
Abstract
Aim:
To determine the most important predictors of inhospital mortality that could be assessed in geriatric patients presenting with ischemic stroke at admission to the emergency department(ED).
Methods:
A retrospective cohort study was carried out in geriatric patients with ischemic stroke who were diagnosed in the ED. The primary outcome measure was determined as all-cause inhospital mortality after 30 days of ischemic cerebrovascular event.
Results:
During the study period, 247 (35.7%) patients died in the hospital and 445 (64.3%) patients survived the 30-day period. The median age of the patients was 78 (72-83). Higher National Institutes of Health Stroke Scale (NIHSS) scores (odds ratio [OR]: 2.085; 95% confidence interval [CI]: 1.835-2.370), increased creatinine levels (OR: 2.002; 95% CI: 1.235-3.243), increased platelet levels (OR:1.006; 95% CI: 1.002-1.010), and hyperglycemia (OR: 2.610; 95% CI: 1.023-6.660) were found as independent predictors of inhospital mortality.
Conclusion:
In evaluating geriatric patients with ischemic stroke, laboratory values including platelet count, creatinine levels, hyperglycemia, and NIHSS scores should be considered to predict inhospital mortality in the ED.
Introduction
Stroke ranks as the fourth leading cause of death, behind heart, cancer, and chronic lower respiratory diseases. It has also generally been regarded as one of the important causes of adult disability. 1 Well-known risk factors include hypertension (HT), diabetes mellitus (DM), heart diseases and rhythm disturbances, elevated blood cholesterol, smoking, physical inactivity, dietary aspects, chronic kidney disease, and hereditary factors. 1 –3
Ischemic stroke is a disease that predominantly occurs in middle-aged and older adults; therefore, aging of population brings important challenges to health care professionals. Aging is an important risk factor, which also determines functional outcome and mortality. 4 Some risk factors do not vary with advancing age, whereas the importance of other risk factors changes from middle adulthood to late life. 5 Stroke outcome is prominently worse in older people, and increased risk of death is commonly attributed to higher occurrence of the severe stroke syndromes in the acute phase. 6
Although some studies included the prognosis of ischemic stroke in older patients, factors causing mortality in geriatric patients were not previously evaluated in an emergency department (ED) population. The aim of this study was to identify predictors of inhospital mortality in a cohort of older patients with ischemic stroke who consecutively presented to an ED.
Methods
Study Design
A retrospective cohort study was conducted in patients who presented to the ED of a high-volume training and research hospital between January 1, 2012, and January 30, 2013, who were diagnosed in the ED as having ischemic stroke and who were later admitted to the neurology ward or intensive care unit. All data were obtained by screening the medical records from the hospital database system using International Classification of Diseases, Tenth Revision diagnosis codes. The research was conducted in accordance with the tenets of the Declaration of Helsinki, and institutional review board approval was obtained for the study.
Outcome Measure
The primary outcome measure was determined as all-cause inhospital mortality after 30 days of ischemic cerebrovascular event.
Study Protocol
Neurological examination of the patients was evaluated using the National Institutes of Health Stroke Scale (NIHSS) score. Differentiation of hemorrhagic and ischemic stroke was investigated via noncontrast computed tomography of brain and/or diffusion magnetic resonance imaging.
Etiology of ischemic stroke was classified according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification system. 7 Patients with ischemic stroke were divided into atherosclerotic/lacunar and embolic stroke. Lacunar and atherosclerotic infarcts were evaluated inside to the same group. Patients having ischemic stroke with unknown cause or due to other causes were excluded from the study. differentiation Differentiation of atherosclerotic/embolic stroke was performed based on the presence of atrial fibrillation (AF), thrombus in echocardiography, and Doppler ultrasonography (US), vegetation in the heart valves, valvular heart disease, and anticoagulant drug (warfarin) use. Presence of HT, DM, and coronary artery disease (CAD) was identified via medical records. Mortality data were also obtained from medical records in the hospital database system.
