
Abstract
Objectives:
The SYNTAX score (SXscore) has emerged as a reproducible angiographic tool to quantify the extent of coronary artery disease based on the location and complexity of each lesion. The aim of this study was to evaluate whether the SXscore is an independent predictor of long-term cardiovascular outcomes in patients treated with primary percutaneous coronary intervention (PCI) for acute ST-segment elevation myocardial infarction (STEMI).
Methods:
A total of 2993 patients with acute STEMI who underwent primary PCI were stratified into the 4 groups according to the SXscore quartiles; quartile 1(Q1, SXscore ≤ 9, n = 819), Q2 (9 < SXscore < 16, n = 715), Q3 (16 ≤ SXscore < 20, n = 710), and Q4 (SXscore ≥ 20, n = 749).
Results:
There were significant differences among the quartiles with respect to age, basal creatinine and glucose levels, and the incidences of diabetes mellitus, Killip ≥2, and anemia. From Q1 to Q4, there were increasing rates of culprit left anterior descending lesion (P < .001), multivessel disease (P < .001), chronic total occlusion (P < .001), and proximal lesion localization (P < .001). At long-term follow-up, all-cause mortality, nonfatal myocardial infarction, stroke, rehospitalization due to heart failure, and the need of revascularization were significantly more frequent among the patients in the highest SXscore quartile. In multivariate analysis, after including the SXscore as a numerical variable into the model, every point of increase was determined as an independent predictor for long-term mortality (hazard ratio [HR] 1.03, 95% confidence interval [CI] 1.01-1.05, P = .008) and for overall major adverse cardiac events (MACEs; HR 1.02, 95% CI 1.01-1.04, P < .001).
Conclusion:
The SXscore is an independent predictor of both in-hospital and long-term mortality and MACE in patients with acute STEMI undergoing primary PCI.
Introduction
The incidence of ST-segment elevation myocardial infarction (STEMI) has been increasing over the last 20 years and it continues to be a significant public health problem in the whole world. 1 Primary percutaneous coronary intervention (PCI) has become the treatment of choice for acute STEMI as it improved the in-hospital and long-term mortality. Despite this improvement, in-hospital mortality rates were reported as 7% to 10% in some registry reports. 2 Therefore, risk stratification is essential for the clinical decision and management. Various risk scores such as Thrombolysis in myocardial infarction (TIMI), GRACE, and ZWOLLE have been used. Furthermore, besides angiographic variables, clinical data, such as anemia and renal impairment, are independent risk factors for in-hospital cardiovascular mortality. 3 –5
The SYNTAX score (SXscore) is a useful scoring system that has been developed to assess the severity and complexity of coronary artery disease (CAD) in order to determine the appropriate revascularization strategy. 6,7 The SXscore evaluated the severity of lesions, not only by luminal stenosis but also by plaque vulnerability, which is an important aspect of coronary artery anatomy in patients with acute STEMI. It has been recently demonstrated that SXscore was associated with postprocedural no reflow, renal functions, mortality, and increased target vessel revascularization rate in patients who underwent primary PCI. The aim of this study was to evaluate whether the SXscore is an independent predictors of long-term cardiovascular outcomes in patients treated with primary PCI for acute STEMI.
Methods
Study Population
We retrospectively reviewed 3457 patients with acute STEMI who underwent primary PCI in Kartal Kosuyolu Heart and Research Hospital (Istanbul) from January 2006 to February 2010. The average period of follow-up was a median of 54 months (range, 43-68). A total of 464 patients were excluded from the study. Exclusion criteria were as follows: patients treated with balloon dilatation only, patients with a previous history of coronary artery bypass graft surgery (CABG) or treated with emergent CABG, and patients with inconclusive clinical data from hospital files and computer records. Thus, the remaining 2993 (86%) patients comprised the study population. The patients were stratified into 4 groups according to the SXscore quartiles; quartile (Q) 1(Q1; SXscore ≤ 9, n = 819), Q2 (9 < SXscore < 16, n = 715), Q3 (16 ≤ SXscore < 20, n = 710), and Q4 (SXscore ≥ 20, n = 749). All patients gave written informed consent to the study protocol that was approved by the institutional ethical review board.
SYNTAX Score and Angiographic Analysis
SYNTAX Score was calculated as reportedpreviously. 8 Both baseline and after wiring/balloon SXscore were calculated for each patient. Since baseline SXscore is better correlated with clinical outcomes and long-term mortality, this score was used in the present study. The SXscore was calculated for all coronary lesions with a diameter stenosis greater than 50% in vessels larger than 1.5 mm. For the calculation, the software on the Web site (http://www.syntaxscore.com) was used. The SXscore was evaluated separately by 2 interventional cardiologists blinded to the study protocol and patient characteristics. When disagreement existed, a senior investigator was consented and a final decision was made by consensus. Patients were pretreated with 300 mg of aspirin and a loading dose of 600 mg of clopidogrel and intravenous (IV) standard heparin 100 U/kg (maximal dose 10.000 U, 60 U/kg in patients who were treated with glycoprotein IIb/IIIa inhibitors) before the procedure. All primary PCI procedures were performed by experienced interventional cardiologists using a femoral approach. The decision to perform direct or conventional stenting was at the discretion of the operator. The final TIMI flow grade and myocardial blush grade (MBG) were assessed. After the intervention, all patients were administered 1 mg/kg of enoxaparin twice daily (dose adjustment was done according to renal function), 150 mg/day of aspirin, and 75 mg/day of clopidogrel.
