
Abstract
N-terminal pro-brain natriuretic peptide (NT-proBNP) levels are associated with short- and long-term mortality in acute coronary syndrome (ACS). We investigated whether baseline NT-proBNP levels are associated with burden of coronary atherosclerosis assessed by SYNTAX score (SXScore). We enrolled 509 patients with ACS who underwent coronary angiography. The patients were divided into tertiles according to the SXScore: low SXScore (≤22), intermediate SXScore (23-32), and high SXScore (≥33). The NT-proBNP levels demonstrated an increase from low SXScore tertile to high SXScore tertile. The NT-proBNP levels according to the SXScore tertiles are as follows: low and intermediate (median 635 vs 1635, P = .014), low and high (median 635 vs 4568, P < .001), and intermediate and high (median 1635 vs 4568, P < .001). In multivariate analysis, NT-proBNP remained an independent predictor of high SXScore (odds ratio: 2.688, 95% confidence interval: 1.315-5.494, P = .007) together with age (P = .002), neutrophil–lymphocyte ratio (P = .017), and presence of non-ST-segment elevation ACS (P = .002). The NT-proBNP was independently associated with burden of coronary atherosclerosis in patients with ACS.
Introduction
Several studies have indicated clinical and laboratory variables that correlate with a poor prognosis in patients with acute coronary syndrome (ACS). 1,2 The SYNTAX score (SXScore) is a useful angiographic scoring system, and it can be used to cumulatively quantify the extent, severity, and complexity of coronary artery disease. 3 –5 The SXScore is an independent predictor of long-term mortality and morbidity in several patient types including ACS. 6 –10
The N-terminal pro-brain natriuretic peptide (NT-proBNP) is synthesised and secreted from the ventricular myocardium in response to increased left ventricular wall stretch 11 but also myocardial ischemia and infarction may stimulate its excretion. 12 –14 Serum NT-proBNP levels increase in several cardiovascular disease, which is the established biomarker for diagnosis, prognosis, and management, in particular in patients with established cardiovascular disease and heart failure. 15 –19 Additionally, serum NT-proBNP levels are closely related to the prognosis as a powerful predictor of both short- and long-term mortality in patients with ACS. 18,20 –26
The extent, severity, and complexity of coronary atherosclerosis are closely associated with cardiovascular prognosis in patients with ACS and could represent a mechanism to explain the relation between elevated NT-proBNP levels and mortality. However, the relationship between NT-proBNP levels and extent, severity, and complexity of coronary atherosclerosis in the settings of ACS remains unclear. In this study, we aimed to investigate whether serum NT-proBNP levels on admission were associated with SXScore in patients with ACS.
Methods
Study Population
We enrolled 509 patients with ACS who underwent coronary angiography between January 2013 and November 2013. The clinical spectrum of ACS consists of ST-segment elevation (STE) myocardial infarction (STEMI; STE-ACS, n = 279, 54.8%) and non-STE (NSTE) myocardial infarction (NSTEMI) or unstable angina (NSTE-ACS, n = 230, 45.2%), which are classified from the acute phase electrocardiography (ECG) changes and the development of myocardial necrosis. The exclusion criteria include patients with ACS who had SXScore of 0, patients with a history of prior coronary artery bypass grafting (CABG) surgery, a history of cardiopulmonary resuscitation before admission, presence of advanced valve disease and advanced renal/hepatic disease, known malignancy, a history of congestive heart failure, and the presence of overt pump failure (≥Killip class III) on admission. Also, all patients were investigated for noncardiac causes, and these patients were excluded.
Diagnostic Criteria for STE-ACS and NSTE-ACS
The leading symptom of ACS is typically chest pain. Patients with STE in ≥2 consecutive leads (with the cutoff point being > 0.2 mV in leads V1, V2, or V3, and > 0.1 mV in the other leads) were defined as having STE-ACS. The working diagnosis of NSTE-ACS is a rule-out diagnosis based on the ECG, that is, lack of persistent STE. Biomarkers (troponins) further distinguish NSTEMI and unstable angina. Imaging modalities are used to rule out or rule in differential diagnoses. The clinical presentation of NSTE-ACS encompasses a wide variety of symptoms. Traditionally, several clinical presentations have been distinguished: prolonged (>20 minutes) anginal pain at rest; new-onset (de novo) angina (class II or III of the Classification of the Canadian Cardiovascular Society); recent destabilization of previously stable angina with at least Canadian Cardiovascular Society Class III angina characteristics (crescendo angina); or postmyocardial infarction (MI) angina. The characteristic ECG abnormalities of NSTE-ACS are ST-segment depression or transient elevation and/or T-wave change. At presentation, the working diagnosis of NSTE-ACS, based on the measurement of troponins, will be further qualified as NSTEMI or unstable angina. Patients with normal troponin T levels were accepted as unstable angina pectoris. Patients with high troponin T levels were accepted as NSTEMI. The study protocol was approved by the local ethics committee, and all patients gave their written informed consent.