Study forms were filled in with data on age, gender, vital signs (systolic and diastolic blood pressures), comorbid diseases (HT, DM, CAD, and history of cigarette smoking), drugs used, history of previous stroke, NIHSS scores at admission to the ED, laboratory parameters (blood glucose, white blood cell count, hemoglobin level, platelet counts, total cholesterol, and creatinine levels), and hospital length of stay of the patients. The patients were accepted as having history of HT, if they were already diagnosed with HT or if they were using antihypertensive medications. Hematological and biochemical parameters were analyzed with Sysmex XE-2100 (Kobe, Japan) and Abbott C-16000 auto analyzer (Abbott Laboratories, Abbott Park, Illinois) equipments, respectively.
Selection of Participants
All patients aged 65 and older who presented to the ED after an acute ischemic cerebrovascular event, which was demonstrated by a radiologic imaging technique, were included in the study. The exclusion criteria were patients with active infection, history of malignant neoplasm, patients who received blood transfusion in the last 6 months, patients who presented to the ED 24 hours after the first symptoms had started, patients with no accessible laboratory values, patients with incomplete cardiac evaluation (medical history, physical examination, electrocardiography, and transthoracic echocardiography), and patients with no Doppler US.
Statistical Analysis
All statistical analyses were performed using SPSS 11.0 statistical package program (SPSS Inc., Chicago, Illinois). Normal distribution of the data was tested with Kolmogorov Smirnov test. Mann-Whitney U test was used in the analysis of the groups of continuous variables with nonnormal distribution, and the data were expressed in median (interquartile range). Categorical data were compared using Pearson chi-square test and were expressed in numbers and percentages. Odds ratios (ORs) were presented with 95% confidence intervals (95% CI). An α value of .05 was accepted as the nominal level of significance.