Data Collection
Baseline clinical and demographic characteristics and previous history of the patients were obtained from the hospital records. Blood biochemistry for creatinine, glucose, uric acid, troponin I, C-reactive protein (CRP), B-type natriuretic peptide (BNP), and complete blood count were measured in all patients on admission. Blood samples were repeated for troponin I every 6 hours until peak levels were reached and were repeated daily thereafter with creatinine and hemogram levels. In order to calculate ST-segment resolution (STR), electrocardiography was obtained on admission and 60 minutes after PCI. The STR greater than 70% was defined as complete resolution. 9 A transthoracic echocardiography was performed using a Vivid 3, (GE; Horten, Norway). Postprocedural left ventricular ejection fraction (LVEF) was measured using modified Simpson method. 10
Anemia was defined as a baseline hemoglobin <13 mg/dL in men and <12 mg/dL in women. Estimated glomerular filtration rate (eGFR) on admission was calculated according to Modification Diet in Renal Disease formula. Major bleeding was evaluated according to TIMI bleeding classification (>5 g/dL decrease in hemoglobin or >15% decrease in hematocrit level or the presence of intracranial bleeding). 11 Contrast-induced nephropathy was defined as a relative increase in baseline serum creatinine of greater than 25% or 0.5 mg/dL within 72 hours after contrast administration.
Definitions
Acute myocardial infarction (MI) was defined as the presence of typical ongoing ischemic chest pain for longer than 30 minutes and ST-segment elevation of 1 mm or greater in at least 2 contiguous leads or a new left bundle branch block on the initial electrocardiogram. Patients who were not treated with thrombolytic agent and presented within the first 12 hours of the onset of symptoms were included in the study. Thrombus burden (baseline and after balloon dilatation) was evaluated according to the TIMI thrombus scoring. The TIMI score ≥4 was defined as high-grade thrombus burden. Distal embolization was defined as distal filling defect with an abrupt “cutoff” in 1 or more peripheral coronary branches of the infarct-related artery. The MBG was assessed using standard methods. 12 Reinfarction was defined as the recurrence of typical clinical symptoms lasting for >30 minutes and new abnormal Q waves with a new elevation of the creatine kinase MB fraction levels >2 times the upper limit of normal or any rise by ≥50% above a previously elevated level. Any repeat revascularization was defined as repeated PCI or bypass grafting of both infarct-related artery and noninfarct-related artery, driven by ischemic symptoms. Although in-hospital outcomes were obtained from hospital records, long-term clinical data were documented by review of hospital records, telephone interviews, and office visits to the outpatient clinic. Patients who could not be reached despite all efforts were excluded from the study as stated previously. We verified the patient mortality by contacting to National Registration Office.
Statistical Analysis
Continuous variables are expressed as mean ± standard deviation or median (interquartile range) and categorical variables are expressed as number (percentage). Group means for continuous variables were compared using 1-way analysis of variance or Kruskal Wallis variance analysis. Categorical variables were compared using chi-square (χ2) or Fisher χ2 test. The Cox proportional hazard model was applied for the relation between the SX score and long-term mortality, reinfarction, revascularization, stroke, and overall major adverse cardiac event (MACE). All variables showing significance values P < .05 (age, diabetes mellitus, hypertension, peripheral artery disease, preinfarction angina, Killip class, pain-to-balloon time, eGFR, baseline anemia, glucose, uric acid, BNP, CRP, SXscore quartiles, final TIMI flow, distal embolization, postprocedural LVEF, STR, MBG, peak troponin I, IABP use, inotropic drug use, IV diuretic use) were included in the model. Variables used for calculation for SXscore were not included in the model. The SXscore was included in the multivariate analysis separately both as a continuous and as a quartile, and the analysis was repeated. Multivariate analysis was applied separately for all outcomes (death, reinfarction, stroke, and revascularization) and overall MACE. The relation between the SXscore quartiles and the incidence of MACE was evaluated. Event-free survival curves were generated by the Kaplan-Meier method and differences in survival were compared using log-rank test. A P value less than .05 was considered statistically significant. All statistical analyses were carried out using SPSS 11.5 for Windows (SPSS Inc, Chicago, Illinois).
