
Abstract
Arterial shear stress was generally implicated in the development of atherosclerotic plaque (AP). Atherosclerotic plaque may be associated with myocardial bridging (MB). We evaluated the metabolic abnormalities which could determine the localization of AP at the proximal coronary segment of MB. We analyzed the patients with MB, AP&MB, and AP on left anterior descending (LAD) artery who were diagnosed by multislice computed tomography coronary angiography. Serum levels of metabolic parameters were compared among study groups. Patients with MB&AP and AP were significantly older than those in the MB group. Patients with MB&AP had AP and MB at the proximal and middle segments of LAD artery, respectively. Total cholesterol, low-density lipoprotein (LDL) cholesterol and very LDL, and triglyceride levels were significantly higher in patients with MB&AP and AP compared to only MB. Low-density lipoprotein cholesterol was significantly correlated with the type of coronary artery disease in multiple regression analysis. Myocardial bridging may be an anatomical determinant for the localization of AP proximal to itself in the presence of hypercholesterolemia.
Introduction
Tropism and development of atherosclerotic plaques (APs) on the middle and large arteries, for example, coronary and carotid arteries have been investigated for several decades. Wall shear stress (WSS) is a significant determinant for the initiation and progression of an AP on the arterial wall. Numerous factors including abnormal flow dynamics (eg, pulsatile, helical, or turbulence flow), osteal, and bifurcated and branching segments of arteries may induce WSS, whereas laminar flow property is less associated with AP. 1 Diameter of arterial vessel, wall thickness, heart rate, and blood pressure are additional factors that could contribute the localization and progression of AP. 2
Myocardial bridging (MB) is a congenital abnormality in which one or more segments of an epicardial coronary artery course under it. 3 It is an anatomic obstacle which constricts the coronary artery from the outside. Although it could be diagnosed by means of systolic compression artery during invasive coronary imaging, it physiologically causes myocardial perfusion abnormality by producing a diastolic flow gradient between the proximal and distal segments of MB. 4 So, a raised intracoronary flow pressure and also a turbulent flow inevitably occur at the coronary segment proximal to it. Close relationship between the hypercholesterolemia and atherosclerotic coronary artery disease (CAD) is precisely documented by numerous studies. It was documented that the content of AP was rich in cholesterol crystals and inflammatory cells. 5 Various mechanisms related to morphological features of coronary arteries and hypercholesterolemia had been proposed for the tropism, initiation, and progression of AP in association with hypercholesterolemia. 6
In this study, we retrospectively evaluated whether the MB was anatomically associated with the localization of AP on the coronary artery of patients with CAD diagnosed by multislice computed tomography (MSCT) coronary angiography. We also evaluated the coexisting laboratory abnormalities which could be related to the development of AP.
Material and Method
Study Design
The study was designed retrospectively. Approval of local ethics committee was obtained. The entire laboratory data were gathered from the digital recordings of medical archives of the patients diagnosed with CAD by MSCT coronary angiography. The study populations are the subgroups of a cohort of 34 patients who were diagnosed as having CAD by MSCT coronary angiography. The criteria for the subgroups were presence of MB and/or AP.
Coronary Artery Imaging
We retrospectively reviewed the medical recordings of patients with CAD. They were grouped according to the findings on the MSCT coronary angiography. Images were reconstructed with 0.5-mm slices and analyzed with postprocess study. The study groups were defined as patients with MB (n = 18), MB&AP (n = 7), and AP (n = 9) on left anterior descending (LAD) coronary artery. The patients underwent MSCT angiography due to equivocal or positive results on treadmill test.
Laboratory Data
Blood samples were obtained from all patients by a venous route at a 12-hour fasting state at 08 00
Complete blood count was studied from the blood sample obtained at a 12-hour fasting state in the morning and performed using Mindray Auto Hematology Analyzer-BC-6800 (A. Menarini Diagnostics, China) device.
Exclusion Criteria
Patients with previous diagnosis of atherosclerotic CAD, ischemic heart disease, congestive heart failure, diabetes, and chronic renal failure were excluded from the study.
Statistical Analysis
Normality of study groups and data were tested by Shapiro-Wilk test. Data with normal distribution was compared with parametric tests (one-way analysis of variance test), while those without normal distribution were compared with nonparametric tests (Kruskal-Wallis test). Post hoc analysis was performed by Tamhane test for data with inhomogeneous variances and Tukey’s test for homogeneous variances. Data which were analyzed by parametric tests due to normal distribution were reported as mean ± standard deviation, whereas those analyzed by nonparametric tests were reported as median (minimum and maximum ranges).
