
Abstract
The aim of this study is to evaluate the incidence and predictors of silent neuronal injury (SNI) after coronary angiography (CAG) and intervention by serial measurement of serum neuron-specific enolase (NSE) in patients presented with acute coronary syndrome (ACS). Ninety-eight consecutive patients presented with ACS and underwent CAG and intervention were included in the study. The NSE levels significantly increased after CAG and intervention compared to baseline levels (22.03 ± 27.70 and 10.08 ± 3.15 consecutively). Left ventricular ejection fraction in the SNI+ group was significantly lower than that in the SNI− group (43.71% ± 12.51%, 50.84% ± 9.34%, P = .002). Maximal creatinine kinase myocardial band, troponin I, and SYNTAX score of the SNI+ group were significantly higher than those of the SNI− group (103.83 ± 99.22, 51.92 ± 78.33, P = .006; 50.04 ± 66.18, 19.18 ± 30.50, P = .002; 103.83 ± 99.22, 51.92 ± 78.33, P = .006; and 50.04 ± 66.18, 19.18 ± 30.50, P = .002 successively). SYNTAX score and performing percutaneous coronary intervention were the independent predictors of SNI (P = .009, odds ratio [OR] = 1.06, 95% confidence interval [CI] = 1.014-1.107, P = .036, OR = 4.262, 95% CI = 1.097-16.56). Percutaneous coronary intervention and coronary artery lesion complexity may increase the risk of SNI in patients with ACS.
Introduction
Silent neuronal injury (SNI) is defined as embolic origin cerebrovascular lesion due to embolic vascular occlusion incidentally diagnosed in otherwise healthy patients. Although SNI is 7 to 9 times common than clinically significant cerebral ischemia, major ischemic cerebrovascular accidents were well studied because of clinical significance. 1 Silent neuronal injury is a common finding among patients with dementia. Even in asymptomatic patients without history of stroke, cranial infarcts may be observed incidentally in cranial imaging modalities. Its prevalence is 11% to 28% and increases with age. 2 More than half of the SNI belongs to the frontal cortex. Patients are usually asymptomatic but mild perception and behavioral disturbances may be present.
Coronary angiography (CAG) is established as the gold standard for the assessment of coronary artery disease (CAD). 3 Percutaneous coronary intervention (PCI) is a safe and effective alternative to coronary artery bypass graft surgery (CABG) and medical therapy. 4 However, postprocedural complications including stroke, myocardial infarction (MI), arrhythmia, vascular complications, dye allergy, hemodynamic derangements, and heart chamber perforation may occur due to PCI. 5,6 Symptomatic embolic cerebrovascular accident is a major complication of PCI. Retrospective data analysis revealed that 0.11% to 0.38% of patients undergoing CAG experienced clinically evident cerebral infarction 7 –9 while the incidence of SNI was 13% to 22%. 7,10,11 After cerebral angiography, SNI is described in 18.5% to 23% of patients. 12,13 Atherosclerotic thromboembolism due to catheter manipulation, thrombus formation at the catheter, air embolism, and contrast agent may cause cerebral injury. 8,13 –15
Neuron-specific enolase (NSE) is a neuronal cytoplasmic enzyme with a half-life of 48 hours. 16 The sensitivity and specificity of NSE for showing neuronal injury were reported as 55% to 80% and 95% to 98%, respectively. 17 The NSE level is correlated with the size of cerebral infarct and Glasgow coma scale. 18 –20
The SYNTAX score (SS) is a widely accepted CAD complexity score based on lesion morphology. The SS was correlated with cardiovascular mortality and morbidity. 20 Higher SS was correlated with poor outcome and major adverse cardiovascular and cerebrovascular events (MACCEs) in many studies. 21 –23
To date, limited data were available regarding the occurrence and predictors of SNI after CAG and PCI. Furthermore, the SNI secondary to PCI was not evaluated in patients presented with acute coronary syndromes (ACSs). The relationship between SS and SNI was not evaluated further. The aim of this study is to evaluate the incidence and predictors of SNI after CAG and PCI by serial measurement of serum NSE levels in patients presented with ACS.
Material and Methods
Study Design
From May 2012 to July 2012, 98 (75 men) patients presented with ACS and underwent CAG and PCI (52%) were included in this prospective study. Patients with recent cerebrovascular accident, intracranial hemorrhage, head trauma, central nervous system tumor, degenerative central nervous system disorders, schizophrenia, septic shock, pneumonia, neuroendocrine tumor, malignancy, Creutzfeldt-Jakob disease, Gullian Barre syndrome, CABG, peripheral vascular disease, hemodynamic decompensation, and requiring intra-aortic balloon pump were excluded from the study. The NSE levels were measured before and 18 hours after the CAG and PCI. Detailed neurological examination along with general physical examination was performed in each patient before, 24, and 48 hours after the procedure and before discharge. The neurological deficit was quantified by the use of the National Institutes of Health Stroke Scale. Consciousness was assessed and cranial nerve examinations were performed. Posture, muscle strength, and tone were evaluated. Deep tendon reflexes were checked. Sensory examination including light touch, pain, vibration, position sensing, and 2-point discrimination was evaluated. Dysmetria and dysdiadochokinesis were examined. All patients were neurologically intact before the enrollment. High-resolution cranial tomography examination was performed prior to discharge in patients with NSE levels above the cutoff value. All patients gave informed consent before enrollment and the study protocol was approved by the Ethics Committee.
Echocardiography Evaluation
Transthoracic echocardiography was performed in each patient after PCI. Left atrial diameter, left ventricular systolic and diastolic diameters, and left ventricular ejection fraction (EF) were recorded.