Results
In this single-center study, 2993 patients were divided into the 4 quartiles according to the SXscores.
Baseline Characteristics
Baseline characteristics are shown in Table 1. There were significant differences among the quartiles with respect to age, basal creatinine and glucose levels, and the incidences of diabetes mellitus, Killip≥2, and anemia. Additionally, plasma BNP and CRP levels were found to be gradually increased from Q1 to Q4. Previous medications and other clinical characteristics were comparable among the SXscore quartiles. There were significant differences among the groups with respect to the rates of inotrope (Q1 = 47 [5.7%], Q2 = 49 [6.9%], Q3 = 75 [10.6%] and Q4 = 123 [16.4%); P < .001] and IV diuretic usage (Q1 = 64 [7.8%], Q2 = 54 [7.6%], Q3 = 103 [14.5%], and Q4 = 148 [19.8%]; P < .001) during the in-hospital period, whereas angiotensin-converting enzyme inhibitor/angiotensin receptor blocker, β blocker, and statin therapy did not significantly differ among the SXscore quartiles.
Baseline Characteristics and Medication.
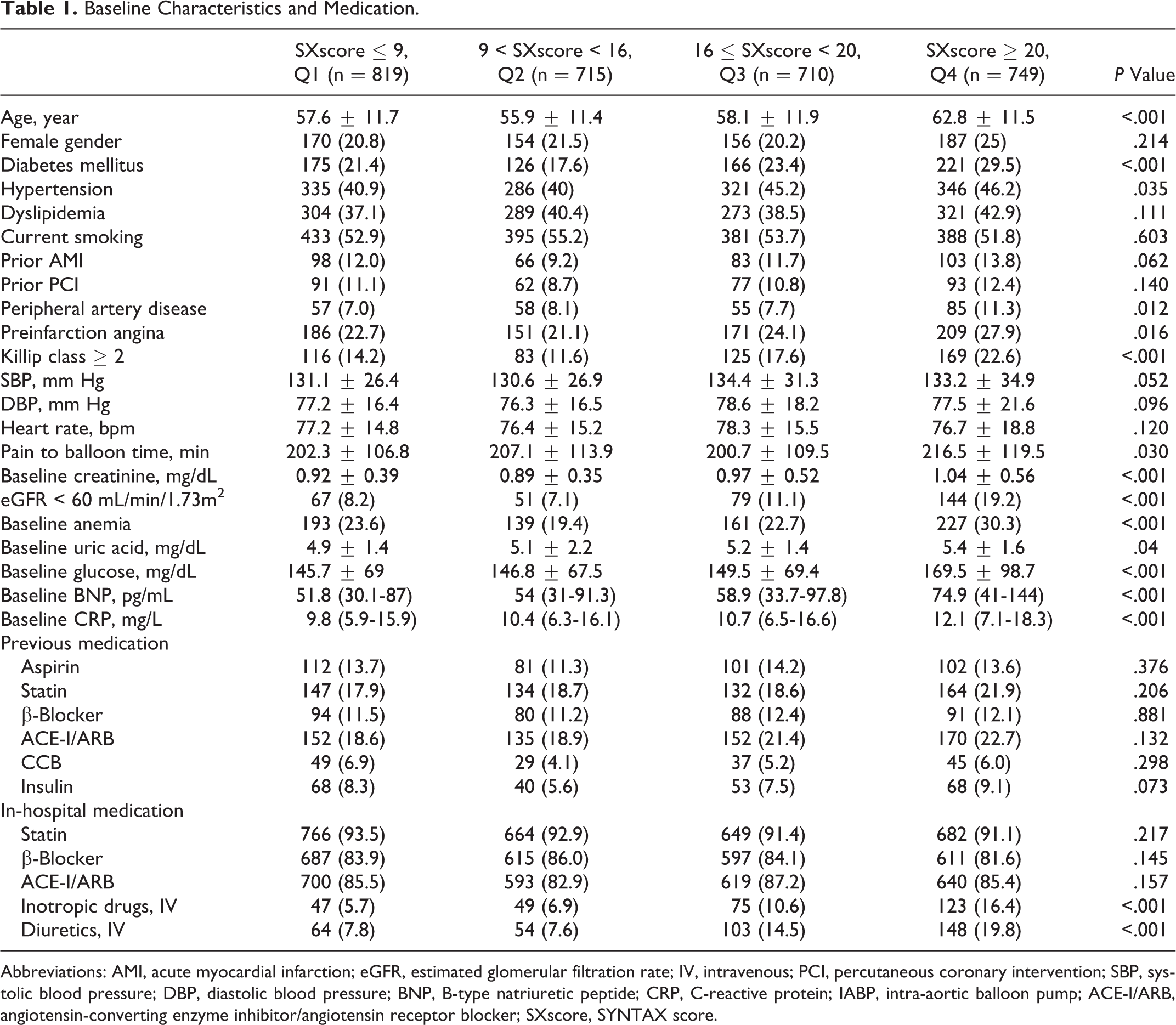
Abbreviations: AMI, acute myocardial infarction; eGFR, estimated glomerular filtration rate; IV, intravenous; PCI, percutaneous coronary intervention; SBP, systolic blood pressure; DBP, diastolic blood pressure; BNP, B-type natriuretic peptide; CRP, C-reactive protein; IABP, intra-aortic balloon pump; ACE-I/ARB, angiotensin-converting enzyme inhibitor/angiotensin receptor blocker; SXscore, SYNTAX score.
