
Abstract
This study was undertaken to provide evidence for the mechanism of venous thromboembolism (VTE) in healthy patients with minor lower limb injury (fracture; Achilles tendon rupture) that was medically managed with plaster cast/brace immobilization. The Plaster Cast clinical trial provided a unique opportunity to identify the natural history of VTE using placebo-controlled patients (n = 183) with validation of the mechanism using the low-molecular-weight heparin (LMWH; reviparin)-treated patients (n = 182). Confirmed VTE in this population was associated with a burst of tissue factor release (and a minor fibrinolytic deficit) leading to thrombin generation that was sustained at least 5 weeks, greater with fractures than with soft-tissue injuries and greater with surgery than with conservative treatment. The root cause likely involves platelet/leukocyte activation (inflammation) rather than endothelial cell injury. Thromboprophylaxis with a low dose of LMWH reduced thrombin generation, with patients undergoing surgery benefitting the most.
Keywords
Introduction
Venous thromboembolic events are a common, life-threatening complication of major trauma. Without prophylaxis, patients with major trauma (including bodily injury from accidents and surgery) have a risk for venous thromboembolism (VTE) that exceeds 50%. 1,2 Pulmonary embolism (PE) is the third most common cause of death in patients with major trauma who survive beyond the first day. 1,3 These observations clearly place patients with major trauma in the high-risk group for VTE.
Patients with trauma having multiple injuries or with isolated lower extremity fractures have a higher risk of VTE than those with single-system, nonorthopedic injuries. 1,4,5 Specific risk factors that were independently associated with an increased incidence of thromboembolism included lower extremity or pelvic fracture, the need for a surgical procedure, increased age, femoral venous line, prolonged immobilization, and duration of hospital stay. In studies of only isolated lower limb trauma, patients with below-knee injuries and immobilization have a 10% to 35% incidence of deep vein thrombosis (DVT) depending on the type and severity of injury, and they have a risk of clinical PE in the range of 0.4% to 2.1%. 4 –10
The Plaster Cast clinical study was conducted by Lassen et al and published in 2002. At the time this investigation was conceived (1996), consensus guidelines stated that patients with isolated lower limb trauma and immobilization are at moderate risk of DVT, but because of the heterogeneity of patient groups and lack of clear evidence, routine prophylaxis was not recommended. 11 –13 The standard of care for patients with lower limb injuries in most countries at that time was no prophylaxis or only short-term prophylaxis in the perioperative setting.
The Plaster Cast clinical study was carried out to confirm the hypothesis that patients treated by functional immobilization with a plaster cast after lower leg trauma require general long-term thromboprophylaxis. 13 This study evaluated the efficacy and safety of the low-molecular-weight (LMW) heparin reviparin (Clivarin; Knoll, Ludwigshafen, Germany), compared to placebo, for the prevention of VTE in patients having an isolated leg injury such as lower extremity fracture or Achilles tendon rupture (ATR). The clinical outcomes demonstrated an incidence of VTE of 19% in patients receiving placebo (including 2 cases of PE) that was significantly reduced to 9% in patients receiving reviparin (P = .01).
At the time the Plaster Cast clinical study was ongoing, we partnered with the Danish clinical investigators to further the appreciation and understanding of the natural history/pathophysiology of VTE associated with isolated lower limb trauma. For the patients of the Plaster Cast clinical study, markers of hemostatic activation were analyzed over time following injury. The obtained data were further analyzed in terms of patients who did and did not receive thromboprophylaxis with the LMW heparin reviparin as a means to validate the identified pathophysiological mechanism. Having a placebo arm in this study provided a unique set of patients to allow such an investigation. This substudy of the Plaster Cast clinical study is described here.
Materials and Methods
Clinical Study
The Plaster Cast clinical study was a prospective, randomized, double-blind, placebo-controlled, parallel group comparison conducted from April 1997 through September 1999 in 6 Danish hospitals. 13 All patients had a lower extremity fracture or an ATR that required at least 5 weeks of functional (ambulatory) immobilization in a plaster cast or brace. They were otherwise healthy. All displaced fractures were treated surgically by open reduction and internal fixation before immobilization. Other fractures were treated conservatively. The ATRs were operatively sutured if it was locally preferred.
All patients gave written informed consent for enrollment into the study. Patients were randomized to either subcutaneous LMW heparin (1750 anti-factor Xa [FXa] units once daily reviparin [Clivarine]) or placebo (saline) administered for a duration of 5 to 6 weeks. Of the 371 enrolled patients who had evaluable venograms, 183 were assigned to reviparin and 188 to placebo. Patients who had undergone surgery before randomization were allowed to receive other heparin prevention but not for more than 4 days prior to enrollment. Mean time from surgery to randomization was 2.3 ± 0.8 days in both the groups.
Bilateral ascending phlebography was performed to detect DVT on the day the brace was removed in all patients. The DVT was confirmed if present on the phlebogram with a constant intraluminal filling defect, or a constant nonvisualization of a proximal vein in the presence of a sudden cutoff, on at least 2 projections. Compression ultrasound could be used for confirmation of the diagnosis only in patients with symptoms of DVT. In this case, an objective documentation (picture) was required. A DVT was considered to be confirmed by compression ultrasound if there was noncompressibility of the popliteal vein in the popliteal fossa or of the femoral vein in the groin. A PE had to be confirmed by ventilation–perfusion lung scan present with a perfusion defect of at least 75% of segmental size with a normal ventilation at the spot or pulmonary angiography present with an intraluminal filling defect or a sudden cutoff of a vessel of 2.5 mm in diameter or more.
Exclusion criteria included present VTE, diastolic blood pressure higher than 100 mm Hg, systolic blood pressure higher than 200 mm Hg, concomitant heparin or LMW heparin, pretreatment and/or any concomitant medication with fibrinolytics or vitamin K antagonists, or myocardial infarction within 3 months of enrollment.
Blood Samples and Hemostatic Activation Markers
Blood specimens were collected on patients at the clinical sites on the day of randomization (baseline) prior to any medical intervention, on day 10 to 14 after the injury occurred, and on the day of the removal of the cast/brace (postbrace) approximately 5 to 6 weeks after injury. Citrated whole blood was collected, immediately prepared for platelet-poor plasma, and stored at −80°C. Directly following all clinical evaluations, plasmas of all patients were shipped frozen by overnight delivery to Loyola University. Analyses were performed during the subsequent weeks following receipt of the samples.
Quantitative determination of hemostatic activation markers was made by commercial enzyme-linked immunosorbent assays: thrombin–antithrombin complex (TAT; Enzygnost TAT Dade Behring, Marburg, Germany), tissue factor (TF) antigen (Imubind, American Diagnostica, Greenwich, Connecticut), soluble thrombomodulin (TM; Imubind, American Diagnostica), plasminogen activator inhibitor type 1 (PAI-1) antigen (Asserachrom, Diagnostica Stago, Asnieres, France), soluble P-selectin (R&D; Minneapolis, Minnesota), and TF pathway inhibitor (TFPI; Imubind, American Diagnostica). Laboratory personnel were blinded to treatment and clinical outcomes of patients. The Asserachrome HPIA kit (Stago Asnieres, France) was used to detect antibodies to the complex of platelet factor 4 and heparin (heparin-induced thrombocytopenia [HIT] antibodies). All assays were performed according to the manufacturers’ instructions with additional controls included in each run. Normal ranges for each assay were determined by the laboratory prior to evaluating the study specimens.
