
Abstract
Objective:
To investigate the occurrence of myocardial infarction or other acute coronary syndromes in rare congenital bleeding disorders.
Patients:
All patients with factor I (FI), factor II (FII), factor V (FV), factor VII (FVII), factor X (FX), factor XI (FXI), or factor XIII (FXIII) deficiency or abnormality reported to have presented a myocardial infarction or another acute coronary syndrome were investigated. The condition had to be demonstrated by objective means, including a coronary/angiography. Cases of stable angina were excluded.
Results:
A total of 53 patients (4 had FI, 2 had FV, 2 had FVII, 36 had FXI, 1 had FXIII deficiency, and 8 patients had platelet disorders) met the inclusion criteria . No patient with FII or FX deficiency and acute coronary disease met the inclusion criteria. In the majority of patients, common risk factors were present, namely hypertension, hypercholesterolemia, smoking, and diabetes. Replacement therapy was involved in 5 cases.
Conclusion:
The congenital hypocoagulability present in these patients was unable to allow a protection from acute coronary diseases. The significance of the findings is discussed.
The occasional occurrence of myocardial infarction (MI) and other acute coronary syndromes (ACSs) in patients with the major congenital bleeding disorders is now an established fact. Recent studies have shown that at least 200 patients with hemophilia A, hemophilia B, or Von Willebrand (vWD) disease have had an MI. 1 –6
Information on rare congenital bleeding disorders are scanty and less clear. 7,8 This is obviously due to the relative rarity of these conditions in comparison with the hemophilias or vWD disease. The only exception appears to be factor XI (FXI) deficiency which, being relatively frequent among the Jewish population, its study has allowed pertinent investigation on the subject. 9,10
Altogether, the rare congenital bleeding disorders, including FXI deficiency, constitute only about 10% of all congenital bleeding disorders. Despite this rarity, they represent an interesting field of investigation and have contributed considerably to the understanding of blood coagulation.
The purpose of the present study is to investigate the prevalence of MI in these rare bleeding conditions in an attempt to discover potential similarities and discrepancies in the role played by single clotting factor deficiencies or by platelet defects in the pathogenesis of arterial occlusions.
Patients and Methods
A time-unlimited PubMed search was carried on March 2013 and again in January 2014 .Several pertinent key words were used together with those supplied by PubMed as the Medical Subject Headings.
The key words and descriptions searched for include rare congenital bleeding defects, congenital platelet disorders, MI, ACSs, arterial occlusions, coronary disease, unstable angina, coronary invasive procedures, coronary angiography, and troponin elevation. The search was also carried out using the single coagulation factor as main heading.
The detail Tabs sometimes supplied by PubMed were also examined in every instance. Cross-checking of the references listed at the end of the each article was also carried out to avoid omission.
Inclusion criteria for the plasmatic defects (fibrinogen, factor II [FII], factor V [FV], factor VII [FVII], factor X [FX], factor XI [FXI], and factor XIII [FXIII] deficiencies) were activity factor level less than 15% of normal and a compatible hereditary pattern. The antigen level of the factor involved was not relevant in the sense that all cases were included, providing the 2 above-mentioned conditions were met. Mutations were included whenever available. Cases of multiple defects such as combined FV and FVIII deficiency and prothrombin complex factors deficiency were excluded. Acquired forms of factor deficiencies were also excluded.
Inclusion criteria for platelet disorders (Glanzmann thrombasthenia [GT], Bernard Soulier syndrome [BSS], and MYH9 macrothrombocytopenia) were based on pertinent platelet count and morphology, bleeding time prolongation when appropriate, compatible hereditary pattern, and lack of concomitant plasmatic defects.
Full fledged MI, non-ST-segment elevation MI, and unstable angina had to be proven by clinical features, electrocardiogram alterations, troponin elevation as appropriate, and coronary angiography. Cases of stable angina or effort angina were excluded even if documented by coronary angiography.
The presence of associated risk factors such as hypertension, diabetes, smoking, obesity, dyslipidemia, old age (>70), and congenital thrombophilia was always recorded whenever feasible. Potential association of the coronary event with replacement therapy was always searched for. The observation period was limited, regardless of the dosage, to a week before the thrombotic event occurred. The therapeutic measures adopted and the evolution of the condition were also always analyzed whenever possible.
Results
The time-unlimited survey of the literature yielded 53 patients with rare congenital bleeding conditions and an MI or an ACS (Table 1).