N-Terminal Pro-Brain Natriuretic Peptide Analysis
Serum NT-proBNP levels were measured from blood samples taken at admission to the emergency department or catheter laboratory. The NT-proBNP measurements were performed in plasma on an Elecsys 2010 analyzer, a commercially available electrochemiluminescent sandwich immunoassay (Elecsys proBNP, Roche Diagnostics, Mannheim, Germany). The lowest and highest detection limits of the assay were at 5 to 35.000 pg/mL. Creatinine clearance was also calculated from plasma creatinine levels assessed from blood sample taken at about 1 hour after first contact. 27
Coronary Angiography and SXScore Analysis
Coronary angiography was performed by the Judkins technique (Siemens Axiom Artis zee 2011; Siemens Healthcare, Erlangen, Germany). The severity and complexity of coronary atherosclerosis were assessed in several ways. The first was a simple classification in number of diseased vessel scoring system. The number of diseased vessels with ≥50% luminal stenosis in major coronary arteries was scored as 1 to 3. In addition, angiograms were scored according to the SXScore system. 4,5 All lesions causing ≥50% stenosis in a coronary artery with a diameter ≥1.5 mm were included in SXScore calculation. For the calculation, the software on the Web site (http://www.syntaxscore.com) was used. The SXScore was evaluated separately by 2 interventional cardiologists blinded to the study protocol and patient characteristics. In the presence of a contradiction between the 2 results, opinion of a senior interventional cardiologist was applied, and a common consensus was obtained. The patients were divided into tertiles according to the following SXScore: low SXScore group (SXScore ≤ 22), intermediate SXScore group (SXScore of 23 to 32), and the high SXScore group (SXScore ≥ 33).
Transthoracic echocardiography was performed for all patients within 48 hours after hospitalization (Vivid 3; GE Medical System, Horten, Norway). Left ventricular ejection fraction (LVEF) was measured using Simpson method.
Statistical Analysis
All analyses were performed using SPSS for Windows (version 18.0, SPSS, Chicago, Illinois). Quantitative variables were expressed as mean ± standard deviation for parametric variables and median and interquartile range (IQR) for nonparametric variables. Continuous variables were analyzed for normal distribution using the Kolmogorov-Smirnov test and analyzed for homogeneity using the Levene test. Comparisons of parametric values among the groups were performed by 1-way analysis of variance. Comparisons of nonparametric values among groups were performed by the Kruskal Wallis test. Categorical variables were compared with chi-square test. Tukey Honest Significant Difference (HSD) (for parametric variables) and Bonferroni adjustment Mann-Whitney U test (for nonparametric variables) were used as a post hoc test for multiple comparisons between the groups. A 2-tailed P < .05 was considered significant. Univariate logistic regression was used to identify independent predictors of high SXScore (variables: age, body mass index, diabetes mellitus, smoking, LVEF, type of ACS, glucose, creatinine, hemoglobin, neutrophil–lymphocyte ratio [N/L ratio], high-sensitivity C-reactive protein [hs-CRP], NT-proBNP [>1614 pg/mL], and low-density lipoprotein-cholesterol). After performing univariate analysis, significantly obtained variables (age, diabetes mellitus, smoking, glucose, creatinine, NT-proBNP [>1614 pg/mL], hemoglobin, N/L ratio, and type of ACS) were used in multivariate logistic regression analysis. The receiver–operating characteristic (ROC) curve analysis was performed in order to determine the best cutpoint value of NT-proBNP and troponin T; the sensitivity and specificity at that point were obtained for predicting high SXSscore.
Results
From the initial 552 consecutive patients who were admitted, 43 patients were excluded due to various exclusion criteria. A total of 509 patients matched the inclusion and exclusion criteria. The baseline characteristics of the study population classified according to SXScore tertiles are presented in Table 1. The mean age of patients in the high SXScore tertile was significantly higher than the intermediate and low SXScore tertiles (71 ± 11, 64 ± 12, 60 ± 12, respectively, P < .001). Prevalence of diabetes was higher, and current smoking patients were fewer in the high SXScore tertile than other tertiles (P = .004, P = .003, respectively). Additionally, LVEF was significantly lower in these patients with high SXScore compared to low and intermediate SXScore tertiles (P < .001). Patients with high SXScore more commonly presented with NSTE-ACS, while patients with low and intermediate SXScore more commonly presented with STE-ACS.
Baseline Characteristics of the Patients Stratified into SYNTAX Score Tertiles.