Neuron-Specific Enolase
Neuron-specific enolase was studied before and 18 hours after the PCI. Blood samples were analyzed by Cobas 601 immunologic analyzer (Roche Diagnostic, Mannheim, Germany) and Elecsys NSE kits (Roche Diagnostics, Mannheim, Germany) with electro-chemiluminisence immunoassay (electroemilumineson immunologic test) method. An NSE level above 17.0 mg/dL was accepted positive according to manufacturer’s instructions.
SYNTAX Score and CAG Data
All patients underwent CAG according to Judkins technique through standard femoral approach. Acetyl salicylic acid 300 mg, 600 mg loading dose of clopidogrel, and intravenous heparin of 70 units/kg were administered before the CAG. Acetyl salicylic acid, clopidogrel, heparin, statin, angiotensin-converting enzyme inhibitor, and β-blocker maintenance therapy were administered after the CAG and PCI according to current guidelines. 23 The left main, left anterior descending, circumflex, and right coronary arteries were defined as major coronary vessels. Each coronary lesion producing ≥50% luminal obstruction in vessels with a diameter of ≥1.5 mm was separately scored and added to provide the vessel SS and then summed to provide the overall SS of the patients (www.Syntaxscore.com). The SS was calculated using dedicated software (version 2.11) that integrates the number of lesions with their specific weighting factors based on the amount of myocardium distal to the lesion and the morphologic features of each single lesion. The SS was divided into 2 tertiles as follows: the upper boundary of the lowest tertile was 22 (low risk) and the lower boundary for the highest tertile was 33 (intermediate-high risk). All angiograms were scored by 2 experienced investigators who were blinded to echocardiography and NSE data. Patients with critical stenosis of coronary arteries which were suitable for PCI underwent PCI in the same session. Duration of procedure and total fluoroscopy time were also recorded.
Clinical and Laboratory Data
For each patient, vascular risk factors, including hypertension, diabetes mellitus, hypercholesterolemia, smoking status, and history of ischemic stroke, were obtained. Patients with blood pressure ≥140/90 mm Hg at 2 occasions or on antihypertensive medication were accepted as hypertensive. 24 Diabetes mellitus was defined as fasting blood glucose >126 mg/dL or patients on oral antidiabetic or insulin therapy. 25 Hypercholesterolemia is accepted as fasting low-density lipoprotein (LDL) level >160 mg/dL or patients on antihyperlidemia therapy. 26 The laboratory data that were measured before CAG (on the day of admission) were recorded. The laboratory data include blood cell counts, fasting glucose, total cholesterol, LDL, urea, and creatinine. Height and weight of patients were recorded and body mass index was calculated. The estimated creatinine clearance rate was calculated according to Cockroft and Gault formula.
Statistical Analysis
SPSS 17.0 statistical software (SPSS Inc, Chicago, Illinois) was used for statistical analysis. Continuous variables were expressed as means ± standard deviation, and categorical variables were expressed as percentages. The Kolmogorov-Smirnov test was used to test the normality of distribution of continuous variables. Group means for continuous variables were compared using Student t-test or the Mann-Whitney U test as appropriate. Categorical variables were compared using the chi-square test. Repeated measure test was used for dependent variable analyses. Logistic regression analysis was used to find independent associates of SNI. The sensitivity and specificity of SS to predict SNI were determined by receiver–operator curve (ROC) analysis. Results were evaluated between the 95% confidence interval (CI), and P < .05 was accepted significant.
Results
All patients underwent CAG. Baseline patient characteristics are shown in Table 1. None of the patients had transient ischemic attack or stroke during hospital stay. All patients were neurologically intact during hospital stay. Of the 98 patients, 18 (18.4%) patients presented with unstable angina pectoris, 49 (50.0%) with non-ST-segment elevation MI, and 31 (31.6%) patients with ST-segment elevation MI (17 patients with anterior MI and 14 patients with inferior MI). Percutaneous coronary intervention was performed in 51 (52%) patients. Silent neuronal injury was detected in 31.6% (31) of patients. Of these 31 patients, 16 patients had microinfarcts in high-resolution computed tomography examination. The NSE levels (22.03 ± 27.70 vs 10.08 ± 3.15, P = .002) significantly increased 18 hours after the CAG (18.56 ± 29.77 vs 9.93 ± 2.84, P = .05) and PCI (25.23 ± 25.38 vs 10.21 ± 3.44, P < .001) compared to basal levels. Age, gender, presence of atrial fibrillation, and frequency of coronary risk factors including smoking, diabetes, hypertension, and hypercholesterolemia were similar between patients with SNI and those without. Laboratory and echocardiographic data are shown in Table 2. Left ventricular EF in the SNI+ group was significantly lower than that of the SNI− group (43.71% ± 12.51% vs 50.84% ± 9.34%, P = .002). Although the mean fluoroscopy time of the SNI+ group was higher (6.37 ± 4.23 minutes for SNI+ vs 4.70 ± 4.16 minutes for SNI−, P = .069), it was not significant. Maximal creatinine kinase myocardial band (CK-MB) and troponin I levels of the SNI+ group were significantly higher than those of the SNI− group (103.83 ± 99.22 vs 51.92 ± 78.33, P = .006 and 50.04 ± 66.18 vs 19.18 ± 30.50, P = .002 successively). The SS was significantly higher in the SNI+ group (28.13 ± 14.68 vs 18.71 ± 13.23, P = .002; Figure 1). Of the 98 patients, 51 (52%) patients had SS > 22, and SNI was significantly higher in patients with SS > 22 than in patients with SS ≤ 22 (41.18% vs 21.28%, P = .034).