Angiographic Data During Primary PCI
Angiographic characteristics are shown in Table 2. From Q1 to Q4, there were increasing rates of culprit left anterior descending lesion (P < .001), multivessel disease (P < .001), chronic total occlusion (P < .001), and proximal lesion localization (P < .001). Likewise, the incidences of high-grade thrombus burden were found as follows: Q1 = 360 (44%), Q2 = 331 (46.3%), Q3 = 336 (47.3%), and Q4 = 390 (52.1%); P < .013. From Q1 to Q4, the rate of postprocedural visible distal embolization was found to be significantly increasing (Q1 = 44 [5.4%], Q2 = 62 [8.7%], Q3 = 45 [6.3%], and Q4 = 61 [8.1%]; P < .001); however, the rate of postprocedural TIMI grade 3 flow was found to be significantly decreasing (Q1 = 754 [92.1%], Q2 = 657 [91.9%], Q3 = 646 [91%], and Q4 = 645 [86.1%]; P < .001). Moreover, the frequencies of intra-aortic ballon pump and mechanic ventilator usages and duration of hospitalization were significantly increasing from Q1 to Q4.
Angiographic and Procedural Properties.
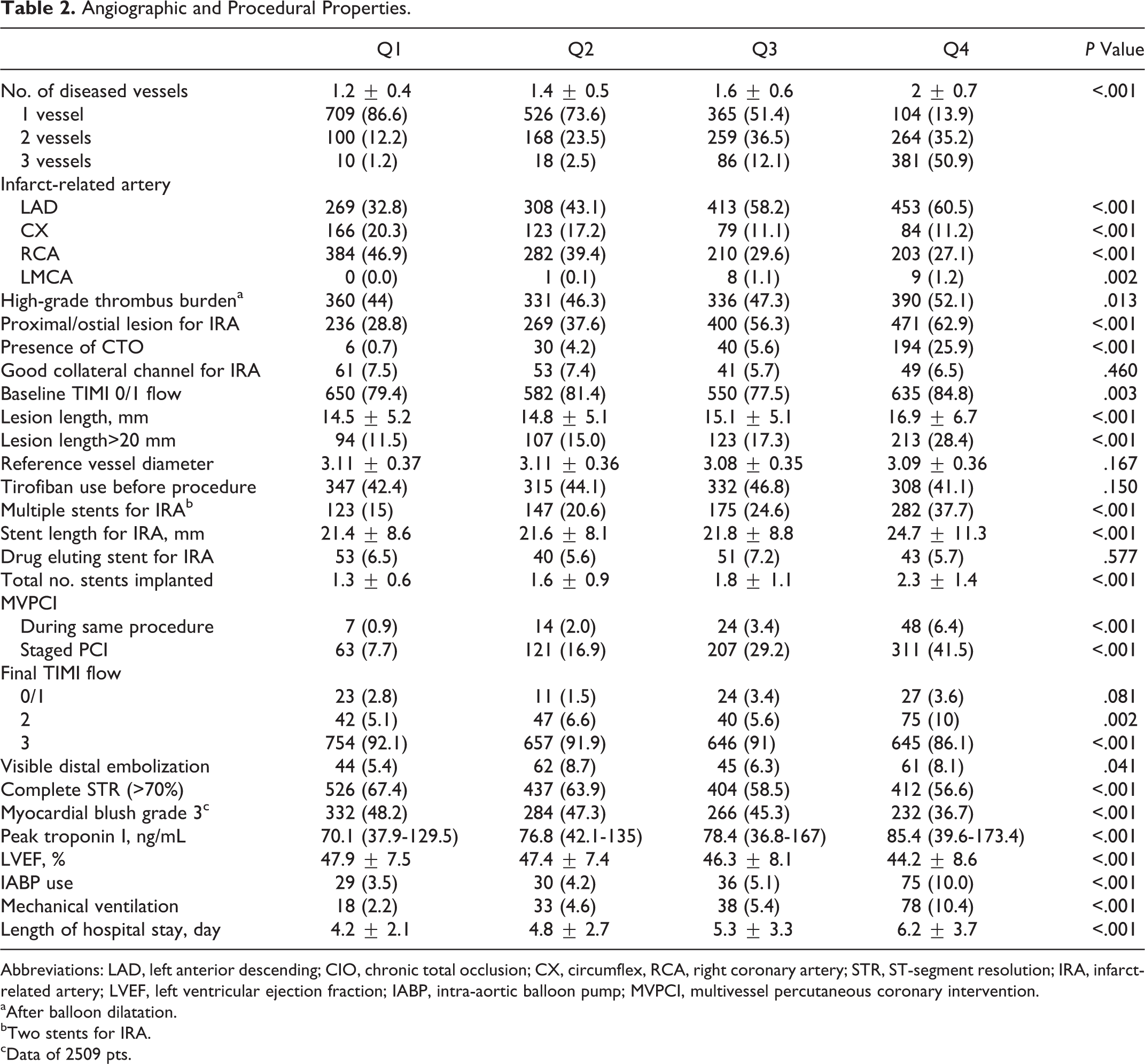
Abbreviations: LAD, left anterior descending; CIO, chronic total occlusion; CX, circumflex, RCA, right coronary artery; STR, ST-segment resolution; IRA, infarct-related artery; LVEF, left ventricular ejection fraction; IABP, intra-aortic balloon pump; MVPCI, multivessel percutaneous coronary intervention.
