
Abstract
Background:
The pharmacokinetic properties of enoxaparin may lead to supratherapeutic antifactor Xa (anti-Xa) levels and increased bleeding when standard treatment doses are used in patients with morbid obesity.
Objective:
To evaluate the dose of enoxaparin needed to achieve therapeutic anti-Xa levels in a prospective, masked observational cohort of heterogeneous inpatients with morbid obesity and to determine whether patients with morbid obesity treated with 1 mg/kg of enoxaparin are at increased risk of supratherapeutic levels and bleeding events compared to patients receiving lower doses.
Methods:
Hospitalized patients with a body mass index ≥40 kg/m2 or actual body weight ≥140 kg and prescribed treatment doses of enoxaparin >60 mg per day were enrolled and consented to phlebotomy for determination of anti-Xa levels.
Results:
Forty-one patients were included for data analysis. The dose of enoxaparin that resulted in therapeutic and supratherapeutic anti-Xa levels at steady state was 0.83 mg/kg and 0.98 mg/kg (−0.11; 95% confidence interval [CI] −0.20 to −0.01, P = .02), respectively. Enoxaparin dose as mg/kg of actual body weight was an independent predictor of having a supratherapeutic anti-Xa level. Patients with doses <0.95 mg/kg versus ≥0.95 mg/kg were less likely to have supratherapeutic levels (odds ratio 0.21 [95% CI 0.05-0.84], P = .02) and had similar rates of subtherapeutic levels. Doses <0.95 mg/kg and ≥0.95 mg/kg resulted in similar bleeding rates of 17.9% and 22.2% (P = .71), respectively.
Conclusion:
Patients with morbid obesity required less than the recommended 1 mg/kg enoxaparin dose to achieve therapeutic peak anti-Xa levels; therefore, initiation with lower dosages is prudent and anti-Xa monitoring should guide dosage adjustments.
Introduction
The incidence of obesity has grown to over 33% in the United States, and hospital admissions of obese patients have proportionally increased. 1,2 With the exclusion of ST-segment elevated myocardial infarction, the recommended treatment dosing of enoxaparin is 1 mg/kg twice daily based on actual body weight (ABW) with no dosing limit. 3 The volume of distribution (Vd) of enoxaparin is roughly equivalent to plasma and does not distribute into adipose tissue. 4 –8 This pharmacokinetic characteristic may increase the antithrombotic activity of enoxaparin in extremely obese patients compared to nonobese patients with the risk of elevated antifactor Xa (anti-Xa) levels, which are associated with increased bleeding events. 9 –12 The American College of Chest Physicians’ guidelines and the College of American Pathologists recommend monitoring the antithrombotic effect of low-molecular-weight heparins (LMWHs) in special populations, including patients with obesity, using the anti-Xa assay with a target peak therapeutic range of 0.6 to 1 IU/mL for twice-daily enoxaparin treatment dosing. 13,14
Clinical studies evaluated enoxaparin with weight-based or fixed dosage regimens, without prospective correlation of clinical outcomes with anti-Xa levels. Stratification by body mass index (BMI) showed no differences in major bleeding events with obese patients in these trials. 15,16 However, the average dose in the obese population was less than the recommended 1 mg/kg dosage. 16 Lower doses are routinely prescribed in this population without prospective trials to guide this practice. 11,17 –19 The aim of the current study was to prospectively evaluate the doses of enoxaparin that achieve therapeutic target anti-Xa levels and to assess the safety and efficacy of current practice dosing strategies in a population of patients with morbid obesity. Our hypothesis was that patients with morbid obesity who received the recommended weight-based enoxaparin dose would be more likely to have supratherapeutic anti-Xa levels and be at a higher risk of bleeding.
Methods
Study Population
This study was a prospective observational cohort study of adult patients with morbid obesity at Houston Methodist Hospital, a tertiary care academic referral center with 5 intensive care units and 824 operating beds. Patients were identified through daily screening of the electronic medical record between October 2011 and June 2012. All patients receiving treatment doses of enoxaparin (greater than 60 mg/d) with a BMI greater than 40 kg/m2 or ABW greater than 140 kg were evaluated for inclusion criteria and enrolled consecutively. These weight descriptors were based on gaps in the existing literature concerning inpatients with morbid obesity receiving treatment enoxaparin dosing, in addition to a perceived dosing cap at the study institution. Patients were excluded if they had renal dysfunction, defined as an estimated glomerular filtration rate (eGFR) less than 30 mL/min using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) calculation, 20 or required hemodialysis (HD), had an expected length of treatment less than 36 hours, received once-daily dosing of enoxaparin, were pregnant, or were unable to provide informed consent. Upon enrollment, patients were assigned a unique, coded study identifier that was used for laboratory assays. At our institution, there is a dose-rounding protocol of enoxaparin to the nearest 10 mg; there are no institutional parameters or protocols for treatment dosing of enoxaparin in obese patients. Initial and subsequent adjustments in enoxaparin dosing were at the discretion of the primary treatment team; there was no intervention by the study investigators. This study was approved by the Institutional Review Board at Houston Methodist Hospital, and informed consent was obtained from all participating patients.