Correlation analysis of numerical and categorized variables was performed by Pearson and Spearman correlation tests, respectively. Parameters that were found to be significantly correlated were tested by multiple regression analysis. P value <.05 was considered as statistically significant. Statistical analyses were performed by IBM SPSS 22.0 for Windows (Chicago, Illinois).
Results
Features of AP and MB and their localization were described in the Table 1. Mean age of patients with MB&AP and AP was significantly higher than patients with MB (Table 2). Serum levels of FBG, AST, and ALT were not different among groups. However, serum levels of total cholesterol (181.6 ± 23.7, 233.8 ± 21.4, and 254.7 ± 23.7; P < .001), LDL-C (98.5 ± 13.7, 159.4 ± 14.8, and 169.7±10.6; P < .001), and VLDL-C (20.8 ± 7.8, 26.4 ± 10.5, and 36.4 ± 22.2; P = .028), and TG (104.2 ± 24.7, 173.4 ± 65.2, and 195.5 ± 56.3; P < .001) levels were significantly higher in patients with MB&AP and AP compared to those with only MB. Total cholesterol, LDL-C, VLDL-C, and TG were found to be significantly correlated with type of coronary lesion of patients in the correlation analysis; however, only LDL-C was found to be significantly correlated with type of CAD in regression analysis (Table 3).
Localization of Atherosclerotic Plaques and Myocardial Bridging on LAD Coronary Artery in Patients With MB, MB&AP, and AP.
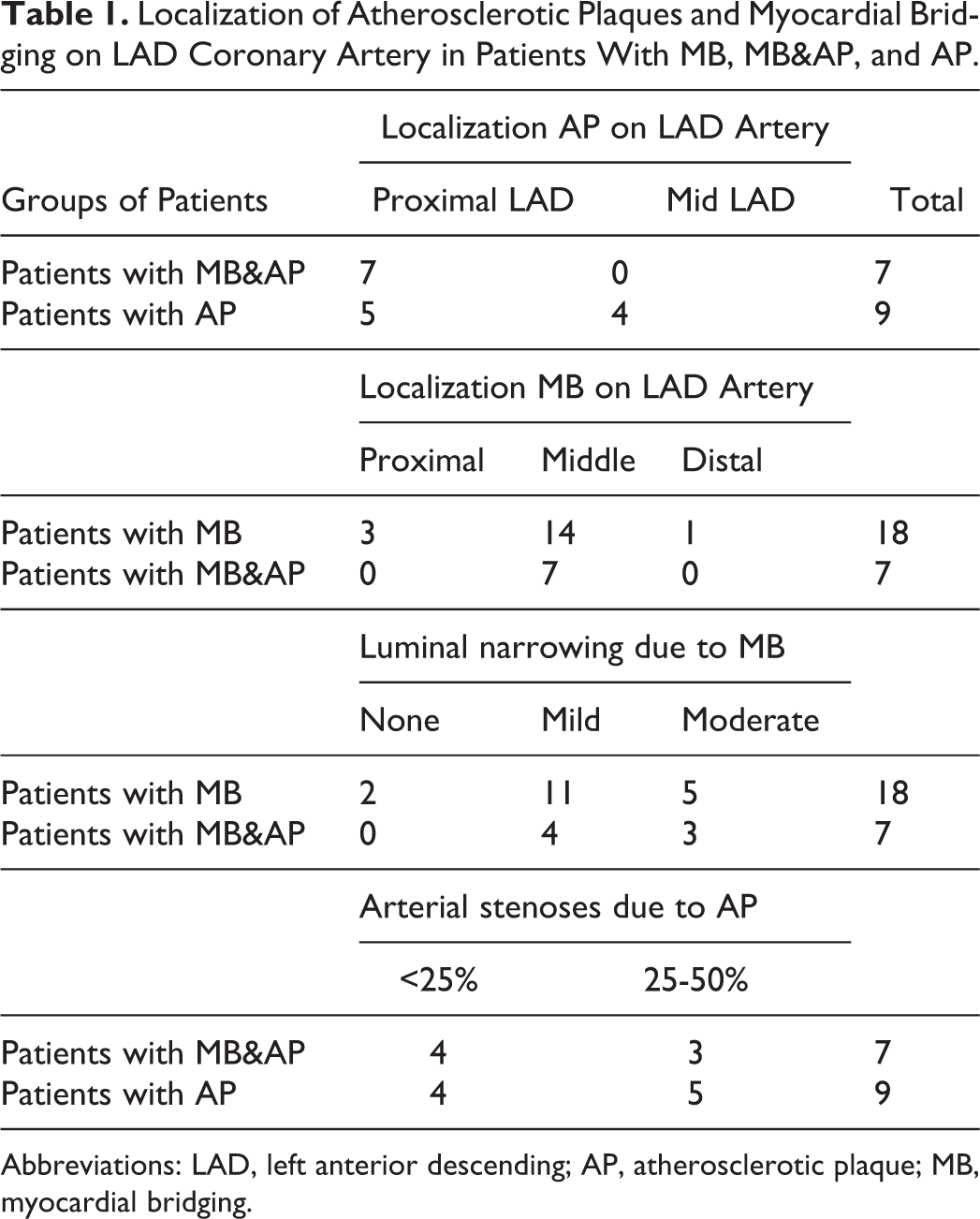
Abbreviations: LAD, left anterior descending; AP, atherosclerotic plaque; MB, myocardial bridging.
