
Abstract
The purpose of this study was to investigate a possible correlation between single-nucleotide polymorphisms (SNPs) of the antithrombin (gene, SERPINC1, and perioperative sensitivity to heparin in patients receiving heart surgery. The SERPINC1 genotype and allele frequency, coagulation parameters 24 hours before and after surgery, and clinical findings were compared among 3 ethnic groups, Han, Uighur, and Kazakh, patientswho received heart surgery. In Han patients, longer coagulation time as well as higher heparin and protamine dosage was observed. SERPINC1 gene sequencing identified 2 mutations in exon 5, g.981A>G (rs5877) and g.1011A>G (rs5878). The minor allele frequency of allele (A>G) for rs5877 and rs5878 was higher in the Han patients and was significantly different among the ethnic groups (P = .004 and P = .006, respectively). The increased SERPINC1 SNP frequency among Han patients receiving heart surgery might contribute to the differences in their perioperative sensitivity to heparin.
Keywords
Introduction
Effective anticoagulation is a prerequisite for successful heart surgery in the presence of cardiopulmonary bypass (CPB). However, failure to optimally reverse anticoagulation using heparin may cause fatal postoperative blood loss. Thus, perioperative management of coagulation is a determinant of successful heart surgery. At present, whole-blood activated clotting time (ACT) is used as an indicator in the management of coagulation. 1
Heparin acts rapidly and is easily counteracted by protamine; thus, it represents an ideal anticoagulant during heart surgery. 2 Heparin acts on antithrombin (AT) to exert its anticoagulation effect. 3 However, in clinical practice, interindividual and interethnic differences in the sensitivity to anticoagulation have been noted, which are characterized by differences in ACT after addition of the same dose of heparin as well as differences in the amount of protamine required to achieve a similar ACT. 3 For example, genetic studies have shown that the dose of warfarin used for anticoagulation maintenance in Chinese patients is significantly lower than that used for caucasian patients, which might be attributed to a polymorphism of the vitamin K epoxide reductase complex, subunit 1(VKORC1) gene promoter that differs among races. 4 –6 Similarly, an intronic polymorphism of the VKORC1 gene of Italian patients was associated with intraindividual variability in warfarin dose requirements. 7 In addition, associations between protein C (PROC) and epoxide hydrolase 1 (EPHX1) polymorphisms with warfarin dose in Han Chinese individuals have been reported. 4 It has been speculated that changes in AT levels or activity may account for the varying sensitivity to heparin, 3,8 which has resulted in studies analyzing the effects of AT supplementation to enhance heparin sensitivity. 9 However, the precise mechanism underlying these differences in perioperative response to heparin remains to be determined.
Antithrombin is a key factor in the heparin-induced anticoagulation cascade, accounting for 70% of the total anticoagulation activity 10 ; it also has anti-inflammatory effects. 11 Therefore, we hypothesized that SERPINC1 single-nucleotide polymorphisms (SNPs) might alter AT activity. Therefore, this study investigated the correlation between AT gene SNP and perioperative sensitivity to heparin in Uighur, Kazakh, and Han Chinese patients receiving heart surgery in the presence of extracorporeal circulation at the First Affiliated Hospital of Xinjiang Medical University in Urumqi. Urumqi is located in the northwest of China and is comprised of various ethnicities, including approximately 10.35 million Uighurs and Kazakhs. In 2012, 1158 patients received heart surgery in our hospital, of whom 375 were Uighurs, 197 were Kazaks, and 608 were Han patients. Thus, minorities accounted for about 50% of patients receiving heart surgery in our institution. In this study, 180 patients were enrolled, and their SERPINC1 genotype and allele frequency was compared along with their coagulation parameters and clinical findings. This analysis may uncover the mechanism underlying intraethnic differences in response to anticoagulation therapy and provide evidence for predicting heparin dosage requirements on an individualized basis.
Materials and Methods
Study Participants
Han, Uighur, and Kazakh patients (n = 60 per group), who received heart surgery, were recruited from the Affiliated First Hospital of Xinjing Medical University. Figure 1 shows the number of patients recruited from each ethnic group as well as the exclusion criteria. This cohort study was registered in the Chinese Clinical Trial Register (ChiCTR) as ChiCTR-OCH-12002708, which was established according to both the World Health Organization International Clinical Trials Register Platform Standard and the Ottawa Group Standard. This study was approved by the Ethics Committee of the Affiliated First Hospital of Xinjiang Medical University, and informed consent was obtained from every patient prior to enrollment in the study.