Anti-Xa Monitoring
Enrolled patients had 6 blood samples drawn on a protocol-defined schedule, consisting of 2 distinct series. The first series of blood samples included a trough blood sample immediately prior to the second or third dose of enoxaparin, a peak blood sample 4 hours after the same dose, and a second trough immediately prior to the subsequent dose. The second series of samples began before the fourth or fifth dose with the same methodology as the first series. Nursing staff were educated on the study protocol and documented the time of blood samples drawn and enoxaparin doses administered on study documentation forms. Deidentified research labels were attached to the blood samples for blinding purposes. Blood samples were anticoagulated by adding 2.7 mL of whole blood to 0.3 mL of 0.109 mol/L sodium citrate, mixed well, and immediately delivered to the coagulation laboratory. After centrifugation, plasma was stored in a designated −70°C freezer. Anti-Xa levels were measured in the citrate anticoagulated plasma using a chromogenic anti-Xa activity assay with reagents and instruments from Diagnostica Stago Inc (New Jersey). The coefficient of variation for anti-Xa assays in our laboratory is 6%. Study investigators remained blinded to the anti-Xa laboratory results during data collection and determination of bleeding and thrombotic events. Anti-Xa results from the study were not entered into the electronic medical record so as to not influence treatment decisions. It was at the discretion of the primary treatment team to order anti-Xa levels for the purposes of monitoring or guiding treatment; these were not included for the purposes of this study.
Outcomes
The primary outcome was the mean dose of enoxaparin (mg/kg) that resulted in therapeutic peak anti-Xa levels at steady state, defined as a blood sample drawn 3 to 5 hours after at least the third enoxaparin dose. 14 Houston Methodist Hospital’s therapeutic range for peak enoxaparin levels is 0.6 to 1.0 IU/mL. Secondary outcomes included the percentage of patients who had therapeutic, subtherapeutic (<0.6 IU/mL), and supratherapeutic (>1.0 IU/mL) anti-Xa levels that received the recommended 1 mg/kg ± 5% dose of enoxaparin (≥ 0.95 mg/kg group) versus those with lower doses (< 0.95 mg/kg group), and the rate of bleeding and thrombotic events associated with dose and correlating anti-Xa levels. A new thrombotic event was defined as any new clinically confirmed symptomatic deep vein thrombosis (DVT) or pulmonary embolism (PE) in a patient being actively treated with enoxaparin, a new arterial thrombosis, or surgical intervention required for original treatment indication, despite medical management (eg, thrombectomy or femoral-popliteal bypass surgery). Bleeding events were classified as major, moderate, and minor. Bleeding was considered major if there was a decrease in hemoglobin ≥4 g/dL or hematocrit ≥12% within a 48-hour period, intracranial hemorrhage, or any retroperitoneal bleed confirmed by diagnostic imaging. Moderate bleeding was defined as a decrease in hemoglobin ≥3 g/dL or hematocrit ≥9% within a 48-hour period or any overt bleeding such as hemoptysis, hematuria, epistaxis, or evidence of a gastrointestinal bleed (eg, positive stool guaiac). Minor bleeding was defined as a decrease in hemoglobin ≥2 g/dL or hematocrit ≥6% within a 48-hour period or a documented injection site hematoma or ecchymosis without an associated decline in hemoglobin. Bleeding or thrombotic events with an undetermined severity categorization were adjudicated by a study physician (JM) blinded to the patient’s weight, enoxaparin dose, and anti-Xa levels.
One compartment pharmacokinetic analysis was performed to calculate Vd (dose/postdose peak—predose trough anti-Xa activity), half-life (t1/2) using first-order kinetics with ke/0.693, and total body clearance of enoxaparin (ke × Vd) using a one compartment model and to establish correlations between anti-Xa levels and dose to ABW, ideal body weight (IBW), 21 adjusted body weight (AdjBW), 22 lean body weight (LBW), 23 percentage of IBW, BMI, 24 and body surface area (BSA). 25 If a patient had only 1 blood sample drawn, unless the blood sample included the steady state peak therapeutic level required for the primary outcome, the patient was excluded from data analysis. If a patient developed renal dysfunction during the study protocol, as defined previously, they were also excluded from the data analysis.
The written and electronic medical records were reviewed by the study investigators for past medical history, comorbid disease states including known risk factors for bleeding and thrombosis, and concurrent pharmacotherapy. New diagnoses made during the admission of the study protocol are included as patient history. Laboratory monitoring of renal function, complete blood count, measures of anticoagulation as well as thrombotic and bleeding events were reviewed daily up until 48 hours after enoxaparin was discontinued or the patient was discharged.