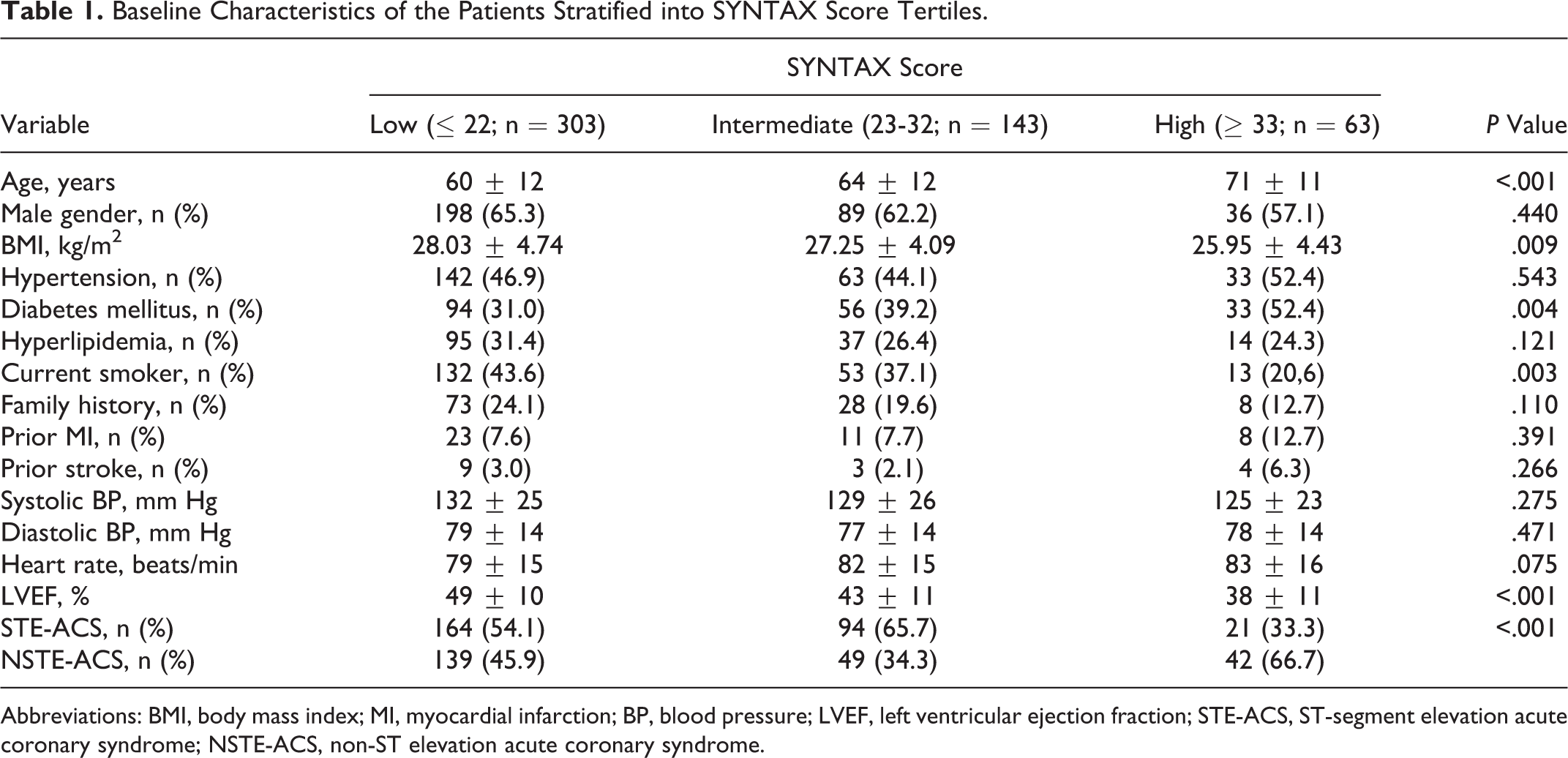
Abbreviations: BMI, body mass index; MI, myocardial infarction; BP, blood pressure; LVEF, left ventricular ejection fraction; STE-ACS, ST-segment elevation acute coronary syndrome; NSTE-ACS, non-ST elevation acute coronary syndrome.
Laboratory measurements of the patients stratified into SXScore tertiles are shown in Table 2. Patients in the high SXScore tertile had significantly higher serum glucose and hemoglobin A1c levels and N/L ratio, while they had lower values of estimated glomerular filtration rate and hemoglobin levels in comparison to patients in the lower tertiles (P value for all <.001). Furthermore, patients in the high and intermediate SXScore tertiles had higher serum hs-CRP and troponin T levels compared to patients in the low SXScore tertile (P < .001, and P < .001, respectively). Serum NT-proBNP levels on admission were significantly higher in the high SXScore patients compared to low and intermediate SXScore patients. The NT-proBNP levels demonstrated an increase from low SXScore to high SXScore tertiles (Table 2; Figure 1).
Laboratory Measurements of the Patients Stratified into SYNTAX Score Tertiles.