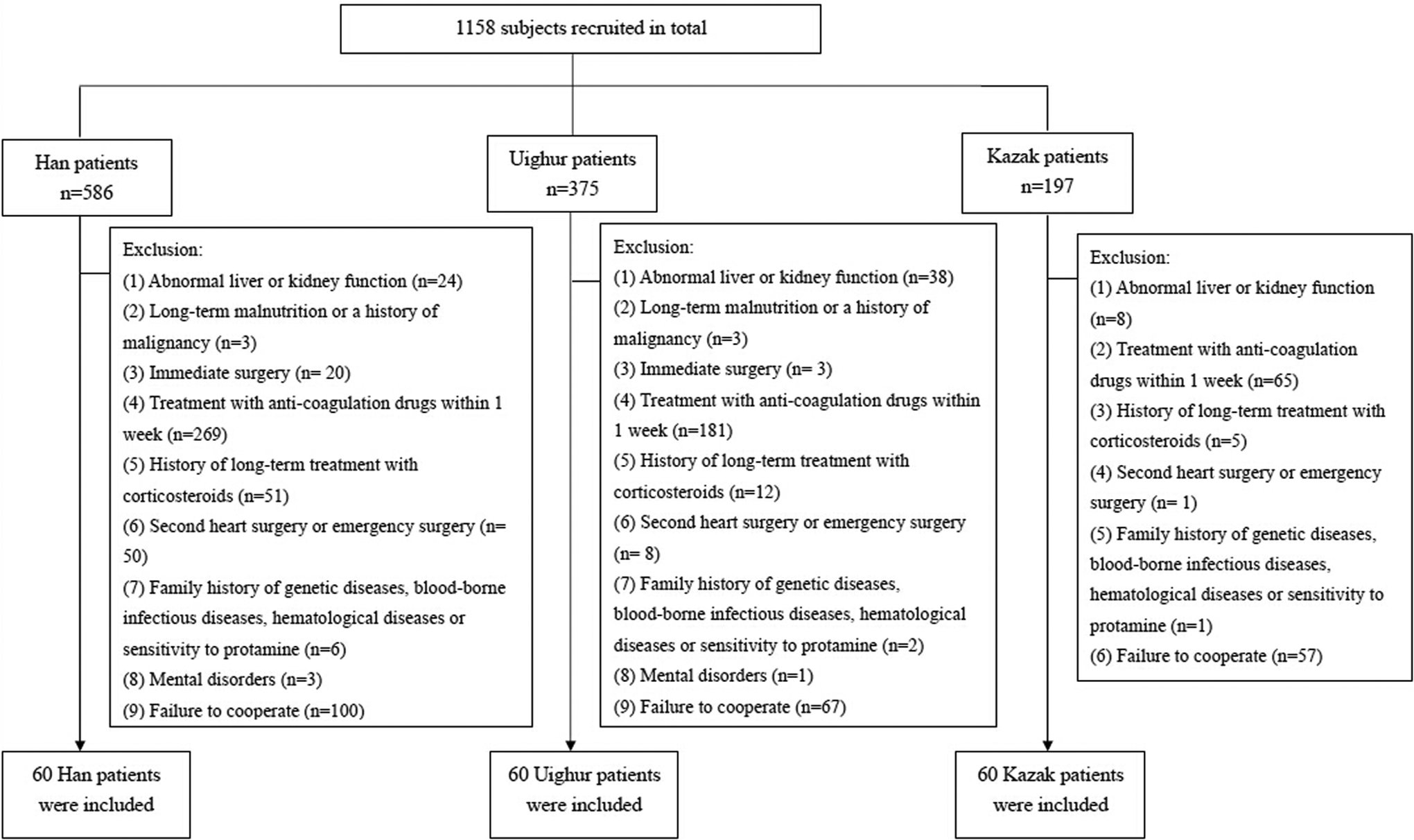
Patient recruitment and exclusion from the study.
Patients, who received selective heart surgery for valve replacement or congenital heart diseases (atrial or ventricular septal defect) and had relatives within 3 generations who were Hans, Uighurs, or Kazakhs were enrolled. Patients disclosed their ethnic backgrounds, which were confirmed by the local government office. In addition, the following inclusion criteria were applied for the present study: (1) age of 18 to 65 years, (2) no family history of thrombotic disorders, and (3) normal preoperative coagulation function.
Patients were excluded if they had 1 of the following: (1) abnormal liver or kidney function prior to surgery, (2) long-term malnutrition or a history of malignancy, (3) surgery immediately before the study, (4) treatment with anticoagulation drugs, such as heparin, oral aspirin, clopidogrel, warfarin, and ticlopidine, within 1 week before the surgery, (5) history of long-term treatment with corticosteroids, (6) second heart surgery or emergency surgery, (7) family history of hematologic genetic diseases (eg, thrombophilia), blood-borne infectious diseases, hematological diseases, or sensitivity to protamine, (8) mental disorders, and (9) refusal to participate due to privacy concerns (Figure 1). Long-term malnutrition was defined as weighing 15% to 20% less than the patient’s ideal body weight or having a body mass index (BMI; weight (kg)/[height (m)]2) of less than 18.5. Ideal body weight was calculated as follows: for males: (body height [cm] − 80) × 0.7 ± 10% and for females (body height [cm] − 70) × 0.6 ± 10%.
Coagulation Function Assessment
Venous blood (3.7 mL) was collected within 24 hours before and after surgery and anticoagulated with citrate at a ratio of 1:9, followed by detection of anticoagulation function by determining the activated partial thromboplastin time (APTT) and the prothrombin time (PT).
For AT activity, plasma was diluted with saline and incubated for 90 seconds with excess human factor IIa (FIIa) in the presence of heparin, forming an AT–thrombin–heparin complex. 12 Excess human FIIa catalyzes the release of p-nitroanaline from a chromogenic substrate. The absorbance measured at 405 nm is inversely proportional to the AT activity concentration in the sample.