Statistical Analysis
Due to the lack of previously published literature involving adult patients with morbid obesity and enoxaparin kinetics, we established sample size estimates based on historical data obtained from hospitalized patients within our institution. This estimate supported that approximately 35 patients would have a power of 80% to detect an absolute difference of 20% in mg/kg ABW enoxaparin dosing that would achieve therapeutic anti-Xa levels between the 2 dosing groups. Baseline variables between patients who received ≥0.95 and <0.95 mg/kg enoxaparin doses were tested for significance using the Student t test, Mann-Whitney U, chi-square, or Fisher exact test as appropriate. Mean with standard deviation was used for continuous data with a normal distribution; median with interquartile range (IQR) was used for continuous data that did not have a normal distribution. Data were tested for normality using the Anderson-Darling Normality Test, with a P value of <.05 signifying nonparametric data. Univariable logistic regression was performed for variables of interest and possible confounders to estimate crude association with development of a supratherapeutic anti-Xa level. The following variables were considered as possible predictors: categorization as ≥0.95 mg/kg or < 0.95 mg/kg enoxaparin dose, eGFR, and number of doses received. Variables with a P value <.20 in the univariable logistic regression analysis were entered into a multivariable model. Patients with missing steady state peak anti-Xa values were censored. The paired Student t test was used when comparing patients’ pharmacokinetic variables between the 2 anti-Xa series. An α value of .05 was set for statistical significance. All statistics were performed using Minitab Version 16 (Minitab, Inc, State College, Pennsylvania).
Results
Patient Characteristics
During the study period, 119 patients met the inclusion criteria of which 72 patients were excluded (Figure 1). Forty-one patients had at least 2 blood samples performed per study protocol and were included in the study cohort for data analysis (Table 1). The median patient weight was 138.1 kg (range 95.3-266.7), median BMI was 45.6 (range 36.8-92.1), and median duration of treatment was 3 days (range 2-12). The mean age of the study cohort was 55.9 years (range 18-81).