Comparison of Laboratory and Complete Blood Count Parameters Among Patients With Myocardial Bridging, Myocardial Bridging and Atherosclerotic Plaque, and Atherosclerotic Plaque.
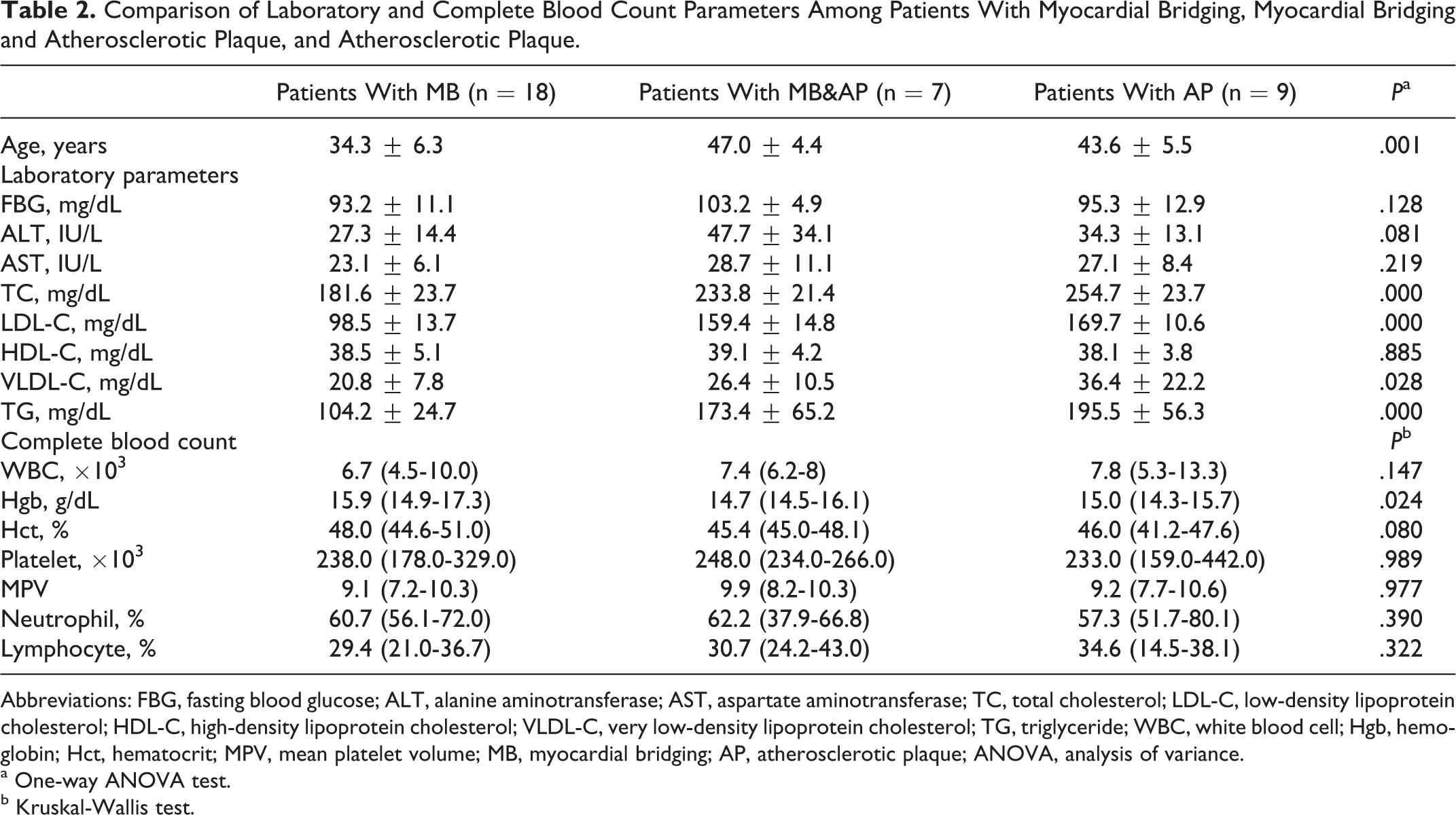
Abbreviations: FBG, fasting blood glucose; ALT, alanine aminotransferase; AST, aspartate aminotransferase; TC, total cholesterol; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; VLDL-C, very low-density lipoprotein cholesterol; TG, triglyceride; WBC, white blood cell; Hgb, hemoglobin; Hct, hematocrit; MPV, mean platelet volume; MB, myocardial bridging; AP, atherosclerotic plaque; ANOVA, analysis of variance.