Characteristics of Patients.
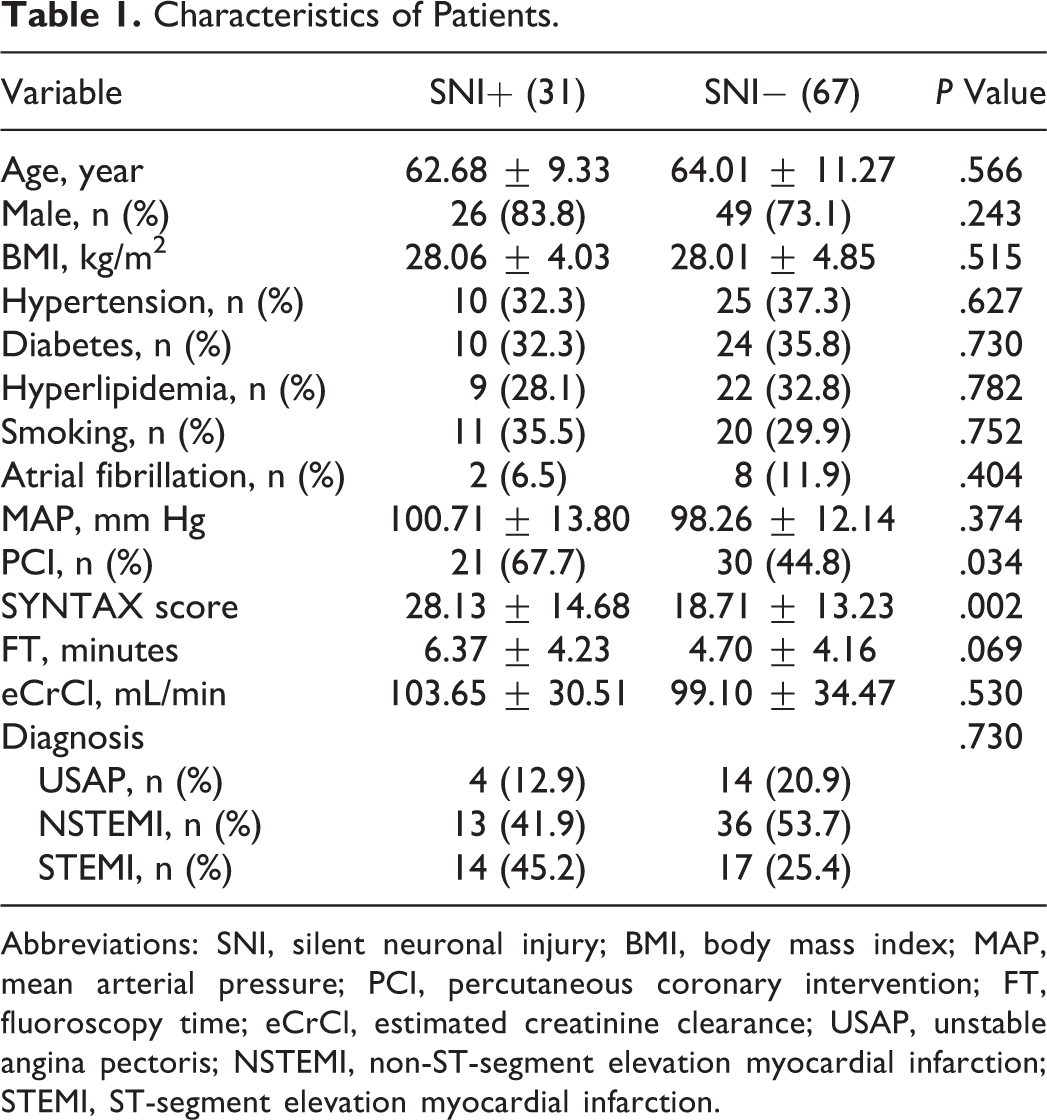
Abbreviations: SNI, silent neuronal injury; BMI, body mass index; MAP, mean arterial pressure; PCI, percutaneous coronary intervention; FT, fluoroscopy time; eCrCl, estimated creatinine clearance; USAP, unstable angina pectoris; NSTEMI, non-ST-segment elevation myocardial infarction; STEMI, ST-segment elevation myocardial infarction.
Echocardiographic and Laboratory Data of Patients.