aAfter balloon dilatation.
bTwo stents for IRA.
cData of 2509 pts.
In-Hospital and Long-Term Prognosis
Table 3 presents the in-hospital adverse outcomes and long-term prognosis after primary PCI. During early in-hospital period, the rates of all cause death, heart failure, new atrial fibrillation development, secondary ventricular tachycardia/fibrillation, and contrast-induced nephropathy were significantly increasing in parallel with the increasing quartiles. However, stroke, major bleeding, and reinfarction rates were not different among the 4 groups. At long-term follow-up, all cause mortality, nonfatal MI, stroke, rehospitalization due to heart failure, and the need of revascularization were significantly more frequent among the patients in the highest SXscore quartile. Overall MACE was determined as follows: (Q1 = 279 [34.1%], Q2 = 257 [35.9%], Q3 = 342 [48.2%], and Q4 = 408 [54.5%]; P < .001).
In-Hospital and Long-Term Outcomes.
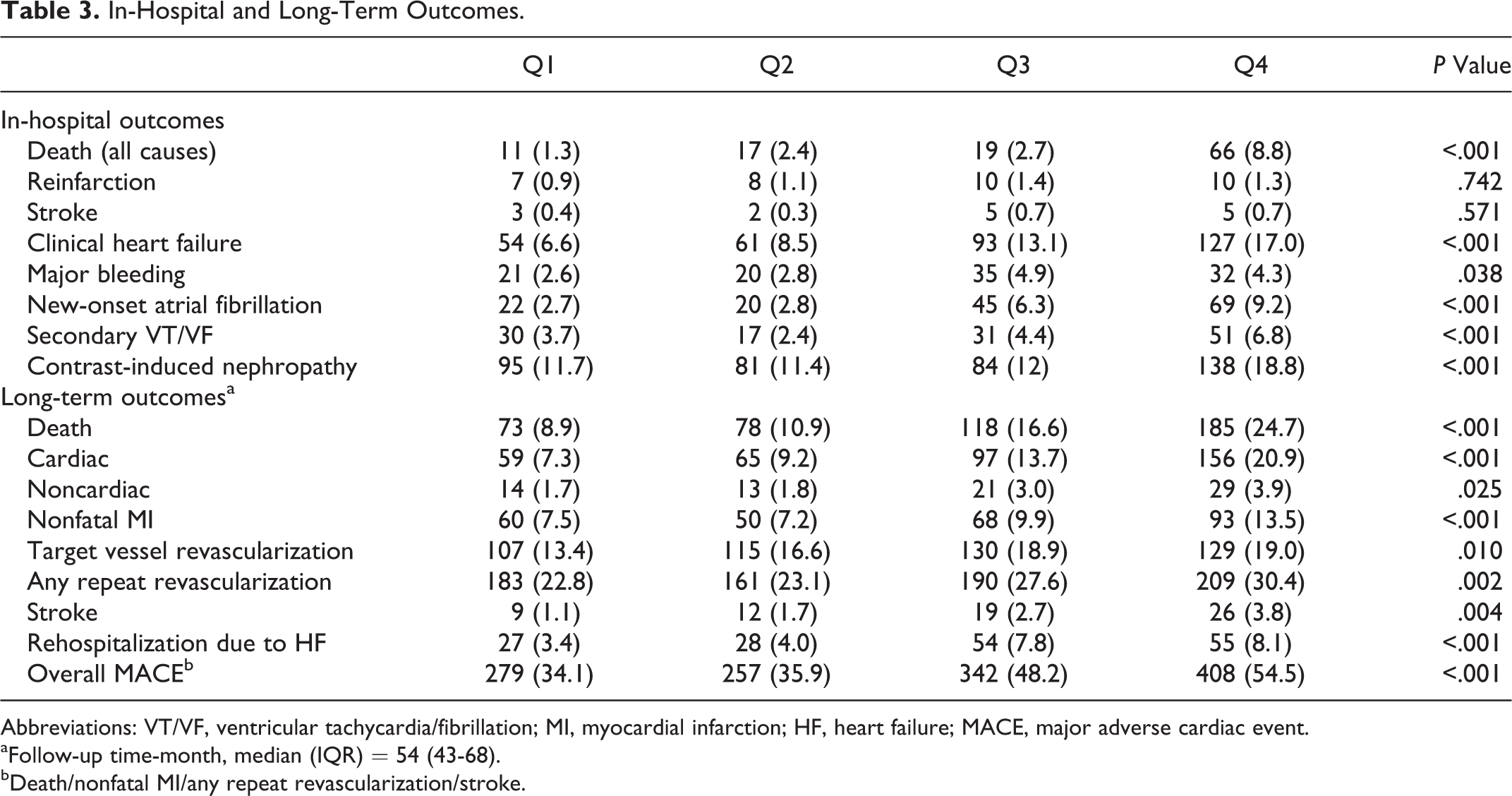
Abbreviations: VT/VF, ventricular tachycardia/fibrillation; MI, myocardial infarction; HF, heart failure; MACE, major adverse cardiac event.
