affects 50% of the patients, especially those with recurrent ipsilateral DVT. Despite diagnosis and treatment, PE causes death in 15% of the patients. 2
Hospitalization and nursing home residency (current or recent) are considered responsible for almost 60% of cases with VTE in the community. Among hospitalized patients, medical illness and surgery account for 22% and 24% of the cases, respectively. 3 Appropriate prophylaxis significantly lowers the prevalence of VTE from 3.44% to 0.06% in hospitalized medical patients 4 and has also shown to be effective and safe in reducing VTE among surgical patients. 5
Some risk factors necessitate provision of VTE prophylaxis like major surgery, multiple trauma, hip fracture, or lower extremity paralysis because of spinal cord injury. Other risk factors, such as previous VTE, increasing age, prolonged immobility, cardiac or respiratory failure, presence of central venous lines, estrogens, and hematological conditions are not sufficient by themselves to warrant prophylaxis, but they increase the risk of VTE. 6 Although a lot is known about VTE and how to prevent it, but the medical and economic burden is still high. This gap between the availability of effective preventive measures and what is happening in practice today is caused by failure to regularly implement evidence-based interventions in patients with high risk of VTE. 7
Since the first step in provision of appropriate VTE prophylaxis is identifying those who are at high risk of VTE, several risk assessment models (RAMs) have been developed in medical and surgical patients, but RAMs for VTE in medical patients lack generalizability and proper validation, and dynamic and independently validated RAMs are needed for VTE assessment. 8
The objective of this study is to compare patients’ VTE risk and agreement of actual VTE prophylaxis with the American College of Chest Physicians guideline 9th edition (ACCP-9) for VTE prophylaxis 9 –11 and the institutional guideline, which is an adaption of the Caprini (2006) risk assessment sheet (Caprini-2006). 12
Methodology
This is an observational cross-sectional study conducted at the Jordan University Hospital (JUH) in Amman, Jordan. The JUH is an educational tertiary care hospital. The institutional guideline is an adaption of the Caprini score 12 in the form of risk assessment sheet that is mandatory upon admission in every patient file. According to hospital policies, the Caprini score should be filled and if required, appropriate prophylaxis is ordered by the physician. The different modalities for prophylaxis include pharmacologic prophylaxis (low-dose unfractionated heparin and low-molecular-weight heparins) and nonpharmacologic prophylaxis like intermittent pneumatic compression devices and graduated stockings.
Inclusion Criteria
The patients were randomly selected according to their file number, only those patients with an odd file number were eligible for the study. Patients who met the following inclusion criteria were included in the study: age ≥18 years, not receiving anticoagulant therapy, and at least 24 hours hospital stay. The medical wards included cardiology, nephrology, gastrointestinal, and respiratory. Surgeries in the surgical ward included vascular, abdominal, endocrine, urologic, and orthopedic surgeries. Patients who met the inclusion criteria were approached for consent form until the number of sample was achieved.
Procedure
The data were collected by the researcher using a case report form that contained the relevant and important data. The data were assembled from files and patients interviews. The data included demographics (age, gender, weight, height, and hospital stay), medication (type, strength, dosage, and route of administration), medical information (reasons for admission for medical patients, VTE risk factors, type of surgery, and previous surgeries for surgical patients), and laboratory data (hemoglobin, alanine aminotransferase, aspartate aminotransferase, platelets, serum creatinine, activated partial thromboplastin time, and prothrombin time). Risks of bleeding were recorded according to the ACCP-9 categories (medical nonsurgical, surgical nonorthopedic, and orthopedic). The type of VTE prophylaxis, dose, and duration were documented, and cost issues concerning the benefits of implementing the ACCP-9 guideline was estimated.