Statistical Analyses
The hemostatic biomarker data are depicted as interquartile ranges using box plots since the data was not normally distributed. The median is depicted as the horizontal line within the box, the 25th and 75th percentiles (interquartile range) are the lower and upper borders of the box, and the 10th and 90th percentiles are the lower and upper whiskers. Data mean values are indicated by a star. The upper limit of the normal reference range is indicated by a line across the figure.
Statistical significance was determined using the Wilcoxon signed-rank test for within-group comparisons between time points or the U test (Mann, Whitney, and Wilcoxon) for comparisons between groups, performed as a 2-tailed test. P values <.05 were considered to be statistically significant. 14 The Sigma Stat (SPSS; Chicago, Illinois) program for Windows was used for all statistical analyses.
Results
In this substudy of the Plaster Cast study, data of patients were analyzed in 2 ways. First, the data of the placebo group and the baseline data of the reviparin group were used to determine the natural history of thrombosis generation in this population. Second, the data of the reviparin group were used to validate the identified mechanism of thrombogenesis.
The patients enrolled in the Plaster Cast study were healthy and active. The median age of patients was 47 years; 52% were male. There were no significant differences in risk factors for vascular disease between the group treated with reviparin and the group treated with placebo, except for smoking (47% placebo group vs 36% reviparin group). Complete demographics are provided in the publication of the clinical trial. 13
The overall rate of venous thromboembolic events (DVT confirmed by phlebography on the day of the brace removal or PE confirmed by ventilation perfusion lung scan or pulmonary angiography) was 14.0% (18.6% in the placebo group and 9.3% in the reviparin group, Table 1). All DVTs were in the injured leg; there were 2 PEs in the placebo group. When the patients of the placebo group were subdivided by surgery or no surgery prior to immobilization and by type of injury (fracture or ATR), the patients who underwent surgery to correct lower leg trauma were found to be at the highest risk to develop thrombosis (75% vs 58% for patients who did not have surgery; 67% for either fracture or ATR; Table 2).
Incidence of Venous Thrombosis in Patients of the Plaster Cast clinical study.
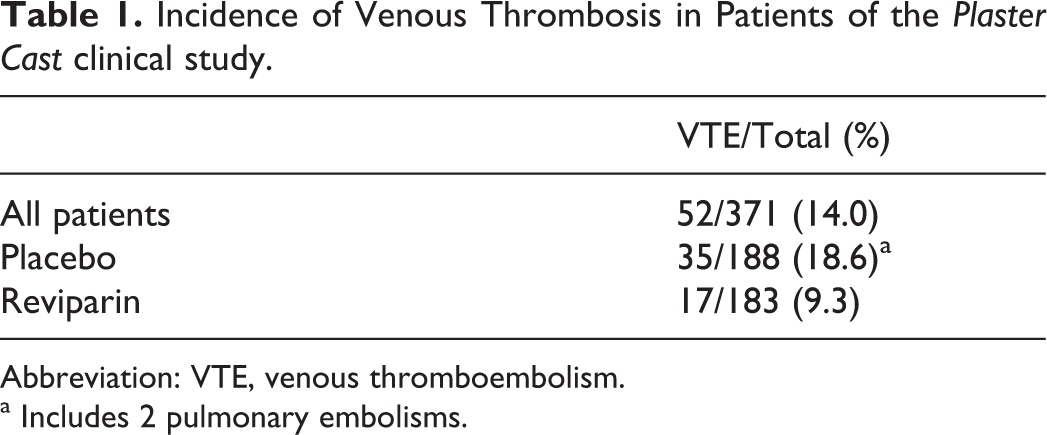
Abbreviation: VTE, venous thromboembolism.
a Includes 2 pulmonary embolisms.
Venous Thrombosis in Patients of the Plaster Cast Clinical Study Categorized by Type of Treatments and Injury.a
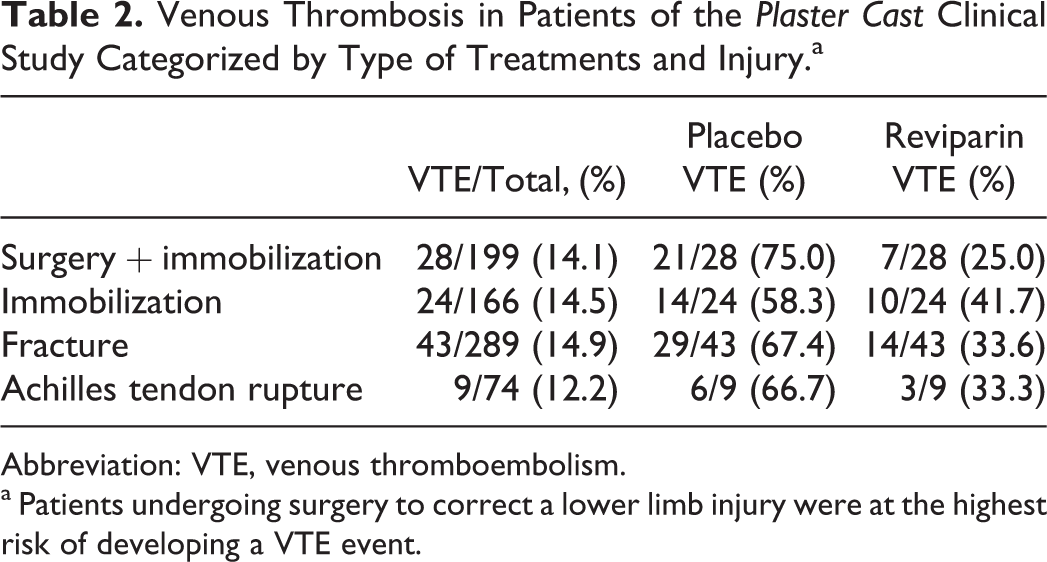
Abbreviation: VTE, venous thromboembolism.
a Patients undergoing surgery to correct a lower limb injury were at the highest risk of developing a VTE event.
Natural History of Thrombogenesis
Thrombin–antithrombin complex
Thrombin–antithrombin complex (TAT), a marker of thrombin generation, was normal (<4.0 ng/mL) at the time of injury in most patients (Figure 1 shows all placebo-treated patients [n = 183]). The median level was 1.90 ng/mL (0.96-4.31 ng/mL; interquartile range). However, the mean level was 4.06 ng/mL with a number of values higher than 10 ng/mL. Throughout the postinjury recovery period, mean and median TAT levels progressively decreased (P < .001) such that nearly all patients had TAT values <4.0 ng/mL at the time the brace was removed.