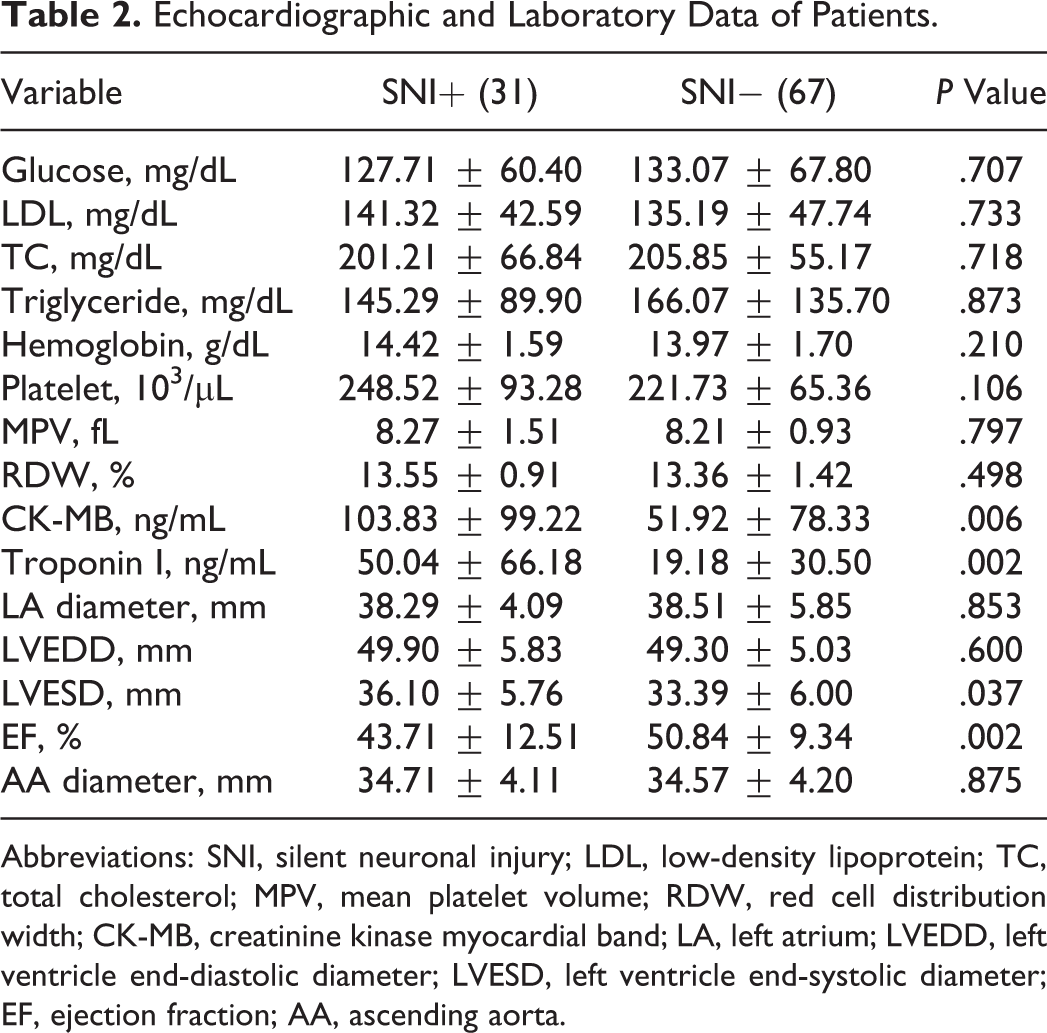
Abbreviations: SNI, silent neuronal injury; LDL, low-density lipoprotein; TC, total cholesterol; MPV, mean platelet volume; RDW, red cell distribution width; CK-MB, creatinine kinase myocardial band; LA, left atrium; LVEDD, left ventricle end-diastolic diameter; LVESD, left ventricle end-systolic diameter; EF, ejection fraction; AA, ascending aorta.
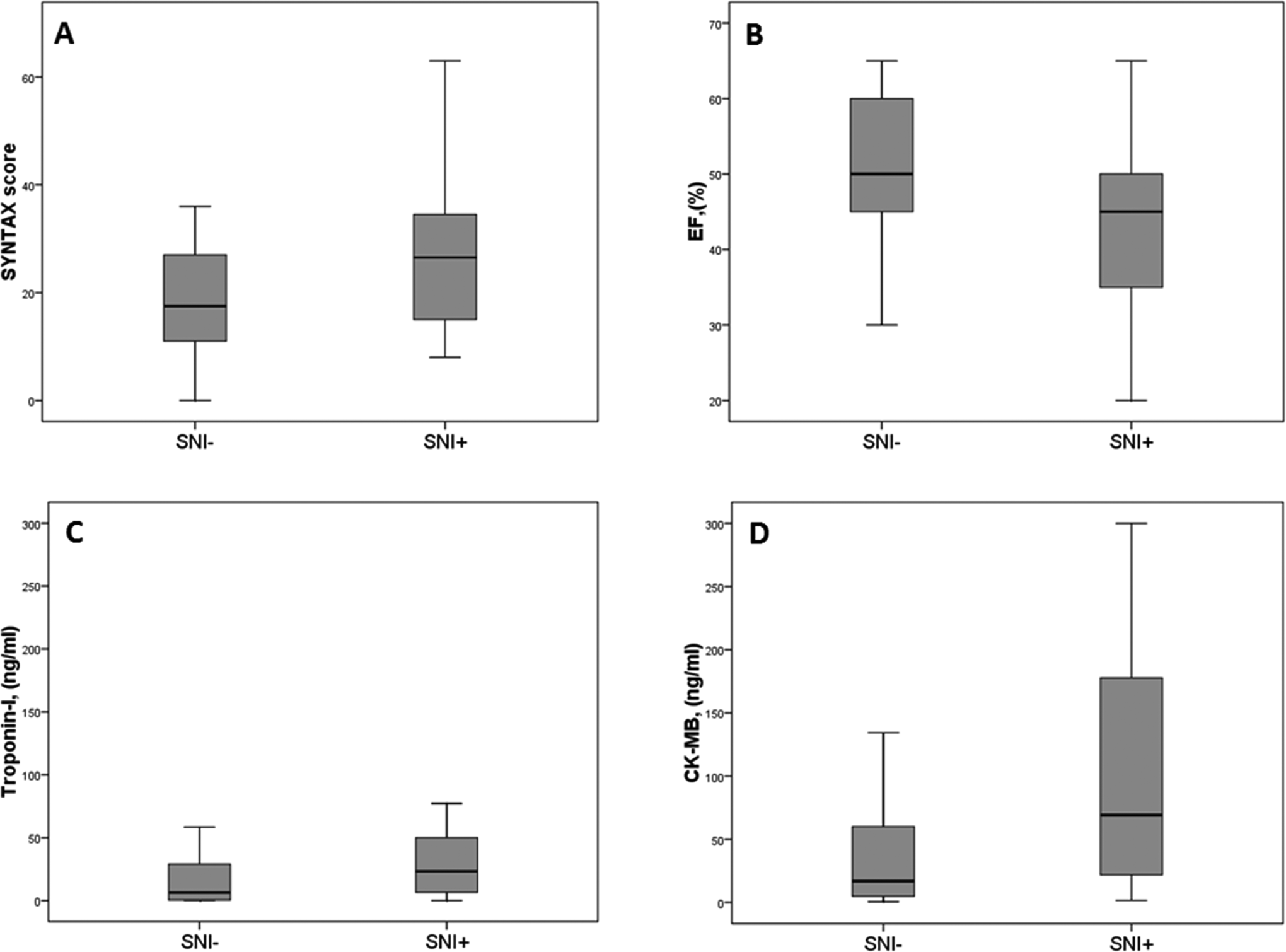
Box plot showing the (A) SS, (B) EF, (C) troponin I, and (D) CK-MB of SNI+ and SNI− groups. SS indicates Syntax score; EF, ejection fraction; CK-MB, creatinine kinase myocardial band; SNI, silent neuronal injury.
