
Abstract
Women with mild bleeding disorders (MBDs) pose a diagnostic challenge and menorrhagia, the most common presenting symptom that remains underreported. We tested the hypothesis that screening apparently normal females using general and gynecological bleeding assessment tools and a global hemostatic assay together with platelet aggregation can help predict MBDs. We assessed 47 women using electronic bleeding assessment tools; e-bleeding questionnaire; and e-Pictorial Bleeding Assessment Chart (e-PBAC) based on previously validated methods, thrombelastography (TEG), and platelet aggregation together with basic coagulation testing. Three women had elevated bleeding score with von Willebrand disease diagnosis confirmed in one case and eleven cases had elevated e-PBAC. We report normal ranges for TEG and platelet aggregation in women during the first half of the menstrual cycle and show 23.4% of apparently normal women may have general or heavy menstrual bleeding. This is a prelude to a larger study to determine the validity of bleeding assessment tools in screening for MBDs in women.
Introduction
Mild bleeding disorders (MBDs) may pose a diagnostic challenge and need to be given special consideration. Patients often present with a variety of clinical and laboratory indicators that can result in diagnostic uncertainty for both physicians and specialists. In more than 50% of the studies, 1,2 von Willebrand disease (VWD) appears to be the most common MBD, followed by platelet function defects (PFDs). However, some studies reported PFDs to be most common in patients with unexplained heavy menstrual bleeding (HMB). 3 Of the women diagnosed with VWD, HMB is present in 4 74% to 92% and 5% to 20% of women present with HMB as their primary symptom for VWD. 5 In general, HMB remains underreported in females who often compare similar menstrual bleeding patterns within families. Due to the subjective nature of menstrual bleeding and its severity, calls have been made to develop tools to measure menstrual blood loss objectively.
Accurate assessment of bleeding symptoms is fundamental to the successful diagnosis and management of MBD. Although less likely to precipitate spontaneous bleeding, MBDs can become particularly severe after major hemostatic challenges such as surgery, trauma, or childbirth and can be potentially life threatening. Quantitation of bleeding symptoms using standardized bleeding questionnaires that produce valid bleeding score (BS) has proven to be useful in the diagnosis of MBDs over the past several years. 6 –8 Considerable variation in hemostasis exists in normal population and in several factors such as age, 9 gender, 10,11 smoking, 12,13 menstrual cycle, and 4,14 oral contraceptives. 15,16 Surgical stress, venipuncture as well as hormonal levels 14,17 are also known to be implicated. If not carefully considered and well controlled for, this variation may affect the interpretations of the results of coagulation tests and subsequently the clinical as well as the research outcomes.
The scientific consensus defines HMB as blood loss greater than 80 mL. A simple and standard terminology has been recommended for the description and definition of symptoms and signs of abnormal uterine bleeding and the term HMB has been recommended to replace the historically known and used menorrahgia. 18,19 Several methods have been reported to evaluate this; a semiquantitative method widely accepted is the Pictorial Bleeding Assessment Chart (PBAC) where sanitary material (tampons and pads) are assigned a numerical value based on the degree of saturation to measure menstrual blood loss. A PBAC score of >100 is equivalent to >80 mL of menstrual blood loss. 20 Although there are advantages and disadvantages to using a pictorial chart, an alternative is the much more complicated alkaline hematin test. It involves collection of used sanitary wear and subsequent blood extraction and analysis. Not only is the PBAC simpler, it is also more cost effective and has been found to correspond well with the alkaline hematin test. Additionally, PBAC has been proven superior compared to patient’s verbal history. 21 Due to the semiobjective nature of the PBAC, some studies have found that the number of tampons worn correlates with personal hygiene more than with menstrual blood loss. 22 However, the sensitivity of the test is 86% and specificity is 89%, 20 which makes it an important tool in the detection of HMB. The PBAC has been validated for use in clinical practice. 23 According to Warner et al, 3 features have been considered of relatively high specificity for HMB: the concurrent iron deficiency, the assessment of pad changing frequency together with the documentation of passing clots. 24
It is reported that 10% to 15% of women with HMB have an underlying bleeding disorder. In the absence of gynecological causes, HMB can reflect the presence of a hemostatic disorder. Since it is the most common presenting symptom of MBD, it is important to quantify both general and menstrual blood loss.