Myocardial Infarction and Other Acute Coronary Syndromes in Rare Congenital Coagulation Disorders.
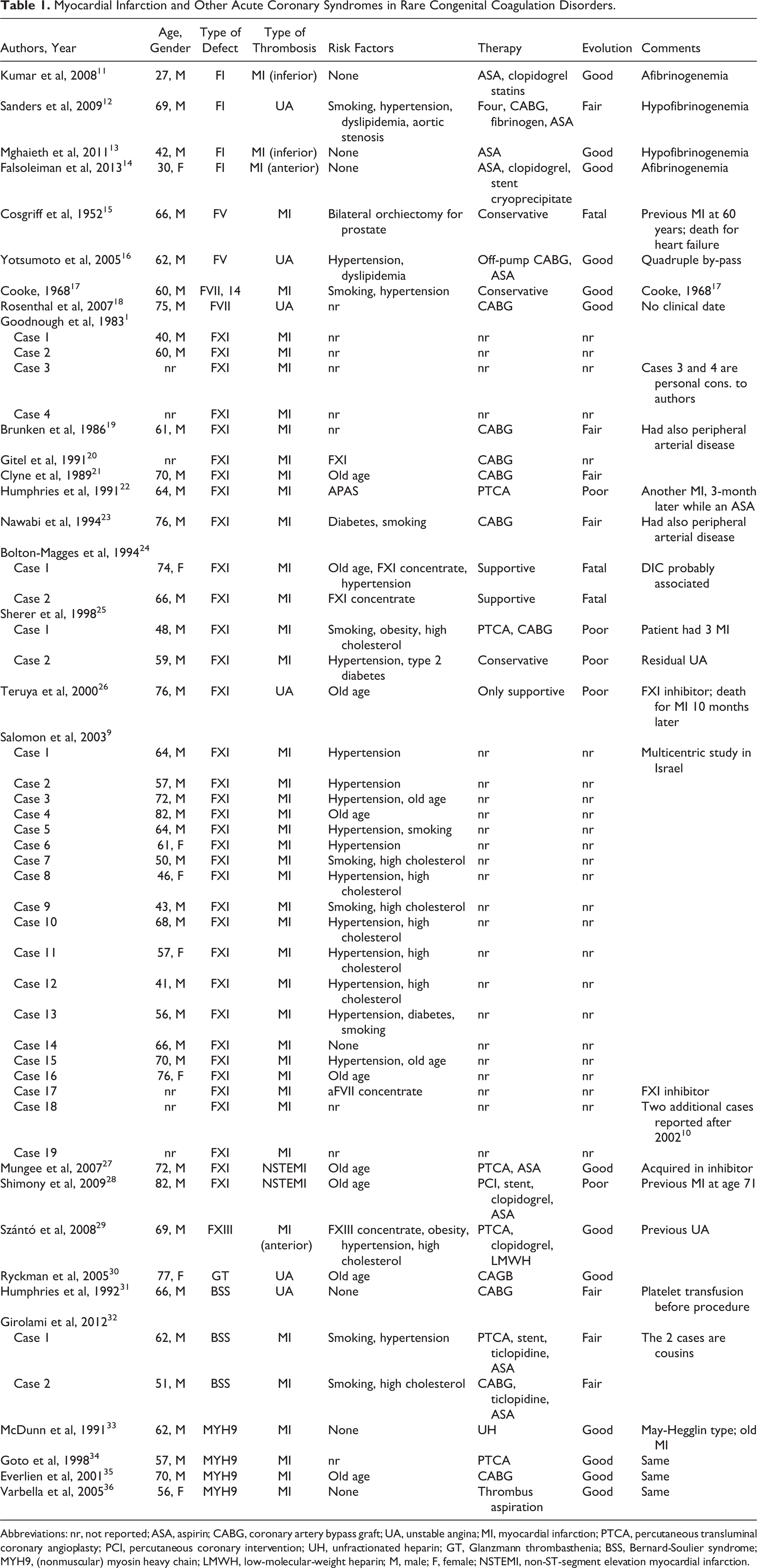
Abbreviations: nr, not reported; ASA, aspirin; CABG, coronary artery bypass graft; UA, unstable angina; MI, myocardial infarction; PTCA, percutaneous transluminal coronary angioplasty; PCI, percutaneous coronary intervention; UH, unfractionated heparin; GT, Glanzmann thrombasthenia; BSS, Bernard-Soulier syndrome; MYH9, (nonmuscular) myosin heavy chain; LMWH, low-molecular-weight heparin; M, male; F, female; NSTEMI, non-ST-segment elevation myocardial infarction.
