
Abstract
Background:
There have been concerns about the possible prothrombotic effects of nilotinib, especially in patients having cardiovascular risk factors. The potential mechanism behind the increased risk of thromboembolic events is still not clear.
Objectives:
In this study, we aimed to evaluate possible harmful effects of nilotinib on endothelial cells. To this aim, we examined proliferative capacity and secretory functions of healthy human carotid artery endothelial cells (HCtAECs) in response to nilotinib.
Methods:
3-(4,5-Dimethylthiazolyl-2)-2,5-diphenyltetrazolium bromide (MTT) cell proliferation method was used to determine antiproliferative effects of nilotinib on HCtAECs. The HCtAECs were incubated with 5, 10, and 100 nmol/L doses of nilotinib for 72 hours. Then, in order to assess the endothelial function, levels of nitric oxide (NO), von Willebrand factor (vWF), tissue plasminogen activator, plasminogen activator inhibitor 1 (PAI-1), and endothelin 1 (ET-1) were evaluated using enzyme-linked immunosorbent assay from tissue culture supernatants.
Results:
There were slight but statistically significant decreases in cell proliferation in response to nilotinib. Nilotinib increased the secretion of t-PA, PAI-1, and vWF in a dose-dependent manner when compared with the untreated control group. The ET-1 secretion was lower in 5 nmol/L and higher in 10 and 100 nmol/L nilotinib-treated cells as compared to untreated cells. Regarding NO secretion, lower levels were observed in 5 and 10 nmol/L, and higher levels were detected in 100 nmol/L nilotinib-treated cells as compared to untreated control group cells.
Conclusion:
Considering the results obtained in our study, nilotinib does not affect the functions of endothelial cells either in a prothrombotic or an antithrombotic fashion, despite a dose-dependent decline in cell viability.
Introduction
Chronic myeloid leukemia (CML) is a clonal disease of pluripotent stem cell and is associated with fusion of the 2 genes: BCR (on chromosome 22) and ABL (on chromosome 9) resulting in the BCRABL1 fusion protein. Deregulated tyrosine kinase activity of this abnormal fusion protein is implicated in the pathogenesis of CML. 1,2
Nilotinib (Tasigna [nilotinib], formerly known as AMN107; Novartis) is a novel oral aminopyrimidine derivative that has been rationally designed to be more selective against the Bcr-Abl tyrosine kinase than imatinib. Nilotinib competitively inhibits adenosine triphosphate binding site of BCRABL1 with higher affinity and specificity than imatinib. The superior effects of nilotinib may result from its strong effects on BCR/ABL (including BCR/ABL-mutants) and its effects on additional drug targets. However, such additional targets are also expressed in nonhematopoietic cells and may thus be responsible for nonhematologic adverse events.
The most common nonhematologic side effects reported are skin rashes, headache, diarrhea, elevations of pancreatic enzymes, serum bilirubin, and fasting plasma glucose. Generally, these side effects are self-limited or easily manageable. 3 –5 Despite these nonlife-threatening side effects, some serious side effects such as severe and treatment resistant peripheral arterial occlusive disease and some other vascular occlusive conditions are being published in either patients who were just on nilotinib therapy or the ones who has switched from imatinib to nilotinib. 6 –8
Up to now, it is well established that these serious side effects are commonly seen in patients who are just harboring well-known vascular disease risk factors like smoking, arterial hypertension, diabetes mellitus, obesity, or advanced age. But still it is unclear that which of the patients on nilotinib therapy are candidates for vascular unwanted complications. 6,7
Some possible explanations are proposed considering the pathogenetic mechanisms of vascular side effects like metabolic side effects of the drug, direct cytotoxic effects of the drug on vascular cells, or the effect of the drug on coagulant and fibrinolytic system. But still it is unclear that which of these proposed mechanisms is the key factor inducing the unwanted vascular events. 3
Considering the venous thromboembolic events, the main responsible pathogenetic mechanisms are stasis and soluble coagulant factors. Unlikely in arterial occlusive diseases, the main pathogenetic mechanisms are endothelial injury and dysfunction. In this manner, we hypothesized that the cytotoxic effects and concurrent endothelial dysfunction caused by nilotinib, which are mainly associated with the alteration of pathways related to tyrosine kinase inhibition, are responsible from the unwanted arterial occlusive side effects. In order to establish the effect of the drug on endothelial cell viability and function, we designed a cell culture study with healthy carotid artery endothelial cells. We evaluated the cell viability with increasing doses of nilotinib and endothelial function with measuring nitric oxide (NO), plasminogen activator inhibitor 1 (PAI-1), endothelin 1 (ET-1), tissue plasminogen activator, and von Willebrand factor (vWF).