An extensive bleeding questionnaire was developed in 2006 and was validated for the diagnosis of VWD type 1 as a part of a European study known as Molecular and clinical markers for diagnosis and management of type 1 von willebrands disease (MCMDM-1VWD). 8 A condensed version 6 of this questionnaire was created in 2008 and validated for the diagnosis of VWD and showed an excellent correlation with the extensive version. Moreover, the condensed version had a sensitivity of 100% and a specificity of 87%. This same questionnaire was modified and validated in 2009 for use in the pediatric population and has shown a diagnostic utility in this population. 25
Mild bleeding disorders are difficult to diagnose and require exhaustive and expensive list of investigation. In this study, we tested the hypothesis that screening apparently normal females with general and gynecological bleeding assessment tools and a global hemostatic assay together with platelet aggregation can help predict MBD.
We developed an electronic bleeding questionnaire (e-BQ) based on the previously validated paper-based version 6 and an electronic PBAC (e-PBAC) based on the paper-based one 20 developed in 1990. The electronic tools were developed to enhance the effectiveness of analysis of a large number of normal women. We used thromboelastography (TEG), an established global hemostatic test as well as a standard whole-blood aggregation test together with basic hematological and hemostasis testing. We show that 23.4% of apparently normal women have elevated BS and/or PBAC. We report normal ranges for TEG parameters and platelet aggregation in women during the follicular phase of menstrual cycle. Although TEG and aggregation did not distinguish clearly between bleeders and nonbleeders, some correlations were observed between BS and/or PBAC with maximum amplitude (MA) parameter and platelet aggregations indicating the potential usefulness of these as screening tools for MBD.
Material and Methods
Participants, Recruitment Process, and Study Outline
The study was conducted at St Lawrence College in Ontario, Canada, following the approval of the Research Ethics Board within the institution. Through the use of the institution’s e-mail system, a call for participation was sent out to the college community. Informed written consent was obtained from all participants, consisting of student body, staff, and faculty. Inclusion criteria were females within the age of 18 to 47 years who had no personal or family history of diagnosis of a bleeding disorder. A total of 60 participants were initially recruited, 10 did not complete the study, and 50 were investigated. The study was conducted in 3 steps: the first included a 10-minute interview to obtain a personal and family medical history and to fill out the e-BQ. In the second step, each participant was asked to chart a menstrual cycle online utilizing the e-PBAC. The third and final step included a 10-minute appointment to collect a morning fasting sample of 30 mL blood by venipuncture on day 7 to 9 of the menstrual cycle. Participants were further subdivided into oral contraceptive users and nonusers. Three participants were excluded from the study due to a personal or family history of a bleeding disorder. One participant’s father had been diagnosed with hypofibrinogenemia, another participant’s mother and maternal uncle had been diagnosed with factor V Leiden, and 1 participant’s mother was diagnosed with idiopathic thrombocytopenic purpura. All participants were free from aspirin, ibuprofen, and selective serotonin reuptake inhibitors for 7 days prior to blood withdrawal. All interviews were conducted and e-BQs were filled out and blood samples were withdrawn by a trained registered nurse. Whole blood was used for conventional and global hemostatic tests as well as platelet aggregation. Figure 1 shows an outline of the study.