Although the SS and left ventricle end-diastolic diameter were significantly higher, EF was significantly lower in patients with SNI who underwent CAG than those without SNI (Tables 3 and 4). The SS, CK-MB, and troponin I levels were significantly higher in patients with SNI in whom PCI was performed than in patients without SNI.
Clinical Features of Patients Who Underwent CAG and PCI.
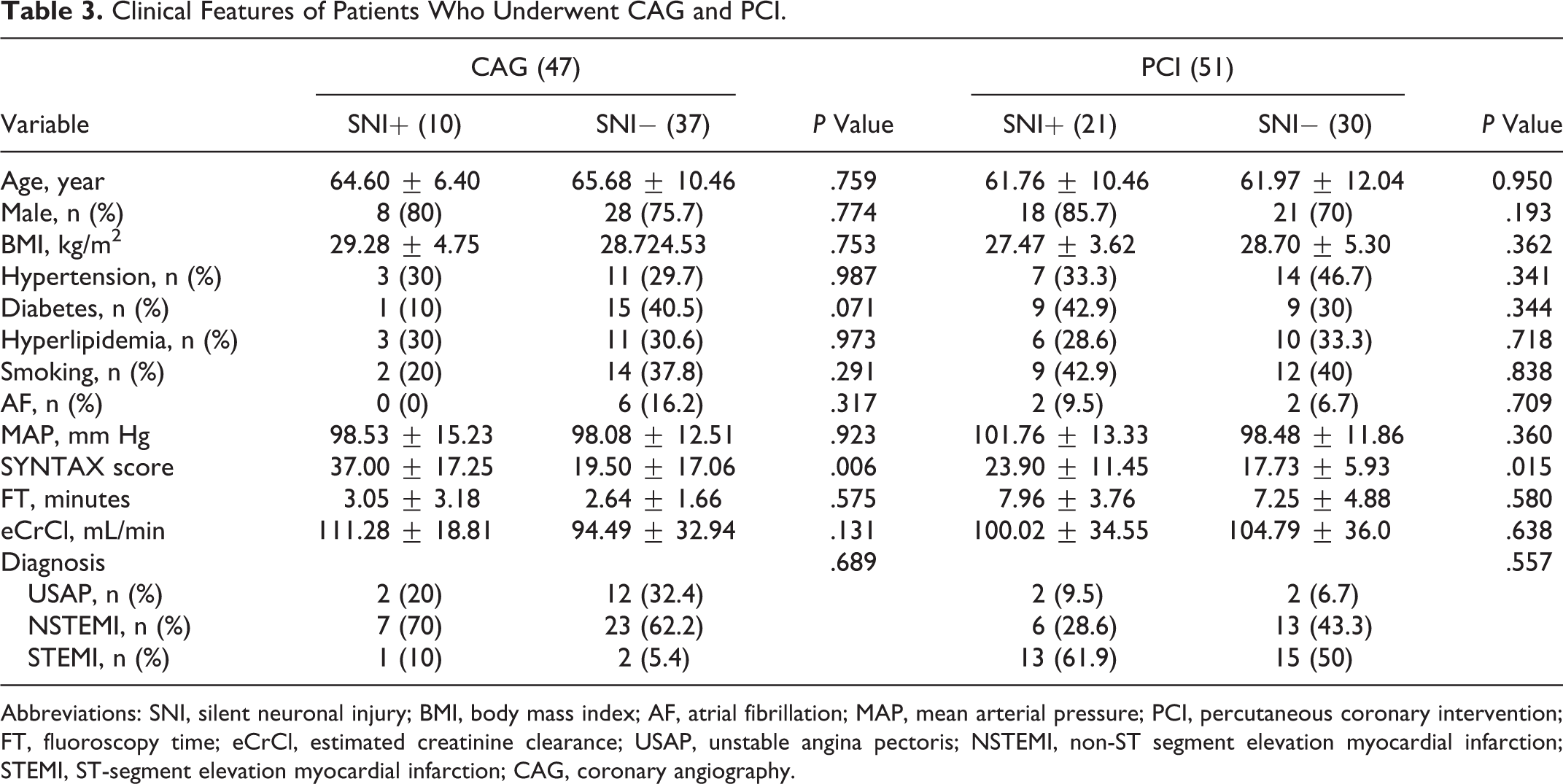
Abbreviations: SNI, silent neuronal injury; BMI, body mass index; AF, atrial fibrillation; MAP, mean arterial pressure; PCI, percutaneous coronary intervention; FT, fluoroscopy time; eCrCl, estimated creatinine clearance; USAP, unstable angina pectoris; NSTEMI, non-ST segment elevation myocardial infarction; STEMI, ST-segment elevation myocardial infarction; CAG, coronary angiography.
