
Abstract
Objective:
To investigate the utility of an electronic version of the condensed molecular and clinical markers for the diagnosis and management of type 1 von Willebrand disease (VWD) bleeding questionnaire (eBQ) in assessing the bleeding phenotype in platelet-type VWD (PT-VWD) and compare it to its closely similar disorder, type 2B VWD.
Methods:
Retrospective analysis of the clinical bleeding and laboratory phenotype of 13 patients with PT-VWD and 12 type 2B VWD.
Results:
Bleeding score (BS) was significantly lower in PT-VWD as compared to type 2B. Bleeding score correlated with platelet count and von Willebrand factor:Ristocetin cofactor activity in PT-VWD but not in type 2B with a significant reduction in platelet count in type 2B VWD compared to PT-VWD. The eBQ had sensitivity of 62% in PT-VWD and 92% in type 2B VWD.
Conclusion:
Objective analysis of bleeding symptoms further the understanding of the phenotype of 2 closely similar bleeding disorders for better diagnosis and follow-up. Larger international prospective studies are warranted to evaluate the utility of the eBQ in PT-VWD and other rare bleeding disorders.
Introduction
The interaction between von Willebrand factor (VWF) protein and its receptor on the platelet, glycoprotein 1bα (GPIbα), is a cornerstone in understanding basic hemostasis. Conformational changes induced by shear stress, in vitro stimuli, or gain-of-function mutations in either the receptor or the ligand increase the platelet–VWF binding affinity and counter-intuitively results in bleeding disorders. Type 2B von Willebrand disease (VWD) and platelet-type VWD (PT-VWD) are known as nonidentical twins representing bleeding disorders with often similar laboratory data and clinical symptoms. 1,2 They share a common characteristic, which is an increased binding of VWF to GPIbα. This heightened responsiveness takes place in vivo without endothelial injury or shear stress induction and typically results in some loss of the hemostatically most active (high molecular weight [HMW]) VWF multimers and usually leads to some clearance of platelets and thus some (usually mild) thrombocytopenia. The loss of VWF and platelets lead to a bleeding diathesis, which might be variable among affected individuals. Although this remains the consensus as to why and how these patients bleed, recent evidence exists that platelets of patients with PT-VWD are poorly activated themselves in response to thrombin 3 and that platelets from some patients with type 2B VWD are also dysfunctional, 4 which can reflect on laboratory data and raise further questions about the phenotype.
The heightened interaction between VWF and GPIbα can also be observed in vitro, using tests of platelet function, where platelet aggregation may occur spontaneously, or in response to low concentrations of ristocetin. This remains the initial test that alerts to the diagnosis of these diseases. 5
In type 2B VWD, it is the VWF gene that is dysfunctional as a result of a gain-of-function mutation, leading to an enhanced binding to normal platelets or at least this is what is typically known about the disease. Over 26 mutations have been documented within the A1 domain of the VWF gene (GPIbα binding region—Val 1212-Lys1491) represented in exon 28 of the VWF gene (http://vwf.group.shef.ac.uk). Several reports on type 2B VWD pose challenging questions regarding the phenotype–genotype correlation affecting the diagnostic certainty or uncertainty of individual cases. 6 While it is established that VWF is the defective element in type 2B VWD cases, much attention has recently been given to the other side of the interaction, namely the platelet, where count, size, structure, and the ultrastructure of these hemostatic fragments together with megakaryopoiesis have also been investigated. 7 –9
Platelet-type VWD is a rare platelet function defect resulting from excessive binding of functionally defective (hyperactive) platelet GPIbα to a normal VWF protein. Platelet-type VWD is a missed diagnosis in 15% of type 2B VWD, and the disease remains underreported. 10 Compared to type 2B VWD, much less information is available about the clinical and laboratory features of PT-VWD, and most of the information available is based on small case series or sometimes even single case reports. Accordingly, definitive information about the severity of presenting bleeding symptoms and the hemostatic support required during times of hemostatic challenge such as pregnancy and childbirth is still limited. 11,12 This is a barrier to the appropriate management of these patients. Six mutations are known so far, to cause hyperresponsive platelet GPIbα; all with the exception of a 27-bp deletion are single point mutations located within a short amino acid stretch (246-255; 230-239 in the old nomenclature) representing the VWF-binding region on the platelet (www.pt-vwd.org/).