A binary logistic regression model was constructed to assess the factors predicting inhospital mortality among geriatric patients with ischemic stroke. The univariate model considered demographic data that included historical characteristics, vital signs, previous medications, hematological, and biochemical variables. Each variable was tested in the univariate model, and those that were significant at an α level of 0.2 were then tested in the multivariate model.
Results
A total of 692 patients including 506 cases with (73.1%) atherosclerotic/lacunar and 186 (27.9%) cases with cardioembolic ischemic stroke were included in the study. During the study period, 247 (35.7%) patients died in the ED, ward, or intensive care unit. Additionally, 445 (64.3%) patients survived the 30-day period. The median age of the patients was 78 (72-83) and most of the patients were female (n = 364, 52.6%). Other baseline characteristics of the study population are shown in Table 1.
Baseline Characteristics of the Study Population.
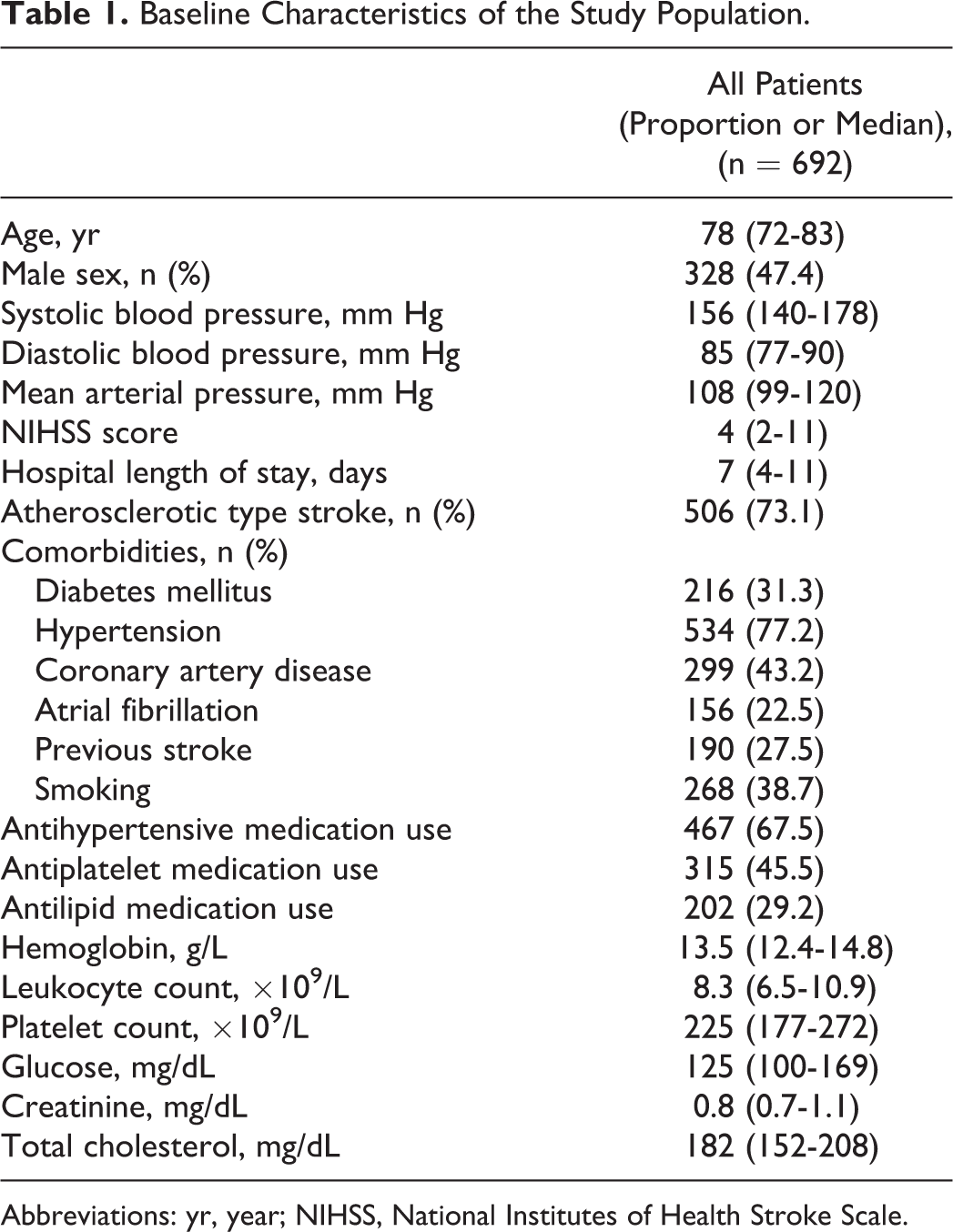
Abbreviations: yr, year; NIHSS, National Institutes of Health Stroke Scale.
Most of the patients had mild to moderate neurologic deficits. The median NIHSS score of the study population was 4 (2-11). Results of the univariate regression model to predict inhospital mortality in geriatric patients with ischemic stroke are shown in Table 2. Compared with surviving patients, patients who died in the hospital were found to be older, hypotensive, and had decreased ejection fraction during the initial evaluation. They had also longer hospital stays and HT in the medical history. Laboratory values between the 2 groups were not similar; there were significant differences regarding leukocyte and platelet counts. Additionally, patients who died were more hyperglycemic and had elevated creatinine levels in the ED. Drugs used secondary to preexisting medical history (antihypertensive, antiplatelet, and antilipid) had no significant effect on mortality. Except HT, other comorbid diseases, including DM, CAD, and AF, had no significant effect on mortality.
Univariate Logistic Regression Model to Predict Inhospital Mortality in Geriatric Patients With Ischemic Stroke.