Patient flow diagram. Baseline Characteristics.a
Abbreviations: ABW, actual body weight; BMI, body mass index; CKD-EPI, Chronic Kidney Disease Epidemiology Collaboration; eGFR, estimated glomerular filtration rate; ICU, intensive care unit; IQR, 25%-75% interquartile range; SCr, serum creatinine; SD, standard deviation.
aData are represented as n (%) unless otherwise indicated.
bOnly 1 patient was included who weighed greater than 140 kg but had a BMI < 40 kg/m2; all other patients were included based on a BMI > 40.
cCKD-EPI eGFR = 141 × min (SCr/k, 1)a × max (SCr/k, 1) − 1.209 × 0.993Age × 1.018 (if female) × 1.159 (if black); k is 0.7 for females and 0.9 for males, a is −0.329 for females and −0.411 for males, min indicates the minimum of SCr/k or 1, max indicates the maximum of SCr/k or 1.
dPercentages do not add up to 100% due to patients with more than 1 treatment indication.
eIncludes a patient with lower extremity venous occlusion, 2 patients with arterial thrombosis, 1 patient with femoral-popliteal bypass with stent placement, 1 patient with an atrial appendage thrombus, 1 patient with aortic thrombus, and 1 patient with protein C and S deficiency.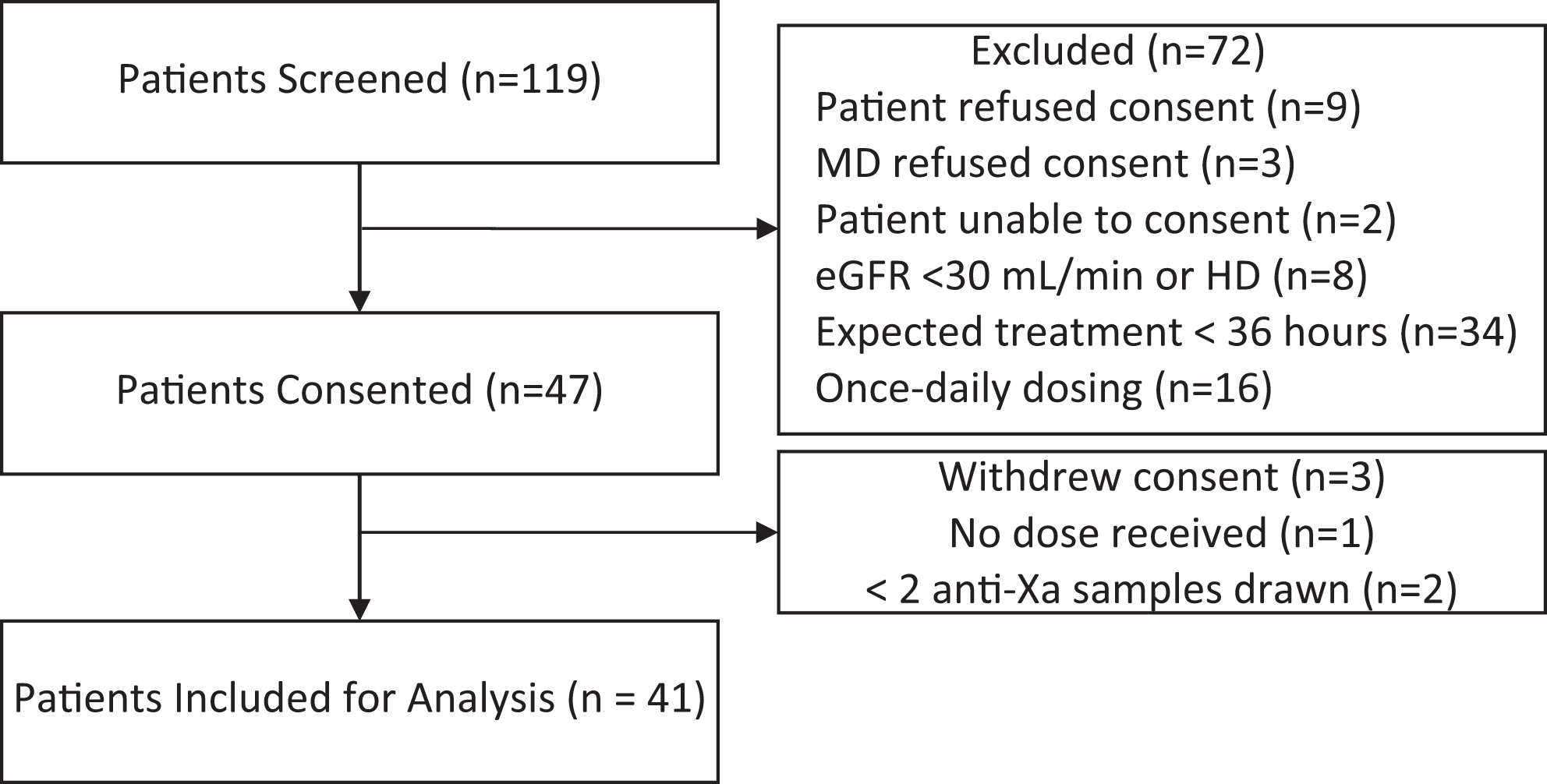
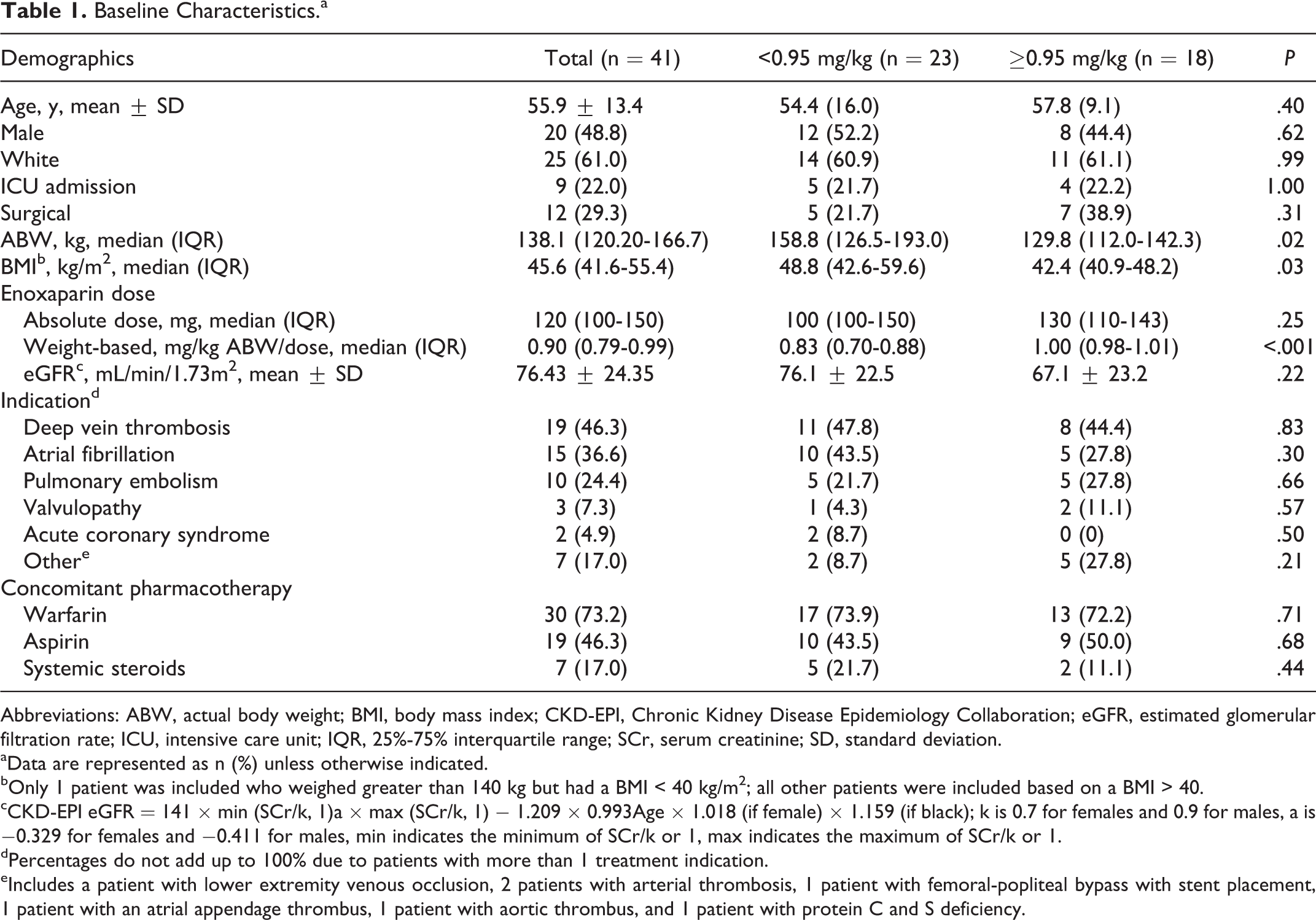
The median weight-based and absolute enoxaparin dose was 0.90 mg/kg (range 0.38-1.04) and 120 mg (range 60-160) every 12 hours, respectively. Twenty-three (56%) patients were prescribed enoxaparin doses ≤0.95 mg/kg per dose. These patients had significantly higher ABW and BMI. Higher ABW was associated with receipt of lower enoxaparin doses (odds ratio [OR] 1.03, 95% confidence interval [CI] 1.01-1.06, P = .01). There was no difference in baseline characteristics between the 2 dosing groups in age, renal function, indication, concomitant pharmacotherapy, or comorbid disease states. Fifteen patients weighed ≥150 kg (the largest prepackaged dose available from the manufacturer); 12 (80%) of these patients received less than the recommended enoxaparin dose versus 11 (31%) patients <150 kg (P = .02).