Quantitation of bleeding symptoms using a standardized bleeding questionnaire that produces a valid bleeding score (BS) has proven to be useful as objective tools in the diagnosis of bleeding disorders. 13 –15 In the past years, many forms of bleeding assessment tools (BAT) were developed. These tools aimed to standardize the assessment of bleeding symptoms to determine patients who require further investigations and to allow the appropriate comparisons between patients. The evolution and validation of these tools have recently been reviewed. 16
So far, there have been no systematic studies to evaluate the bleeding phenotype in PT-VWD in comparison to its twin type 2B VWD using bleeding questionnaire. This study aimed to systematically and objectively analyze the clinical bleeding and laboratory phenotype of these 2 similar disorders and to investigate the utility of an electronic bleeding questionnaire (eBQ) in this assessment.
Materials and Methods
Patients’ Data Collection
The study received ethics approval in accordance with Queens University Ethics Research Board. A call for participation in the study was made available on International Society on Thrombosis and Haemostasis (ISTH) website, and individual participation was also invited via e-mails sent to physicians and potential collaborators. Each participating center obtained ethics approval and patients’ consents according to their institution’s guidelines. Each physician was provided with a unique ID and passcode to fill in the online eBQ (http://pt-vwd.org/ebq/) for assessment of the bleeding phenotype either as a part of the patient’s regular follow-up or patients’ chart review or recorded information. The study investigated a total of 25 previously diagnosed cases: 13 PT-VWD and 12 type 2B VWD. Diagnosis of PT-VWD and type 2B VWD was based on low VWF:Ag, VWF:Ristocetin cofactor (RCo), and VWF RCo:Ag ratio, enhanced ristocetin-induced platelet aggregation (RIPA), and loss of HMW VWF multimers in plasma, and their differentiation was based on DNA analysis of each of the A1 domain coding region of the VWF gene as well as the platelet GP1BA gene. Laboratory data were extracted from patients’ chart review or recorded information within the same time frame of assessment of the clinical symptoms. All cases were molecularly diagnosed, and mutations were identified and recorded. Sixteen healthy volunteers with no personal or family history of bleeding conditions with no medications that interfere with hemostasis were included in this study as a comparative group.
Electronic Bleeding Questionnaire
An electronic version 17 of the condensed molecular and clinical markers for the diagnosis and management of type 1 VWD (MCMDM-1VWD) questionnaire 18 was developed as a web application using the PHP scripting language and MySQL relational database platform. Security was ensured by using password protection, database encryption, and encrypted transfer protocols. Electronic questionnaire responses collected via the application were validated to ensure congruency with the MCMDM-1VWD scoring key and thus maintain the same specificity and sensitivity as the original questionnaire. Internal validation and archiving of data at the point of entry eliminated transcription/interpretation error and allowed automatic computation of the BS upon completion of the questionnaire. A physician or trained personnel conducted the interview/entered responses in the eBQ. The eBQ link can be accessed at http://pt-vwd.org/ebq/. The following is a trial ID and pass code, the reader can use as a representation ID: CUVC7Y, pass code: 1e5ca8d1a64936b.
Statistical Analysis
Analyses were performed using GraphPad Prism Software 6 for Windows (GraphPad Software). The comparative analysis of the BS, platelet counts, and VWF levels between type 2B VWD and PT-VWD was performed using student t test. Assessment of dispersion of BS data was performed using variance (V; the average of the squared differences from the mean). Correlations were calculated using Pearson correlation coefficient. P values less than .05 were considered significant. Sensitivity and specificity were calculated on the basis of the disease diagnosis of the patients and the ability of the eBQ to identify the disease status compared with controls.
Results
Patients and BSs
A total of 25 patients and 16 healthy controls were analyzed using the eBQ. Bleeding scores are expressed in whole numbers. A BS of ≥4 was considered abnormal for adult analyses. 19
A total of 13 patients with PT-VWD were analyzed (average age 37.6 years [range: 4-67]; 2 males and 11 females) from 8 countries representing 6 different mutations: Gly249Ser (5 patients; 4 were blood relations—granddaughter and grandfather; mother and daughter), 20,21 Gly249Val (2 patients), 22,23 Met255Val (2 patients), 24,25 Asp251Tyr (2 patients; father and daughter), 26 436 to 444 del 9 (1 patient), 27 and the recently reported Trp246Leu (1 patient). 28 The BSs were variable (median = 4, range: 0-17), with 5 patients with BS <4 and 8 with BS ≥4 (Table 1).