For AT antigen level measurement, thrombin–antithrombin complex-derived human enzyme-linked immunosorbent assay kit (ab108907; AbCam China, Shanghai, China) was used in accordance with manufactures’ instructions. The Bio-Rad xMark microplate absorbance spectrophotometer (Bio-Rad, Hercules, California) was used for reading of all micro plates.
Anticoagulation Management
Perioperative heparin-induced anticoagulation management was carried out as described previously. 13 In brief, the threshold for coagulation function was set as an ACT value >480 seconds during extracorporeal circulation at the time of heart surgery. Protamine was used after the surgery to counteract the heparin-induced anticoagulation, thereby returning the coagulation state to normal.
Peri- and Postoperative Study Parameters
The turnaround time and auxiliary time of intraoperative extracorporeal circulation, the amount of heparin used to maintain the ACT at ≥480 seconds, the number of patients receiving blood transfusion, and the postoperative blood loss (drainage volume within 24 hour) were determined. In addition, the number of intensive care unit (ICU) days and hospital days was determined.
SERPINC1 Genotype and Allele Frequency
Whole blood (3 mL) was collected from the radial artery before surgery and stored at −80°C for subsequent SERPINC1 gene sequencing. Genomic DNA extraction from 200 μL of samples was performed using a whole-blood genomic DNA extraction kit according to the manufacturer’s instructions (Aidlab Inc, Beijing, China). The polymerase chain reaction (PCR) mixture included 2 μL of 10× EX Buffer, 1.6 μL of 2.5 mmol/L dNTP, 1 μL of forward primer, 1 μL of reverse primer, 1 μL of Ex Taq polymerase (5 U/µL), 1 μL of genomic DNA, and 12.4 µL ddH2O. Forward and reverse primers were designed and synthesized for all 7 exons of the SERPINC1 gene as described by Caspers et al. 14 Details of primers used for SERPINC1 genotyping and allele frequency analysis are listed in Supplementary Table 1. The reaction conditions were as follows: denaturation at 95°C for 10 minutes, 35 cycles of annealing at 60°C for 30 seconds and extension at 72°C for 45 seconds, and a final extension at 72°C for 10 minutes. Products were stored at 4°C until sequencing analysis. The PCR products were subjected to sequencing by Beijing Microread Gene Co, Ltd (Beijing, China)
Statistical Analysis