The breakdown figures were fibrinogen deficiency: 4 patients; FV deficiency: 2 patients; FVII defects: 2 patients; FXI defect: 36 patients; FXIII: 1 patient 4,5,9 –29 ; and platelet disorders: 8 patients, 1 with GT, 3 with BSS, and 4 with MYH9 defects. 30 –36 The age varied between 27 and 82 (mean age was 60.2). No patient with either FII or FX deficiency was found to meet the inclusion criteria; 7 were female, 39 were male whereas in 6 instances, gender was not reported.
One or more than one associated risk factor were present in 36 patients. In 6 patients, there were no risk factors, whereas in the remaining patients no information was supplied in this regard.
The most frequent risk factors were hypertension, smoking, and hypercholesterolemia (Figure 1). Old age was present in 9 instances whereas replacement therapy was traced only in 5 patients. Miscellaneous risk factors included aortic stenosis, antiphospholipid antibodies syndrome (APAS), and surgery (Figure 1).
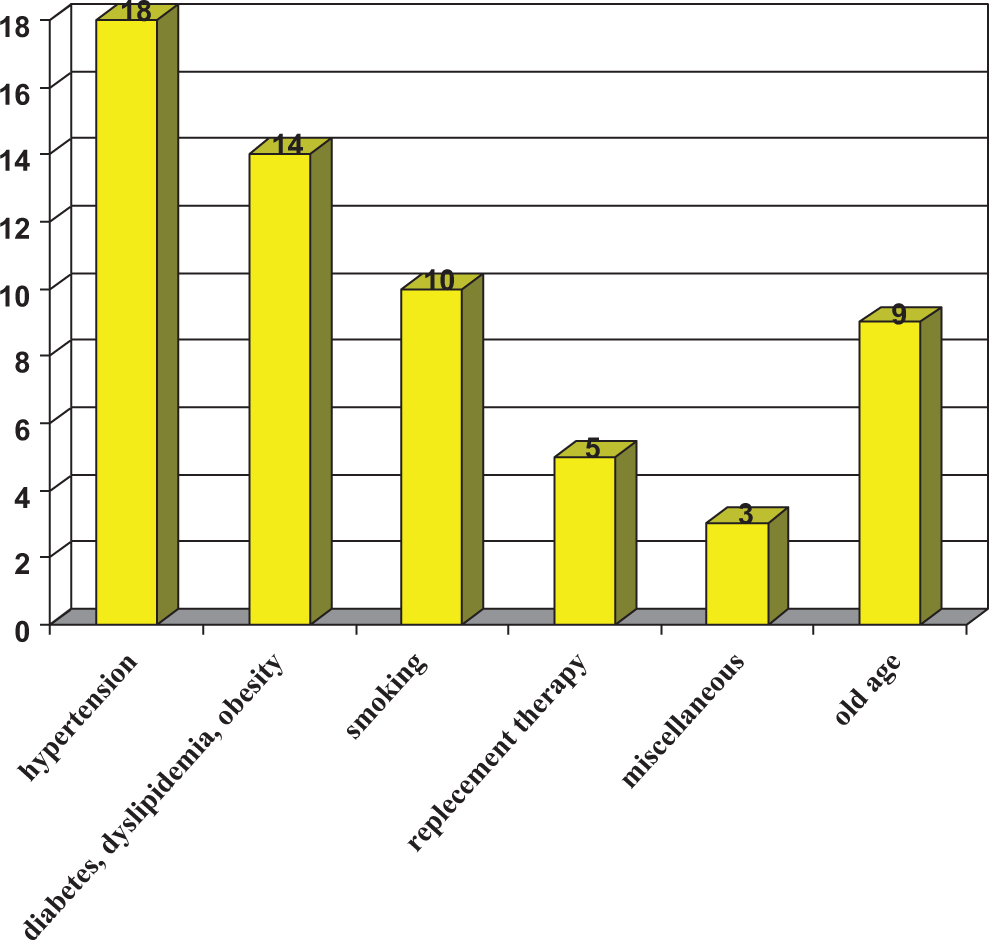
Risk factors present in 36 patients. In 6 patients, there were no risk factors whereas in the remaining patients, no mention was made as to the presence or absence of risk factors. Some patients had more than one risk factor.