Characteristics of the Bleeding Phenotype in All Investigated Patients Based on the eBQ.a
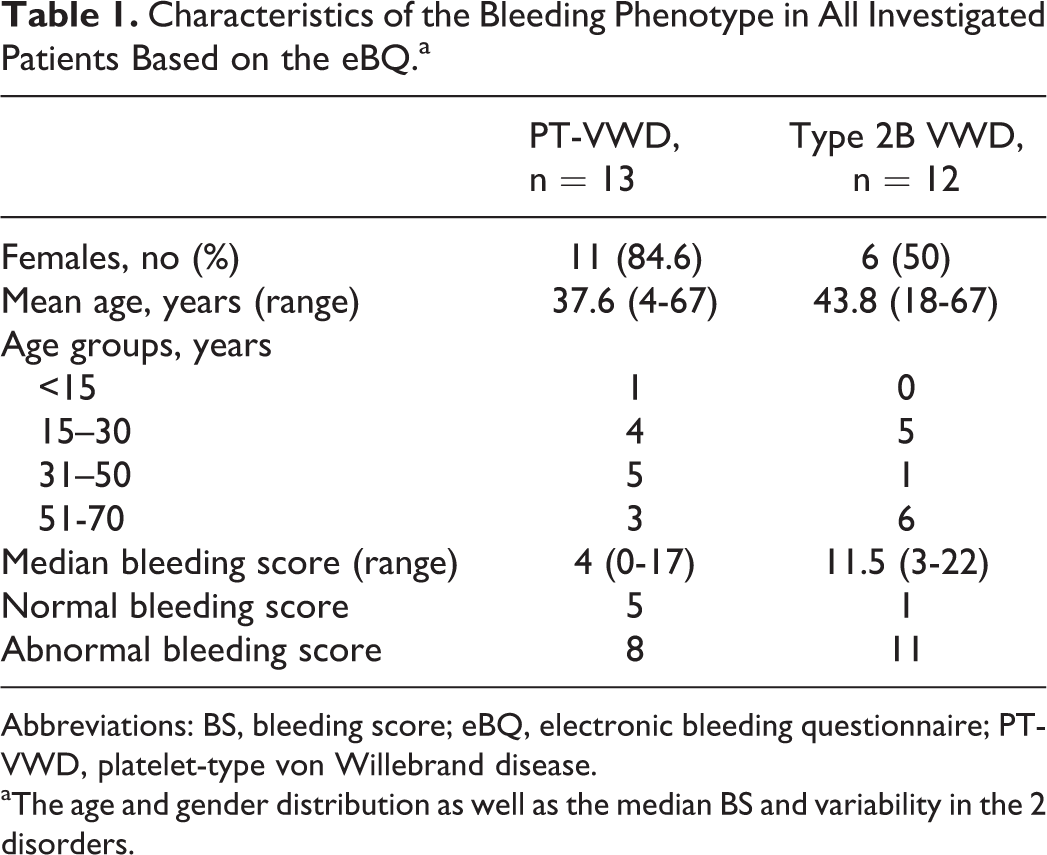
Abbreviations: BS, bleeding score; eBQ, electronic bleeding questionnaire; PT-VWD, platelet-type von Willebrand disease.
aThe age and gender distribution as well as the median BS and variability in the 2 disorders.
A total of 12 patients with type 2B VWD were analyzed (9 from Canada and 3 from Brazil; 6 females and 7 males; average age = 43.8 years, range: 18-67) representing 4 different mutations: Arg1341Gln (4 patients), His1268Asn (1 patient), Val1316Met (5 patients), and Arg1306Trp (2 patients). Only 1 patient had BS <4, and all other patients had BS ≥4. The BSs were variable (median = 11.5, range: 3-22).