a One-way ANOVA test.
b Kruskal-Wallis test.
Analysis of Correlation Between the Coronary Arterial Lesion Type of Patients and Serum Levels of TC, LDL-C, VDL-C, and TG.
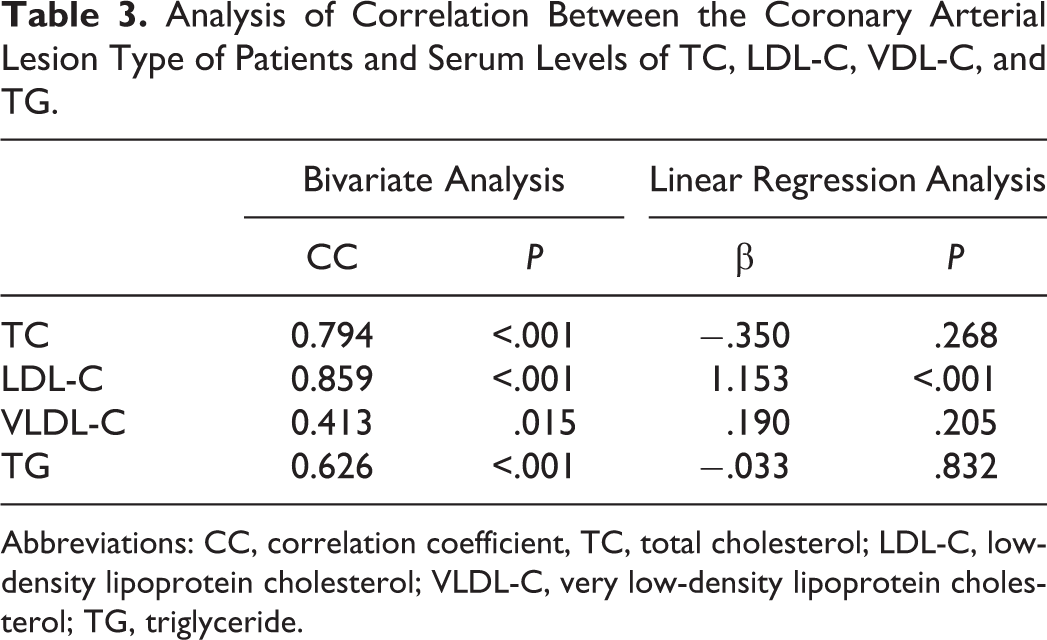
Abbreviations: CC, correlation coefficient, TC, total cholesterol; LDL-C, low-density lipoprotein cholesterol; VLDL-C, very low-density lipoprotein cholesterol; TG, triglyceride.
Discussion
How and why an AP had initiated and intended to certain regions or segments of a coronary artery have been investigated by numerous studies for a long period. Various hemodynamic changes and insults due to blood flow and anatomic variations of arteries had been accused for this condition. 1,2 Although the biological and genetical properties are certainly the determinative factors for the atherosclerotic process, identification of etiologies that are mechanistically related to AP will enable the cardiologist to control and prevent the atherosclerotic process and clinical events.