The therapeutic approach was conservative or only supportive in 7 cases. Invasive coronary procedures (CABG, PTCA, stent implantation, and thrombus aspiration) were carried out in 20 cases. Therapeutic management was not reported in the remaining patients. Evolution was graded as good or fair for 21 patients. It was poor in 5 and fatal in 3 cases. No data were supplied for the remaining patients. 7
Discussion
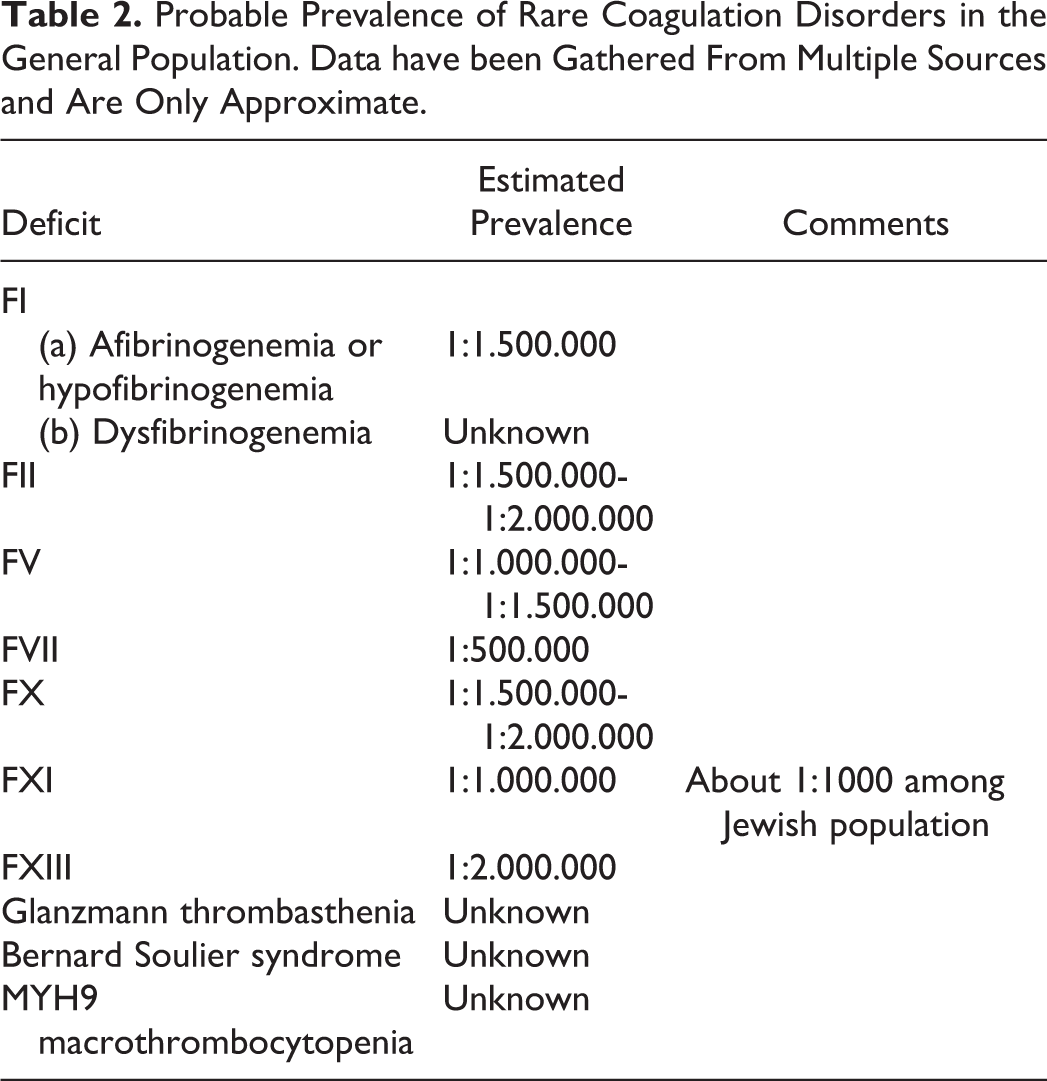
The approximate prevalence of these rare coagulation disorders in the general population is gathered in Table 2. Needless to say that the prevalence of FXI deficiency refers to the approximate overall world wide incidence and not to the Jewish population where it is much higher.
Probable Prevalence of Rare Coagulation Disorders in the General Population. Data have been Gathered From Multiple Sources and Are Only Approximate.