Continuous data were summarized by means ± standard deviations or medians and interquartile ranges (IQR; 25th and 75th percentiles), depending on the normality of the data distribution. Categorical data were expressed by frequencies and percentages. The differences among the 3 ethnic groups were detected by 1-way analysis of variance or the Kruskal-Wallis test for continuous data as well as the chi-square test or Fisher exact test for categorical data when applicable. Post hoc pairwise comparisons were performed using the Bonferroni approach to control for type I error. Comparisons of APTT and PT before and after the surgery were conducted using the Wilcoxon signed rank test. All statistical analyses were performed with SAS software version 9.2 (SAS Institute Inc, CaryNorth Carolina). A 2-tailed P < .05 indicated statistical significance.
Results
Baseline Characteristics
A total of 180 patients (120 males and 60 females), consisting of 60 Han, 60 Uighur, and 60 Kazak, were enrolled in this study. The age of the patients ranged from 18 to 75 years, with a median of 50 years (IQR: 41-59 years; Table 1). No significant differences in age, gender, BMI, ejection fraction, New York Heart Association (NYHA) Functional Classification (NYHA class), diagnosis of heart disease, length of ICU stay, length of hospital stay, and AT activity were observed among the 3 ethnic groups (Table 1). However, the mean antigen level was significantly higher in the Han group than in the Kazak group (105.3 vs 83.4, P = .004).
Baseline and Clinical Characteristics of Patients by Ethnic Background.
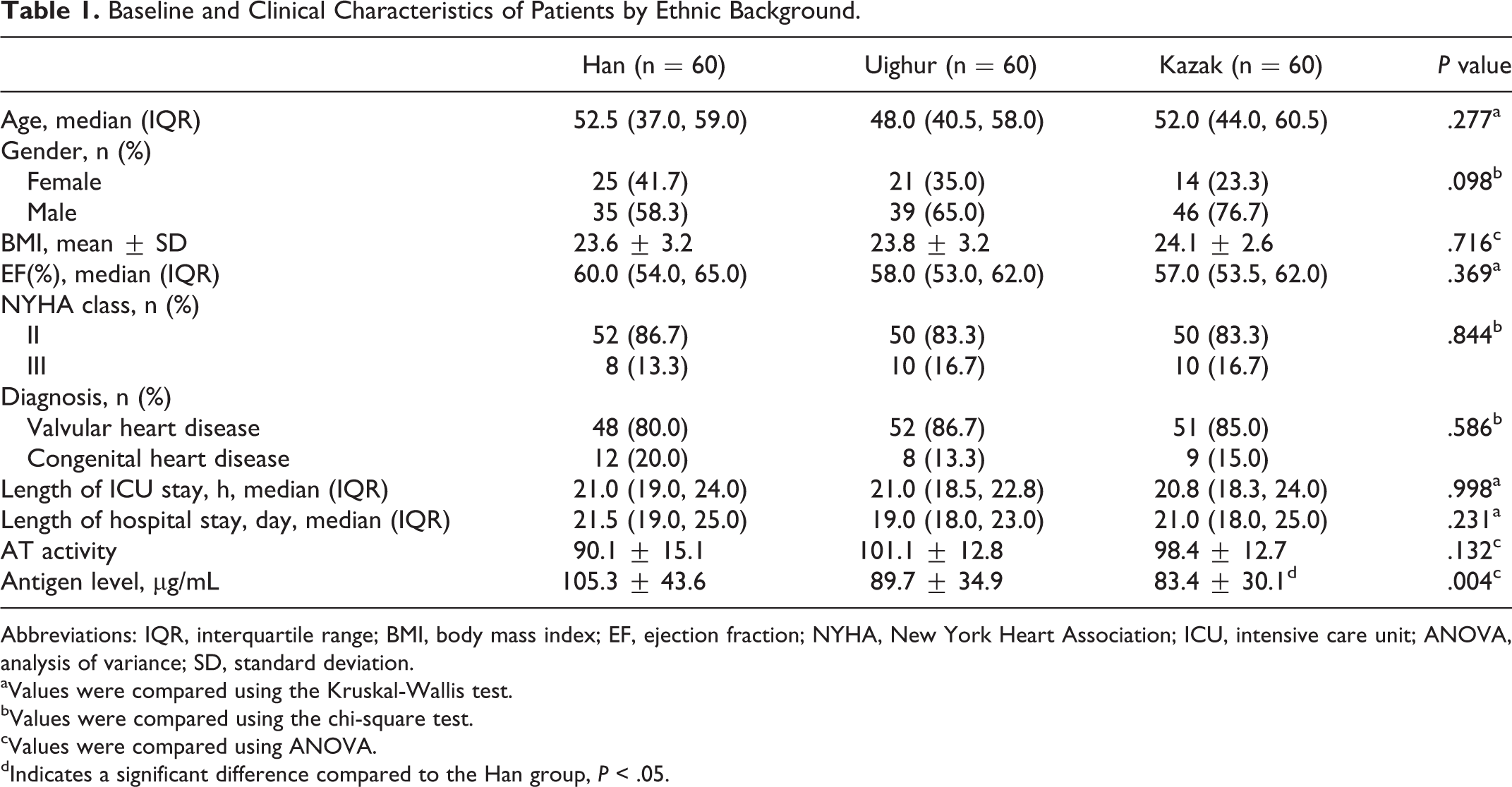
Abbreviations: IQR, interquartile range; BMI, body mass index; EF, ejection fraction; NYHA, New York Heart Association; ICU, intensive care unit; ANOVA, analysis of variance; SD, standard deviation.
aValues were compared using the Kruskal-Wallis test.
bValues were compared using the chi-square test.
cValues were compared using ANOVA.
dIndicates a significant difference compared to the Han group, P < .05.
Proportion of SERPINC1 Mutations by Ethnic Background
After sequencing all 7 exons of the SERPINC1 gene, the following 9 SNP sites were identified in exons 5 and 7: g.981A>G, g.984G>T, g.1000G>T, g.1002A>G, g.1011A>G, g.1030G>A, g.1267G>A, g.1334G>A, and g.1336G>A (Figure 2). Significant differences were noted in the frequency of the g.981A>G (rs5877) and g.1011A>G (rs5878) genotypes among the 3 groups.
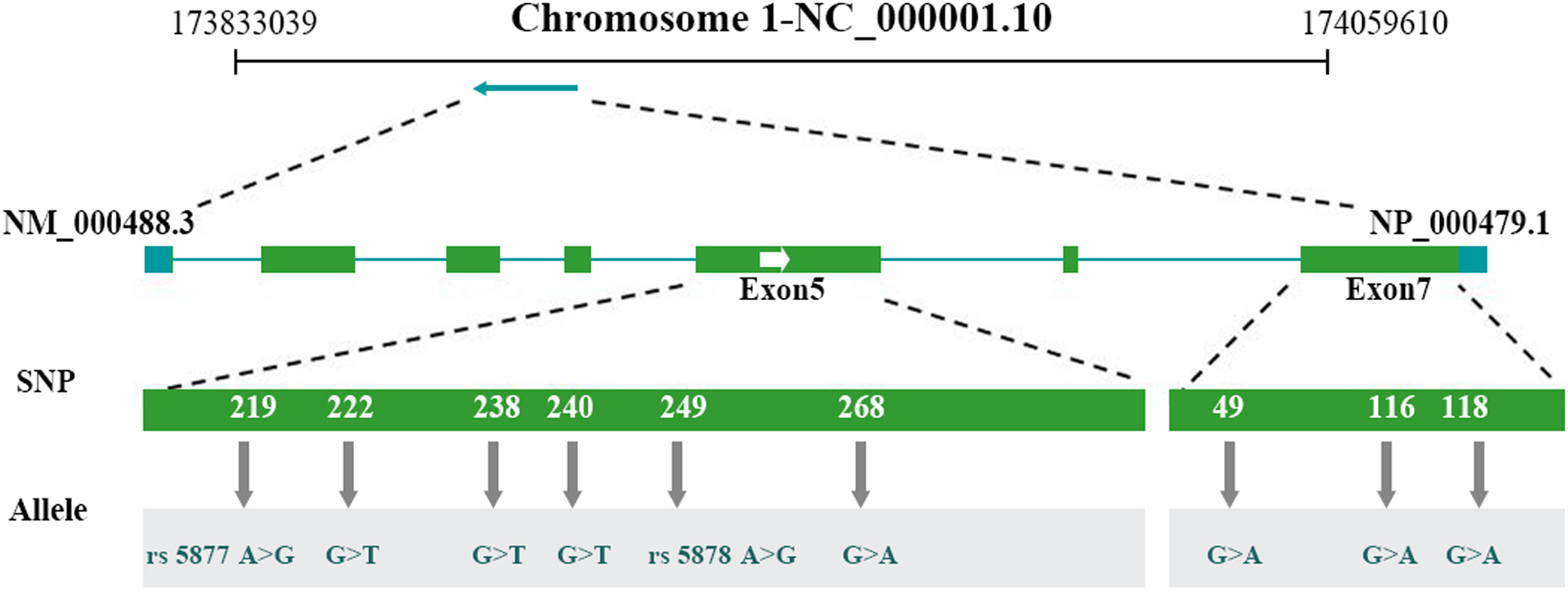
The reverse arrow showed a total of 9 SNP sites within 7 exons of the antithrombin gene, SERPINC1. The figure showed Gene ID 462 (SERPINC1) as well as merged features of NP_000479.1 and NM_000488.3 with 13 579 bps.