Laboratory and Echocardiographic Variables of Patients Who Underwent CAG and PCI.
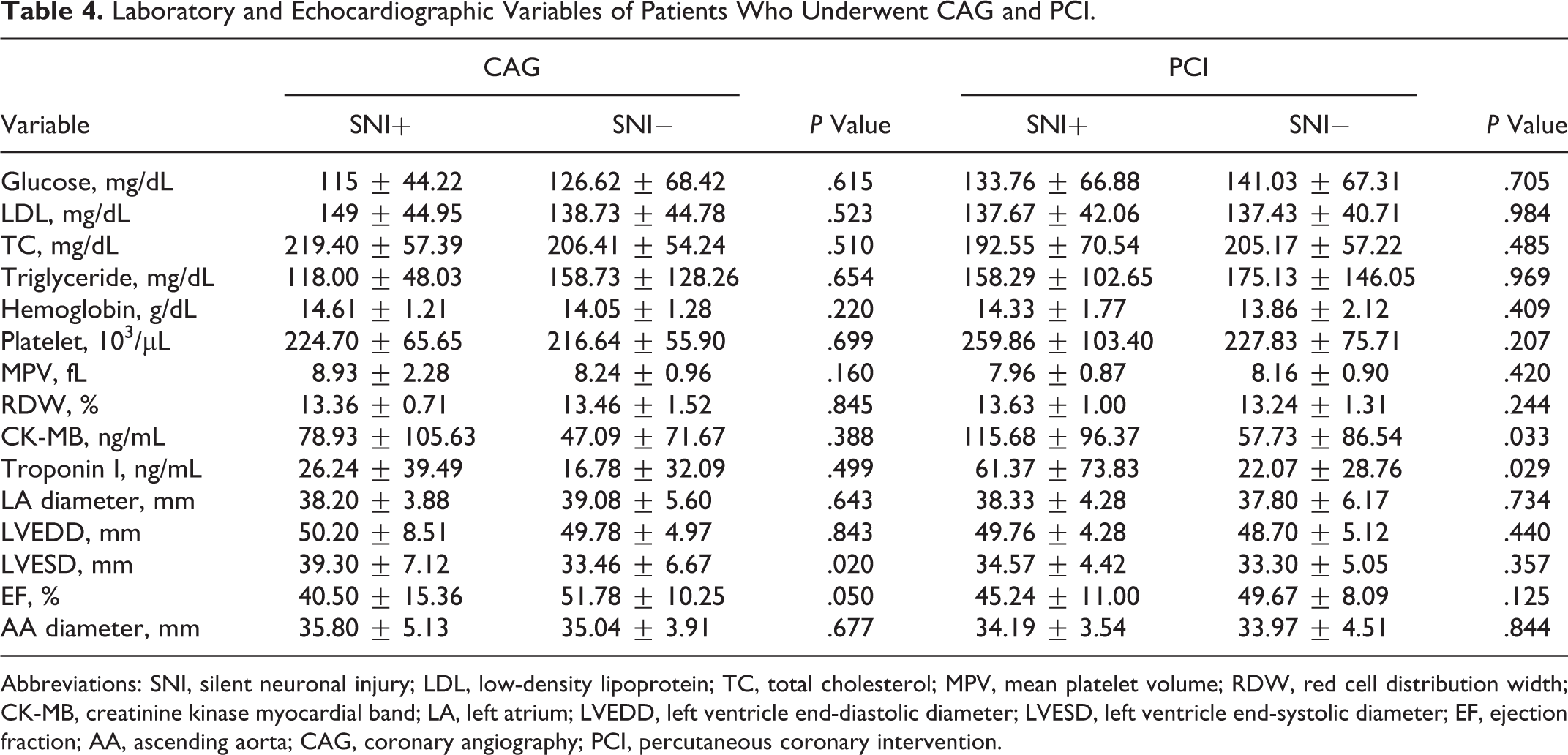
Abbreviations: SNI, silent neuronal injury; LDL, low-density lipoprotein; TC, total cholesterol; MPV, mean platelet volume; RDW, red cell distribution width; CK-MB, creatinine kinase myocardial band; LA, left atrium; LVEDD, left ventricle end-diastolic diameter; LVESD, left ventricle end-systolic diameter; EF, ejection fraction; AA, ascending aorta; CAG, coronary angiography; PCI, percutaneous coronary intervention.
Independent Predictors of SNI
SYNTAX score and performing therapeutic PCI were the independent predictors of SCI in logistic regression analysis (P = .009, odds ratio [OR] = 1.06, 95% CI = 1.014-1.107 and P = .036, OR = 4.262, 95% CI = 1.097-16.56; Table 5).
Results of Logistic Regression Analysis.