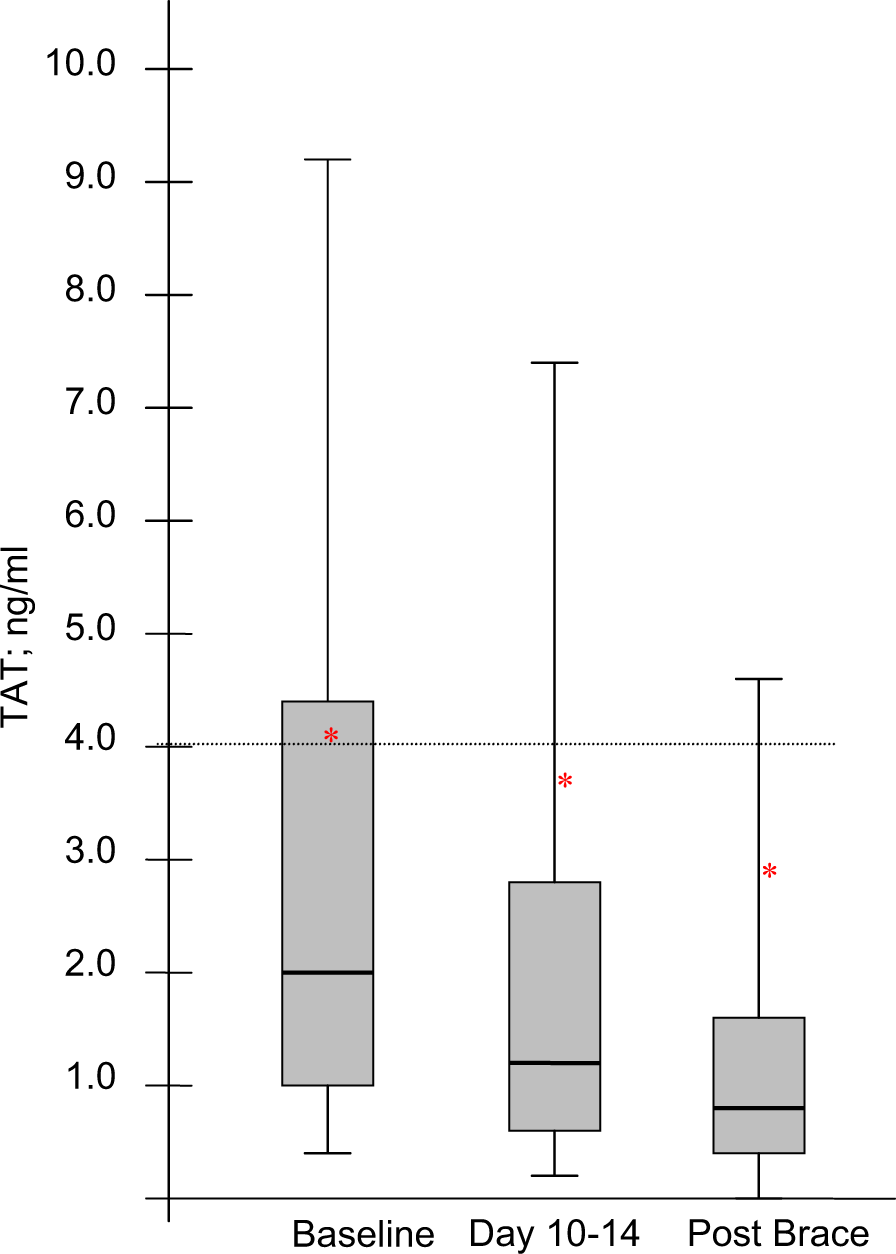
Thrombin generation in patients with leg trauma during the recovery period. The TAT levels were in the high normal range at the time of injury (n = 183 placebo-treated patients) with certain patients showing excessively high levels. Levels consistently decreased over the 5-week period in all patients (median values: P < .001 baseline vs day 10-14; P < .001 day 10-14 vs post-Brace). TAT indicates thrombin–antithrombin complex.
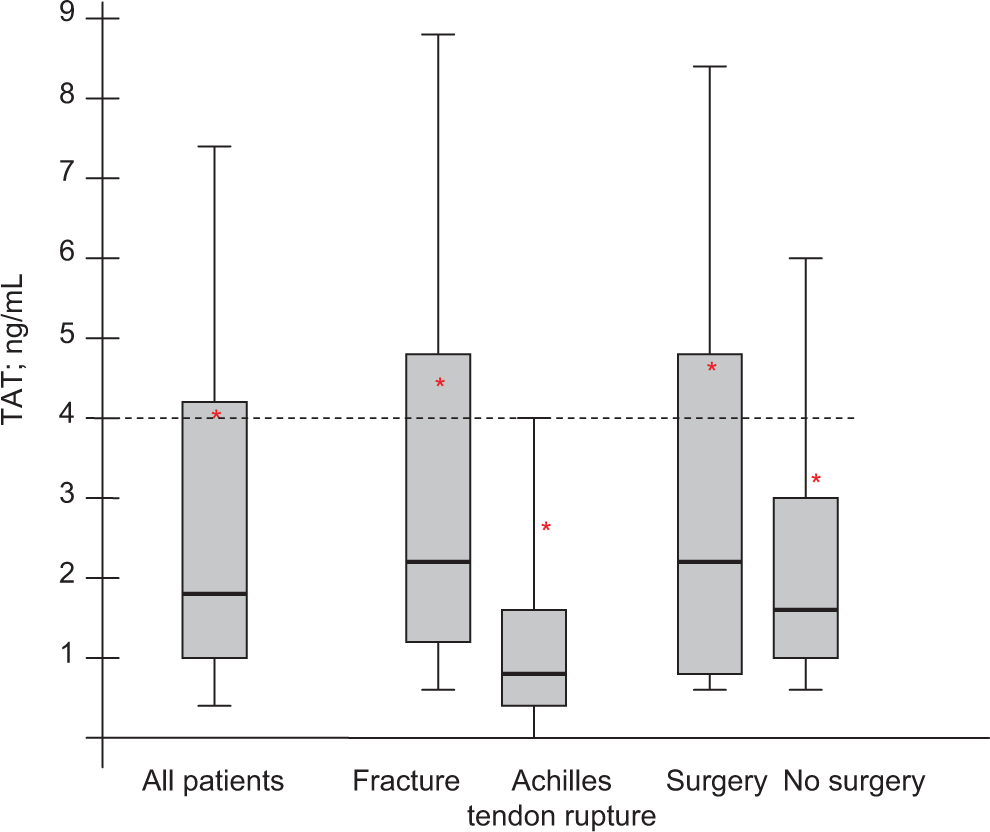
Thrombin generation in patients with leg trauma categorized by severity of injury. Although in general the patients with leg trauma (baseline samples on all patients; n = 365) had TAT levels within the normal range, patients with fracture and/or surgery had highly elevated levels. Classified by type of injury, median TAT levels were higher in the fracture group than in the ATR group (P < .001). Classified by type of treatment, TAT levels were higher in patients of the surgery group (median values: P = .113 vs conservative nonsurgical treatment). TAT indicates thrombin–antithrombin complex; ATR, Achilles tendon rupture.