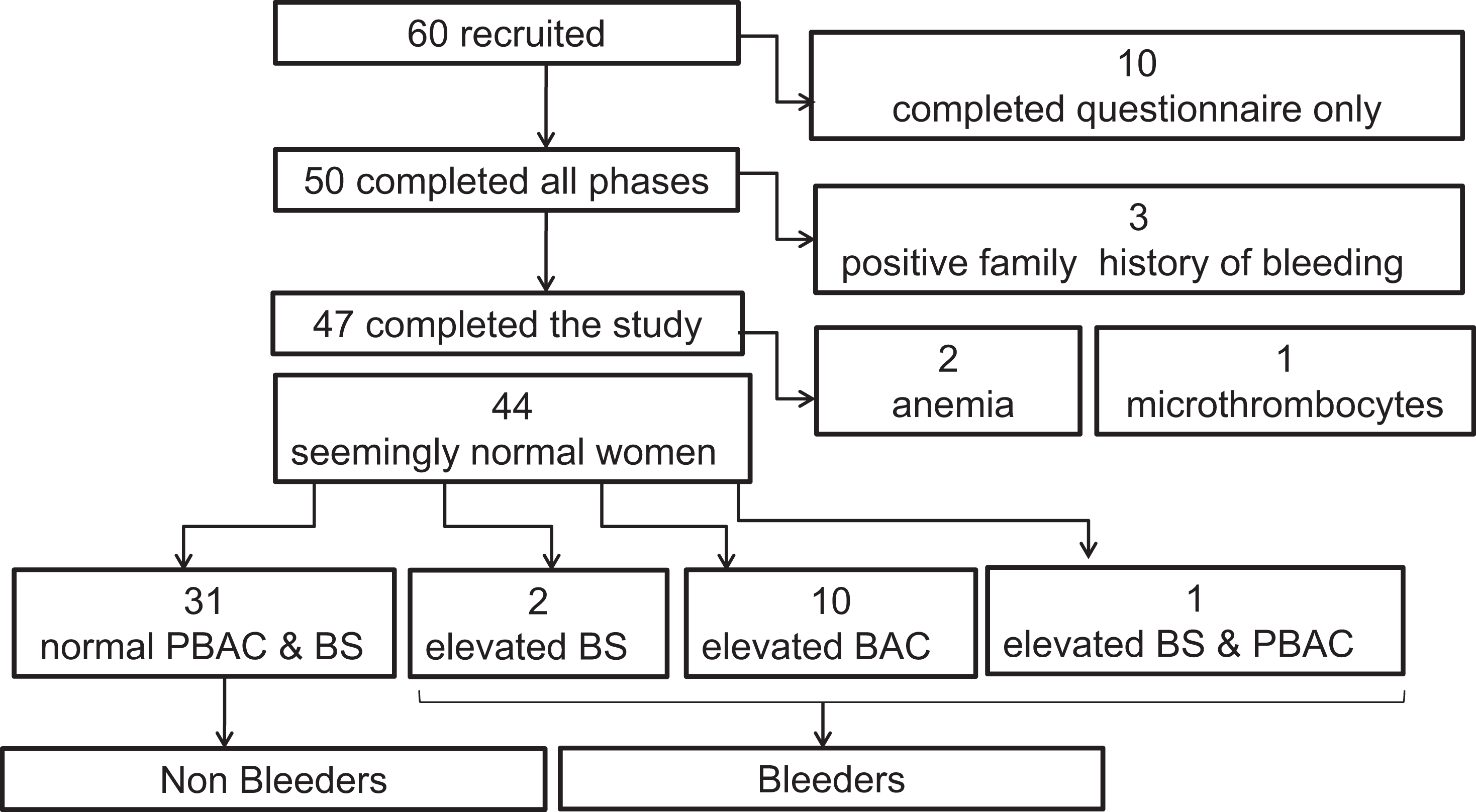
Recruitment of participants and study outline.
Electronic Bleeding Questionnaire
The development of the e-BQ was based on the condensed MCMDM-1questionnaire paper version. The questionnaire is accessed using any Web browser that is cross platform compatible. It is stored on a local computer and is security enabled using enterprise class 128-bit data encryption, with access to the data protected by a user-defined password. The researcher can find and manipulate records within the database from the main screen. A unique participant identification (ID) and randomized password are generated with each participant record, which, at a later date, was used by the participant to access the online version of the e-PBAC. Each field within the questionnaire is coded to accept only the appropriate data (text or numerical). This approach allows data to be validated at the point of entry and also facilitates data entry and analysis by preventing the addition of corrupted or inaccurate data. Tight data controls allow us to automatically calculate a reliable BS upon completion of the questionnaire. The e-BQ was an exact representation to the published paper-based version using the same scoring −1 to 4. Minor modifications were made on few occasions (postdental bleeding, bleeding after surgery, and postpartum hemorrhage) to adjust for the electronic format and to further clarify the questions posed. The e-BQ link can be accessed at http://pt-vwd.org/ebq/aID. The following is an ID and pass code the reader can use as a representation ID: CUVC7Y, Pass code: 1e5ca8d1a64936b.