aFollow-up time-month, median (IQR) = 54 (43-68).
bDeath/nonfatal MI/any repeat revascularization/stroke.
In order to predict the long-term mortality, multivariate analysis was performed (Table 4). After adjusting Q1 level as a reference point, all cause mortality was found significant for Q3 and Q4, hazard ratio (HR; 95% confidence interval [CI]) 1.44 (1.05-1.99), P = .026; 1.46 (1.06-2.01), P = .022, respectively, whereas no significant association was noted for Q2 (P = .54).
Hazard Ratios for Long-Term Clinical Outcomes According to SXscore Quartiles; Cox Proportional Hazard Model.
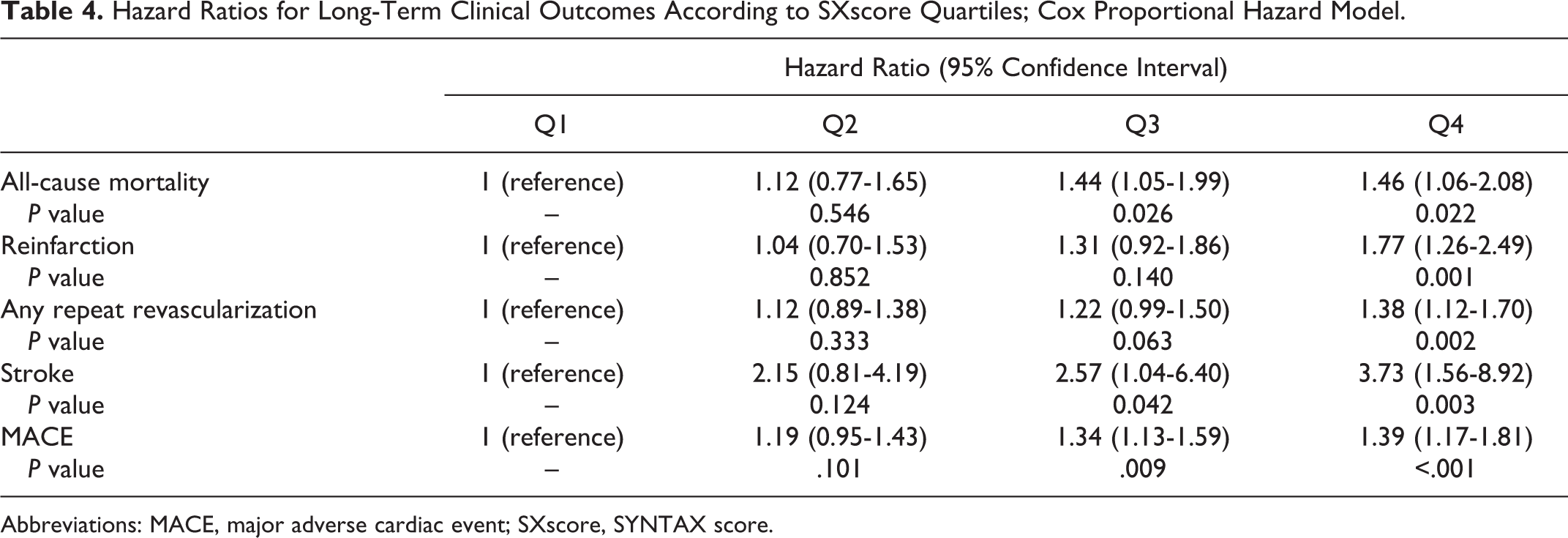
Abbreviations: MACE, major adverse cardiac event; SXscore, SYNTAX score.