Materials and Methods
Chemicals
The stock solution of nilotinib was dissolved in dimethylsulfoxide (DMSO) at a concentration of 10 mmol/L, stored at −20°C, and diluted in cell culture medium. The final concentration of DMSO did not exceed more than 0.1% in culture. Artery endothelial cell growth medium was obtained from Cell Applications Inc (San Diego, California. ABD).
Cell Line and Culture Conditions
Human carotid artery endothelial cells (HCtAECs) were obtained from Cell Applications Inc (ABD) and grown in T-75 flask containing 15 mL of artery endothelial cell growth medium under conditions as recommended by the manufacturer. Briefly, the cells were incubated in a 5% CO2 atmosphere at 37°C and passaged when reaching 80% confluency. In order to avoid any changes in cell physiology, the cells were only used within 3 to 5 passages. The HCtAECs were previously used to demonstrate the endothelial responses to hemodynamic stress and inflammation. 9 –11
Measurement of Cytotoxic Effects of Nilotinib on HCtAECs by 3-(4,5-Dimethylthiazolyl-2)-2,5-diphenyltetrazolium Bromide Cell Proliferation Assay and Determination of Nilotinib Effect on HCtAEC Confluency
Because of the cell culture—in vitro design of the study, the in vivo effective plasma concentrations of nilotinib was ignored, and cytotoxic effects of nilotinib on HCtAECs were determined by 3-(4,5-dimethylthiazolyl-2)-2,5-diphenyltetrazolium bromide (MTT) cell proliferation assay. The basic principle of this assay is based on the reduction of the yellow tetrazolium MTT in metabolically active cells by the action of dehydrogenase enzymes partly. The resulting intracellular purple formazan can be solubilized and quantified by spectrophotometric techniques. In short, 5 × 10 3 cells/well were seeded into 96-well plates containing 100 µL of the growth medium in the absence or presence of increasing concentrations of nilotinib (0.1-100 nmol/L) and then incubated at 37°C in 5% CO2 for 48 and 72 hours. After incubation period, the cells were treated with 20 µL MTT for 4 hours. Then, plates were centrifuged for 10 minutes at 580g. After centrifugation, supernatants were removed from the plates, and then the MTT crystals were homogenized by adding 100 µL DMSO into each well. In order to homogenize the pellets more efficiently, the plates were shaken for 5 minutes by shaker. Afterward, the plates were read under 570 nm wavelengths by enzyme-linked immunosorbent assay (ELISA) reader (Thermo Electron Corporation Multiskan Spectrum, Finland). Finally, half maximal inhibitory concentration value (drug concentration that inhibits cell growth by 50%) of nilotinib was calculated from the cell proliferation plots. The effect of 48- and 72-hour nilotinib treatment on the confluency of HCtAECs was also checked. To achieve this, HCtAECs were seeded in 2 mL growth medium with a density of 1 × 10 6 cells/well in 6-well plates. After attachment of the cells to the surface, they were treated with different concentrations of nilotinib (5, 50, and 100 nmol/L).
Collection of HCtAECs Treated With Nilotinib for ELISA Assay
The HCtAECs were seeded in 2 mL growth medium with a density of 1 × 10 6 cells/well in 6-well plates. After attachment of the cells to the surface, they were treated with different concentrations of nilotinib (5, 10, and 100 nmol/L) for 72 hours. Control cultures were incubated with growth medium. After 72 hours incubation, cell culture supernatants were collected and frozen at -80°C before analysis by ELISA.