All the patients were assessed for agreement with the ACCP-9 and the Caprini-2006 for appropriate VTE prophylaxis in terms of the implementation of the guideline recommendations (whether the patient needed or didn’t need prophylaxis). Patients in the surgery ward were categorized into 2 groups, those who had an operation were categorized as “surgical patients” and those who were admitted for evaluation or were not operated upon at the time of inclusion in the study were considered as “surgical ward medical patients.” The surgical patients were stratified to very low-, low-, moderate-, and high-risk groups according to the ACCP-9 guideline and low-, moderate-, high-risk, and highest risk groups according to the Caprini-2006. The medical ward patients were stratified to low- and high-risk groups according to the ACCP-9 guideline and low-, moderate-, high-risk, and highest risk groups according to the Caprini-2006.
The risk factors for every patient were assessed according to both the ACCP-9 guideline and the Caprini 2006. The recommendations for VTE prophylaxis were either the same or different; if the recommendations differed, the comparison between the ACCP-9 guideline and the Caprini-2006 was conducted in the following manner: if both guidelines recommended pharmacologic prophylaxis (with or without mechanical prophylaxis) the recommendations were considered to be the same. Any guideline that recommended pharmacologic prophylaxis versus choosing either pharmacologic or mechanical prophylaxis was considered to place the patient at a higher risk level. Any guideline that recommended pharmacologic prophylaxis versus mechanical prophylaxis was considered to place the patient at a higher risk level. Any guideline that recommended mechanical prophylaxis versus no prophylaxis was considered to place the patient at a higher risk level.
Sample Size Calculation