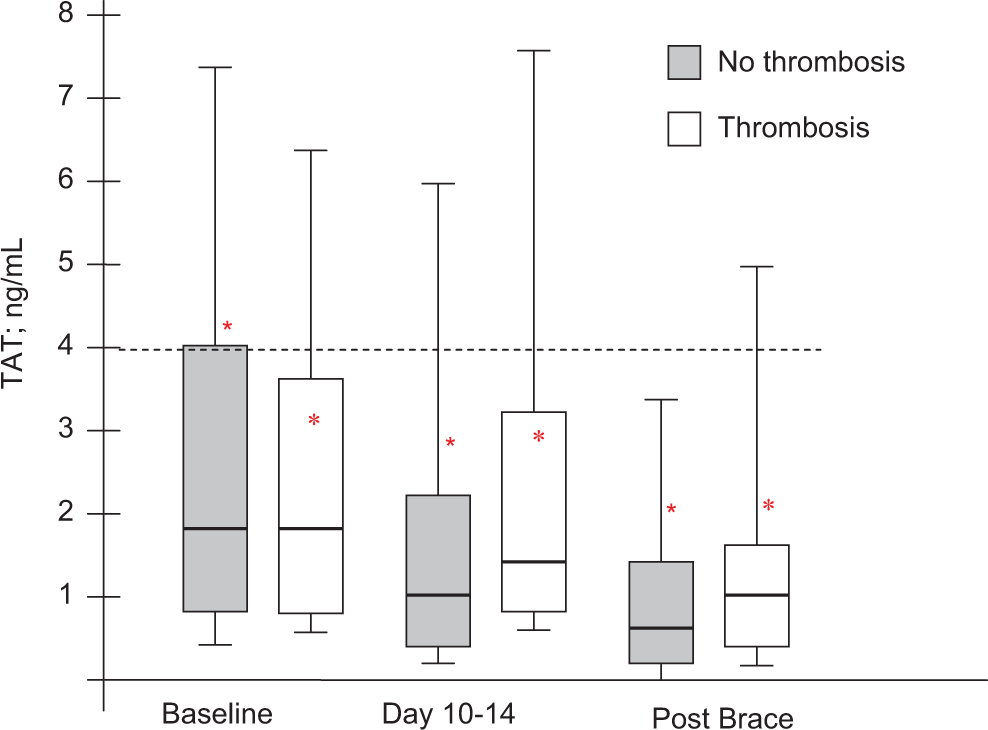
Analysis of thrombin generation in the VTE group of patients with leg trauma. Compared to the non-VTE group (n = 313), median TAT levels were higher in the VTE group (n = 52) on day 10 to 14 (P = .012) and at the postbrace time period (P = .035). VTE indicates venous thromboembolism; TAT, thrombin–antithrombin complex.
Classified by severity of injury (ie, medical condition defined by type of injury and treatment), the median TAT level at baseline was 2.09 ng/mL (n = 289; 1.23-4.68 ng/mL) in the fracture group and 0.78 ng/mL (n = 76; 0.49-1.57 ng/mL) in the ATR group (P < .001; Figure 2). Mean TAT levels were also higher in the fracture group (4.31 ng/mL) than in the ATR group (2.76 ng/mL). Some patients in the fracture group had TAT levels as high as 40, 60, and 100 ng/mL.
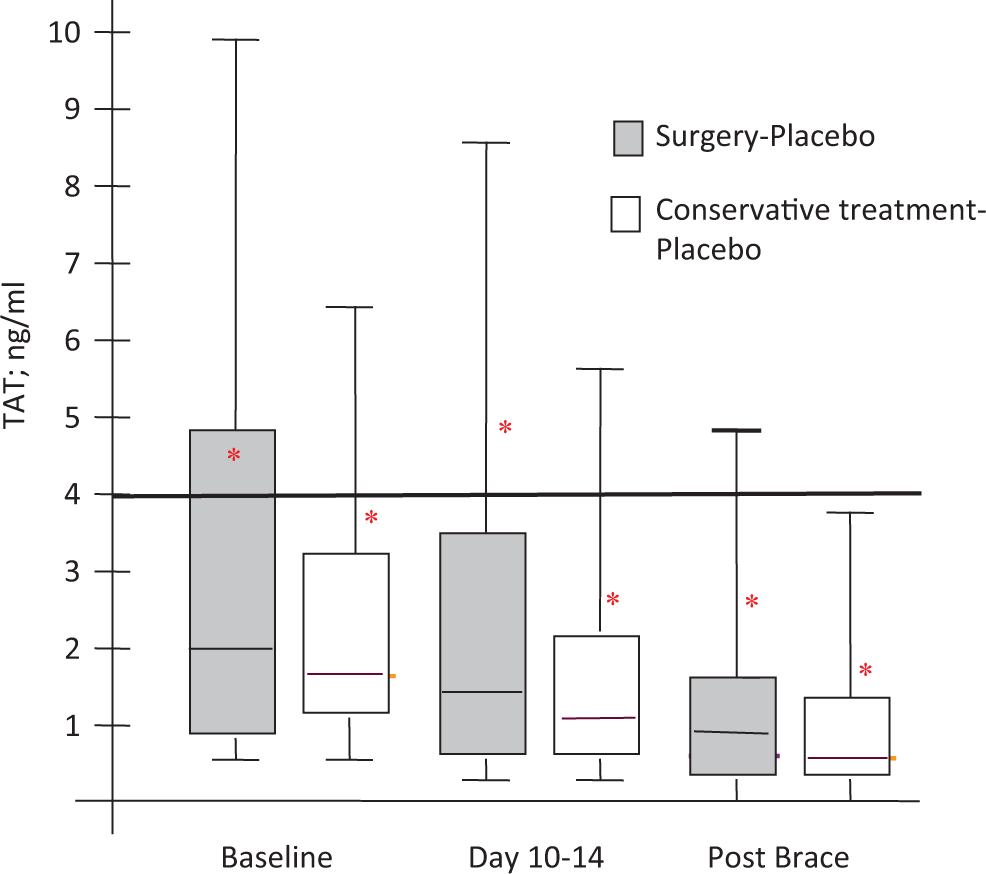
Thrombin generation in surgical and nonsurgical patients during the recovery period. Compared to the conservatively treated group (n = 82 placebo-treated patients), TAT levels were higher in the surgery group (n = 106 placebo-treated patients) at all time points. The difference between groups was consistent and unchanged throughout the recovery period but did not reach significance. TAT indicates thrombin–antithrombin complex; VTE, venous thromboembolism.