DNAMAN6.0 software was next used to analyze the nucleotide sequence of the PCR products. Specifically, the influence of the g.981A>G (rs5877) and g.1011A>G (rs5878) genotypes on gene translation was evaluated. Results showed that valine 295 and glutamine 305 remained unchanged in the presence of the g.981A>G (rs5877) as well as the g.1011A>G (rs5878) genotype, suggesting that the AT protein structure is not influenced by these SNPs (data not shown).
Comparison of the SERPINC1 Gene Polymorphisms Among Han, Uighur, and Kazak Patients
The MAFs of allele (A>G) for rs5877 and rs5878 were higher in the Han patients and were significantly different among the ethnic groups (P = .004 and P = .006, respectively; Table 2).
Comparison of the SERPINC1 Gene Polymorphism Among the 3 Ethnic Groups.a
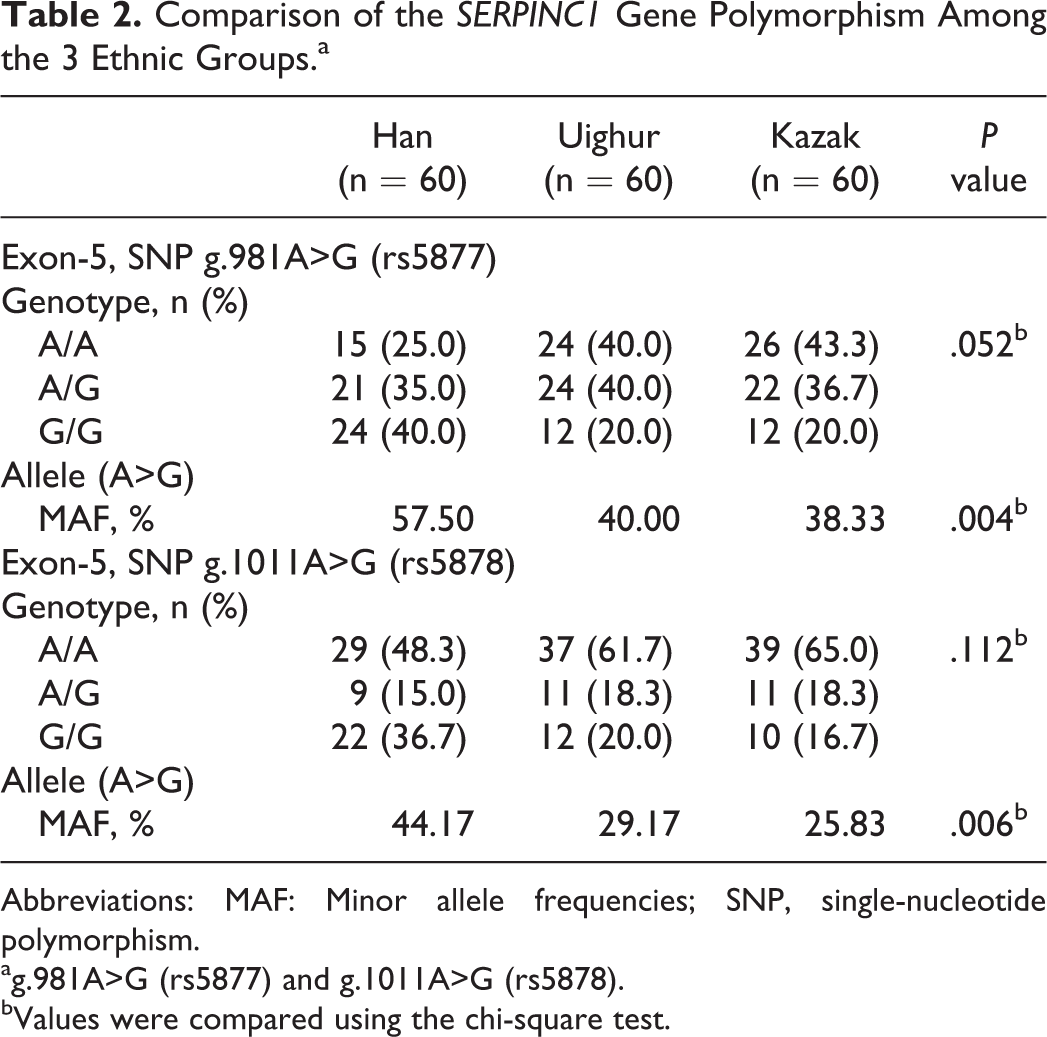
Abbreviations: MAF: Minor allele frequencies; SNP, single-nucleotide polymorphism.
ag.981A>G (rs5877) and g.1011A>G (rs5878).
bValues were compared using the chi-square test.