Myocardial bridging is a congenital coronary abnormality which has gained importance due to its close association between various types of cardiovascular events. It is now accused for the development of atherosclerotic process at the arterial segment proximal to MB. Nakaura et al analyzed clinical variables and comorbidities of 188 patients who underwent MSCT and reported that 50 patients with MB located at the middle segment of LAD had atherosclerosis at the proximal segment. 7 This association was independent of other clinical factors such as age, diabetes, and so on. Independence of a relationship between MB and atherosclerosis from age may be a rationale for the close relationship of cholesterol and atherosclerosis at the proximal segment to MB instead of age in our study groups. Although Nakaura et al reported that the arterial segment underlying MB was protected from atherosclerosis, the fact is hidden in the mechanism of coronary flow abnormality induced by MB. Klues et al defined the complexity of the interactions which were accused for the development of atherosclerosis in the proximity of MB. 8 The study was about the recovery of coronary hemodynamic abnormalities following the intracoronary stent placement to the bridged coronary segment. An abrupt diastolic flow acceleration followed by mid-diastolic plateau and retrograde systolic flow was the typical intracoronary Doppler flow velocity profile induced by MB. After the stent implantation, pressure gradients between the proximal and distal coronary lumen interrupted by MB were completely normalized and relatively a laminar flow was achieved. Actually, the myocardium is perfused during the diastolic phase of coronary flow, and coronary lumen under the MB get smaller due to systolic compression. Also, a retrograde systolic flow within the MB segment may be one of the protective mechanisms which spare the bridged coronary segment from atherosclerosis. As it was mistakenly reported that MB was associated with the protection of atherosclerosis, 9 they proposed that low tensile stress and reduced coronary wall motion due to external myocardial support could have been accounted for the protection. Similarly, Loukas et al proposed the protective effect of MB against atherosclerosis. They reported that smooth muscle cells and macrophages decreased under the subendothelial layer which was compressed by MB during systolic period. 10 Atherosclerotic plaque initiates at the subendothelial intimal layer and progresses into the coronary lumen and the media layer which consists of smooth muscle cells. 11 Since it was documented that MB significantly reduced the intimal thickness of arterial wall of LAD artery compared to proximal and distal segments by IVUS study, 12 we propose that lipoproteins, lipid particles, and phagocytic cells could not have been inoculated to initiate a streak or a plaque of atherosclerosis. Recently, Yoshino et al documented that the microvascular endothelia dysfunction was significantly associated with increased vasoreactivity and decreased FFR following acetylcholine infusion into the coronary lumen in symptomatic patients with MB. 13 Their study groups had small number of patients similar to that in our study groups. Endothelial dysfunction may not only be accounted for the patients’ symptoms but also related to the initiation and progression of atherosclerosis. Thus, the most harmful and devastating effect of MB was on the proximal segment of the coronary artery, as it is highlighted and explained by several recent studies. Tian et al surveyed thousands of patients who underwent MSCT angiography. 14 They reported that most patients with LAD stenosis (n = 3359) had MB on LAD artery (n = 1658), and that MB in the LAD artery was independently associated with atherosclerosis in the proximal segment to MB. Similarly, Hong et al reported that angiographic and clinical factors, for example, systolic narrowing rate, male gender, diabetes, and severity of coexisting coronary artery stenoses were associated with the development of AP proximal to MB. 15 We observed that AP was localized at the proximal segment of LAD, while MB was located at the middle segment in 7 patients (Table 1). Mild and moderate luminal narrowing of the middle segment of LAD was observed in 4 and 3 patients with MB&AP. Mild and moderate luminal narrowing was observed in 11 and 5 patients with only MB, while 2 did not have any luminal narrowing. Localization of MB in patients with MB was proximal, middle, and distal in 3, 14, and 1 patient, respectively.