A previous study that was conducted to evaluate the appropriate VTE prophylaxis in the JUH in 2006 reported that the rate of appropriate VTE prophylaxis was estimated as 26%. After the study was published, the hospital adopted the institution guideline for VTE prophylaxis using the Caprini score. The sample size of our study was calculated based on the assumption that after the implementation of the Caprini score, the rate of appropriate prophylaxis at least doubled to 52%
13
which suggested a sample size of 350 based on the following equation
14
:
where P is the proportion expected = 52%, Q = 1 − P, (1.96)2 = (Zα/2)2, α is type 1 error = 5%, and E is the margin of error = 10%, N = 350.
Statistical Analysis
The data were analyzed using the statistical software IBM SPSS Statistics version 20. Frequency and percentage were used to summarize categorical data, N (%), and quantitative data were described using the mean (mean ± standard deviation). Chi-square was used to test for statistically significant difference in categorical data. P values less than .05 were considered statistically significant.
Results
Data collection started in September 2013 and ended in January 2014. Of the 361 patients who were eligible for the study, only 7 patients refused to give consent. Three hundred and fifty-four patients were included in the study; 220 (62.1%) patients in the medical ward and 134 (37.9%) in the surgical ward, details are shown in Figure 1.
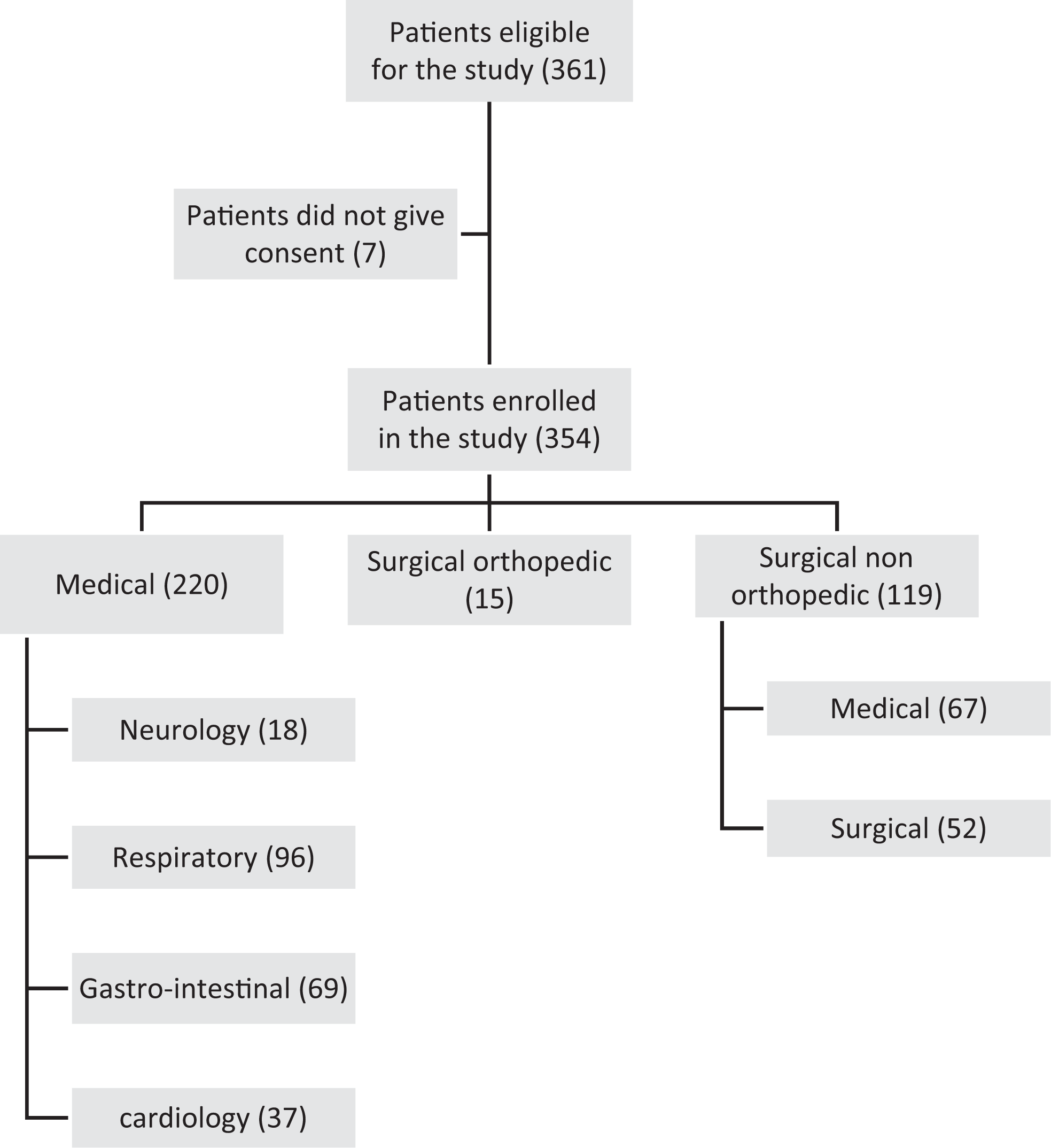
Study patients’ recruitment flowchart.
More than two-thirds of all patients were older than 40 years, and about 40% of them were obese. The general characteristics of the patients are summarized in Table 1. According to the Caprini 2006, 34.2% of the patients enrolled in the study were in the high-risk group (Caprini score 3-4), 29.4% in the highest risk group (Caprini score ≥ 5), 18.9% in the low-risk group (Caprini score 0-1), and 17.5% in the moderate-risk group (Caprini score 2). The mean hospital stay was the highest in the surgical orthopedic patients (12.13 ± 5.50 days).
General Characteristic of the Patients.