Determination of PAI-1, t-PA, ET-1, vWF, and Total NO Levels by ELISA
The PAI-1 protein levels in supernatants were measured by using sandwich ELISA kit (Wuhan Boster, Wuhan, China) which employs antihuman PAI-1 antibody as the capture antibody. Following kit instructions, the supernatant was incubated in precoated microtest wells and was detected with a secondary biotinylated antibody that recognizes the bound PAI-1 molecules. Adding 100 μL avidin biotin peroxidase completed the formation of the antibody–enzyme detection complex. After the addition of 90 μL tetramethylbenzidine (TMB) substrate, a blue-colored solution was formed. The levels of PAI-1 were quantified by measuring solution absorbances at 450 nm and comparing the values with those of a standard curve prepared from 6 human PAI-1 standard dilutions.
Human t-PA platinum ELISA (e-Bioscience, California) kit was used for quantitative detection of human t-PA in the supernatants. This system includes microwells coated with antihuman t-PA coating antibody. The supernatant was added to recoated microwells and then 50 μL horseradish peroxidase (HRP)-conjugated antihuman t-PA antibody was added and bound to human t-PA captured by the first antibody. Tetramethylbenzidine substrate of 100 μL was added, and colored product was formed in proportion to the amount of human t-PA present in the sample. Absorbance is measured at 450 nm. A standard curve is prepared from 7 human t-PA standard dilutions and human t-PA concentration determined.
The ET-1 protein levels in supernatants were detected by using human ET-1 sandwich ELISA kit (Cusabio, Wuhan, China). Supernatants of 100 μL were pipetted into the wells that were precoated with antihuman ET-1 antibody. Then, 100 μL biotin-conjugated antibody specific for ET-1 is added to the wells. After washing, 100 μL avidin-conjugated HRP was added to the wells. Following a wash to remove any unbound avidin-enzyme reagent, 90 μL TMB solution was added to the wells and color developed in proportion to the amount of ET-1 bound in the initial step. The intensity of the color was measured at 450 nm. A standard curve is prepared from 6 human ET-1 standard dilutions.
To determine the vWF levels, sandwich ELISA kit (Asserachrom, Boehringer-Mannheim, Germany) using antihuman vWF antibody as the capture antibody was used. Diluted supernatants of 200 μL were put into the precoated microwells, and then 200 μL anti-vWF peroxidase was added after several washing steps. Then, 200 μL TMB substrate was added to the wells, and color intensity was measured at 450 nm. Levels of vWf were determined by comparing the values with those of a standard curve prepared from 4 human vWF standard dilutions.
For the quantitative determination of NO concentrations in the supernatants, Total Nitric Oxide and Nitrate/Nitrite Assay kit (R&D Systems, Minnesota) with 2 options, endogenous nitrite and total nitrite measurements, was used. To obtain the nitrite concentration, endogenous nitrite is subtracted from the total nitrite value. Endogenous nitrite level was determined as a first step. After the addition of 50 μL diluted samples to the wells, 50 μL reaction diluent, 50 μL Griess reagent I (sulfanilamide), and 50 μL Griess reagent II (N-(1-naphthyl)ethylenediamine) were introduced into the wells in an order. The optical density (OD) of each well was measured using a microplate reader set at 540 nm, and endogenous nitrite concentration was calculated by using a standard curve prepared from 6 nitrite standards. As a second step, to measure the amount of total nitrite, 50 μL diluted samples, 50 μL reaction diluent, 25 μL β-nicotinamide adenine dinucleotide, and 25 μL nitrite reductase were added to the wells, and mixture is incubated at 37°C. After incubation period, 50 μL Griess reagent I and 50 μL Griess reagent II were added and incubated at room temperature. Finally, OD of each well was measured at 540 nm. Total nitrite concentration was calculated by using a standard curve prepared from 6 nitrite standards. The study was approved by the local ethics committee of Dokuz Eylul University.