We evaluated the laboratory data and complete blood count in patients diagnosed with only MB, AP proximal to MB, and only AP on the LAD coronary artery by MSCT angiography. Laboratory data may provide information about hyperlipidemia and its subtypes, and the chronic inflammatory diseases of the liver which are documented to be closely associated with atherosclerosis. 16 We found that the comparison of serum levels of TC, LDL-C, and VLDL-C, TG was significantly different among patients with MB, MB&AP, and AP (Table 2). In subgroup analysis, we observed that patients with MB and MB&AP had significantly higher serum levels of TC, LDL-C, VLDL-C, and TG compared to those in patients with only MB (Figures 1 -3), whereas the difference among patients with MB&AP and AP was not statistically significant. While TC, LDL-C, VLDL-C, and TG were found to be positively correlated with the type of coronary disease in correlation analysis, only LDL-C was significantly correlated with the type of CAD in regression analysis (Table 3). Cholesterol is not only a major coronary risk factor but also an important component of AP content. Loukas et al documented that smooth muscle cells had increased migratory activity and proliferation and intimal thickening was also prominent in the arterial segments proximal and distal to MB. 10 It may be interpreted that intimal layers of proximal and distal arterial segments of MB are physiologically and histologically available for the initiation and progression of atherosclerosis provided that any promoting factors coexist. We suggest that cholesterol particles are the unique promoting factors in the arterial segments proximal to MB. We observed that patients with MB had significantly lower serum levels of TC, LDL-C, VLDL-C, and TG compared to patients with MB&AP and AP (Table 2). These patients did not have AP at any arterial segments either proximal or distal to MB despite the intimal layers of those segments having an increased inflammatory and cellular activity, as documented by Loukas et al. Higher levels of TC, LDL-C, VLDL-C, and TG were probably the determining factor for the coexistence of AP proximal to MB in patients with MB&AP. Higher levels of TC, LDL-C, VLDL-C, and TG in patients with only AP may be an evidence of potentiating the effect of cholesterol on the development of atherosclerosis in the milieu which is genetically or morphologically determined. However, we found that only LDL-C was significantly correlated with the type of CAD in regression analysis even though all TC, LDL-C, VLDL-C, and TG were positively correlated in the correlation analysis. The limited number of our study groups might have been accounted for that result. Also, we suggest that our results clearly represent the mechanistic association of LDL-C with AP at the segment proximal to the bridged segment and the causative factor of MB. Since we excluded the patients with comorbidities, previous diagnosis of CAD, and statin therapy, our results are far from the effects of any comorbidity. Although comparison of serum levels of ALT among groups was not statistically significant, ALT tended to be higher in patients with MB&AP compared to only MB group (P = 0.066). Contribution of an inflammatory state, for example, low-grade hepatic steatosis, may be proposed for the association of MB and AP.
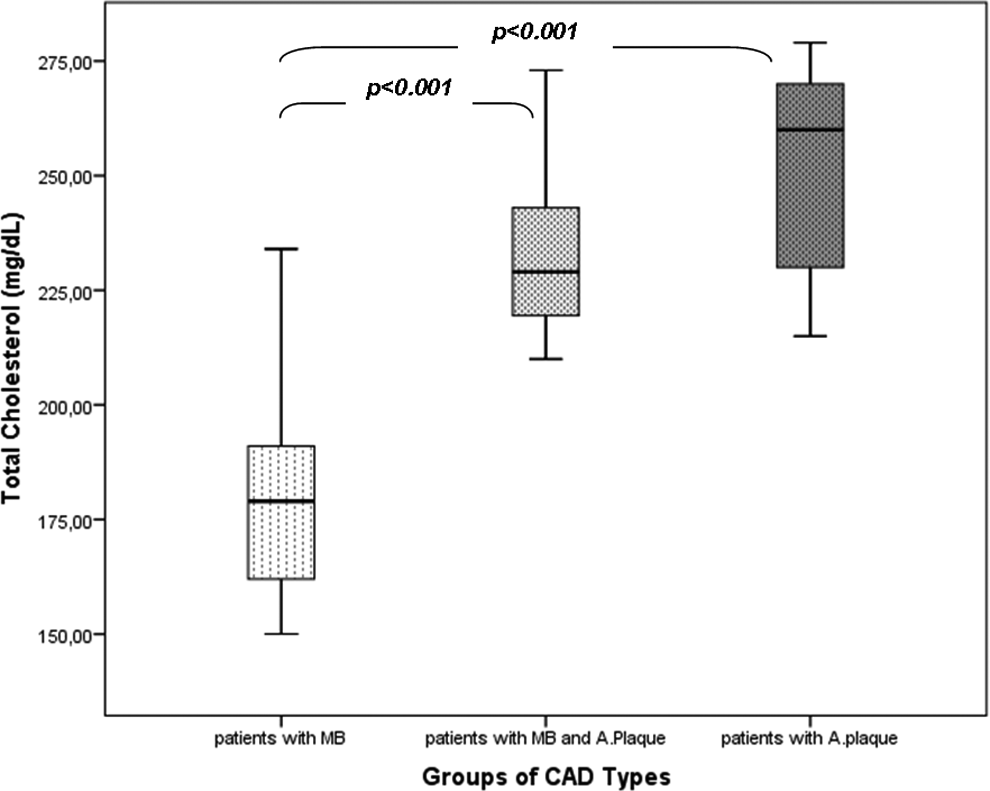
Comparison of serum levels of total cholesterol among patients with myocardial bridging, myocardial bridging and atherosclerotic plaque, and only atherosclerotic plaque.