Differences in Coagulation Parameters Among Han, Uighur, and Kazak Patients
As shown in Table 1, although the Han group had the lowest AT activity of the groups analyzed, it did not reach statistical significance (P = .132). The median preoperative APTT for the Han, Uighur, and Kazak patients was 31.65, 30.00, and 30.20 seconds, respectively (P = .006; Table 3). After Bonferroni correction, the Han patients had significantly longer preoperative APTT as compared to the Uighur patients (P < .05). However, no differences in pre-operative PT were observed (Table 3).
Comparison of APTT and PT Among the 3 Ethnic Groups.
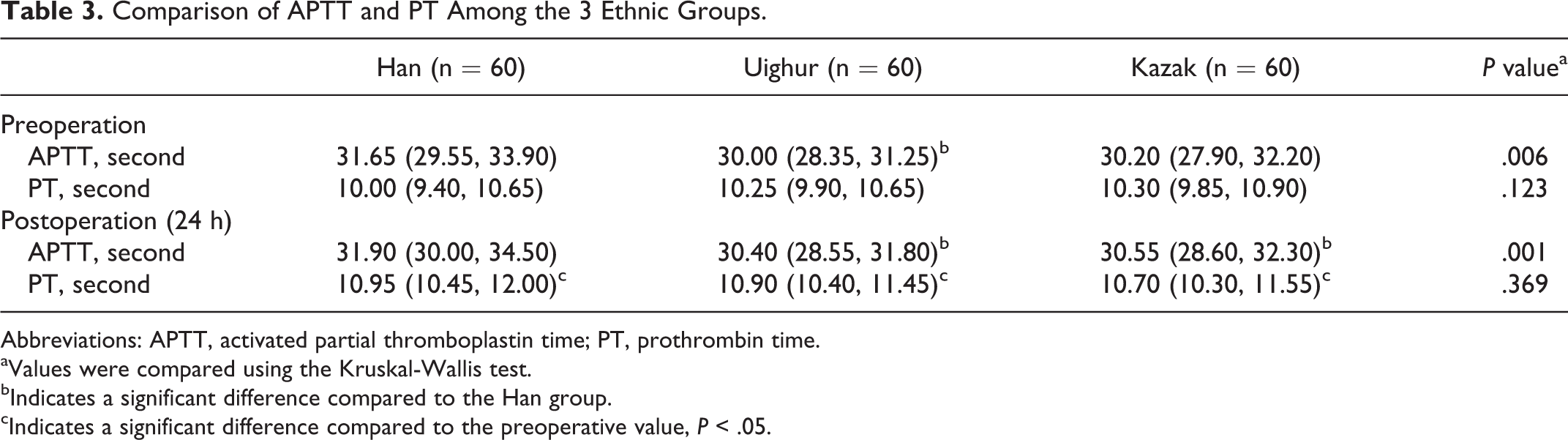
Abbreviations: APTT, activated partial thromboplastin time; PT, prothrombin time.
aValues were compared using the Kruskal-Wallis test.
bIndicates a significant difference compared to the Han group.
cIndicates a significant difference compared to the preoperative value, P < .05.
Postoperative APTT and PT were determined at 24 hours postsurgery. As shown in Table 4, the median postoperative APTT for the Han, Uighur, and Kazak patients was 31.90, 30.40, and 30.55 seconds, respectively (P = .001). After Bonferroni correction, the Han patients had significantly longer postoperative APTT than both the Uighur and the Kazak patients (P < .05). However, no differences in postoperative PT were observed among the groups (Table 3). Although no differences in pre- and postoperative APTT were detected in any of the ethnic groups, the postoperative PT was significantly longer for all the groups compared with their preoperative values (P < .05; Table 3).
Comparison of the Extracorporeal Circulation Parameters by Ethnic Background.