Statistics
Results were expressed as mean ± standard deviation. Data were analyzed by 1-way analysis of variance followed by Tukey post hoc test depending on the 6 measurements achieved for each parameter. Values with P < .05 were accepted as significant comparing control.
Results
Cytotoxic Effects of Nilotinib on HCtAECs
Cytotoxic effects of nilotinib on HCtAECs were determined by MTT cell proliferation assay. Based on the MTT results, there were very small but statistically significant decreases in the proliferation of the cells in a dose- and time-dependent manner (Figure 1). At higher concentrations of nilotinib (50 and 100 nmol/L), there were still approximately 80% alive cells even after 72-hour treatment. Therefore, it could be concluded that the treatment with nilotinib could not cause significant damage to HCtAECs. The effect of nilotinib on the confluency of HCtAECs was also visualized under microscope. Although 48-hour nilotinib treatment did not affect their confluency at 5 and 10 nmol/L nilotinib, there was 10% decrease in their confluency at 100 nmol/L nilotinib applied samples as compared to untreated control group. On the other hand, the cells were confluent like control sample at 5 nmol/L nilotinib, but there were 10% and 20% decreases in their confluency at 10 and 100 nmol/L nilotinib after 72 hours incubation, respectively.
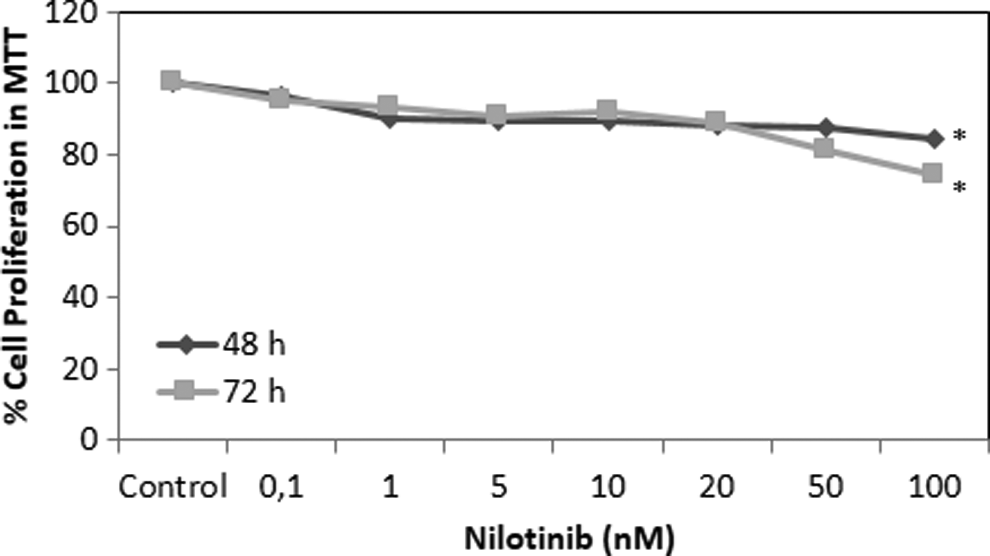
Cytotoxic effects of nilotinib on human carotid artery endothelial cell (HCtAEC). The results are the means of 3 independent experiments. The error bars represent the standard deviations. Statistical significance was determined using 1-way analysis of variance, and *P < .05 was considered to be significant.