Electronic PBAC
The development of the e-PBAC was based on the previous paper version 20,21 and is accessed via the Internet. Study participants were presented with a calendar interface to record their daily menstrual data on the month that followed their e-BQ. Access was gained using the unique participant ID number and password generated from the eBQ. No participant demographics were stored on the Internet. A PBAC score of >100 is considered an indicator of HMB.
Thromboelastography
Thromboelastography is a global hemostatic assay that analyzes the kinetics of clot formation and dissolution from the time of initial fibrin formation to fibrinolysis. The technique has been available since the 1940s but only in the last decade has it shown great impact within the clinical practice arena. The TEG measures the interactive dynamic coagulation process from the initial fibrin formation to platelet interaction and clot strengthening to fibrinolysis, which makes it superior to other conventional tests. This test utilizes a recalcified citrated whole blood sample and generates a trace with different parameters reflecting the whole hemostatic process. These tests were performed at Queens University’s research laboratory.
Briefly, blood samples were collected by venipuncture using 21-gauge needles, into 1.8-mL Vacutainer tubes (Becton Dickinson, Canada with 3.2%sodium citrate (0.105 mol/L trisodium citrate). Blood sample of 340 μL was transferred to a 37°C prewarmed disposable cup containing 20 μL calcium chloride and TEG was run for 1 hour for each patient. Five parameters were assessed: R (n = 9-27 minutes, time to initial fibrin formation), α angle (22°-58°, α angle, rate of clot formation), MA (n = 44-64 mm, MA, absolute clot strength), coagulation index (CI; n = −3 to +3, derived from R, K, α, and MA), and LY30 (n = 0%-8%, fibrinolysis at 30 minutes after MA). Maintenance and quality controls were performed daily in strict accordance with manufacturer recommendations, and all tests were performed by the same operator.
Whole Blood Aggregation
This analyzer tests platelet aggregation in whole blood specimens utilizing impedance Aggregometry in response to platelet agonists. In this study, we tested for three 3 major platelet agonists: adenosine diphosphate (ADP), collagen, and ristocetin using the Chrono-Log® Model 591/592 Whole Blood Aggregometer (Chronolog, USA). According to the manufacturer's instructions, the blood specimen was drawn with minimum trauma or stasis at the venipuncture site and anticoagulated with 3.2% sodium citrate (0.105 mol/L trisodium citrate). Testing of the specimen was conducted within the allotted time of up to 1 hour from initial collection, and 500 μL of whole blood was pipetted into a 37°C prewarmed cuvette containing 500 μL of saline and a stir bar. The contents were then warmed for 5 minutes in the incubation well. During the warming time, the Aggrolink WBA program was selected and participant data inserted. Once the aforementioned process was completed, the cuvette was moved to the reaction well, the electrode was inserted, and the baseline was set. Once the green status indicator became steady green and the baseline returned to 0, the appropriate agonist was added: collagen (5 μg/mL), ristocetin (1 mg/mL), or ADP (20 μmol/L). The test ran for 6 minutes and each test was conducted in triplicate. Daily normal control was performed to ensure validity of the aggregation testing. These tests were performed at St Lawrence College research laboratory.
Complete Blood Count
A complete blood count was performed using an EDTA blood sample and standard automated analyzer for each participant as a basic screening test offering valuable diagnostic hemostatic information. The study analyzed the participants’ hemoglobin (reference range 120-160 g/L), hematocrit (reference range 0.370-0.470), reflecting the red blood cell mass, platelet count (reference range 150.0-450.0 × 103/μL) being an integral component in assessing bleeding disorders, and mean platelet volume (reference range 7.0-11.0 fl) which indicates uniformity of size of the platelet population. This test was performed at St Lawrence College hematology laboratory.
Statistical Analysis
Student t test was used to compare TEG parameters and aggregation to different platelet agonists in bleeders and nonbleeders and in oral contraceptive users and nonusers. P < .05 was considered significant. Spearman correlation test was used to assess the relationship between various TEG parameters and various aggregation results with each of BS and PBAC scores in bleeders and nonbleeders and in oral contraceptive users and nonusers.