The eBQ was also evaluated in 16 normal controls, average age 27 years (range = 4-44; 11 females and 5 males). All these individuals had BS <4 (median = 0, range: -2 to 2).
In general, BS was variable in both disorders (PT-VWD variance = 32 and type 2B VWD variance = 30). Variability was seen in patients with similar mutations and appeared independent of patient age. There was no significant correlation between BS and age or gender in both the patient groups (r = -.224; P = .15 and r = -.133; P = .41, respectively). The BS was significantly higher in patients with type 2B VWD compared to that of PT-VWD (P < .05; Figure 1).
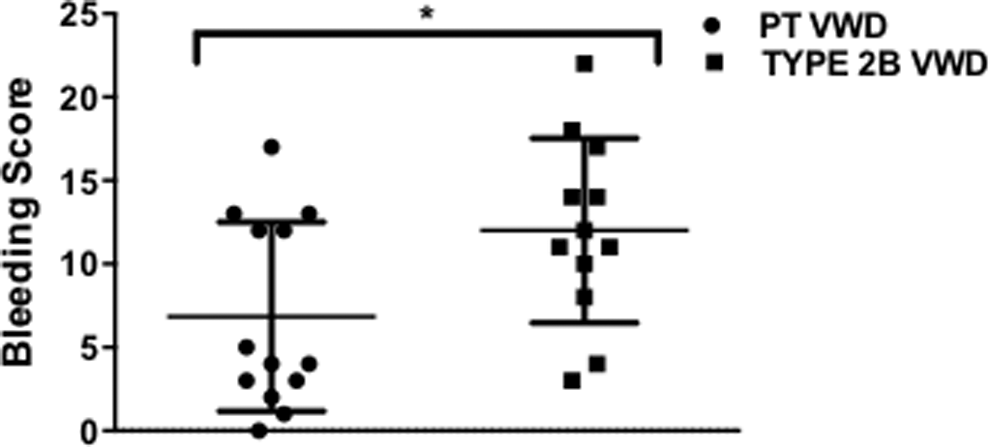
Comparative analysis of bleeding score. The BS of the patients is shown in a scattergram with the horizontal line indicating the median for each group. There was a significant increase in BS of type 2B VWD in comparison with PT-VWD (*P < .05). BS indicates bleeding score; PT-VWD, platelet-type von Willebrand disease.
Comparative Phenotypic Analysis Between PT-VWD and Type 2B VWD
As shown in Table 2, platelet count was found to be significantly lower in patients with type 2B VWD compared to PT-VWD (P < .05). In terms of the VWF data, there was a trend toward significant reduction in VWF:Ag (P = .12) in type 2B VWD compared to PT-VWD and a significant reduction in VWF:RCo/VWF:Ag ratio (P = .08) in PT-VWD compared to type 2B VWD. The RIPA was enhanced in all the PT-VWD cases, and HMW VWF multimers were either decreased, absent, or abnormal. As shown in Figure 2, in PT-VWD, there was a significant correlation between the BS and platelet count (r = -.558; P < .05) and the VWF:RCo (r = -.607; P < .05). There was also a trend toward significance in the correlation between BS and VWF:Ag (r = -.517; P = .07) and between BS and VWF:RCo/VWF:Ag (r = -.503; P = .08). However, there was no correlation between BS and any of the laboratory data in type 2B VWD. With respect to platelet size, the mean platelet volume (MPV) in PT-VWD was 12.16 ± 0.55 with macrothrombocytopenia observed in 100% of patients. In type 2B VWD, the MPV was 11.16 ± 1.97 with only 58.3% showing macrothrombocytopenia. Spontaneous platelet aggregates were reported in a similar percentage (˜70%) of patients with both disorders.