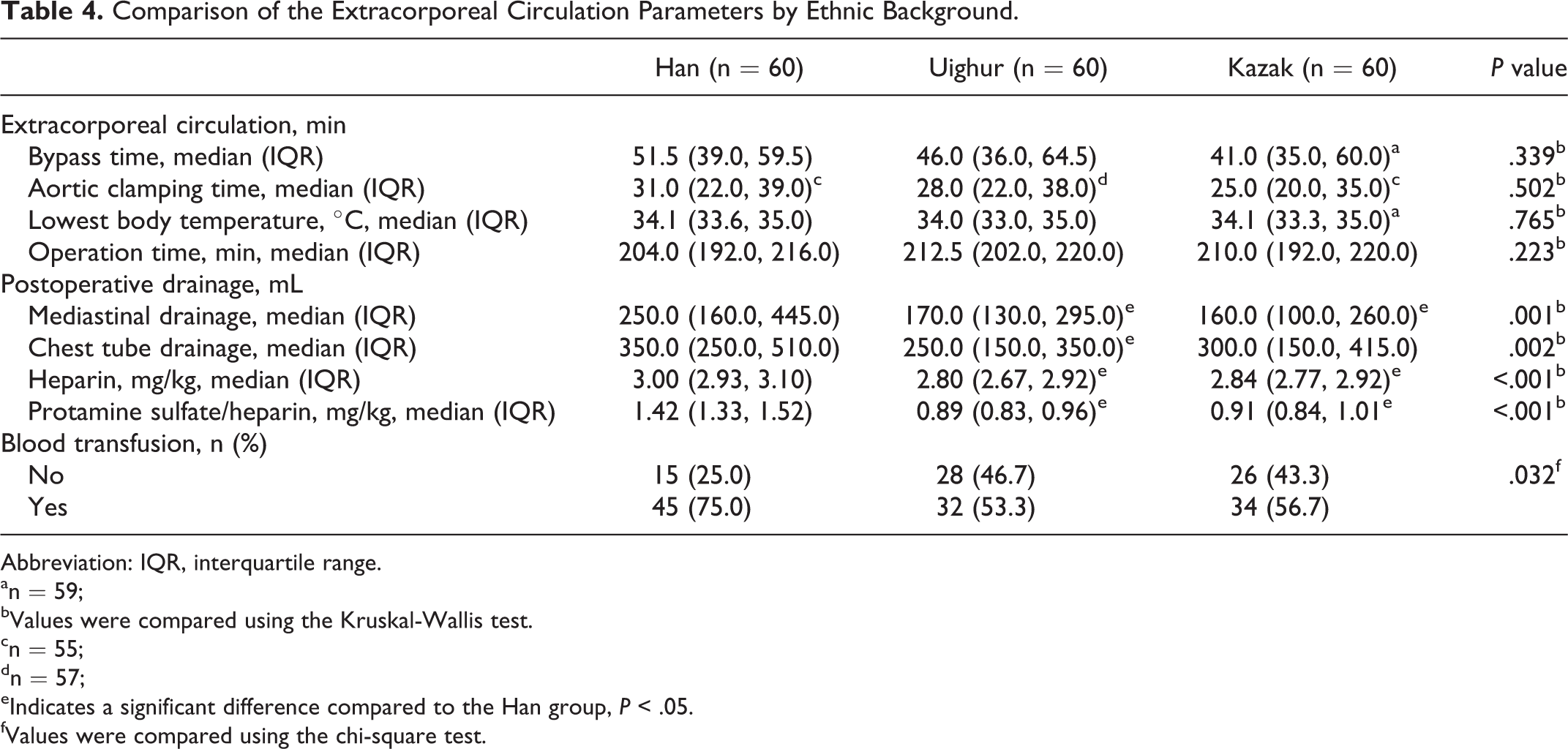
Abbreviation: IQR, interquartile range.
an = 59;
bValues were compared using the Kruskal-Wallis test.
cn = 55;
dn = 57;
eIndicates a significant difference compared to the Han group, P < .05.
fValues were compared using the chi-square test.
Comparison of Extracorporeal Circulation Parameters Among the Han, Uighur, and Kazak Patients
As shown in Table 4, no significant differences were found in bypass time, aortic clamping time, lowest body temperature, and operation time among the 3 ethnic groups analyzed. However, significant differences in postoperative mediastinal drainage (P = .001) and chest tube drainage (P = .002) were observed. In addition, the proportion of blood transfusions differed significantly by ethnic background with a greater proportion of Han patients requiring blood transfusion (P = .032). Moreover, the dosage of heparin and protamine sulfate/heparin in Han patients was significantly higher than that observed in the other patients of Uighur and Kazak ethnicity (both P < .001; Table 4).
Discussion
Maintenance and management of perioperative coagulation is a determinant of the success of a surgery. To prevent coagulation or thrombosis, heparin, which acts on AT, is used for anticoagulation during extracorporeal circulation. However, varying responses to heparin have been reported, which may be due to altered AT levels or activity. 8 Therefore, this study aimed to investigate the correlation between SERPINC1 SNPs and sensitivity to heparin-induced anticoagulation in Han, Uighur, and Kazakh patients undergoing heart surgery with the goal of identifying patients at risk of hemorrhage-related complications and predicting heparin dosage requirements on an individualized basis as has been undertaken for warfarin. 5 Two SNPs (rs5877 and rs5878) were observed in exon 5 of SERPINC1 which were detected in a greater proportion of the Han patients. In addition, differences in coagulation function, heparin and protamine dosage, and blood transfusions were observed in this subset of patients.
In the present study, Han, Uighur, and Kazakh patients receiving heart surgery with extracorporeal circulation were recruited. These patients were randomly selected from residents of Xinjiang, and patients with factors influencing sensitivity to heparin were excluded. Thus, the recruited patients were representative of the population of Xinjiang.