Results
Electronic Tools: Classification of Study Participants and General Findings
Following assessment of the 47 participants, women who had normal BS and normal PBAC were considered healthy and identified as “nonbleeders.” Women with elevated BS or PBAC score were identified as “bleeders.” Participants who had any prior personal or family history of bleeding were excluded from the study. Accordingly, the study participants were grouped as 31 nonbleeders (BS ≤ 4) and 13 bleeders (elevated BS and/or PBAC). The analysis of 47 participants showed 3 (6.4%) with an abnormal BS: 5 to 7 (normal = −1 to +4), 11 (23.4%) with an abnormal e-PBAC scores: 105 to 744 (normal ≤ 100), and 1 (2.1%) with a combined abnormal BS and e-PBAC score.
We calculated the sensitivity and specificity of e-BQ in order to assess its effectiveness in predicting HMB. The e-BQ had a sensitivity of 9.1%, while it maintained a specificity of 93.9% with a positive predictive value and a negative predictive value of 0.33 and 0.76, respectively. These data indicate that the e-BQ may not be useful in detecting bleeders when they have HMB alone but rather perhaps multiple symptoms. The combination of both e-BQ and PBAC to assess bleeding in females would be recommended.
All 11 participants with elevated PBAC were then referred to a gynecologist at Kingston General Hospital (KGH). Only 3 of 11 responded to the referral and attended the clinic; they were fully investigated. The following diagnoses were made: adenomyosis in 1 woman and unexplained menorrhagia in 2 women. All 3 participants with elevated BS were referred to a hematologist at KGH for further investigation. Demographic data of all study participants are shown in Table 1.
Demographic Data of all Study Participants.
Abbreviations: BS, bleeding score; NSAIDs, nonsteroidal anti-inflammatory drugs; PBAC, Pictorial Bleeding Assessment Chart.
Participants were further subdivided into oral contraceptive users (n = 19) and nonusers (n = 25). The analysis of these 2 groups showed that there is no significant difference between the BS (P = .614) and e-PBAC (P = .167) in oral contraceptive users and nonusers. Similarly, there was no significant difference found in clotting index (P = .407) and platelet aggregation in the presence of ADP (P = .38), ristocetin (P = .071), and collagen (P = .158).
Establishing the Study’s Normal Range for TEG Parameters and Assessing the 13 Bleeders
Thromboelastography data showed considerable variations in the 31 nonbleeders from the manufacturer’s normal range. The manufacturer recommends that each study should determine its own normal values from at least 20 healthy volunteers. Since blood samples were taken from all females at the same phase of menstrual cycle, we speculated that the variation among the healthy women could be related to this phase of menstrual cycle. Variation was most evident with respect to the R time and the MA, both leaning toward hypercoagulability. Accordingly, we considered the range determined from the 31 healthy participants as the control for this population and further used it to assess the data retrieved from the 13 bleeders. We found that 1 of the 11 participants who had elevated e-PBAC showed hypercoagulable TEG parameters and trace. This case maybe at a risk of thrombosis and needs to be further investigated. Three participants of this group had lower aggregation response to collagen and/or ADP. None of the 3 participants who had elevated BS showed any abnormalities in any of the TEG parameters. Using student t test, there was no significant difference in any of the TEG parameters between the bleeders and nonbleeder groups (Figure 2). Spearmen correlation showed none of the TEG parameters was associated with BS except for MA, which showed a trend toward positive correlation (r = .3; P = .08). There was no significant correlation between TEG parameters and PBAC. We also found no significant correlation between BS and ePBAC, CI, and platelet aggregation in response to ADP, collagen, and ristocetin in oral contraceptive nonusers. Similar results were found in oral contraceptive users except in collagen-mediated platelet aggregation that showed a positive correlation with BS (r = .47; P = .04). The individual data of the bleeders (with elevated eBQ and eBPAC), the normal published range, and the study range for 4 TEG parameters are shown in Table 2, parts (A) and (B).