A total of 204 blood samples were obtained from the 41 patients included for data analysis. Twenty-four (59%) patients had complete series of blood samples drawn per protocol. Reasons for incomplete series were patient discharge before protocol completion (n = 10), conversion to an alternate anticoagulant (n = 4), and unavailability of the patient at a scheduled time for a blood sample (n = 3).
Achievement of Therapeutic Anti-Xa levels
Thirty-six (87.8%) patients had an appropriate steady state peak anti-Xa level drawn. In all, 14 (38.9%) patients had a therapeutic anti-Xa, 18 (50.0%) were supratherapeutic, and 4 (11.1%) were subtherapeutic. The median dose of enoxaparin that resulted in therapeutic and supratherapeutic anti-Xa levels at steady state was 0.83 mg/kg and 0.98 mg/kg (−0.11; CI −0.20 to −0.01, P = .02), respectively. The median dose of patients who were subtherapeutic was 0.72 mg/kg (P = not significant compared to patients who were therapeutic or supratherapeutic). Univariable logistic regression identified mg/kg dosing based on ABW as an independent predictor of having a supratherapeutic anti-Xa level at steady state, OR 0.21 for <0.95 mg/kg dosing versus ≥0.95 mg/kg dosing (95% CI 0.05-0.84, P = .02). Renal function was also found to be an independent predictor of developing a supratherapeutic anti-Xa level, OR 4.0 for eGFR <60 mL/min versus >60 mL/min (95% CI 0.95-16.77, P = .02). The effect of a higher enoxaparin dose and development of supratherapeutic anti-Xa levels remained significant when renal function was included as a covariate in the multivariable analysis (OR 0.21, 95% CI 0.05-0.92; P = .01). The number of doses received was not significant (OR 1.05, 95% CI 0.92-1.20, P = .47) and was not included in the multivariable analysis. Patients who received ≥0.95 mg/kg ABW enoxaparin doses had significantly higher anti-Xa levels than those who received <0.95 mg/kg ABW at all time points except the last trough (Figure 2); steady state peak anti-Xa levels were 1.38 ± 0.55 IU/mL versus 0.96 ± 0.28 IU/ML, respectively (0.41, 95% CI 0.04-0.78; P = .03). For the <0.95-mg/kg and ≥0.95-mg/kg dosing groups, anti-Xa levels were therapeutic in 52.6% versus 23.5% (P = .07) of patients, supratherapeutic in 31.6% versus 70.6% (P = .02) of patients, and subtherapeutic in 15.8% versus 5.9% (P = .35) of patients.