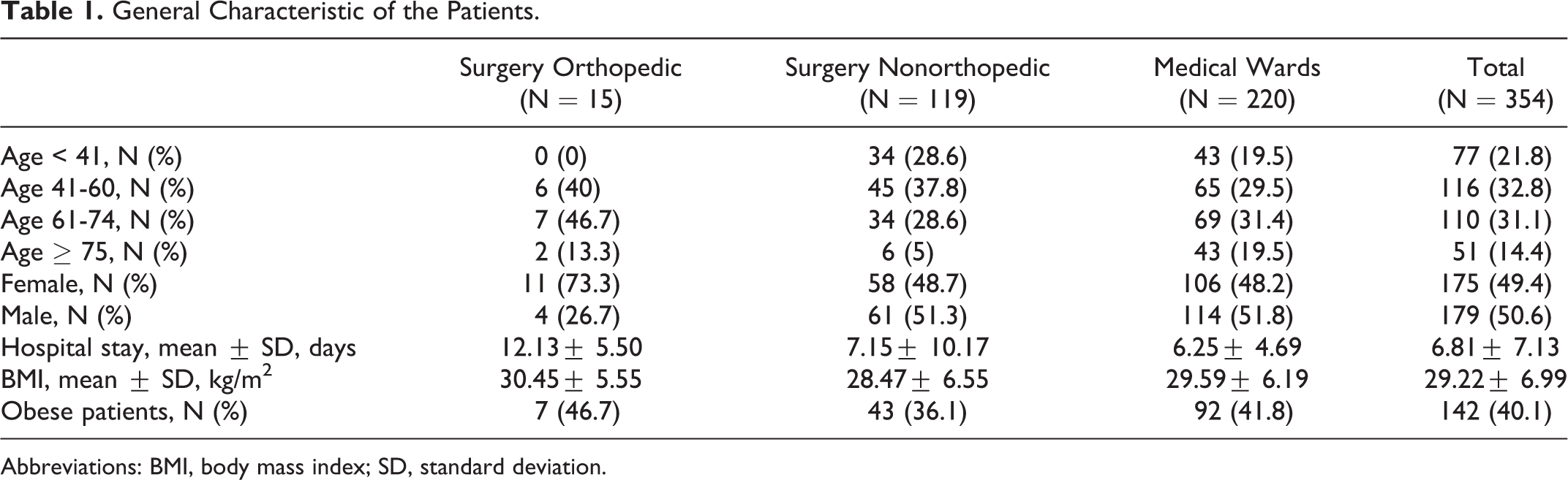
Abbreviations: BMI, body mass index; SD, standard deviation.
In the surgery ward and according to the Caprini 2006, the high-risk and highest risk groups accounted for more than half (59.6%) of the surgical patients, 15.4% of patients were in the low-risk group, and 25% were in the moderate-risk group. As for the medical patients in the surgery ward, most (62.7%) of the patients were in the high-risk and highest risk group. In the medical wards, the respiratory ward had the highest frequency of the high or highest Caprini risk group (78.1%). Details of frequency of the Caprini risk groups in medical wards are shown in Table 2.
Frequency of Caprini Risk Groups in Medical Wards.

According to the ACCP-9 guideline, surgical patients were classified as follow: 8 (15.4%) were in the very low-risk group, 9 (17.3%) in the low-risk group, 22 (42.3%) in the moderate-risk group, and 13 (25%) in the high-risk group. Among the medical patients of the surgery ward, 58 (86.6%) were in the low-risk group and 9 (13.4%) in the high-risk group.
The degree of agreement with the ACCP-9 was higher than with the Caprini-2006 in the total number of patients (74.9% vs 59.89%, P < .0001). Among surgical patients, the VTE prophylaxis was in agreement with the ACCP-9 in 63.5% of the patients and in agreement with the Caprini score in 53.8%. In medical patients of the surgery ward, the rate of agreement with the ACCP-9 recommendations was 79.1% (n = 53) and with the Caprini recommendations was 44.8% (n = 30). Among the medical wards, the extent of agreement with the Caprini-2006 was 62.72% and the agreement with the ACCP-9 guidelines was 75%. These values were higher or lower depending on whether patients were receiving prophylaxis or not.
In the surgical nonorthopedic patients, 71.7% (51.9% + 19.2%) of the recommendations regarding surgical patients were almost the same in Caprini and ACCP-9 guidelines. In 9.6% (5.8% + 3.8%) of the surgical patients, the ACCP-9 overestimates the risk, and in 19.2% (3.8% + 9.6% + 5.8%) of the patients, the Caprini overestimates the risk (Table 3).
Comparison Between the ACCP Guideline, Ninth Edition (ACCP-9) and the Caprini Risk Groups in Surgical Nonorthopedic Patients.