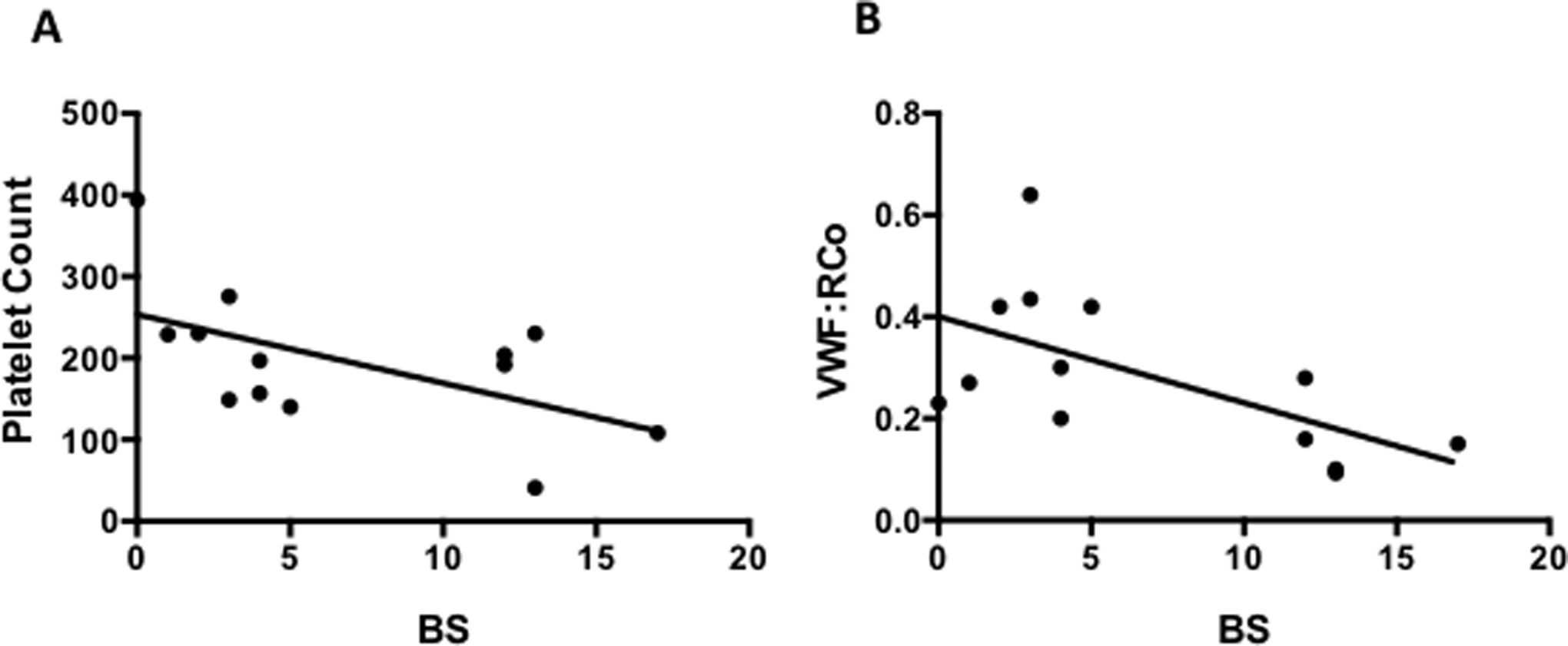
Correlation between BS and laboratory parameters in PT-VWD. The correlation between BS and platelet count (A) and BS and VWF:RCo (B) is shown in a scattergram with the horizontal line indicating the linear regression. There was a significant negative correlation in the 2 groups (*P < .05). BS indicates bleeding score; PT-VWD, platelet-type von Willebrand disease.