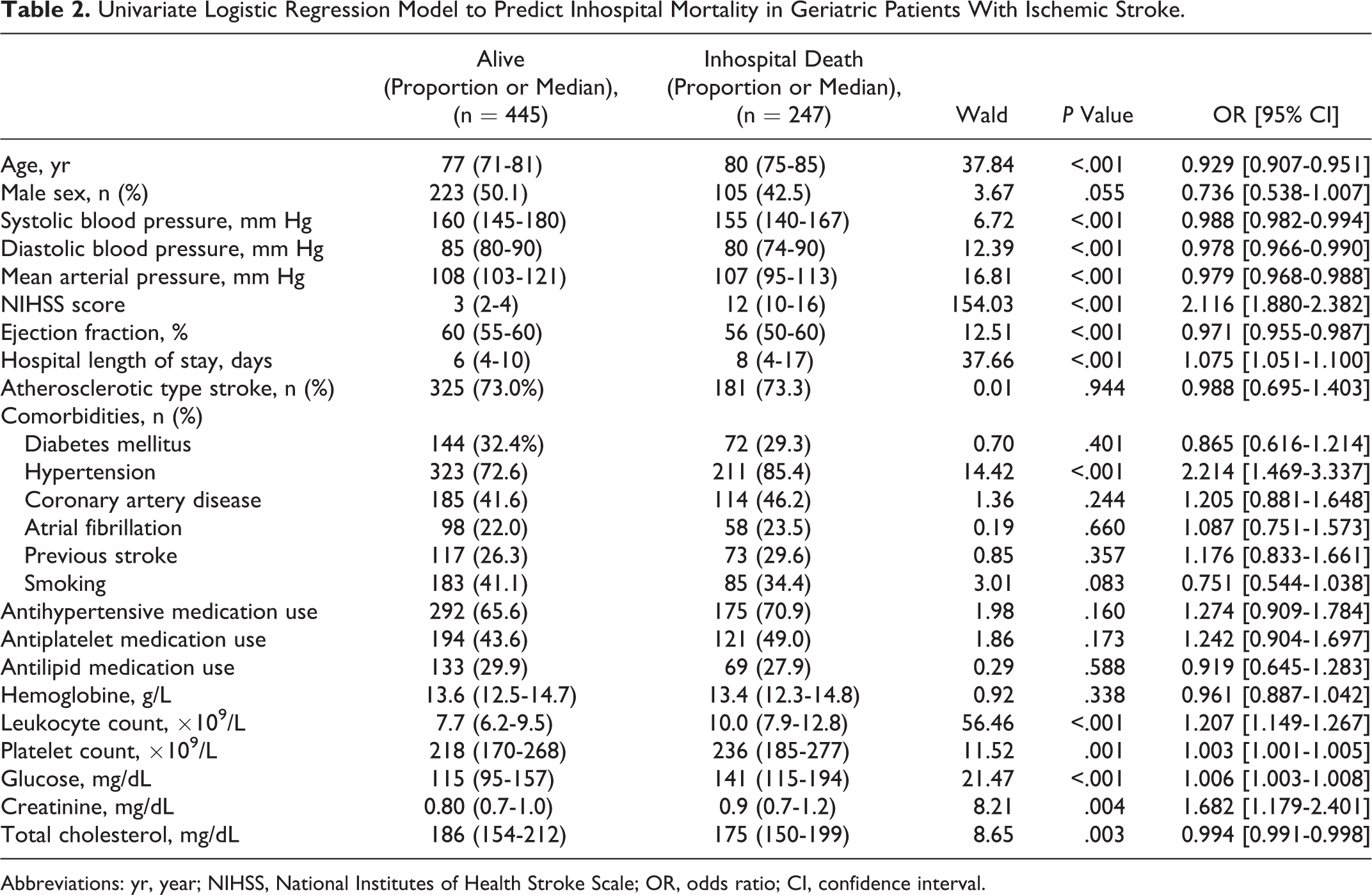
Abbreviations: yr, year; NIHSS, National Institutes of Health Stroke Scale; OR, odds ratio; CI, confidence interval.