Patients who underwent surgery prior to immobilization (n = 199) had a higher TAT mean value level than patients who did not underwent surgery (n = 166), 4.62 ng/mL (median 2.05 ng/mL; 0.86-4.78 ng/mL) compared to 3.30 ng/mL (median 1.59 ng/mL; 0.95-3.11 ng/mL; Figure 2). The highest TAT values in the entire study population were found in the surgical patients with VTE. Because of a wide range of values, the difference between these 2 groups was not significant (P = .113).
The levels of TAT were not significantly different at baseline for the VTE group (n = 52) and non-VTE group (n = 313; Figure 3). The TAT levels reduced over time for patients who did not experience a thrombotic event. The median TAT level in the non-VTE group was 1.84 ng/mL (0.91-4.10 ng/mL) at the time of injury, 1.02 ng/mL (0.46-2.19 ng/mL) at day 10 to 14, and 0.69 ng/mL (0.25-1.49 ng/mL) at the time the brace was removed, representing a significant change from time point to time point (P < .001). In contrast, TAT levels in patients with VTE remained elevated at day 10 to 14 and only trended toward normal at time of brace removal. Patients with VTE had a significantly higher median TAT level on day 10 to 14 (1.44 ng/mL; 0.91-3.16 ng/mL; P = .012) and at the time the brace was removed (0.98 ng/mL; 0.49-1.60 ng/mL; P = .035) compared to the non-VTE group.
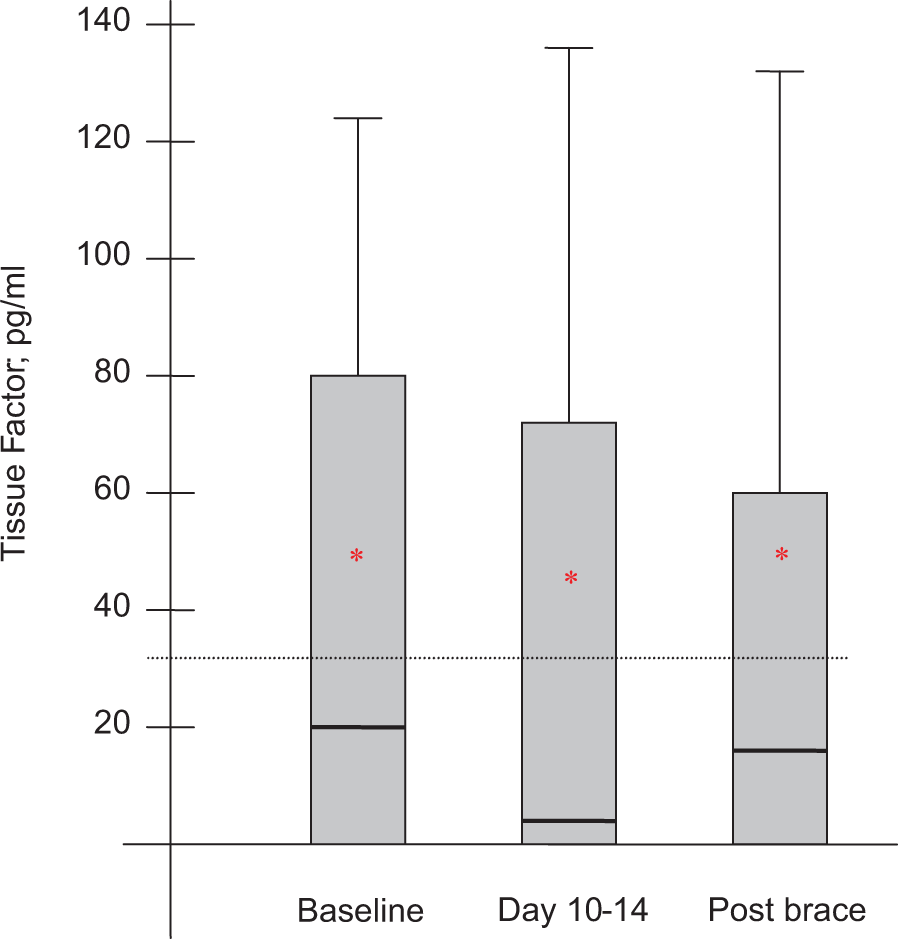
Tissue factor in patients with leg trauma during the recovery period. The median TF level was not elevated at the time of injury (n = 183 placebo-treated patients); however, multiple patients had levels above the upper limit of normal. Certain patients had excessively high levels of >100 pg/mL. The median TF level did not significantly change over time. TF indicates tissue factor.
As shown in Table 2, the surgical patients experienced the highest rate of VTE. In the placebo arm of the study, mean and median TAT levels were consistently higher in the surgery group (n = 106) than in the nonsurgery group (n = 82) throughout the recovery period (P = .012; Figure 4). The highest TAT levels were found in the subgroup of surgically treated patients with VTE on day 10 to 14. The TAT levels reduced over time in both the groups. However, the difference between the surgically and nonsurgically treated groups at each time point did not reach significance due to the range of TAT values within each group.
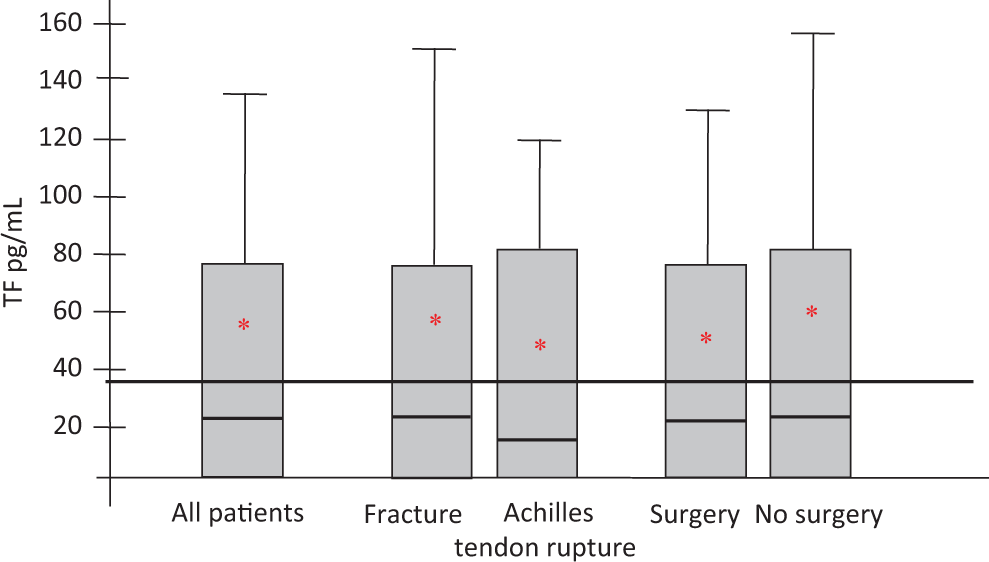
Tissue factor in patients with leg trauma categorized by severity of injury. Many, but not all, patients with leg trauma (baseline samples on all patients) had elevated TF levels at the time of injury. Classified by type of injury, TF levels were higher in the fracture group than in the ATR group. Classified by type of treatment, TF levels tended to be higher in the nonsurgery group. TF indicates tissue factor; ATR, Achilles tendon rupture.