Comparison of the Laboratory Data for PT-VWD and Type 2B VWD.a
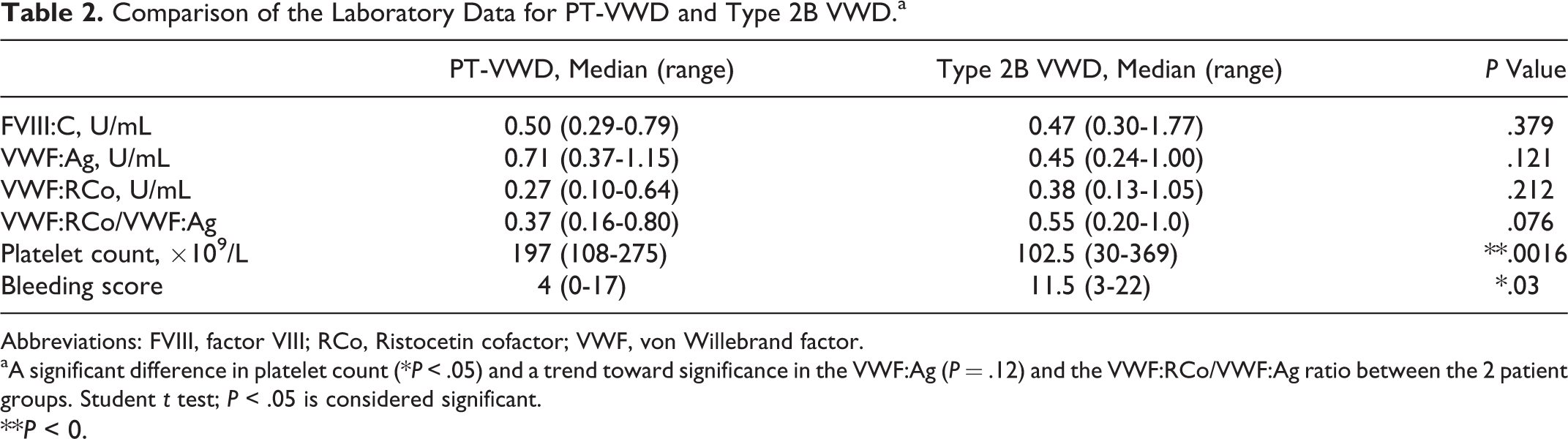
Abbreviations: FVIII, factor VIII; RCo, Ristocetin cofactor; VWF, von Willebrand factor.
aA significant difference in platelet count (*P < .05) and a trend toward significance in the VWF:Ag (P = .12) and the VWF:RCo/VWF:Ag ratio between the 2 patient groups. Student t test; P < .05 is considered significant. **P < 0.
Clinical Severity of the Bleeding Phenotype in Type 2B VWD and PT-VWD
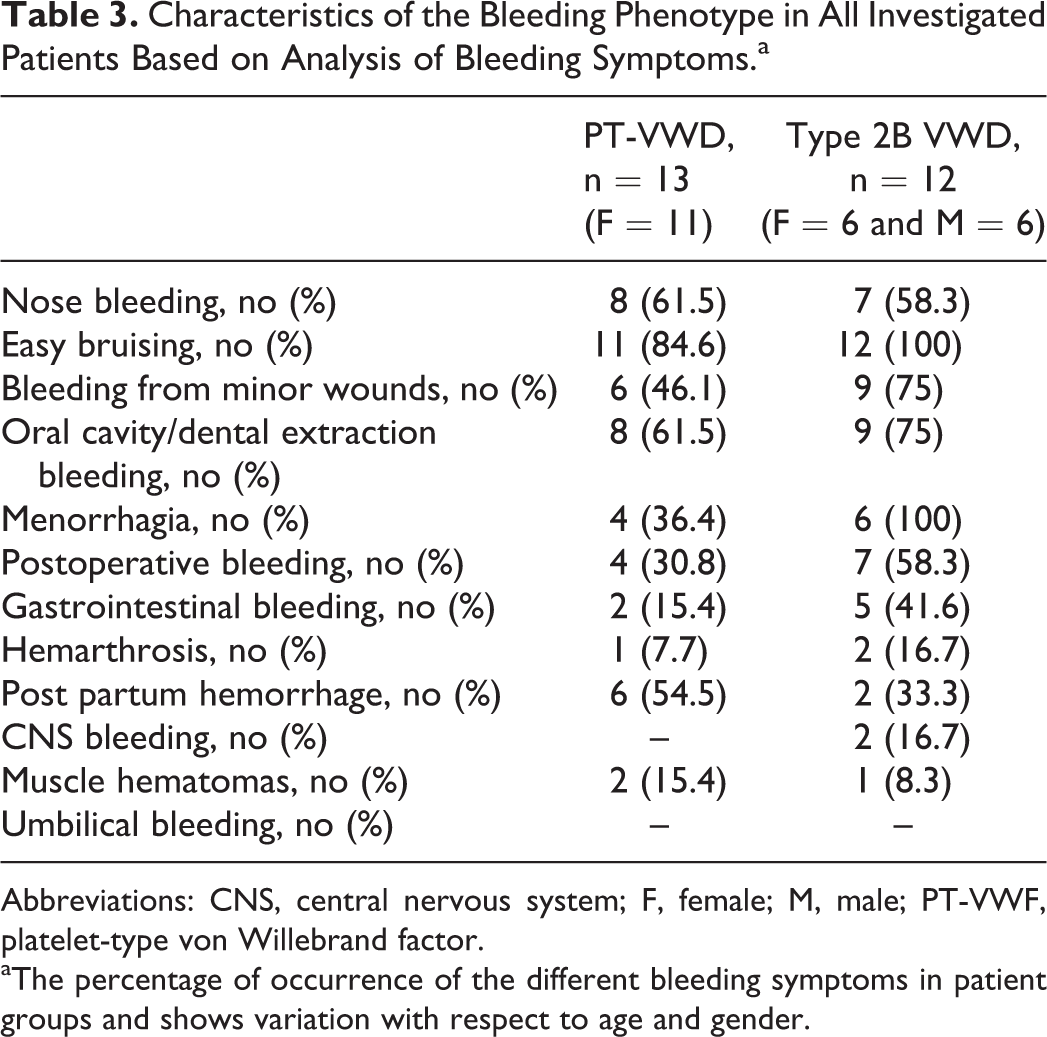
In comparing the severity of the clinical phenotype, heavy menstrual bleeding (HMB) was found the most common symptom in female patients in type 2B VWD but not in PT VWD. All female patients in type 2B VWD (100%) had HMB, while only 4 (36%) of the 11 females in the PT-VWD group showed that symptom. Epistaxis, easy bruising, and prolonged bleeding after a tooth extraction or gingival bleeding were generally the most commonly observed symptoms in all patients. Detailed bleeding symptoms and their occurrence and severity in the 2 disorders are summarized in Table 3.
Characteristics of the Bleeding Phenotype in All Investigated Patients Based on Analysis of Bleeding Symptoms.a
Abbreviations: CNS, central nervous system; F, female; M, male; PT-VWF, platelet-type von Willebrand factor.
aThe percentage of occurrence of the different bleeding symptoms in patient groups and shows variation with respect to age and gender.
Assessment of the Utility of the eBQ