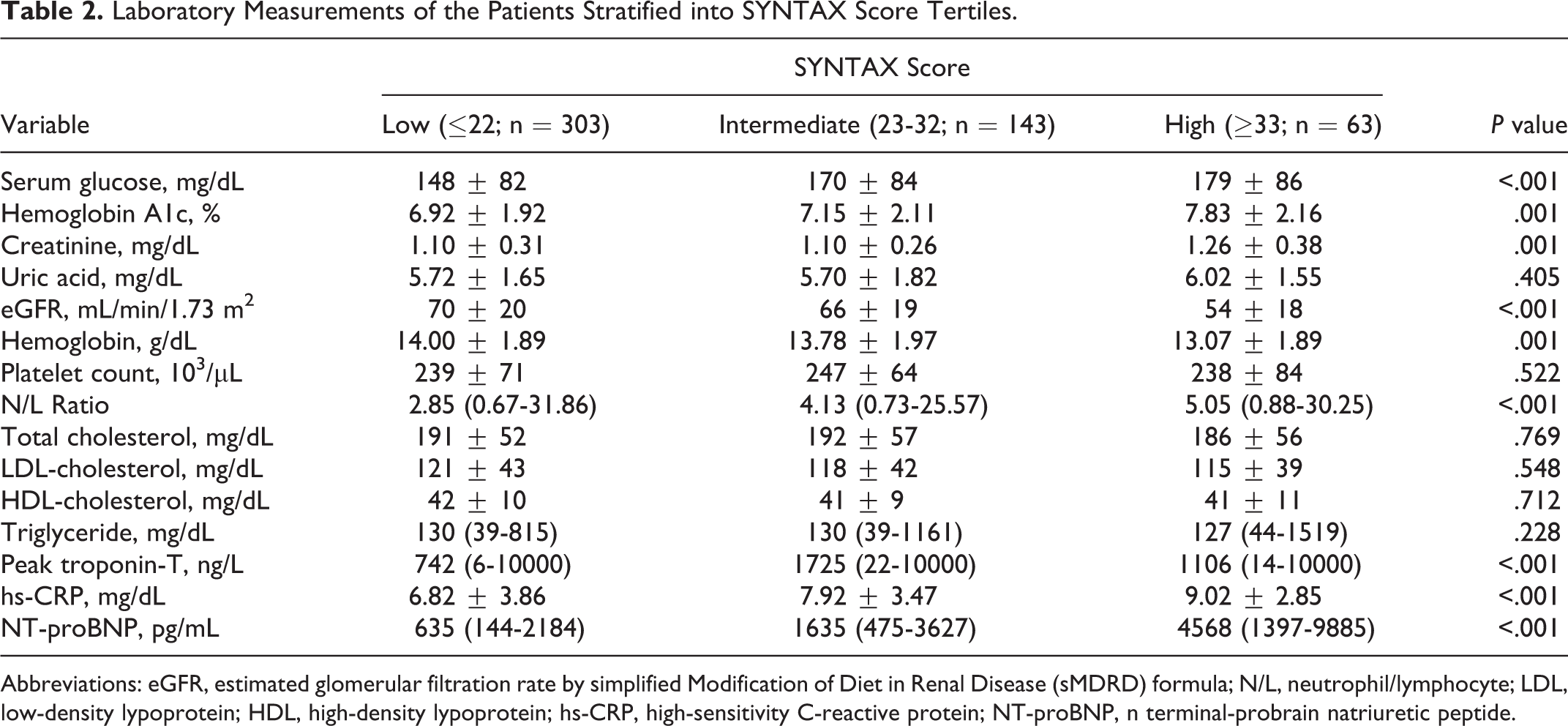
Abbreviations: eGFR, estimated glomerular filtration rate by simplified Modification of Diet in Renal Disease (sMDRD) formula; N/L, neutrophil/lymphocyte; LDL, low-density lypoprotein; HDL, high-density lypoprotein; hs-CRP, high-sensitivity C-reactive protein; NT-proBNP, n terminal-probrain natriuretic peptide.
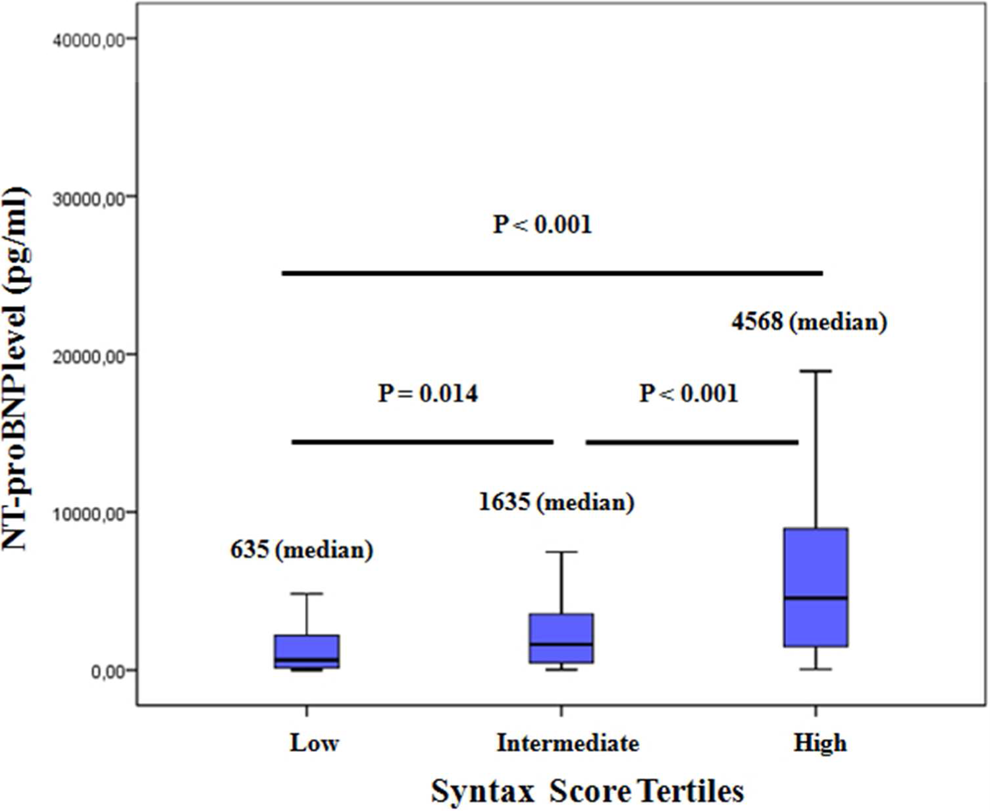
Comparison of N-terminal pro-brain natriuretic peptide (NT-proBNP) levels among groups.