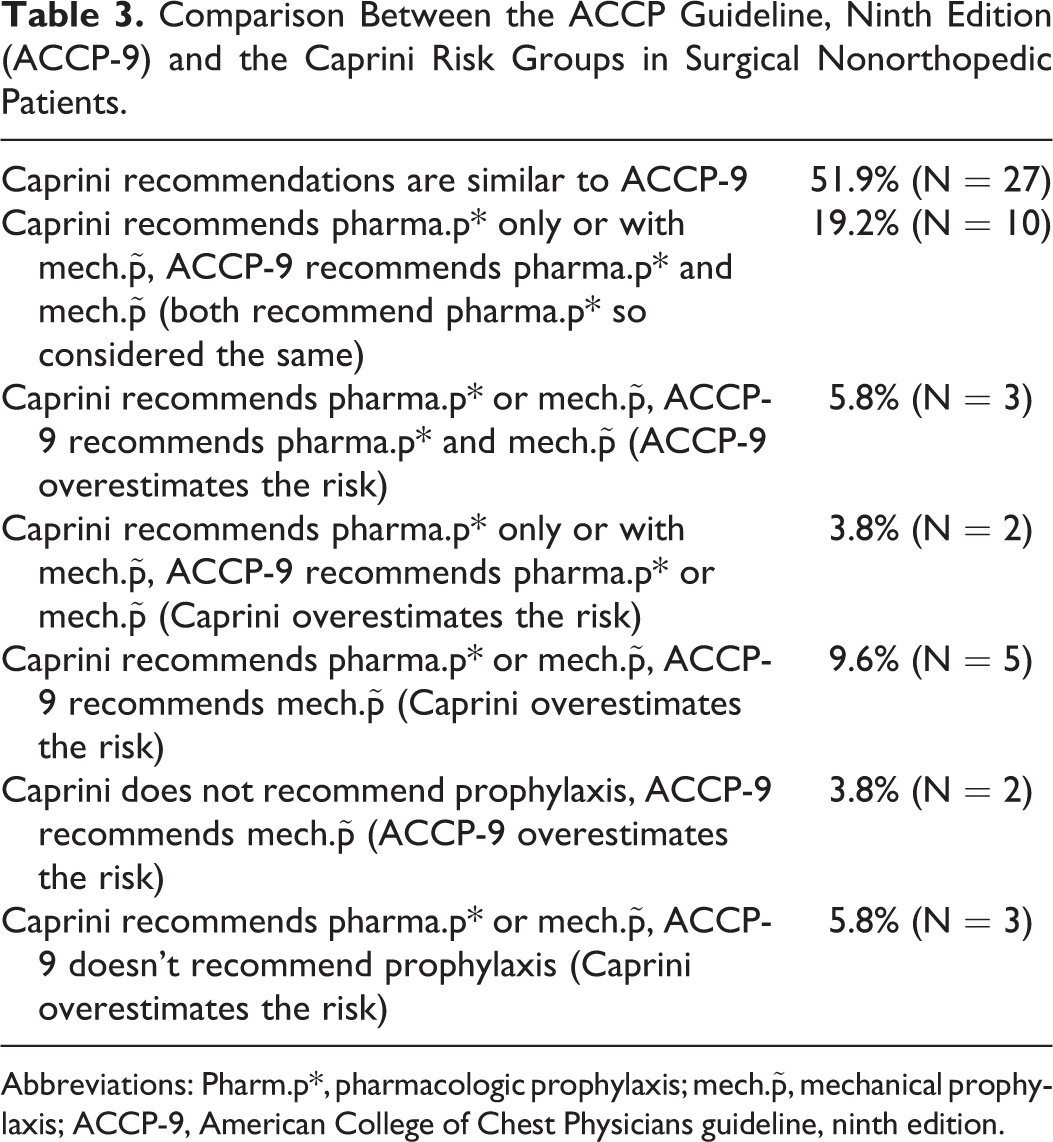
Abbreviations: Pharm.p*, pharmacologic prophylaxis; mech.
In the medical patients of the surgery ward, the Caprini score overestimated the risk in 71.7% (62.7% and 9%) of the cases, while the ACCP-9 overestimated the risk in 7.5% of patients. In the medical wards, the recommendations were the same in 38.2% of the patients. The Caprini score overestimated the risk in 52.7% (40.9% + 11.8%) of the patients, and the ACCP-9 guideline overestimated the risk in 9.1% of the patients.