Tissue factor
Tissue factor (TF), an important activator of thrombin generation, was not elevated above normal (<35 pg/mL) at the time of injury in most patients as shown by median values (Figure 5). However, numerous patients had values higher than 90 pg/mL pushing the mean over the normal limit to 51.0 pg/mL, with excessively high TF levels in multiple patients as high as 200 and >500 pg/mL. The extremely high TF levels kept the mean consistent and over the normal range throughout the study period. Nonsignificant fluctuations in the median were noted from baseline to day 10 to 14 to postbrace time.
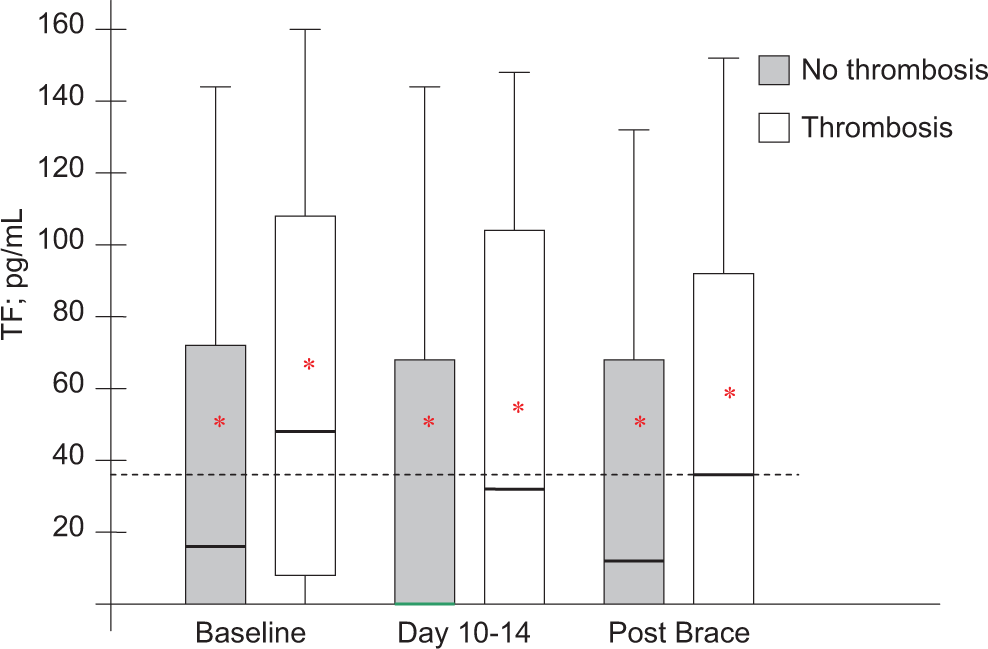
Tissue factor in the VTE group of patients with leg trauma. Compared to the non-VTE group (n = 313), median TF levels were higher in the VTE group (n = 52) at baseline (P = .003) and continued to remain higher through day 10 to 14 and at the postbrace time period. TF indicates tissue factor; VTE, venous thromboembolism.
Classified by severity of injury (ie, medical condition defined by type of injury and treatment), the TF levels were nonsignificantly higher in the fracture group (mean 55.14 pg/mL and median 22.30 pg/mL with an interquartile range of 0-75.68 pg/mL; n = 289) than in the ATR group (mean 46.36 pg/mL and median 13.81 pg/mL with an interquartile range of 0-83.25 pg/mL; n = 76) at baseline (Figure 6). Patients who underwent surgery prior to immobilization had a lower TF mean level (49.44 pg/mL) than patients who did not have surgery (58.10 pg/mL) but a similar median level. Because of a wide range of values, differences among all groups were not significant.
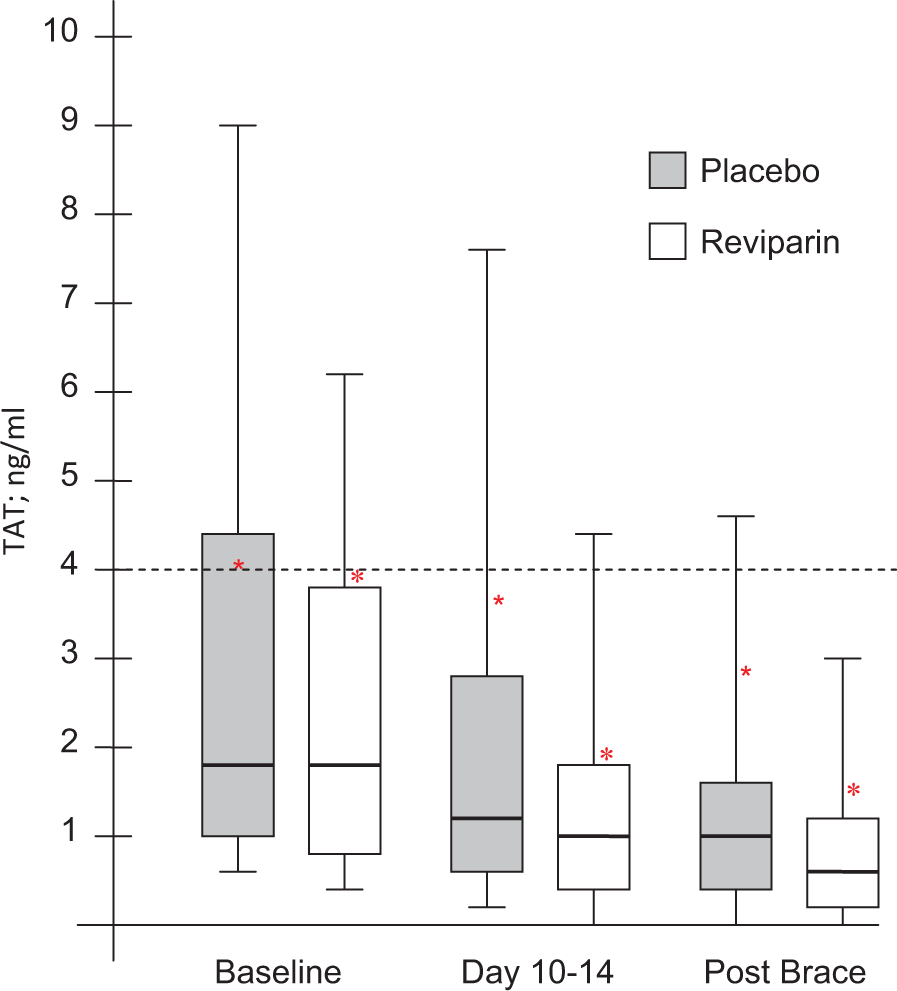
Thrombin generation in patients with leg trauma undergoing reviparin treatment. TAT levels were rapidly normalized in nearly all patients treated with the LMW heparin reviparin (P < .001 vs baseline; n = 182). Compared to placebo treatment (n = 183), reviparin treatment was associated with lower TAT levels at day 10 to 14 (P = 0.16) and at the postbrace time (P = .020). TAT indicates thrombin–antithrombin complex; LMW, low-molecular weight.