Angiographic and procedural characteristics and management of patients according to SXScore tertiles are presented in Table 3. Patients with high SXScore had significantly higher rate of multivessel disease and chronic total occlusion compared to low SXScore and intermediate SXScore patients (P < .001 and P < .001, respectively). Single-, 2-, and 3-vessel disease were detected in 191 (37.6%), 160 (31.5%), and 157 (30.9%) patients, respectively. The left anterior descending artery was more commonly the culprit vessel in the high SXScore tertile. The rate of direct stenting was higher in patients with low SXScore, while decision of CABG surgery was more common in patients with high SXScore.
Angiographic and Procedural Characteristics of the Study Population.
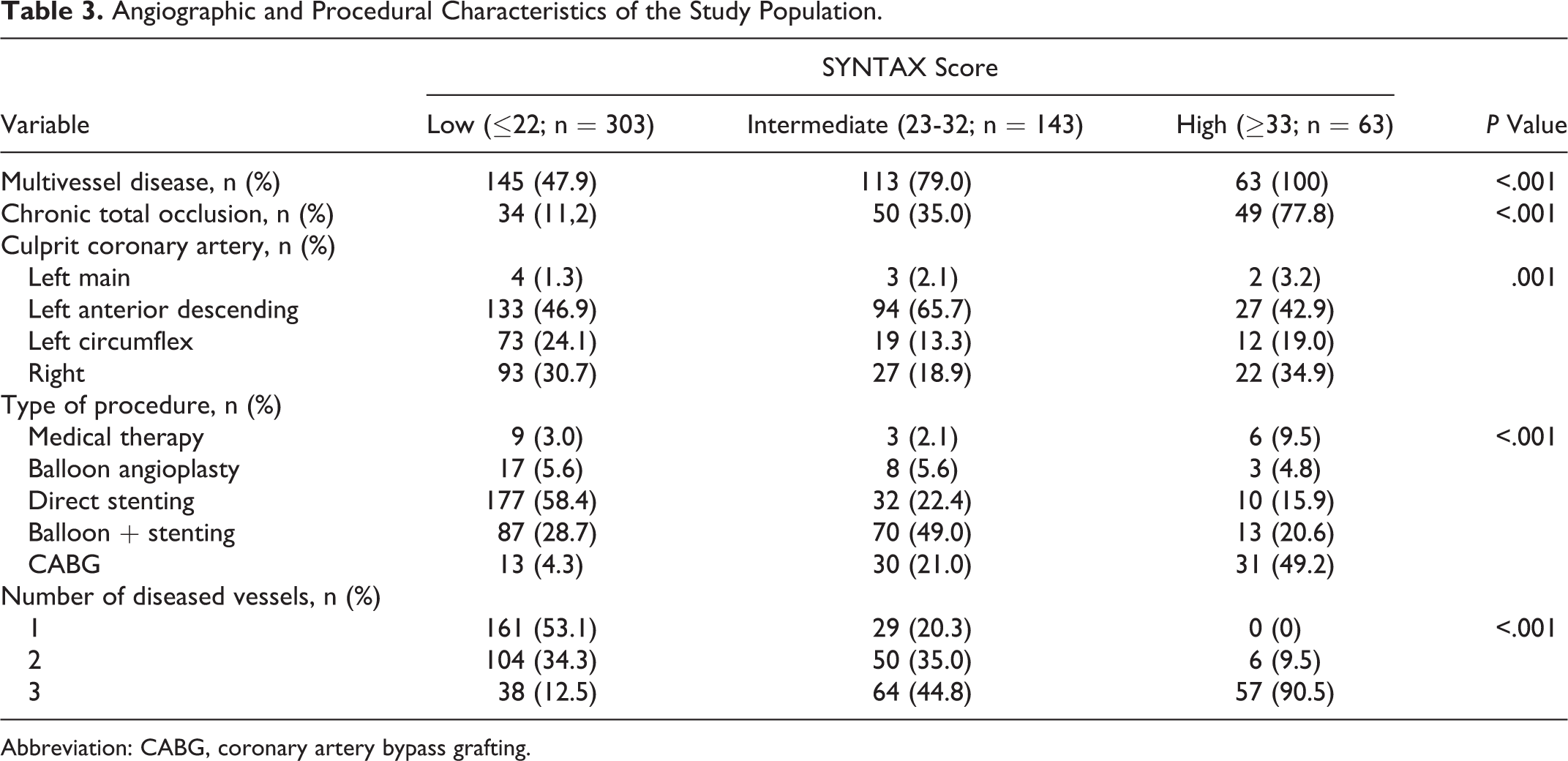
Abbreviation: CABG, coronary artery bypass grafting.