We created a multivariate model, which contained significant predictors from the univariate analysis (Table 3). Age, sex, leukocyte count, platelet count, glucose level, creatinine, total cholesterol, ejection fraction, history of HT, NIHSS score, and smoking habitus were included in the multivariate analysis as potential predictors for inhospital mortality. The glucose level and ejection fraction were dichotomized in the model. Also, mean arterial pressure was removed from the model, since this parameter was interdependent with history of HT. With regard to results, increased creatinine levels (OR: 2.002 [95% CI: 1.235-3.243]), elevated platelet count (OR: 1.006 [95% CI: 1.002-1.010]), NIHSS score (OR: 2.085 [95% CI: 1.835-2.370]), and increased glucose levels (OR: 2.610 [95% CI: 1.023-6.660]) were found to be independent predictors of inhospital mortality.
Multivariate Logistic Regression Model to Predict Inhospital Mortality in Geriatric Patients With Ischemic Stroke.
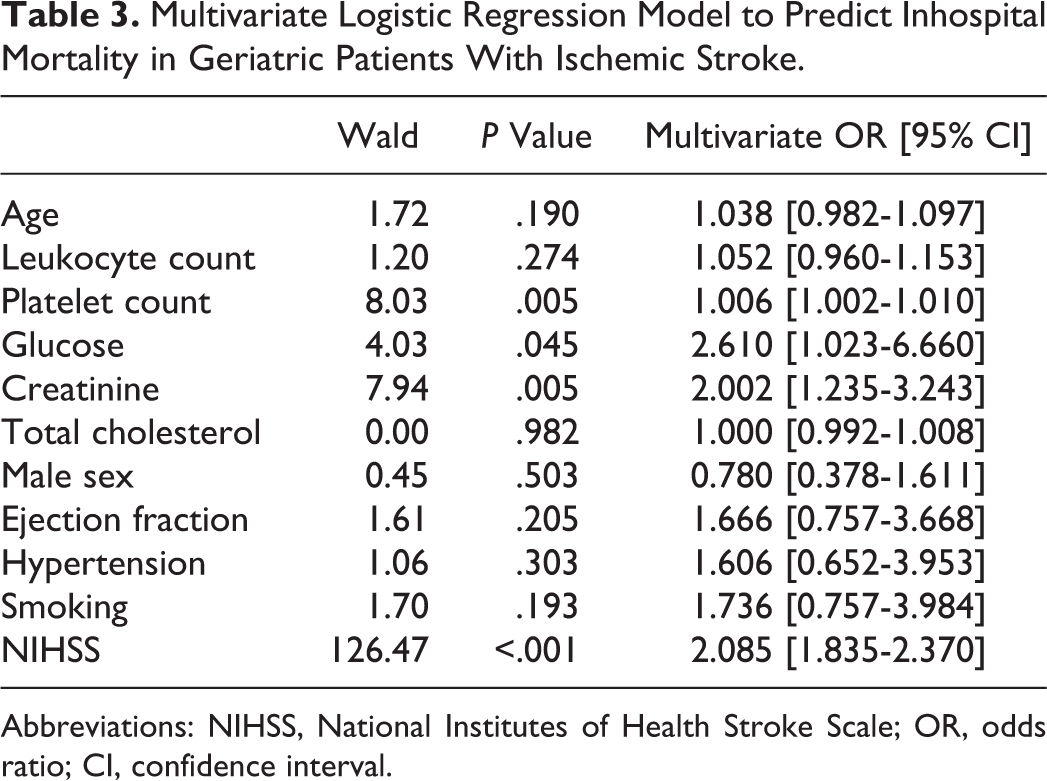
Abbreviations: NIHSS, National Institutes of Health Stroke Scale; OR, odds ratio; CI, confidence interval.
Discussion
In this study, we analyzed the independent predictors of 30-day inhospital mortality in a geriatric population presented to an urban ED with ischemic stroke. Hyperglycemia, elevated creatinine levels, increased platelet count, and increased NIHSS score were found to be independent predictors of mortality. Regarding the literature, very few studies generated predictive models for early mortality using a specific cohort, such as geriatric patients with ischemic stroke.