Comparison of serum levels of low-density lipoprotein (LDL)-cholesterol among patients with myocardial bridging, myocardial bridging and atherosclerotic plaque, and only atherosclerotic plaque.
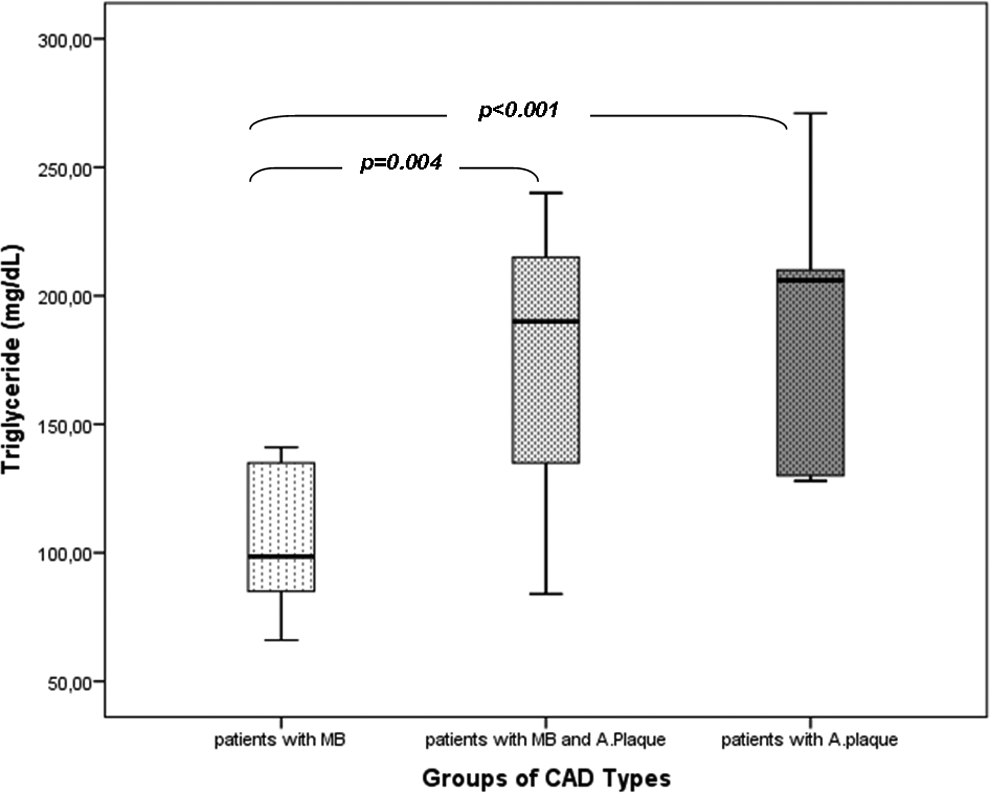
Comparison of serum levels of triglyceride among patients with myocardial bridging, myocardial bridging and atherosclerotic plaque, and only atherosclerotic plaque.
The initial stage of AP is the intimal layer thickening characterized by increased smooth muscle cell, and subsequently, foam cell formation. It was documented that proximal and distal segments of MB were histologically found at that stage. Since the atherosclerosis is a lipoprotein associated disease of vessels, accumulation of extracellular cholesterol and lipid particles into the thickened intimal layer promotes the progression of AP to further stages, for example, intimal inflammation, necrosis, fibrosis, and calcification. 17
Higher diastolic pressure gradients at arterial segments proximal to MB may be the most powerful driving force for the entrance of cholesterol to subendothelial layers if the patients had higher levels of cholesterol as seen in our study. Enforcement of cholesterol, lipoprotein particles, and phagocytic cells may be defined as “seeding effect” of high diastolic gradient just at the proximal segment of the bridged segment. Additionally, it was documented that an increased vascular shear stress was induced at the proximal segment of MB. den Dekker et al experimentally created an AP with higher lipid and phagocytic cell content at the arterial segment under artificial vascular shear stress. 18 Moreover, targeting low cholesterol levels may be reasonable in order to reduce the probability of development of an AP proximal to MB.