Univariate logistic regression analysis was used to identify independent predictors of high SXScore (variables: age, body mass index, diabetes mellitus, smoking, LVEF, type of ACS, glucose, creatinine, hemoglobin, N/L ratio, hs-CRP, NT-proBNP [>1614 pg/mL], and LDL cholesterol). After performing univariate analysis, significantly obtained variables (age, diabetes mellitus, smoking, glucose, creatinine, NT-proBNP [>1614 pg/mL], hemoglobin, N/L ratio, and type of NSTE-ACS) were used in multivariate logistic regression analysis. Multivariate logistic regression analysis showed that the strongest predictors of high SXScore were increased serum NT-proBNP levels (odds ratio [OR]: 2.688, 95% confidence interval [CI]: 1.315-5.494, P = .007) together with age (OR: 1.052, 95% CI: 1.019-1.087, P = .002), N/L ratio (OR: 1.069, 95% CI: 1.012-1.128, P = .017), and presence of NSTE-ACS (OR: 2.793, 95% CI: 1.427-5.291, P = 0.002; Table 4). Thus, increased serum levels of NT-proBNP were the strong predictor of high SXScore in patients with ACS, but NSTE-ACS was the strongest predictor of high SXScore.
Predictors of High SYNTAX Score (≥33) in Univariate and Multivariate Analyses.a
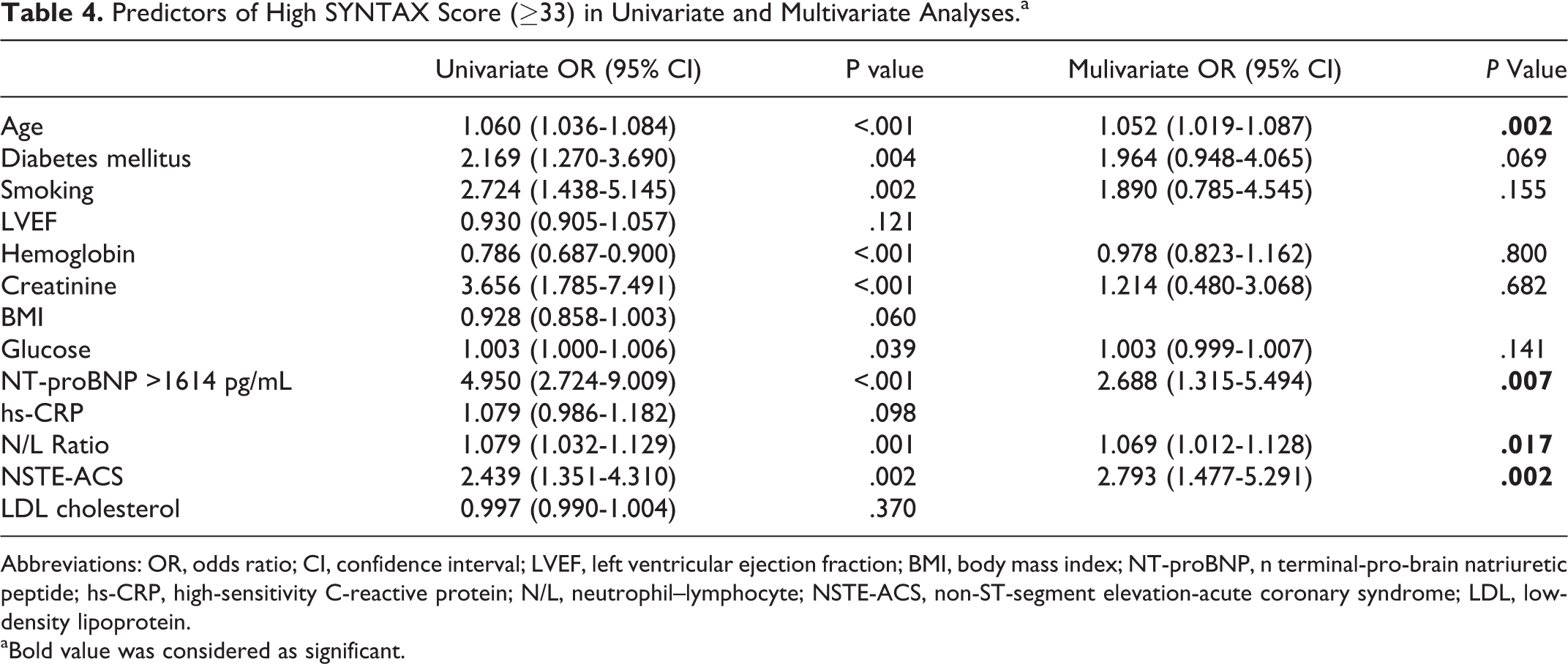
Abbreviations: OR, odds ratio; CI, confidence interval; LVEF, left ventricular ejection fraction; BMI, body mass index; NT-proBNP, n terminal-pro-brain natriuretic peptide; hs-CRP, high-sensitivity C-reactive protein; N/L, neutrophil–lymphocyte; NSTE-ACS, non-ST-segment elevation-acute coronary syndrome; LDL, low-density lipoprotein.