Antifactor Xa (anti-Xa)level time series. P, Peak; T, Trough; Series 1 included a trough blood sample immediately prior to the second or third dose of enoxaparin, a peak blood sample four hours after the same dose, and a second trough immediately prior to the subsequent dose. Series 2 began before the fourth or fifth dose with the same methodology as the first series. *p < 0.05.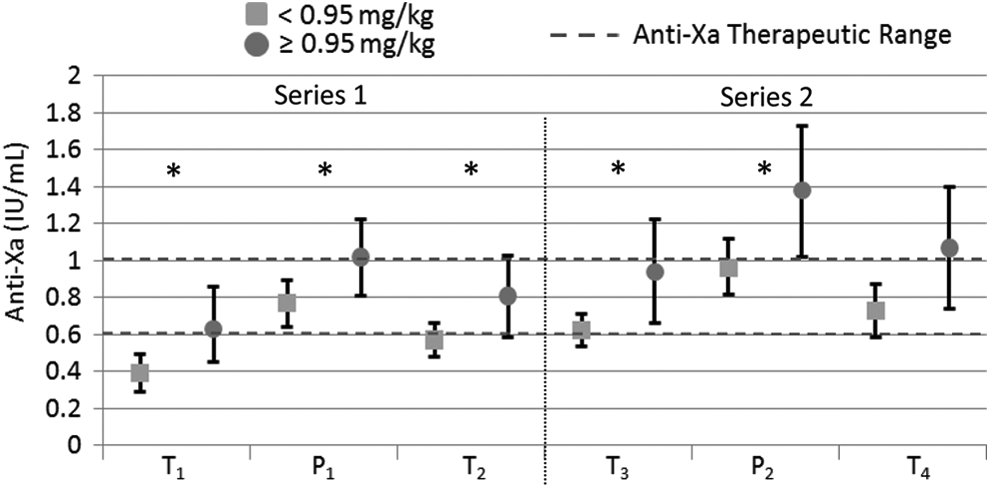
Clinical Events
Bleeding Outcomes.a
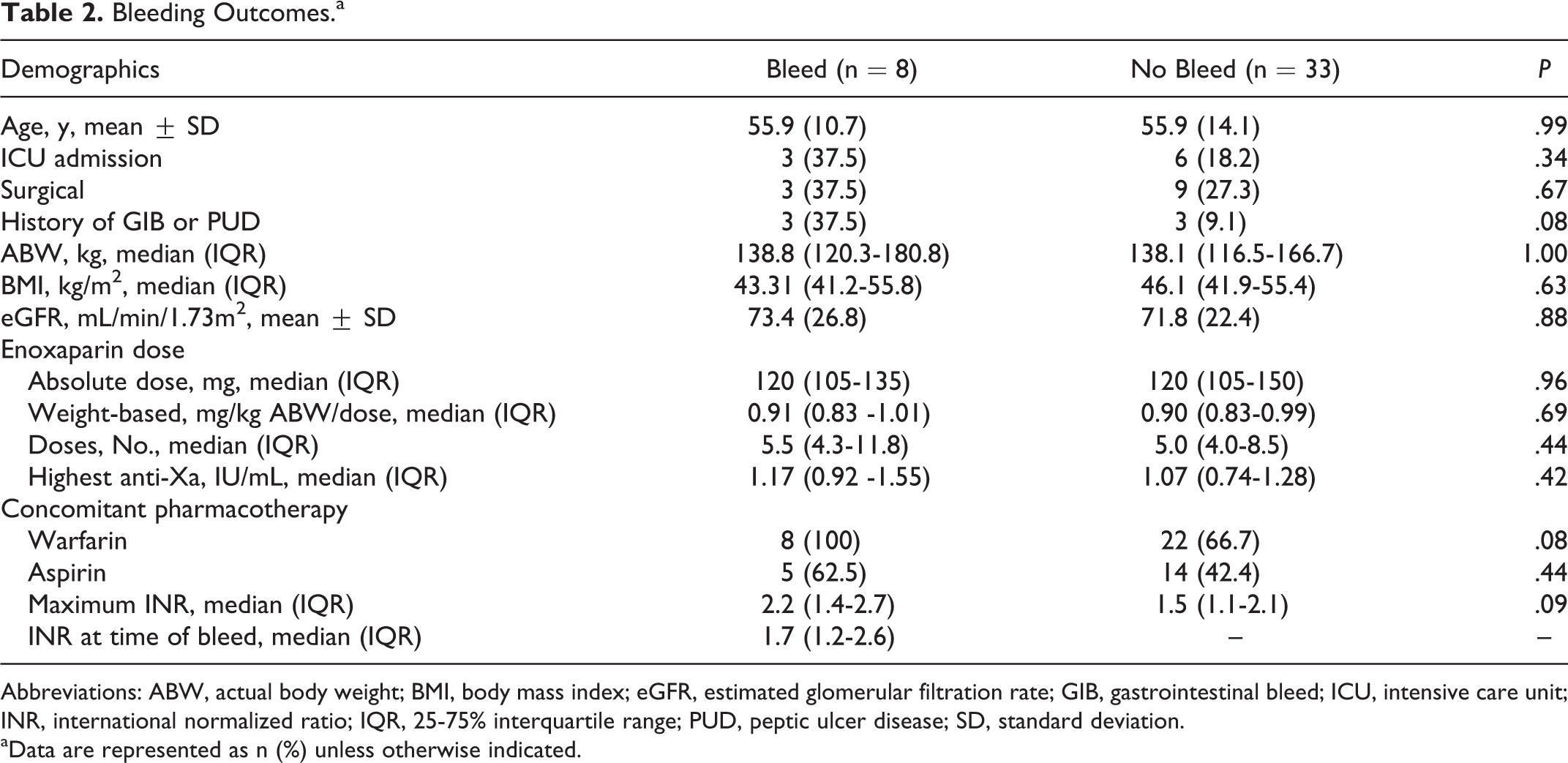
Abbreviations: ABW, actual body weight; BMI, body mass index; eGFR, estimated glomerular filtration rate; GIB, gastrointestinal bleed; ICU, intensive care unit; INR, international normalized ratio; IQR, 25-75% interquartile range; PUD, peptic ulcer disease; SD, standard deviation.
aData are represented as n (%) unless otherwise indicated.