In addition, although Q4 was determined as an independent predictor for reinfarction and revascularization, Q3 and Q4 were found to independently predicting stroke and MACE. After including the SXscore as a numerical variable into the model, every point of increase was determined as an independent predictor for long-term mortality (HR 1.03, 95%CI 1.01-1.05, P = .008) and for overall MACE (HR 1.02, 95% CI 1.01-1.04, P < .001).
In the Kaplan-Meier survival analysis, log-rank P < .001 was found for long-term survival (Figure 1). In subgroup analysis, Q1 versus Q2 P = .327, Q1 versus Q3 P < .001, Q1 versus Q4 P < .001, Q2 versus Q3 P = .002, Q2 versus Q4 P < .001, and Q3 versus Q4 P = .046 were detected.
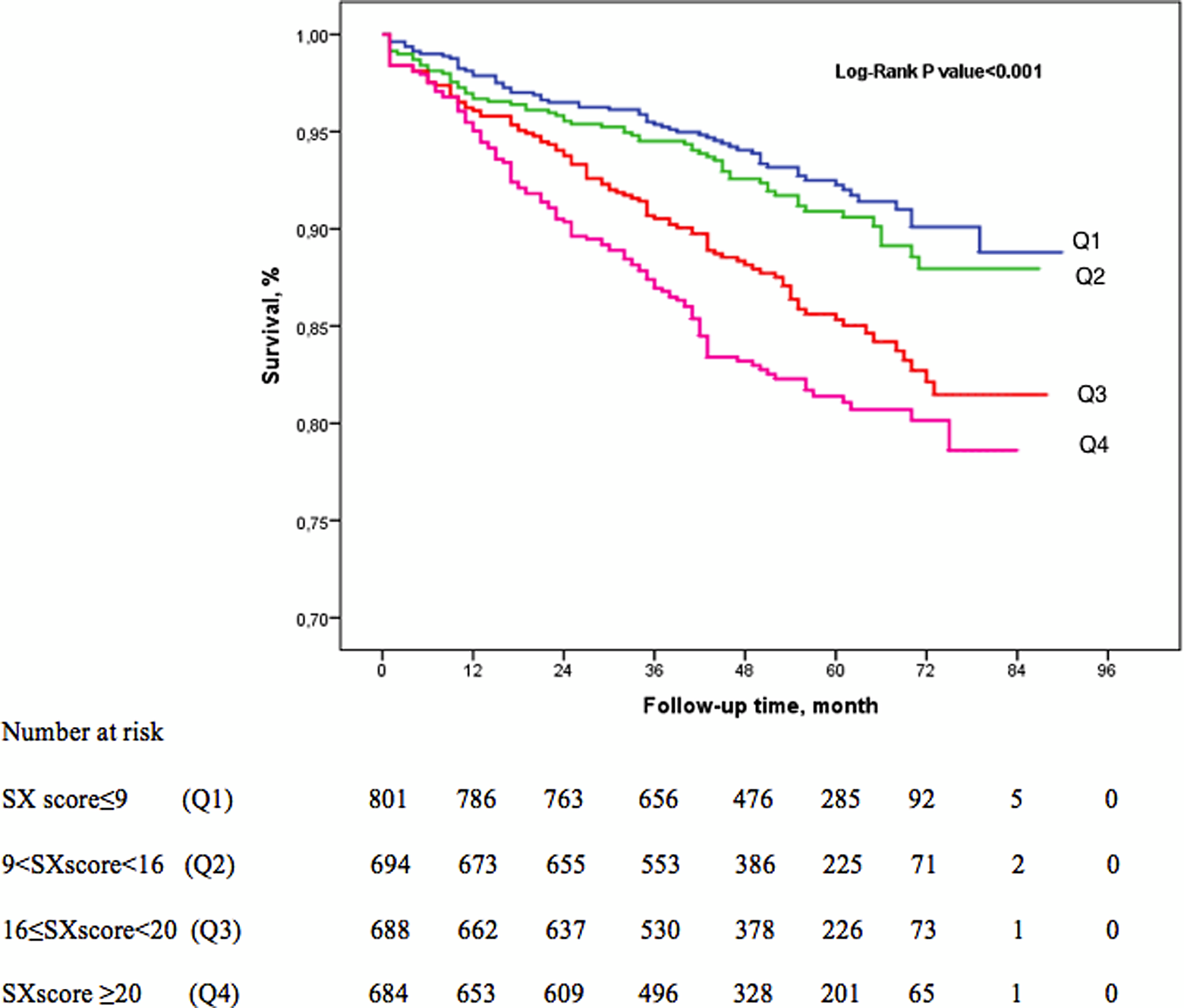
Kaplan-Meier survival analysis for long-term follow-up.