aBold value was considered as significant.
The ROC curve analysis showed that the NT-proBNP at a cut point of 1614 pg/mL was highly sensitive (75%) and specific (68%) and was a strongly independent predictor of high SXScore in patients with ACS (area under the curve [AUC] = 0.761, P < .001), while the ROC curve analysis showed that the peak troponin T levels at a cut point of 1044 ng/L was moderately sensitive (64%) and specific (60%) for predicting high and intermediate SXScores in patients with ACS (AUC = 0.63, P < .001; Figure 2).
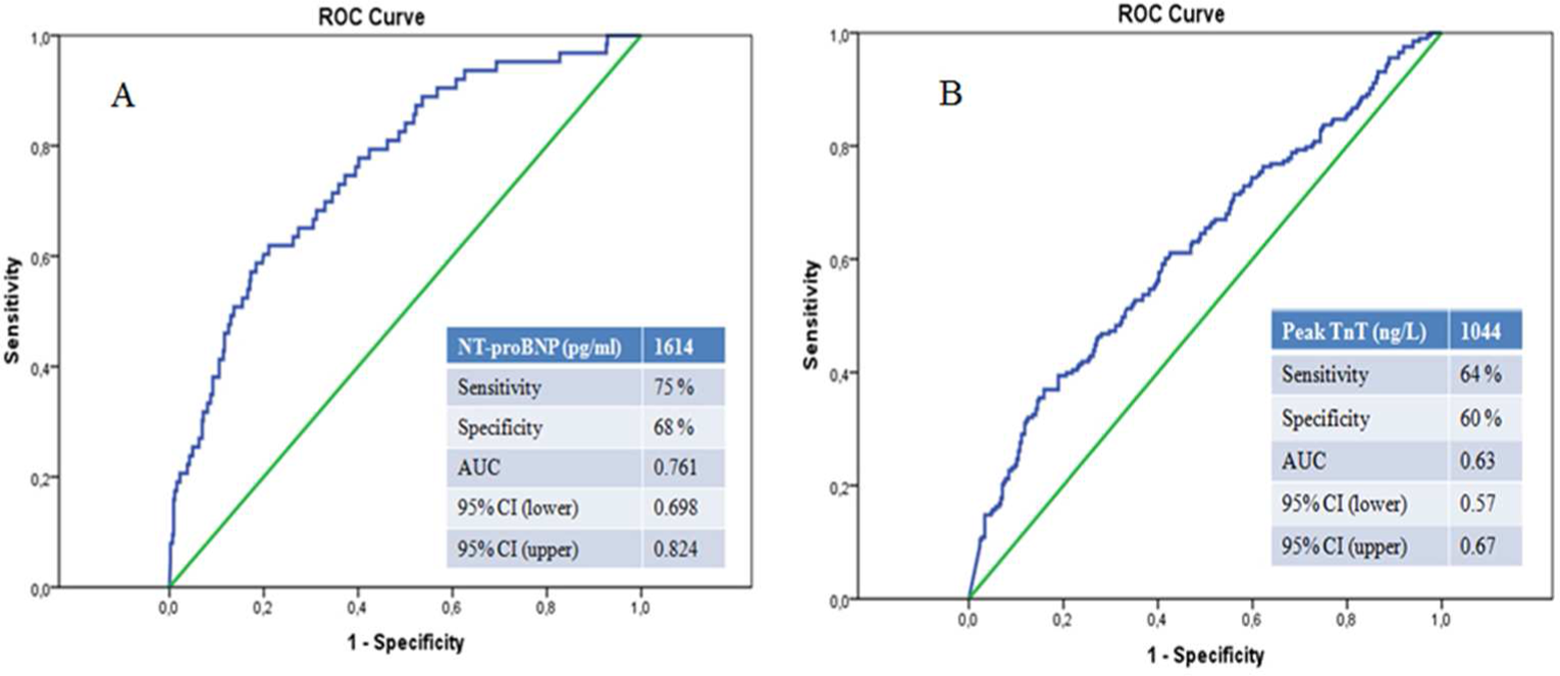
A, The receiver–operating characteristic (ROC) curve analysis for N-terminal pro-brain natriuretic peptide (NT-proBNP) levels in predicting patients with high SYNTAX score. Area under the curve (AUC): 0.761 (0.698-0.824). B, The ROC curve analysis for peak troponin T levels in predicting patients with intermediate and high SYNTAX scores. AUC: 0.635 (0.571-0.672).