Classified by VTE (n = 52) or none (n = 313), the patients who developed VTE had TF values higher than the normal limit (mean 68.73 pg/mL; median 49.05 pg/mL with an interquartile range of 6.47-109.54 pg/mL) and far higher than the group that did not have VTE (mean 50.83 pg/mL; median 14.86 pg/mL with an interquartile range of 0-73.19 pg/mL) at baseline (Figure 7; P = .003). The highest TF levels were found in patients with fractures who developed VTE. The higher TF levels in the group of patients with VTE held throughout the study period. The TF levels in both the groups did not significantly decline over time.
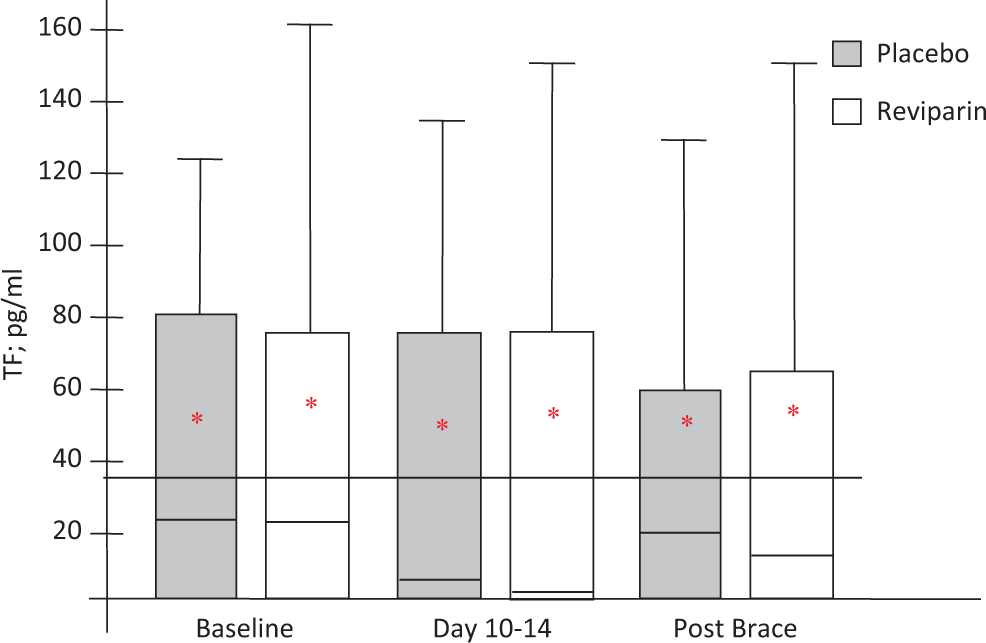
Tissue factor in patients with leg trauma undergoing reviparin treatment. TF levels remained elevated in many patients throughout the study period regardless of treatment with the LMW heparin reviparin or placebo. Compared to placebo treatment (n = 183), reviparin treatment (n = 182) was associated only with slightly lower TF levels at day 10 to 14 and at the postbrace time (not significant). TF indicates tissue factor; LMW, low-molecular weight.
Other biomarkers
The median PAI-1 level was within the normal range (<45 ng/mL) at the time of injury. The median PAI-1 level was slightly increased at day 10 to 14 (P < .001 vs baseline; n = 162) and at the postbrace time. By subgroup analysis, patients with VTE had higher PAI-1 levels (P = .01). The PAI-1 levels in the VTE group at baseline ranged from 7.2 to 197.1 ng/mL (n = 52) with a mean level of 43.8 ng/mL (median 33.9 ng/mL; 22.53-58.45 ng/mL interquartile range). At day 10 to 14, PAI-1 levels in the VTE group increased to a mean of 49.0 ng/mL (median 43.9 ng/mL; 24.15-58.40 ng/mL interquartile range). At the postbrace time period, the mean PAI-1 level was 47.0 ng/mL (median 40.5 ng/mL; 25.10-54.60 ng/mL interquartile range) in the VTE group.
Soluble thrombomodulin levels were not elevated above the upper limit of normal at baseline in any patient, and levels remained steady throughout the study period for all subgroups.
Soluble P-selectin levels were elevated above the upper limit of normal (>40 ng/mL) for all patients at baseline with an increase at day 10 to 14 that sustained through the postbrace period. For patients with VTE (n = 52), the baseline mean level was 76.8 ± 21.3 ng/mL (standard deviation), the day 10 to 14 mean level was 99.3 ± 48.7 ng/mL, and the postbrace mean level was 86.5 ± 26.8 ng/mL. In comparison, a control group that consisted of randomly selected non-VTE patients (n = 51) had a baseline mean level of 79.0 ± 41.6 ng/mL, a day 10 to 14 mean level of 82.7 ± 26.7 ng/mL, and a postbrace mean level of 84.9 ± 45.8 ng/mL. The increase that occurred at day 10 to 14 was not significant but was more evident in the VTE group.
The HIT antibodies were detected in 6.6% of the total Plaster Cast study population, considering positivity at any time point of the study. The HIT antibody positivity was not significantly more frequent in the reviparin-treated group (n = 12) than in the placebo-treated group (n = 12). Of further interest, only 2 (8.3%) of 24 HIT antibody-positive patients, confirmed positive for HIT by a platelet function test ( 14 C-SRA), developed VTE (0.5% of the total population), and both were placebo-treated patients.
Validation of Thrombogenesis Mechanism
Thrombin–antithrombin complex
Thrombin–antithrombin complex levels in reviparin-treated patients (n = 182) demonstrated an accelerated decrease from baseline to day 10 to 14 and remained low at the postbrace time (P < .001; Figure 8). Reviparin treatment normalized the TAT levels in nearly all patients from day 10 to 14 onward. For the reviparin-treated group at day 10 to 14, the median TAT level was 0.97 ng/mL (0.45-1.89 ng/mL) with a mean level of 1.96 ng/mL, and at the postbrace time point, the median TAT level was 0.59 ng/mL (0.22-1.36 ng/mL) with a mean level of 1.51 ng/mL. Levels were markedly lower in the reviparin-treated group than in the placebo-treated group where median/mean levels never reached levels as low as those in the reviparin group. The median TAT level in the placebo-treated group (n = 183) at day 10 to 14 was 1.24 ng/mL (0.56-2.90 ng/mL) with a mean of 3.55 ng/mL (P = .016 vs reviparin group). At the postbrace time, the median TAT was 0.89 ng/mL (0.40-1.64 ng/mL) with a mean of 2.80 ng/mL (P = .020 vs reviparin group).