Postoperative hemorrhage often due to dysfunctional coagulation is a common complication of heart surgery. The incidence rate of postoperative bleeding was 6% to 25%. 15 After heart surgery, a variety of coagulation factors (eg, Factors III, VII, and XI) are consumed, and a large amount of proinflammatory cytokines, including C-reactive protein, tumor necrosis factor, and interleukin 6, are released due to surgical trauma and extracorporeal circulation. 16 These factors may influence coagulation function to a certain extent. In addition, low levels of AT activity are associated with a poor outcome (eg, prolonged ICU stay, incidence of surgical reexploration, adverse neurologic events, and incidence of thromboembolic events) after CPB. 17 In the present study, the preoperative coagulation function of all patients was normal. Analysis of pre- and postoperative APTT and PT revealed longer APTT in Han patients than the Uighur and Kazakh patients. Although no differences in PT were detected between the ethnic groups analyzed, PT values within 24 hours after surgery were significantly longer than those before surgery. Moreover, the prolongation of PT was more evident in the Han patients. In addition, a greater proportion of Han patients required blood transfusions and had greater blood loss within 24 hours of surgery when compared to the Uighur and Kazakh patients. Furthermore, the amount of heparin and protamine used in the perioperative period was significantly larger in the Han patients when the influencing factors (ie, operation time and duration of extracorporeal circulation) were similar, suggesting a higher sensitivity of the Uighur and Kazakh patients to heparin than the Han patients. Furthermore, the longer baseline APTT, which is not impacted by AT, in Han patients is suggestive of the presence of a completely distinct pretest variable (acquired or genetic) in this subset.
Antithrombin is a serine protease inhibitor (serpin) that has a role in anticoagulation by targeting proteases within the contact activation pathway, resulting in their inactivation. 18 Heparin may bind to AT, leading to a conformational change that exposes the reactive center loop of AT and increasing AT anticoagulation activity by several thousand-fold. 19 –21 Specifically, heparin binds the AT protein at amino acids 41 to 49 and 107 to 156. 22 In addition, Arg47, Lys114, Lys125, and Arg129 also play important roles in the binding of AT to heparin. 22 We identified 2 SNPs, g.981A>G (rs5877) and g.1011A>G (rs5878), in exon 5 of the SERPINC1 gene with the highest frequency noted in the Han patients. However, further analysis showed the translation of 295 Val and 305 Gln, respectively, was not influenced by these SNPs.
Chuang et al 23 reported that the variations in the P1 position (Arg393) of AT altered its specificity without influencing its activation by heparin. Although the 2 silent mutations identified in the present study do not influence protein structure expression, they may still affect protein function and, therefore, a patient’s sensitivity to heparin.
Hyperpyrexia, infection, increased platelet count, and the presence of concomitant diseases, including atrial myxoma, can all affect a patient’s sensitivity to anticoagulation management. 24 In a fashion similar to that reported for polymorphisms in CYP2C9 and VKORC1 and warfarin sensitivity, 5 abnormalities in AT activity and expression due to SERPINC1 gene mutation also influence sensitivity to heparin. 25 In healthy Spanish caucasian individuals, several SNPs of the SERPINC1 gene have been identified, including 1 in the promoter region and 1 in intron 1. 26 Although the promoter polymorphism did not alter AT function, the one located on exon 1 was associated with plasma anti-factor X activated and AT levels. 26 In the present study, concomitant diseases were excluded. Therefore, we speculate that these homozygous mutations of the SERPINC1 gene may influence the stability of AT and its sensitivity to heparin in Han patients as compared with Uighur and Kazakh patients, resulting in increased heparin and protamine usage, postoperative blood loss as well as intraoperative blood transfusion in Han patients. There is evidence showing that individualized anticoagulation with heparin during the heart surgery in the presence of extracorporeal circulation may improve the clinical outcome, 27,28 which is supported in the present study.
The study is limited in that the impact of the SERPINC1 gene mutations on AT messenger RNA or protein structure as well as specificity was not assessed. Further studies are required to analyze the full impact of these mutations. In addition, the coagulation response was not directly correlated with the presence of SERPINC1 mutations. Therefore, further studies with a large sample size are required to confirm our findings.
Understanding the molecular and genetic mechanisms underlying differences in heparin sensitivity by ethnicity is important for the management of perioperative anticoagulation. Antithrombin is a key factor involved in the heparin-induced anticoagulation cascade. Differences in heparin sensitivity were noted in Han patients analyzed, which was apparent in the increased dosage of heparin and protamine used, the longer APTT, and the greater proportion of patients receiving intraoperative blood transfusion compared with Uighur and Kazakh patients. In addition, Han patients had a higher frequency of SERPINC1 gene SNPs, which may result in altered sensitivity to heparin. Further studies with larger cohorts are necessary to confirm our findings, which may be of clinical importance in developing protocols for individualized perioperative anticoagulation management.
Footnotes
Authors’ Note
Jiang Wang carried out study concepts and design and participated in supervision of experimental studies. Hai-Ping Ma carried out clinical studies, experimental studies, manuscript preparation, and editing. Ai Lai Ti Ta Lai Ti participated in the literature research, clinical studies, and experimental studies. Yong-Qiang Zhang carried out experimental studies, data acquisition, data analysis, and statistical analysis. Hong Zheng participated in the study design, manuscript editing and review, and supervision of whole project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Higher Education Specialized Research Fund for the Doctoral Program jointly funded project [grant number 20126517110005] and the Xinjiang Autonomous Region Key Discipline Project [New Scholar and Researchers (2010), No. 7].