Discussion
In the present study, we first demonstrated that there were significant differences in NT-proBNP levels among SXScore tertiles, and serum NT-proBNP levels were significantly higher in the high SXScore tertile group than in the low and intermediate SXScore tertile groups in patients with ACS. Thus, our study suggests that NT-proBNP levels measured on admission were strongly and independently associated with the extent, severity, and complexity of the coronary atherosclerosis in the setting of ACS.
There are various scales for the assessment of the extent and severity of coronary atherosclerosis. However, SXScore enables the assessment of extent and severity and also differs from the other methods by allowing us to evaluate the complexity of cononary lesion. 3 Moreover, several studies have shown that SXScore is strongly associated with the long-term major adverse cardiovascular events and mortality in several patient types including ACS. 6 –10 Since the extent and complexity of coronary atherosclerosis are important determinants of the risk of cardiovascular mortality, it is essential to identify serum markers to predict prognosis.
The NT-proBNP is released from the cardiac ventricles in response to increased wall stress and to ischemia per se. Several clinical studies have shown that the degree of NT-proBNP elevation can be used to predict future cardiac events and survival. 23,24 The NT-proBNP levels were found to be significantly higher in patients with coronary slow flow compared to a normal flow group. 28 Tuğcu et al 29 have shown that serum NT-proBNP levels were elevated in diastolic heart failure independent of left ventricular hypertrophy. Weber et al 12 have demontrated that NT-proBNP predicts extent of coronary artery disease and ischemia in patients with stable angina pectoris. In several studies on patients with STE-ACS and NSTE-ACS, the elevation in NT-proBNP has been observed. 30 –32 After ACS, NT-proBNP has been found as a major prognostic factor, independent of LVEF. 17,22 Elevated serum NT-proBNP levels on admission in patients with STEMI have been known as a predictor of cardiovascular mortality. 33,34 The NT-proBNP is also a reliable independent predictor of sudden cardiac death after MI. 35 Modulation of NT-proBNP is multifactorial, depending on left ventricular dysfunction, remodeling, left intraventricular pressure, and residual myocardial ischemia. 36,37 In this regard, ventricular dysfunction and/or myocardial ischemia per se can cause an increase in cardiac NT-proBNP expression followed by augmented secretion. 14,38 –40
In our study, although the underlying pathophysiological mechanism of the association between elevated NT-proBNP levels and higher SXScores in ACS is not completely understood, multiple mechanisms may be involved. One of the most reliable explanation may be related to severity of myocardial ischemia. Myocardial ischemia induces elevated cardiac filling pressures that result in increased myocardial stretch enhancing synthesis and release of NT-proBNP. Furthermore, ischemic or injured myocardial tissue releases additional NT-proBNP irrespective of hemodynamic factors. 14 Additionally, serum levels of NT-proBNP may be a new way to detect silent myocardial ischaemia. 41 In this regard, the study by Goetze et al 14,40 strongly suggests that acute myocardial hypoxia/ischemia per se stimulates BNP expression and the release of a newly synthesized NT-proBNP. In the present study, serum NT-proBNP levels were gradually increased according to low to high SXScore tertiles in patients with ACS, especially in the NSTE-ACS group. We suggested that more severe ischemia due to higher SXScores may be more likely to lead to increased NT-proBNP levels.
The NT-proBNP plays a role in vascular function and remodeling. Besides myocardial stretch and ischemia, other factors including endothelin, angiotensin II, and tumor necrosis factor have been found to stimulate secretion of NT-proBNP in vitro. 42,43 Both cardiac myocytes and fibroblasts secrete BNP which leads to fibrosis through induction of matrix metalloproteinases. 44
The other explanation for this relationship between higher NT-proBNP levels and higher SXScores may be related to left ventricular dysfunction besides the severity of myocardial ischemia or injury and inflammatory cytokines. Serum NT-proBNP level has been well known to rise in patients with congestive heart failure (CHF) and has become a powerful maker for diagnosis of CHF. 45,46 In patients with higher SXScore, lower LVEF and left ventricular dysfunction due to increased atrial or ventricular stretch from pressure or volume overload may be the underlying mechanism of the association between elevated NT-proBNP and high SXScores in our population. In our study, it was not significant in regression analysis; LVEF was decreasing stepwise with tertiles of SXScore (Table 1).
Study Limitations
The assessment of coronary angiographic findings was limited to visual interpretation, and angiography is a technique that detects only major coronary arterial lesions.
Conclusion
Serum NT-proBNP levels on admission were independently associated with extent, severity, and complexity of coronary atherosclerosis in patients with ACS together with age, NLR, and presence of NSTE-ACS. To the best of our knowledge, this is the first study to demonstrate that NT-proBNP is highly sensitive and specific and is a significant independent predictor of high SXScore in patients with ACS. Thus, NT-proBNP assessment may be considered in clinical practice for early risk stratification of patients with ACS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.