Pharmacokinetics
Pharmacokinetics.
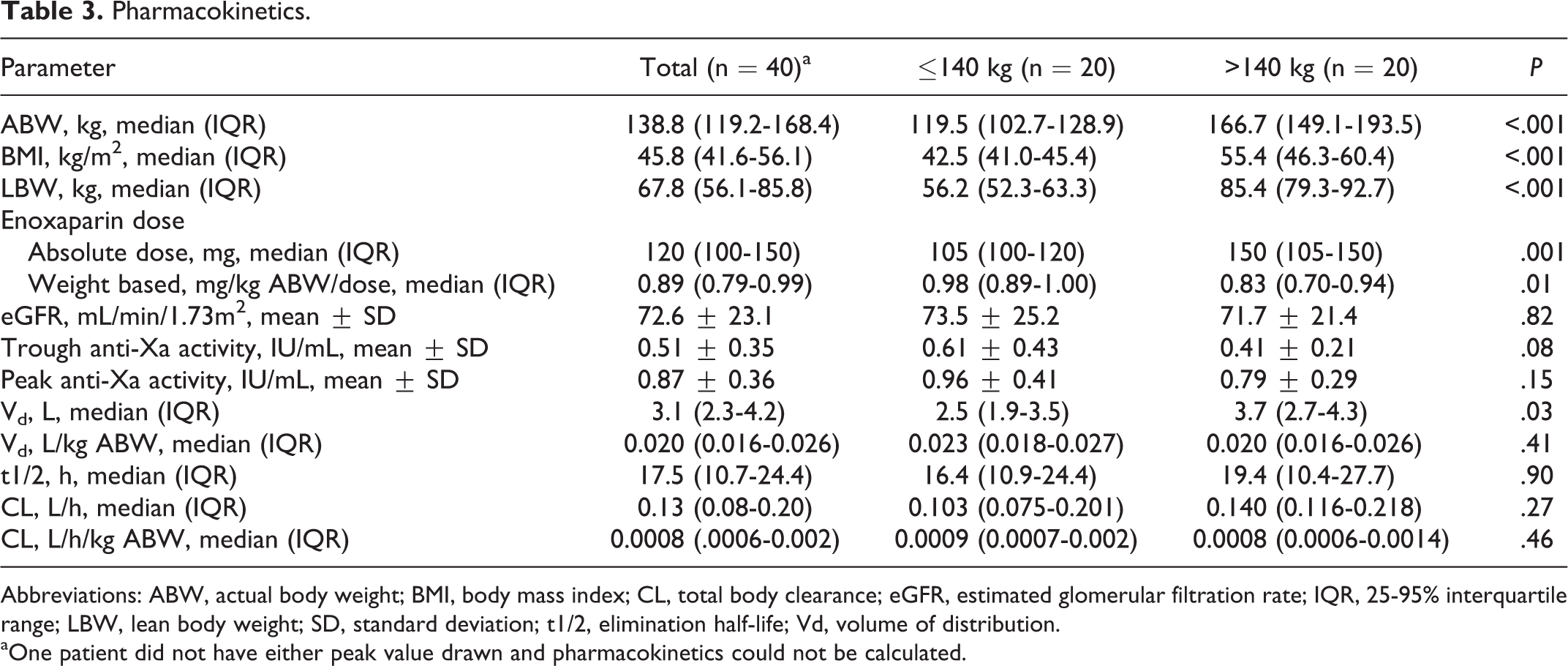
Abbreviations: ABW, actual body weight; BMI, body mass index; CL, total body clearance; eGFR, estimated glomerular filtration rate; IQR, 25-95% interquartile range; LBW, lean body weight; SD, standard deviation; t1/2, elimination half-life; Vd, volume of distribution.
aOne patient did not have either peak value drawn and pharmacokinetics could not be calculated.