Grube et al investigated the influence of acute complications on outcome 3 months after acute ischemic stroke. In this study, older age, stroke severity, prestroke dependency, and previous strokes were found to be predictors of poor outcome at 3 months. They divided patients with ischemic stroke in terms of age to predict mortality, and patients older than 85 years had an OR of 6.76 (95% CI, 2.66-17.20) compared to patients younger than 65 years. Mortality was evident in patients older than 75 years in this study. 8 Similarly, Kaplan et al stated that advanced age was an independent predictor of death and coronary heart disease events but not recurrent stroke. 9 As the population ages and geriatric patients represented a heterogenous group, we found aging to be a nonsignificant determinant in predicting mortality (OR: 1.038 [95% CI, 0.982–1.097]). Most of the studies stated that the effect of aging on mortality was observed in patients younger than 70 years. 8 –10
Hypertension is an important risk factor for ischemic stroke. Some studies, which consisted of patients with ischemic stroke, stated a moderate to no relationship between history of HT and poor stroke outcome in the elderly and general population. 11,12 However, a multicenter study, consisting of 2349 patients with ischemic stroke, was analyzed; the independent influence of early inhospital complications and history of HT was found to be one of the independent predictors of mortality 3 months after ischemic stroke. 8 There is still debate about the relationship between a history of HT and outcomes in geriatric population.
Blood pressure at admission typically spontaneously decreases during the acute phase of ischemic stroke and the initial measurement of blood pressure has extremely limited value for stroke outcome. 13,14 Decrease in the mean arterial pressure was found to be statistically significant in the univariate analysis; however, the multivariate analysis did not confirm the results.
Preexisting renal functions also play an important role in stroke outcome. Renal impairment in patients with acute stroke was not uncommon. In acute setting, more than 25% of all patients with stroke presented with different stages of renal dysfunction. 15 A retrospective study, evaluating patients having stroke with functional outcome, argued that lower creatinine clearance calculated at admission is an independent predictor of inhospital mortality in ischemic and hemorrhagic strokes. 16 Additionally, several earlier studies confirmed this finding in both stroke subtypes. 17,18 However, a recent study argued that a reduced glomerular filtration rate was a strong predictor of poor outcomes for hemorrhagic but not for ischemic strokes. 15 Renal dysfunction is also a growing problem among elderly patients. 19 After an ischemic cerebrovascular event, preexisting renal dysfunction and prolonged hospitalization concomitant with dehydration due to decreased oral intake may worsen renal impairment and may result in poor outcomes in older patients compared to younger individuals. Although creatinine clearance was not calculated at admission in our study population, basal creatinine levels could also accurately predict a worse outcome in the emergency setting.
Regarding our results, elevated leukocyte levels was not found to be an independent predictor of inhospital mortality. Elevated white blood cell count is postulated as a part of the strong systemic inflammation, which is triggered by necrosis in the brain of patients with acute stroke; it is strongly associated with initial stroke volume and severity. 20 –22 However, in older individuals, elevated white blood cell counts might also originate from concurrent acute or chronic infections or underlying atherosclerosis. 23 Regardless of the underlying reason, elevated leukocyte count in the acute phase of stroke was accepted as an independent predictor of initial stroke severity, poor clinical outcome after 72 hours, and discharge disability. 24 Our findings did not confirm these results in older individuals.
Atrial fibrillation was not found to be an independent predictor of mortality in this study. This finding is similar to previous studies of patients older than 80 years. 25,26 Additionally, the ejection fraction affected mortality in univariate results; however, this finding was not apparent in the multivariate analysis.
There are several limitations to this study. First, this is a retrospective, single-center study, and all data were gathered from medical records using a hospital database system. The study group consisted only of patients who had sufficient data to be included in the analysis. Second, only 30-day inhospital mortality from data available in the ED was analyzed in the present study. Long-term follow-up might add additional information about predictors of mortality, such as the need for mechanical ventilation, days in the intensive care unit, or documentation of infectious complications.
In conclusion, the present study dealt with a specific cohort of patients with ischemic stroke. We found that increased NIHSS score, hyperglycemia, renal impairment, and elevated platelet count were independent predictors of mortality in older individuals who presented to ED with ischemic stroke.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.