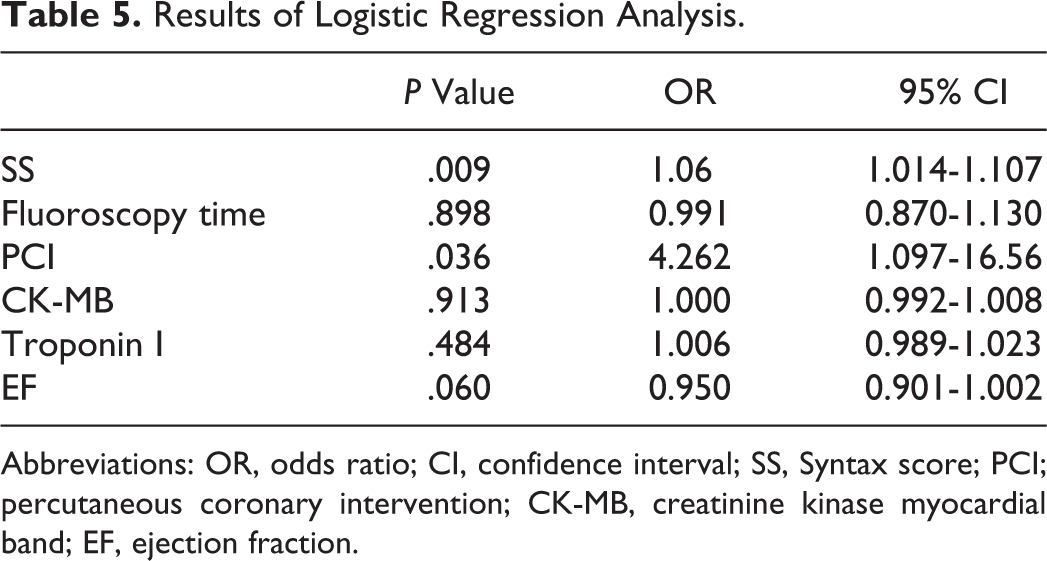
Abbreviations: OR, odds ratio; CI, confidence interval; SS, Syntax score; PCI; percutaneous coronary intervention; CK-MB, creatinine kinase myocardial band; EF, ejection fraction.
The sensitivity and specificity of SS ≥ 32 for predicting SCI were 71% and 92%, successively, in ROC analysis (P = .005, area under the curve = 0.677, 95% CI = 0.563-0.791, Figure 2).
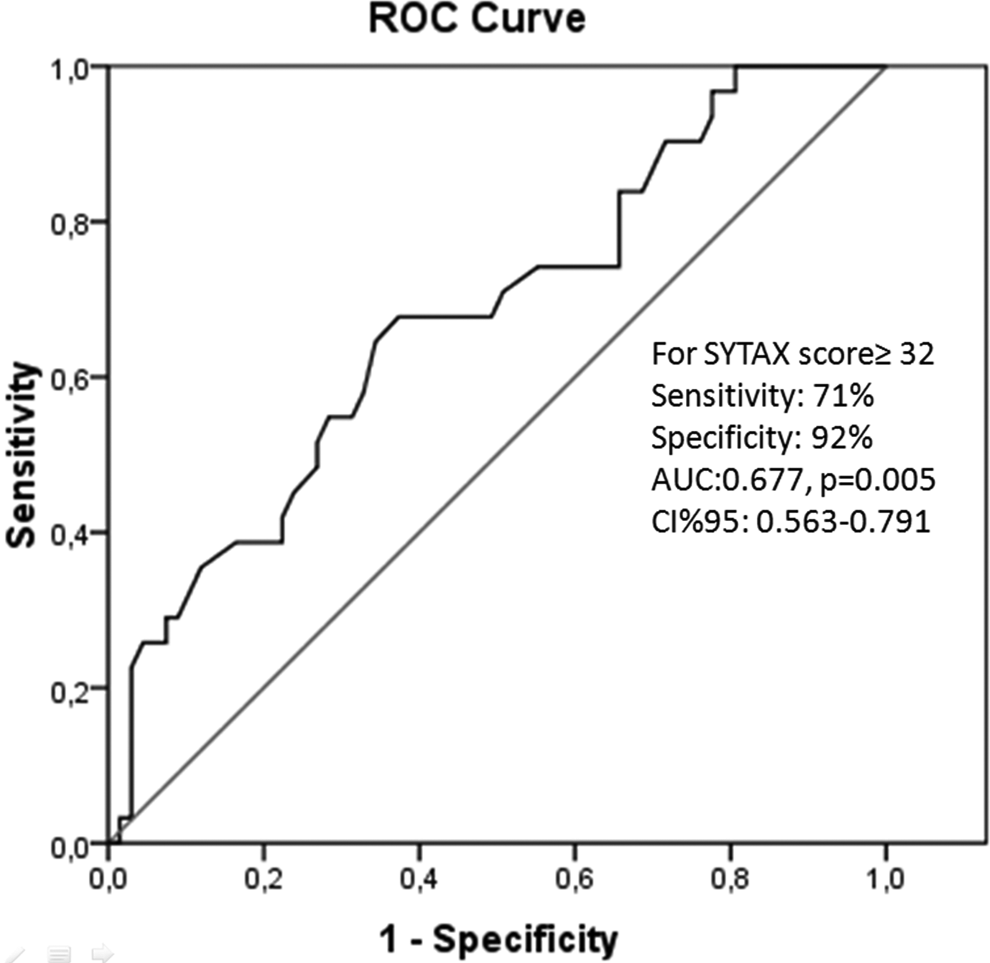
Receiver–operator curve (ROC) shows the sensitivity and specificity of SS to predict SNI. SS indicates SYNTAX score; SNI, silent neuronal injury.
Discussion
We have found that 31.6% of patients presented with ACS developed SNI. The SS, left ventricular end-systolic diameter, cardiac troponin I, and CK-MB were significantly higher, while left ventricle EF was significantly lower in patients with SNI. Percutaneous coronary intervention was also an important determinant of SNI. The SS and PCI were the independent predictors of SNI in logistic regression analysis.