The cost issues were estimated based on the recommendations of the ACCP-9 guidelines in both Jordanian dinar (JOD) and American dollar (US$). In total, according to ACCP-9 guidelines, 61 (17%) cases of overuse were detected (the patients were taking pharmacologic prophylaxis but did not need it) at an average cost of 4 JODs (US$5.6) for every subcutaneous injection of enoxaparin (the most commonly used pharmacologic prophylaxis) daily. Since the mean hospital stay in surgical and medical wards was 7 days, then every patient would cost 28 JODs (US$39.4) during the patient’s hospital stay.
Discussion
The proportion of patients who received appropriate prophylaxis recommended by the ACCP-9 2012 was 74.9%; this percentage exceeds the 36.9% of ACCP-9 2004 appropriate prophylaxis in the Middle East region revealed by the Assessment for VTE Management in Hospitals in the Middle East (AVAIL ME) study. 15 The appropriate prophylaxis according to Caprini score was 59.9%, which is double the percentage reported by the study conducted in the same institution several years ago, which was 26%. 13 These values show an improvement in the frequency of appropriate VTE prophylaxis. Surprisingly, results from all wards were more in agreement with the ACCP-9 rather than the Caprini-2006, which is enforced by the institution. This was especially evident among the medical wards patients and the medical patients of the surgical ward. This result showed that physicians’ clinical judgment is in agreement with the ACCP-9 guideline rather than the Caprini 2006, which could suggest a lack of confidence by the physicians in the recommendations of the Caprini score. When the patients were further categorized according to provision of VTE prophylaxis, those patients not receiving prophylaxis had a higher agreement with the ACCP-9 than the Caprini-2006, while those receiving prophylaxis had a lower agreement with the ACCP-9 than Caprini-2006. This indicates that there is a tendency of Caprini-2006 to overestimate risk. Further analysis reveals a 19.2% increase in the risk level of surgical nonorthopedic patients in the Caprini-2006 compared to the ACCP-9. The ACCP-9 risk assessment for the surgical nonorthopedic patients is the modified Caprini, which was validated retrospectively by Bahl et al. 16
In the medical wards, there was a 43.6% overestimation of the risk level in the Caprini-2006, this is due to the fact that the ACCP-9 guideline for the medical patients uses the Padua prediction RAM 9 and it differs significantly from the Caprini score. The Padua score includes 11 risk factors with 1, 2, and 3 scoring points, and pharmacologic prophylaxis starts at accumulative score of 4, while the Caprini-2006 includes 41 risk factors with 1, 2, 3, and 5 scoring points and prophylaxis whether pharmacologic or nonpharmacologic starts at a cumulative score of 2.
Limitations
Although the recommendations based on the ACCP-9 guideline, which had a lower VTE risk estimation than the Caprini-2006 especially in medical patients, could have resulted in lower pharmacotherapy rates and savings, the effect on the reduction in bleeding events due to a decrease in the rate of pharmacologic prophylaxis was not estimated. This difference has not been measured in terms of incidence of clinical outcomes such as DVT/PE. This study was performed only in the general surgery ward and 4 medical wards, further studies should be performed in other wards of the hospital as well as other hospitals to account for variability if any.
Conclusion
The agreement of VTE prophylaxis in the JUH with the ACCP-9 guideline was higher than with the Caprini-2006. The Caprini-2006 overestimates the VTE risk in hospitalized patients, especially in medical patients which could lead to higher levels of pharmacologic prophylaxis and possibly an increase in costs and bleeding events. It is recommended that Caprini-2006 is replaced with the ACCP-9. The suggested form is summarized in a form of a concise—1 page—VTE risk assessment sheet as the new institutional guideline (Figure 2).