All normal controls showed normal BS using the eBQ. The analysis of the 25 patients included in this study shows that the sensitivity and specificity of the eBQ in diagnosing the bleeding condition (both PT-VWD and type 2B VWD combined) was 76% and 100%, respectively, with a sensitivity of 62% in PT-VWD and 92% in type 2B VWD. The BS was highly variable within the 2 disorders.
Discussion
This study showed that the eBQ score is elevated in both type 2B and PT-VWD but with significantly higher level in type 2B VWD. This evaluation is not influenced by age factor or level of exposure to hemostatic challenges as only 1 patient with PT-VWD was younger than 15 years and is supported by the fact that 5 of the 13 in PT-VWD and only 1 of the 12 in type 2B VWD had normal scores. Another important observation is that thrombocytopenia was much more evident with larger variation in platelet count in type 2B VWD compared to PT-VWD. Furthermore, the relatively lower BS in PT-VWD (compared to 2B) correlated strongly with VWF activity and with platelet count. This was not seen in type 2B despite the more evident thrombocytopenia and much lower VWF levels. These data indicate that type 2B VWD may exhibit a severe bleeding phenotype with higher level of heterogeneity compared to that of PT-VWD.
Platelet-type VWD is more frequently diagnosed in females compared to males. Of the 53 cases reported worldwide, 37 (70%) are females (www.pt-vwd.org). Although it is generally acceptable that this is likely due to menstruation and childbirth, only 4 of the 11 of our PT-VWD in this study had menorrhagia and no postpartum hemorrhage reported. It is possible that menstruation, childbirth, or other factors add stresses that worsen the bleeding condition creating other types of bleeds. This can explain the over representation among females.