These data are consistent with the decrease in VTE observed in the reviparin-treated patients compared to placebo-treated patients (Tables 1 and 2), being particularly obvious in the patients who underwent surgery (Table 2).
Tissue factor
Compared to the placebo-treated group, median TF levels were slightly lower in the reviparin-treated group throughout the treatment period but without statistical significance (Figure 9). The TF levels decreased but not significantly throughout the study period in both the reviparin- and placebo-treated groups. Levels remained higher than normal in many patients throughout the study period. Mean levels did not differ between reviparin- and placebo-treated groups.
Other biomarkers
Reviparin treatment was associated with an increase in TFPI level (P < .001). From an average TFPI level of 72 ng/mL in the placebo-treated patients throughout the study period, the reviparin-treated patient group had higher mean TFPI levels of 85 ng/mL on day 10 to 14 and 87 ng/mL at the postbrace time. PAI-1, soluble thrombomodulin, and soluble P-selectin levels were unaffected by reviparin treatment.
Discussion
Trauma and immobilization are independent risk factors for developing VTE. Even the simple trauma of isolated lower limb fractures or Achilles tendon injury where patients have functional immobility has a moderate risk of VTE. 10 Although most patients are at low risk of DVT/PE, these adverse events do occur. A 2007 clinical study not only confirmed past findings showing a 29% DVT prevalence in 49 patients with Achilles tendon injury treated surgically and a 39% DVT prevalence with 3 PEs in 46 patients treated nonoperatively but also was used to develop a scoring system to evaluate outcomes after treatment. 15 Experts continue to determine optimal treatment regimens 16 in an effort to promote universal practice.
In the Plaster Cast clinical study, there was an overall 14% rate of VTE in otherwise healthy individuals who had lower leg injuries medically treated with plaster cast/brace immobilization. The VTE was determined to be associated with a hypercoagulable state characterized by a burst of TF release that sustained over the weeks of the immobilization period. Our findings in these patients with minor trauma were first reported in 2003 and 17 –19 were similar to the findings in a study of patients with major trauma published that same year. 20 Tissue factor is present in cellular membrane, and upon tissue damage/activation its circulating levels are increased. It is one of the major mediators of coagulation system activation resulting in thrombin formation and fibrinogen conversion to fibrin. Although tissue factor levels were within the normal range for most patients, some patients had significantly elevated levels with a few having levels similar to those found in patients undergoing hip replacement surgery. 21
The induced hypercoagulable state in the Plaster Cast study patients was clearly defined by increased thrombin generation. The serine protease thrombin, once formed, complexes with the endogenous serine protease inhibitor antithrombin. The formed thrombin–antithrombin complex circulates in blood of patients who sustain thrombotic disorders. In our study, thrombin generation was greater with fracture than soft-tissue injuries and greater with surgery than with conservative treatment (ie, no surgery).
Of the biomarkers evaluated, tissue factor was determined to be the primary inducer of the hypercoagulable state in the Plaster Cast patient population. Tissue factor is found in endothelium, leukocytes, and activated platelets. 22 The PAI-1, found in endothelial cells and platelets, was slightly increased suggesting a potential fibrinolytic deficit that would add to the hypercoagulable state. Thrombomodulin, a surface receptor on endothelial cells, was not different from normal in any subgroup analysis comparing absolute levels between groups or between group changes from time point to time point. P-selectin, found in platelets and endothelial cells, was only slightly elevated. The findings on TF, PAI-1, and P-selectin suggest that in the Plaster Cast patients, there was some degree of vascular damage and platelet activation. Vascular damage per se may be downplayed due to the lack of thrombomodulin release. However, an upregulation of inflammation causing TF release from leukocytes cross-talking with activated platelets may be an important underlying mechanism that contributes to thrombin generation (TAT). Thrombin generation (from the injury) along with reduced fibrinolytic activation (from stasis due to edema causing venous compression and plaster cast/brace immobilization) provides the basis for thrombotic risk in patients with minor lower limb injuries.
Long-term thromboprophylaxis with the LMW heparin reviparin greatly reduced thrombin generation (TAT). This was observed to the greatest extent within the first 2 weeks of reviparin treatment. Interestingly, LMW heparin treatment was not associated with a decrease in TF levels. Subgroup analysis showed that patients undergoing surgery to correct lower leg trauma, who receive no long-term thromboprophylaxis, are at highest risk to develop VTE. Long-term prophylaxis with LMW heparin benefitted patients in general regardless of type of injury or type of medical treatment. However, patients undergoing orthopedic surgery to correct their trauma benefited most from thromboprophylaxis. As the antithrombotic mechanism of LMW heparin is inhibition of FXa (with a component of thrombin inhibition), it would be of interest to consider a potential anticoagulant role for the new oral drugs that inhibit FXa, such as apixaban, edoxaban, and rivaroxaban, for thrombosis prophylaxis in patients with functional immobilization. In addition, inhibition of platelet activation and inflammation may also prove beneficial.
After prolonged treatment for 5 to 6 weeks, only 2 cases of VTE in patients with functional HIT antibodies occurred (<1.0% of the study population). Both cases were in placebo-treated patients. Antibody development may have been related to exposure to LMW heparin enoxaparin prior to enrollment in the study. Thus HIT was not an essential cause of VTE in this patient population.
In addition to exposure to LMW heparin prior to enrollment in the study (determined not to be a confounding factor in the final analysis of the clinical trial data 13 ), there were several other limitations of this study. Baseline samples were collected on the day of study randomization not on the day of trauma. Other blood sample collection did not coincide with day of surgery or initiation of the thrombotic event. Individual data on trauma severity score were not collected. The size of the subgroups is small, and the variation in the results is relatively high. The data in Figures 3 and 7 include a mixed population of reviparin- and placebo-treated patients. The delay between conducting the study and final publication was only due to time constraints placed on the authors; however, the data was publicly released in a timely manner 17–19 .
This study, strengthened by the inclusion of a placebo group, confirms that otherwise healthy individuals who incur lower leg injuries and plaster cast/brace immobilization are at risk of developing VTE, which is due to a sustained release of TF and possibly a fibrinolytic deficit leading to thrombin generation. The hypercoagulable state is greater with fractures than soft-tissue injuries and greater with surgery than conservative treatment. Treatment with LMW heparin during the immobilization phase is effective in reducing thrombin generation to a normal state, restoring the hemostatic balance. The mechanisms of VTE identified by this study support the inclusion of medical conditions relevant to lower limb injury in thrombosis risk scoring systems 23 and support the recommendation for thromboprophylaxis with LMW heparin in this patient population in consensus statements. 10
Footnotes
Acknowledgment
Studies were supported by internal funding through Loyola University Chicago and no commercial funding was used.
Authors’ Note
The investigations reported herein were conducted in partial fulfillment of the dissertation for the medical doctoral degree of Ms Phoebe Kaiser through the University of Heidelberg.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.