Effects of Nilotinib on the Secretory Functions of HCtAECs
To determine the expressions of t-PA, PAI-1, ET-1, vWF, and total NO in HCtAECs, we subjected the cells to increasing concentrations of nilotinib for 72 hours and assessed protein expression by ELISA. The investigation of the effect of increasing concentrations of nilotinib on the secretion of t-PA displayed that nilotinib caused 1.14-, 1.28-, and 1.32-fold increases in t-PA levels from HCtAECs as compared to untreated control cells in response to 5, 10, and 50 nmol/L nilotinib, respectively (Figure 2A). On the other hand, there were 1.13-, 2.25-, and 2.5-fold increases in the expression of PAI-1 at 72 hours (Figure 2B). As indicated in Figure 2C, ET-1 expression was not significantly induced at 5 nmol/L nilotinib but there were 1.14- and 1.35-fold increases at 10 and 100 nmol/L nilotinib, respectively. The expression of vWF increased for 2.61- and 2.12-fold in response to 10 and 100 nmol/L nilotinib, respectively, although there was no significant effect of 5 nmol/L nilotinib (Figure 2D). Moreover, total nitride oxide level increased only at the highest nilotinib concentration when compared to untreated cells (Figure 2E).
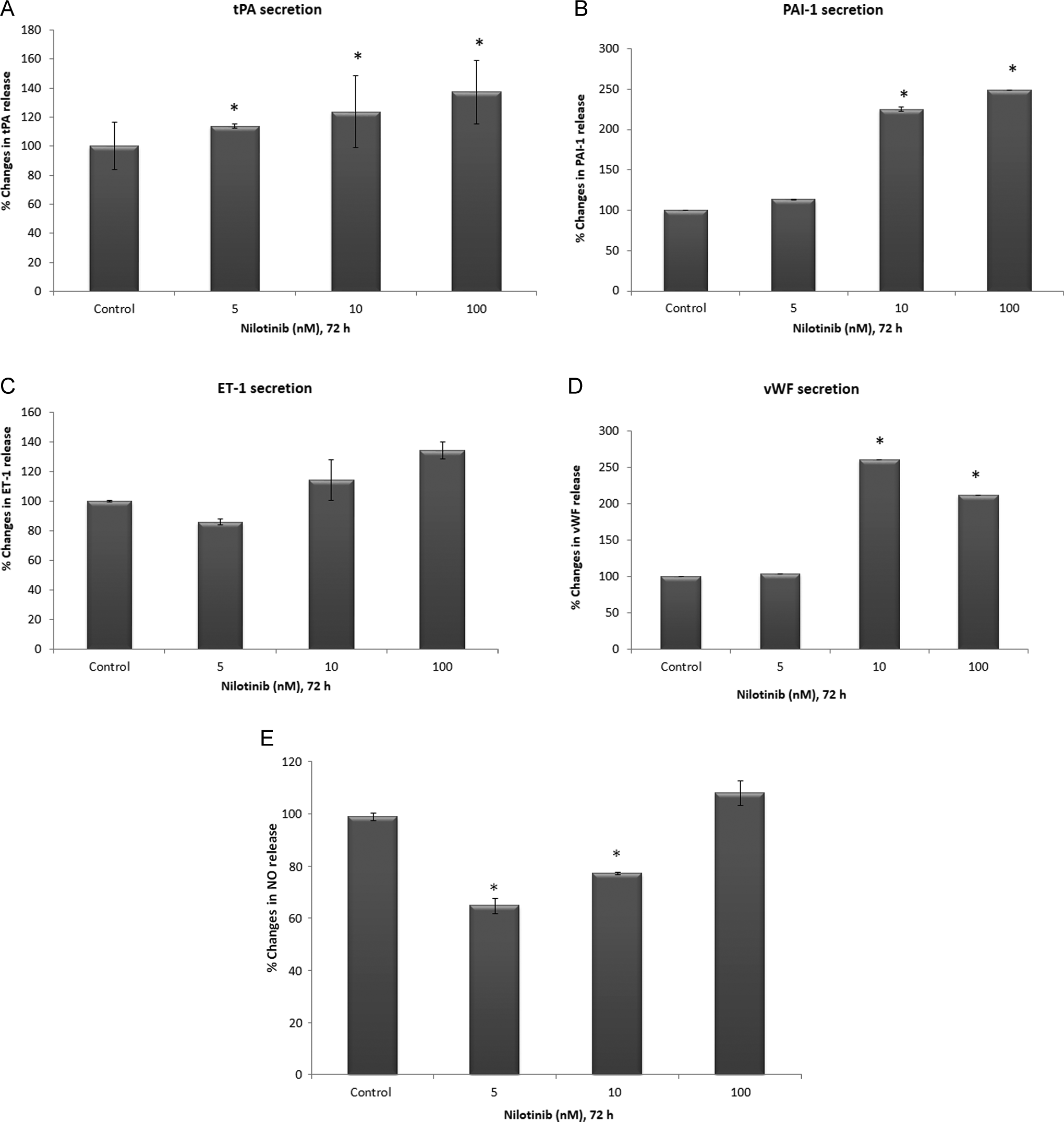
Effects of nilotinib on the release of t-PA (A), plasminogen activator inhibitor 1 (PAI-1; B), endothelin 1 (ET-1; C), von Willebrand factor (vWf; D), and nitric oxide (NO; E). The results are the means of 2 independent experiments. The error bars represent the standard deviations. *P values <.05 were considered statistically significant.