Percutaneous coronary intervention is an invasive procedure associated with several postprocedural complications including cerebrovascular accident. 5,6 Cerebrovascular accident is one of the major causes of disability and death. Clinically apparent cerebrovascular accidents occur in 0.11% to 0.38% of cases after CAG and PCI. 7 –9 However, SNI after the CAG and PCI is inadequately evaluated. Furthermore, to our knowledge SNI after CAG and PCI in patients with ACS is not investigated. The incidence of SNI after cerebral angiography has been reported to be 18.5% to 23%. 12–13 It has been shown that 11% to 12% of patients after CAG developed SNI. 7,11 The SCI was observed in 22% of patients with aortic stenosis after diagnostic catheter procedures. 10 Busing et al reported that SNI was twice common after PCI (23%) compared to CAG (11%), but it was not statistically significant. In their series, a total of 48 patients were included and PCI was performed in 13 patients. 7 Similarly, we have found that PCI significantly increased the risk of SNI (OR: 4.26, P = .036) compared to CAG. The increased frequency of SNI may be related to the sensitivity of NSE in our study. Furthermore, our study population was larger (includes 98 patients) and PCI was performed in 51 patients.
Decreased cerebral perfusion secondary to prolonged hypotension may be another reason for brain injury. 27 However, we followed patients at coronary care unit under close hemodynamic monitorization and there were no episodes of significant systemic hypotension.
Former studies evaluated the SNI after CAG by magnetic resonance imaging (MRI). 7,10,11 Although MRI is the most sensitive noninvasive cerebral anatomical examination method available, it is reasonable to suppose that morphological abnormalities smaller than an MRI pixel size, which is 2.0 to 1.8 mm2, will not be detected. It is, therefore, probable that the degree of acute cerebral injury may be more extensive than that visualized by diffusion-weighted MRI. Therefore, the reported incidence of SNI 11% to 12% was underestimated. This view is supported by the findings of Brown et al who performed neuropathological examinations in patients who died after cardiopulmonary bypass and showed that extensive cerebral pathological findings with thousands of small capillary and arteriolar dilatations caused by microembolization. 28 Moreover, Lund et al reported that microembolization to cerebral circulation was common in elective left heart catheterization. 11 In their series, cerebral microembolization (92.1% gaseous and 7.9% solid) was observed in all patients demonstrated by transcranial Doppler ultrasonography.
Multivessel CAD, depressed EF, female gender, and left ventricular hypertrophy are the risk factors for the development of complications after CAG. 29 In our study, although the EF was significantly lower in patients with SNI, it was not an independent predictor of SCI in logistic regression analysis. Performing internal mammary artery angiography also increases the risk of SNI. 30 But we did not perform internal mammary artery angiography in this study. Busing et al reported that duration procedure was associated with SNI after CAG. 7 Moreover, Omran et al and Bendszus et al reported that fluoroscopy time was correlated with SNI in patients who underwent cerebral angiography. 10,13 But the same correlation of duration of fluoroscopy time and SNI was not observed in our study. Additionally, plaque mobilization from the ascending aorta or the aortic arch, thrombosis of the tip of the catheter, and an air embolism should be considered. 13,15 The risk of thrombus formation and vascular plaque mobilization may increase with the prolongation of the procedure. Furthermore, ACS is a hypercoagulable state, thus the in situ thrombus formation in cerebrovascular tree could not be excluded in our study.
Atherosclerosis and arteriolosclerosis affect vascular tree. Ischemic cerebrovascular accident is associated with atherosclerosis. 31 The SS is a widely accepted CAD complexity score based on lesion morphology. Higher SS was correlated with poorer outcome and MACCEs. 21 –23 The association between SS and SNI was not evaluated previously. We have found that SNI occurred significantly higher in patients with higher SS. This finding may be attributable to patients with higher SS who had excessive atherosclerotic burden, calcification, and complexity not only in coronary vasculature but also in aorta, carotid, and cerebrovascular arteries. Moreover, the procedural difficulty is more pronounced in patients with higher SS requiring longer procedural time, excessive catheter manipulations, and difficulty in engagement of coronaries. Increased vascular stiffness is associated with SNI. 32 Therefore, patients with higher SS may be prone to excessive aortic injury secondary to catheter manipulations of vulnerable aorta.
All of our catheterization procedures were carried out at a high volume center where more than 5000 diagnostic and 2000 therapeutic interventions are performed per year so lack of qualification could be excluded.
Silent neuronal injury is considered as a precursor of symptomatic stroke. The presence of SNI at MRI increases the risk of dementia which is associated with worse performance on neuropsychological tests with a steeper decline in global cognitive function. 33 Although the patients with SNI had no evidence of neuropsychological complications during the follow-up period in this study, longer and more careful follow-up will be needed in this patient subset.
Complications following percutaneous interventions in particular embolic complications are an important topic concerning many patients. Different efforts are made to minimize the risk of embolic complications like antithrombotic pharmacotherapy and embolic protection devices, but it still exists. However, there is insufficient data in the literature regarding the embolic protection of the cerebrovascular system after percutaneous intervention.
Study Limitations
The present study has several potential limitations. First, study populations included patients with ACS who mainly had significant CAD. The risk of SNI after PCI therefore may be overestimated. Second, MRI was not performed which is the gold standard diagnostic imaging modality for the evaluation of cerebrovascular injury. Neuron-specific enolase is affected by hemolysis, thus catheterization-related hemolysis may overestimate the results further. Assessment of psychological tests may provide additional information.
Conclusion
Percutaneous coronary intervention and coronary artery lesion complexity may increase the risk of SNI which is associated with deterioration in cognitive functions and dementia in patients with ACS. This silent complication should be considered after PCI.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.