Many bleeding questionnaires have been reported in the literature for the purpose of diagnosis of bleeding disorders, 15,29 –31 but only a few studies are available with respect to RBDs. 32 –34 In addition, little information is available with respect to correlating BS with other parameters such as age or laboratory data. One study that used the condensed MCMDM-1VWD questionnaire showed a strong inverse correlation between BS and VWF:Ag in type 1 VWD. 18 Another study using the same questionnaire showed a significant inverse correlation between BS and VWF:Ag and factor VIII activity in patients with VWD. 35
The eBQ was first developed in 2010 and was designed to facilitate large worldwide studies. It was recently used to evaluate the potential of mild bleeding disorder (MBD) in a group of normal females and while assessing HMB using semiobjective method. The eBQ helped predicting MBD in 6.4% of the 47 women evaluated. 17,36 In this study, the eBQ helped further characterization of the bleeding phenotype in 2 closely similar clinical bleeding disorders.
A major difference in the eBQ used in this study compared to previously published and validated bleeding questionnaires lies in the electronic nature of the questionnaire that facilitated gathering of distant data worldwide. We believe the eBQ has the following advantages: (1) relatively easy to use in primary care setting and allows the clinician to summarize the clinical information about an individual and help follow-up in frequent clinic visits; (2) suitable tool for international research studies as it improves time management, communication, and record keeping; and (3) provides an automatic computation and archiving data at the point of entry that improves efficiency and reduces errors.
We cannot ignore the recent development and evidence of usefulness of ISTH BAT endorsed by the ISTH. This tool is expected to be used by the scientific community and attain a universal use in worldwide studies in the long term. Recently, the ISTH-BAT was evaluated in predicting defects in platelet functions in participants with suspected inherited platelet function disorders. Although the tool was proven powerful for documenting lifelong bleeding history, the scores were not predictive of the presence of platelet function defect on aggregometry in patients with suspected inherited platelet function disorders. 37 –39
Despite the relatively small number of patients evaluated, the study comprises a significant proportion of the well-characterized patients known to have the PT-VWD worldwide (53 patients according to the PT-VWD database www.pt-vwd.org). Nevertheless, validation is needed through a larger worldwide prospective study where PT VWD is better recognized and more patients are available for the study.
Based on this small study, the eBQ is highly specific in diagnosing bleeders affected by any of the 2 diseases but its sensitivity in predicting bleeding in PT-VWD is only 62% with a negative predictive value of 72.7%. This indicates that although all abnormal BSs were associated with disease diagnosis, a normal BS does not necessarily exclude a diagnosis of PT-VWD. Interestingly, the sensitivity was higher in type 2B VWD compared to PT-VWD. It is to be noted the 100% specificity observed in our study carry some selection bias and may not be achievable in the real world in terms of identifying patients with PT-VWD or 2B VWD versus noncases. Although the eBQ appears to have potential, its validity in other RBDs needs to be verified in a larger prospective study that enables the analysis of sufficient number of individual RBDs and evaluation of the peculiar clinical features of each disease.
In conclusion, the meticulous assessment of bleeding phenotype in PT-VWD and type 2B VWD can help understand more about the clinical presentations and guide an effective perhaps individualized management. Despite the close similarity of the 2 disorders and the universal consensus that the clearance mechanism of VWF–platelet complex is largely behind the bleeding diathesis, there is a possibility—given the different nature of the defects—of other mechanisms that can explain bleeding. Could certain PT-VWD mutations differentially alter platelet structure/function? Could there be other factors that modify the bleeding phenotype? Why would some patients with PT-VWD have normal BS? Future investigations are yet to reveal the answers to these questions.
Footnotes
Acknowledgments
We would like to thank Dr Paolo Gresele from the Department of Internal Medicine, Section of Internal and Cardiovascular Medicine, University of Perugia, Italy; Dr James O’Donnell, Director Haemostasis Research Group at Trinity College Dublin, Ireland; Dr Ian Chin-Yee, Dr Leonard Minuk, and Ms Lori Laudenbach from the Bleeding Disorders Program at the University of Western Ontario, for the wonderful cooperation in providing the clinical and laboratory data on patients with PT-VWD.
Authors’ Note
HK designed the study, acquired the PT-VWD data, analyzed the data, and wrote the article. MO acquired and analyzed the data related to the Brazilian type 2B VWD and reviewed the article. SS designed the eBQ and established/maintained the online eBQ. PJ acquired and analyzed the data related to the Canadian type 2B VWD and reviewed the article. MO designed and coordinated the study, supervised the data collection, analyzed the data, and wrote the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded by a research grant on PT-VWD by the Canadian Haemophilia Society.