Discussion
Incidence of CML and also the comorbid cardiovascular disorders increase parallelly with aging. This issue has an important impact on the therapeutic approaches, disease management, prognosis, and even survival. Tyrosine kinase inhibitors revolutionally altered the outcome of the disease. They are generally well tolerated and exhibits significantly less side effects compared with the conventional chemotherapeutics. Nevertheless, especially in patients harboring cardiovascular risk factors, they can cause serious life-threatening side effects like prolongation of QT time, symptomatic heart failure, and sudden cardiac death. 12
Despite well-known and established cardiovascular side effects, some rare toxicities and complications are being published. Some of those important and life-threatening side effects are therapy resistant or relapsing arterial occlusive and coronary disorders, which are mainly affecting the patients on nilotinib treatment or the ones which was switched to nilotinib. In some cases, these unwanted occlusive events occur with no attributable cardiovascular risk factor. 6 –8,13,14
At a recent work of Emir Hadzijusufovic et al, which was presented as a poster in ASH 2012 and not yet published, in vitro effects of nilotinib on human umbilical vein endothelial cells (HUVECs) were evaluated. They have shown that nilotinib, but not imatinib, was found to inhibit HUVEC migration and sprouting in a scratch-wound healing assay. Finally, nilotinib but not imatinib was found to block the growth of various human pancreatic cell lines, including human caucasian pancreatic cell line 1 (PANC-1) and the insulin-producing cell line 1.4E7. They have concluded that their data showed that nilotinib exerts direct inhibitory effects on endothelial cells and pancreatic cells. In addition, the exact proatherogenic effect of nilotinib in second-line- and first-line-treated patients with CML remains unknown since no data from prospective clinical trials focusing on this issue are available. Until these questions and safety issues have been clarified, they mentioned that it may be advisable to take certain comorbidities into account when considering the use of nilotinib in patients with CML. In addition, the follow-up of long-term-treated patients should include parameters that can detect vascular events and predisposing comorbidities as early as possible. In this study of Hadzijusufovic, the examined cells were venous cells, and the endothelial cell functions were not evaluated.
Considering the results obtained in our study, nilotinib does not affect the functions of endothelial cells either in a prothrombotic or an antithrombotic fashion. In this manner, specification of a tyrosine kinase pathway considering the endothelial secretory functions affected with nilotinib is not possible. The carotid artery endothelial cell viability decreases with increasing doses of nilotinib. Thus, it can be suggested that the “endothelial regeneration” under certain circumstances is impaired and can cause tendency to thrombosis in patients using nilotinib. In addition to these implications, one of the limitations of our study is the difficulty of constructing net relevancy between the in vitro and in vivo conditions. Besides, to our knowledge, this is the first report establishing the effect of nilotinib on arterial endothelial cell viability and function. Some further studies may better clarify the mechanism responsible from the cytotoxic effect of nilotinib on endothelial cells and contribute to a better knowledge to manage these unwanted life-threatening occlusive side effects.
Footnotes
Authors’ Note
The article was presented at “18th Congress of European Hematology Association” in Sweden, 2013.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.