Discussion
This study showed that high SXscore is associated with worse clinical status on admission(higher coincidences of diabetes mellitus, anemia, renal dysfunction, and worse Killip class) and more complex angiographic features. Moreover, duration of in-hospital period was longer and IV inotrop and diuretic need, in-hospital mortality, and MACE were more common in patients with high SXscore. The main finding of this study is that SXscore is an independent predictor of long-term mortality and MACE in patients treated with primary PCI for acute STEMI.
Coronary artery disease is the most common cause of death in the world. According to the European Society of Cardiology guidelines, 1 of the every 6 men and 7 women dies from MI. The STEMI is an important part of the acute coronary syndromes. In-hospital mortality rates ranged between 6% and 14%. 13 Many factors are known to predict this event. Previous MI, door to balloon time, the presence of diabetes, anemia, chronic renal failure, and ejection fraction on admission are the main predictors of mortality. 14 Risk scores such as TIMI and GRACE are used as an indicator of mortality. Beyond clinical data, angiographic data are also used to predict the long-term prognosis. Biondi-Zoccai et al showed in a meta-analysis that patients with STEMI having multivessel disease have worse clinical outcomes than those with single-vessel disease. 15 Likewise, Brown et al showed that lesion complexity was predictive of mortality at a follow-up of 2 years. 16 In our study, we found that increasing lesion complexity from Q1 to Q4 was a predictor of both in-hospital and long-term mortality.
The SXscore has emerged as a reproducible angiographic tool to quantify the extent of CAD based on the location and complexity of each lesion. It is an important determinant of decision-making process in patients with left main or multivessel disease. Apart from this, SXscore was shown to be related to bad angiographic appearance and poor clinical outcome in small clinical trials consisting of elective cases and acute coronary syndromes. 6,8 Şahin et al showed that high SXscore was an independent predictor of no-reflow development. 17 In our study, we showed that high SXscore was associated with more frequent visible distal embolism and less final TIMI grade 3 flow rates. Furthermore, high SXscore was found to be related to contrast-induced nephropathy and poor clinical outcome in different studies. On the other hand, modified SXscore was developed in order to increase the predictive role of SXscore. A coronary lesion with a diameter stenosis of at least 50%, in vessels at least 1.5 mm is scored in classical SXscore. Fractional flow reserve has been incorporated into SXscore to form the “functional SXscore” by Nam et al. 18 This score exhibited better patient risk stratification than the conventional angiography-based SXscore. Farooq et al used merged data from 7 contemporary coronary stent trials to develop “Clinical SXscore” by logistic regression model. They developed a core model by combining the SXscore with age, ejection fraction, and creatinine clearance. Compared to the SXscore, the clinical SXscore significantly enhances the risk stratification of patients with PCI for death at 1 year and allows for a more personalized assessment of long-term patient risk. 19 The same group also showed that residual SXscore (SXscore was calculated based on the remaining obstructive coronary disease after treatment with PCI) was a powerful indicator of 5-year mortality. A residual SXscore >8 was associated with 35.3% all-cause mortality at 5 years. 20 In our study, classical SXscores were found as good prognostic factors for long-term outcome in primary PCI patients. Furthermore, increased age, worse ejection fraction, and decreased creatinine clearance, which are used in clinical SXscore, were found to be higher in Q4.
Current guidelines for the management of STEMI indicate that culprit-only intervention should be performed acutely during primary PCI in the absence of cardiogenic shock. However, primary percutaneous intervention for noninfarct-related artery was shown to be useful in a recently published article. A total of 465 patients with STEMI were randomly assigned to undergo infarct artery-only PCI or additional PCI in noninfarct arteries during the initial procedure. Staged or delayed PCI was allowed only in patients with angina or positive ischemia findings. The study was stopped early after a mean of 2 years of follow-up because of a significant between-group difference in the primary composite end point of cardiac death, nonfatal MI, or refractory angina which occurred in significantly less patients in preventive PCI group (9% vs 23%, HR; 0.35, CI 0.21-0.58; P < .001). 21 Our study and previous studies were designed to open infarct artery only in the light of current guidelines. Since patients with high SXscore have more multivessel disease or complex lesions, not to open nonculprit lesions during the initial procedure may give rise to these bad clinical outcomes in these patients.
Limitations
Our study has some important limitations. First, this study has a retrospective and single-center design. Despite retrospective involvement, the patients were prospectively followed up. In order to prevent bias, in-hospital and follow-up data were collected by different investigators. Second, we included patients with acute STEMI who underwent primary PCI. Thus, the results of this study may not be extrapolated to all patients such as presented with other form of acute coronary syndrome or who were not treated with PCI. To confirm this hypothesis more effectively, a study with a large sample with attendance of multicentre is required.
Conclusion
The SXscore is an independent predictor of both in-hospital and long-term mortality and MACE in patients with acute STEMI undergoing primary PCI.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.