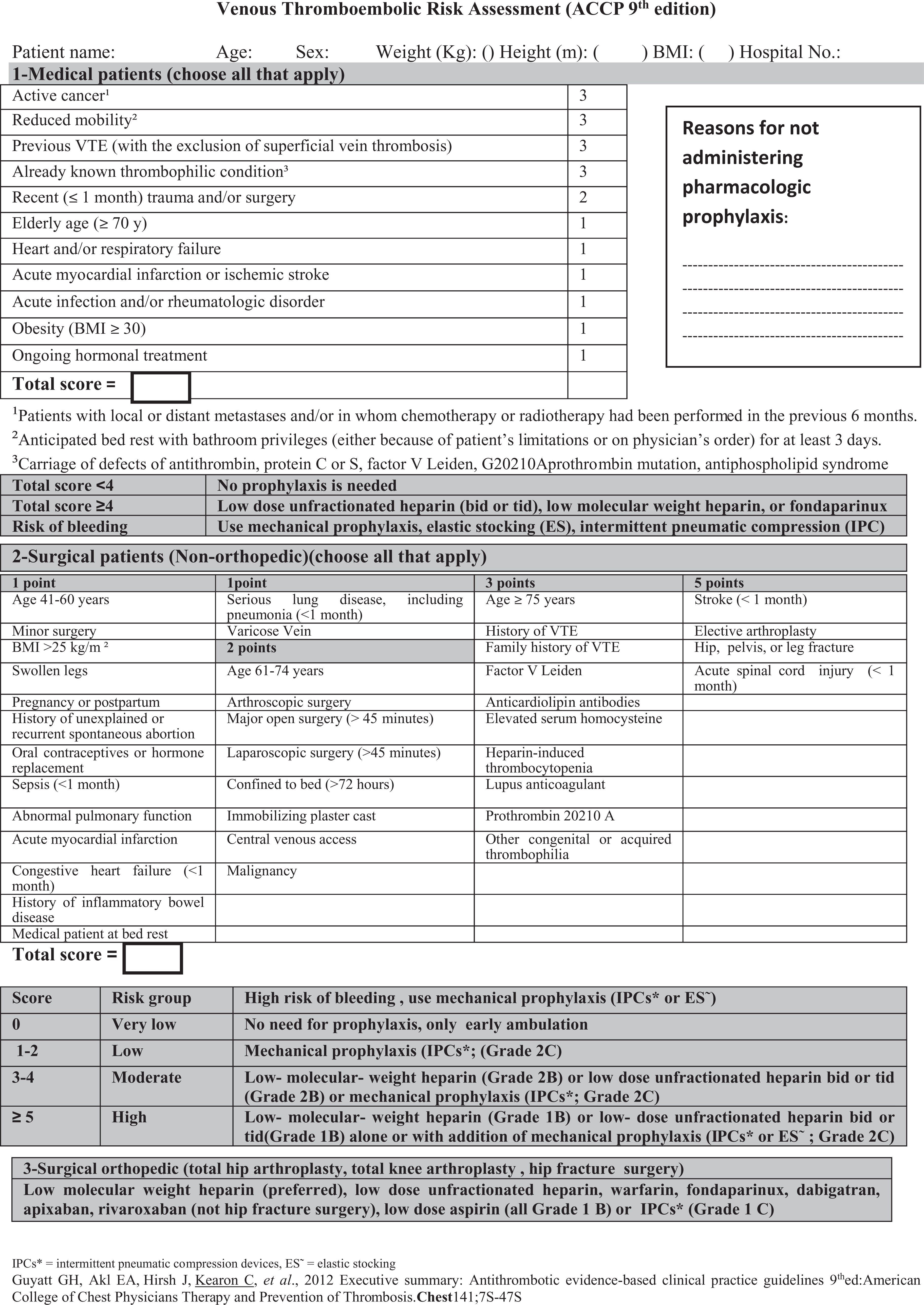
Recommended American College of Chest Physicians (ACCP) guideline, 9th edition risk assessment sheet and recommendations for venous thromboembolism (VTE) prophylaxis.
Footnotes
Acknowledgments
We thank the physicians, nurses, and pharmacists of the Jordan University Hospital for their cooperation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.