An AP could take several decades to progress to clinically symptomatic cardiovascular events unless any thromboembolic coronary occlusion due to plaque rupture or an inflammatory state interferes with the progression. 17 In this study, we observed the patients with only MB were significantly younger compared to others (Table 2 and Figure 4). Our results may represent that the time period for the development of AP due to MB in association with hypercholesterolemia at the fourth and fifth decades of a patient’s life. Also, those patients with AP may represent the patients with asymptomatic but inherited premature atherosclerosis during the fifth decades. Additionally, we observed that MB&AP group tended to have more frequent AP with mild stenosis, whereas AP group tended to have moderately stenotic lesions.
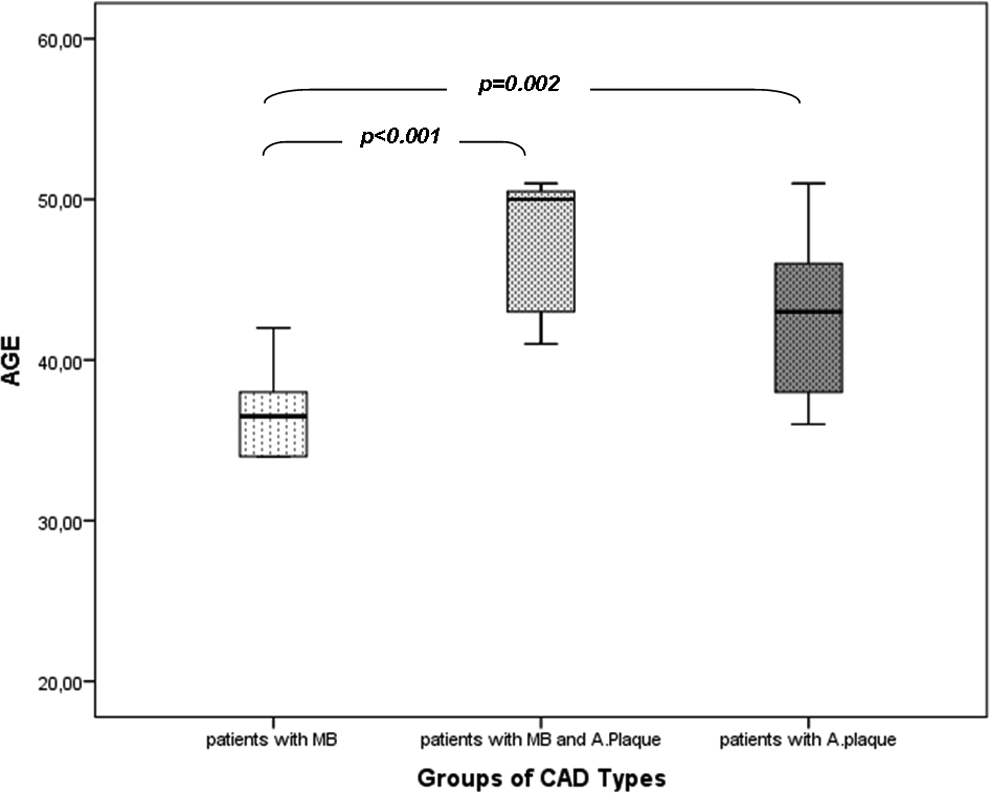
Comparison of age of patients with myocardial bridging, myocardial bridging and atherosclerotic plaque, and only atherosclerotic plaque.
All previously and recently reported data may raise a question about the criteria for the initiation of statin therapy in patients with MB. Statin therapy is strictly recommended in either primary or secondary prevention of atherosclerotic cardiovascular diseases. 19 Coexistence of hypercholesterolemia in a patient with MB at any coronary artery may be a strong predictor of development of AP in those patients in the further life period. Thus, it will be better to determine whether the presence of MB on the coronary artery in a patient is a coronary risk factor or a CAD equivalent similar to diabetes. Since targets of LDL-C may differ according to the definition, whatever is accepted it seems rationale to start a statin drug in a patient with MB and hypercholesterolemia even if he or she does not have AP.
Conclusion
We suggest that MB is a potential promoting factor for the development of AP at the proximal arterial segment in the presence of a coexisting hypercholesterolemia. Absence of any AP in patients with only MB but not hyperlipidemia may be a rationale for targeting the lower serum levels of cholesterol either by statin therapy or dietary and lifestyle changes in order to prevent further development of atherosclerosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.