The first observation to be made is the lack of MI or ACSs in patients with FII or FX deficiency. This confirms previous studies, which failed to report even venous thrombosis in these patients. 7 For all the remaining defects, even for those which have a prevalence similar to that of FII or FX deficiency, a few cases of MI have been reported. Whether this has a meaning, or it is just due to chance because of the rarity of these disorders, remains to be proven.
The ACSs seen in these patients is usually not accompanied by the presence of peripheral arteries occlusion but for the case of fibrinogen defects. Occasional ischemic strokes, on the contrary, have been reported. There is an evident discrepancy between the number of MI seen in FXI deficiency and those seen in the other defects.
This is due, mainly, to the high prevalence of the defect in Israel and among the Jewish population of other countries as demonstrated by the observation that the articles with most cases come from Israel. As a matter of fact almost all patients with FXI deficiency and an MI or an ACS have a Jewish background even in the reports coming from outside Israel. The significance of this finding is unclear whether one takes into account the observation that ischemic strokes have been considered relatively rare in the same patients. 10 Interesting, even venous thrombosis has been reported to be rare in FXI deficiency. 37 It would seem that among Jewish people with FXI deficiency, there is a different prevalence between MI or ACS and ischemic stroke. In this regard, it may be also worth noting that at least 2 patients with FXI deficiency presented here also showed peripheral arterial occlusions. 19,23 The single report of an acute coronary disorder in GT is in contrast with the several reported cases of venous thrombosis seen in this condition. 38 Since in BSS syndrome, the opposite seems true, it may be concluded that the defect responsible for GT (abnormalities of Gp IIb/IIIa complex) appears to protect mainly from the arterial thrombosis while the defect present in BSS (defect of GpIb/ IX–V complex) seems to protect mainly from venous thrombosis. This is a fascinating observation, which, should it be confirmed in a large number of patients, would indicate that a defective binding to vWF (abnormalities in the GpIb-IX-V complex) protects more from venous thrombosis whereas a defective binding to fibrinogen (abnormalities in the GpIIb/IIIa) protects more from arterial thrombosis.
In hemophilia A and B, peripheral arterial occlusion or thrombosis has never been described. 1,3
This is another important observation of the present report in the striking prevalence of male gender among the patients, regardless of the defects involved. The ratio is 5.5. Since all these diseases have an autosomal inheritance, one could have expected a more balanced distribution among the 2 genders. Due to the limited number of cases, it is difficult to draw conclusions as to the prevalence of ACS in these patients. An indication may be formulated for FXI deficiency in which the prevalence has been calculated in Israel similar to that observed in the general population. 9
It was known that patients with hemophilia A, hemophilia B, and vWD may develop MI and other ACSs. Now it has been demonstrated that this may occur in almost all other coagulation factors or platelet defects. This indicates that the underlying clotting defect, under certain circumstances, is unable to exercise the expected protection.
The demonstration that in the large majority of these patients common risk factors are present indicates the pivotal role of these risk factors in the pathogenesis of coronary disease. This negative effect may occur even in the presence of a congenital hypocoagulability.
Replacement therapy with FXI concentrate appears particularly dangerous since 3 of the 4 fatalities were patients treated with this concentrate. This is not surprising since that concentrate has been demonstrated to activate the coagulation cascade. 39
The acute management of ACS in these patients is still not well defined. However, similar to that occurred for patients with hemophilia, there is a tendency to treat them as normal individuals with antiplatelet medications providing the underlying defect is, at least, partially connected. 3,8
The significance of the lack of MI or other ACSs in patients with FII or FX deficiency remains to be clarified. These are usually severe bleeding conditions often associated, especially in the past, with early mortality for brain hemorrhage. It is possible that, as a consequence of this, no adequate observation period could be obtained. However, it is also to be noted that FII and FX play a pivotal role in the blood coagulation mechanism and therefore their deficiency may represent a perfect, risk-proofed hypocoagulable state. The recent development and apparent success of the new oral anticoagulant with anti-FIIa or anti-FXa activity could be in agreement with the latter interpretation.
As it had happened for hemophilia A, hemophilia B, and vWD, the study of thrombotic events occurring in patients with rare congenital bleeding disorders has opened new fields of investigation in the understanding of the mechanism of blood coagulation.
Due to the rarity of these bleeding conditions and to the exceptional occurrence in them of a thrombotic event, adequate and useful information may be gathered only by an evaluation of all reported cases.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported in part by the “Associazione Emofilia ed altre Coagulopatie delle Tre Venezie”.