Discussion
To our knowledge, this is the first prospective, blinded evaluation of enoxaparin dosing and anti-Xa levels in adult, hospitalized, morbidly obese patients. The dosing practices observed in our patient cohort were reflective of those seen in other reports, with 53% of patients receiving less than the recommended 1 mg/kg dose. 18,19 Fifteen patients in our cohort weighed ≥150 kg, but only 1 patient received an enoxaparin dose over 150 mg, reflective of an arbitrary dosing limit in practice. Despite the prevalence of underdosing in our cohort, over half of the patients had supratherapeutic anti-Xa levels, with only 4 subtherapeutic. The median dose that resulted in a therapeutic anti-Xa was 0.83 mg/kg ABW. This is similar to the 0.81 mg/kg ABW dose recently reported to result in therapeutic levels in pediatric patients with obesity, compared to 1.1 mg/kg dose for controls. 9 In a similar retrospective evaluation of adult patients with a BMI > 40 kg/m2, Deal and colleagues reported a dose of 0.74 mg/kg ABW in patients with therapeutic anti-Xa levels, compared to a dose of 0.85 mg/kg ABW in patients who were supratherapeutic. The mean anti-Xa levels for patients who bled and those who did not were 1.5 IU/mL and 0.95 IU/mL (P < .01), respectively. 10
Increased pharmacodynamic response to enoxaparin in obese patients is likely reflective of the drug’s Vd, which is roughly equivalent to plasma volume and reflects poor distribution into adipose tissue as well as altered pharmacokinetic parameters in obesity. 4 –8 Adipose weight and lean mass disproportionately increase as ABW increases, with a decrease in the LBW to adipose tissue ratio with increased total weight. 26 Blood volume, and in turn plasma volume, measured as mL/kg, similarly decreases nonlinearly with increasing total body weight. 27 Increases in kidney and liver mass, the organs responsible for drug clearance, increase nonlinearly with total body weight reaching a sex-specific asymptote around 100 to 150 kg. 28 Sanderlink and colleagues have previously reported a lower weight-adjusted Vd in obese patients compared to their nonobese controls. 6 The weight-adjusted Vd of 0.020 L/kg in our cohort is lower than 0.059 L/kg found in their analysis; this phenomena may be explained by the more extreme obesity in our cohort (mean ABW 138.1 kg and BMI 45.6 kg/m2, compared to 99.6 kg and 34.8 kg/m2). 6
We saw no significant difference in bleeding or thrombotic events for patients receiving 1 mg/kg versus those who received lower doses. The principal limitation was a small sample size with inadequate power to detect a difference in clinical events. Additionally, the protocol was a nonrandomized design, patients felt to be at a higher risk of bleeding may have been prescribed lower doses of enoxaparin further increasing β error. At this time, anti-Xa levels have not been prospectively correlated with clinical outcomes; however, several large registries suggest an increased risk of bleeding with enoxaparin in obese patients. In over 19 000 patients with acute coronary syndrome from the Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA guidelines (CRUSADE) registry, 80% of patients with an ABW >150 kg received less than the recommended 1 mg/kg dose of enoxaparin. Compared to patients who weighed <100 kg, these patients were found to have an increased risk of bleeding, despite significantly lower weight-based doses (0.65 vs 1.01 mg/kg, P < .0001). In addition, patients who weighed >150 kg who received 1 mg/kg of enoxaparin had a nonsignificant trend toward increased bleeding compared to patients >150 kg who received a lower weight-based dose (OR 2.42, CI 0.70-8.37). 11 The Computerized Registry of Patients with Venous Thromboembolism (RIETE) registry prospectively evaluated the use of anticoagulation in 8845 patients for the treatment of venous thromboembolism, stratified by body weight. The mean daily dose of LMWH (100 IU = 1 mg enoxaparin) was 148 IU/kg for patients weighing >100 kg versus 181 IU/kg for patients weighing 50 to 100 kg (P < .001), and the percentage of patients who received <175 IU/mL daily was 74% and 33%, respectively (P < .001). There were no differences in bleeding or thrombotic events observed between the groups in this large cohort, despite the significantly lower weight-based doses used in the larger patients. Patients with an ABW >100 kg were also more likely to receive unfractionated heparin for initial treatment compared to those <100 kg (17% vs 9%, P < .001), despite the fact that the patients with an ABW >100 kg were younger and had better renal function. 17 Enoxaparin has shown superiority to and is recommended over unfractionated heparin in several indications, and thus these patients may potentially be deprived of a superior treatment modality. 29
Conclusion
Consensus guidelines and the package insert recommend enoxaparin dosing of 1 mg/kg with no dosing limit, although a significant proportion of these patients receive lower dosing in practice. Patients with morbid obesity receiving the recommended dose are more likely to develop supratherapeutic anti-Xa levels and may be placed at increased risk of bleeding events. It may be prudent to initiate therapy at a lower initial dose in this patient population, and anti-Xa levels should be monitored and used for dose adjustments.
Footnotes
Acknowledgments
The authors would like to thank Kevin Garey, PharmD, MS, for his expertise with biostatistics.
Authors’ Note
The article has been reviewed in full and approved by all authors. N. Thompson-Moore, D. Putney, P. Nguyen, W. Chandler, and J. Muntz designed the study. N. Thompson-Moore, M. Wanat, D. Putney, and P. Nguyen consented patients for enrollment and performed data collection. N. Thompson-Moore and D. Putney analyzed the data. N. Thompson-Moore wrote the manuscript. M. Wanat, D. Putney, P. Nguyen, W. Chandler, and J. Muntz critically reviewed and revised the manuscript. All authors agreed to the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research was funded by Houston Methodist Hospital’s Department of Pharmacy.