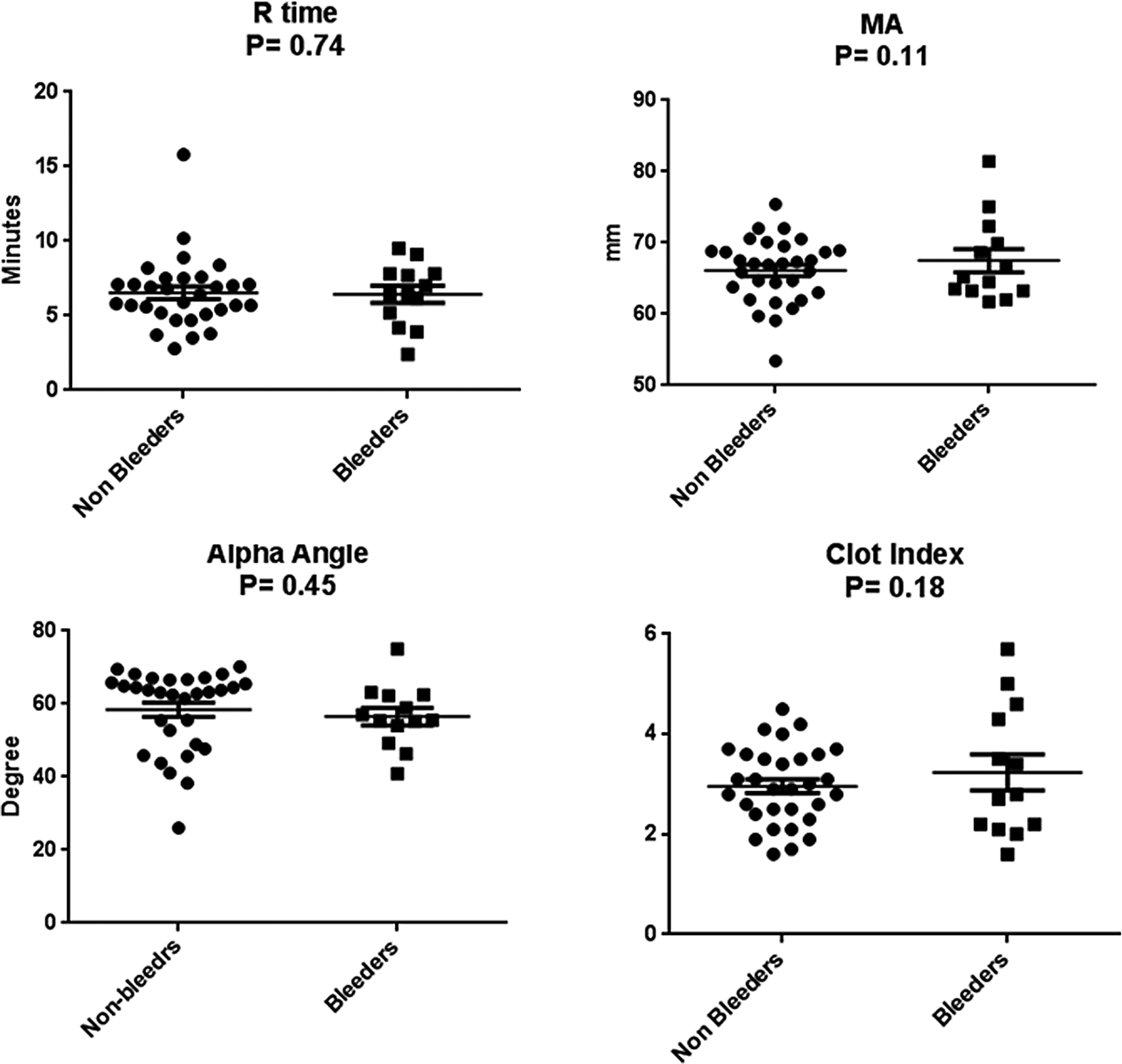
Comparison of thrombelastography (TEG) parameters between bleeders and nonbleeders. Student t-test shows there is no significant difference in any of the TEG parameters between the 2 groups.
Detailed Hemostatic Data in the Bleeder Group (13 Women).
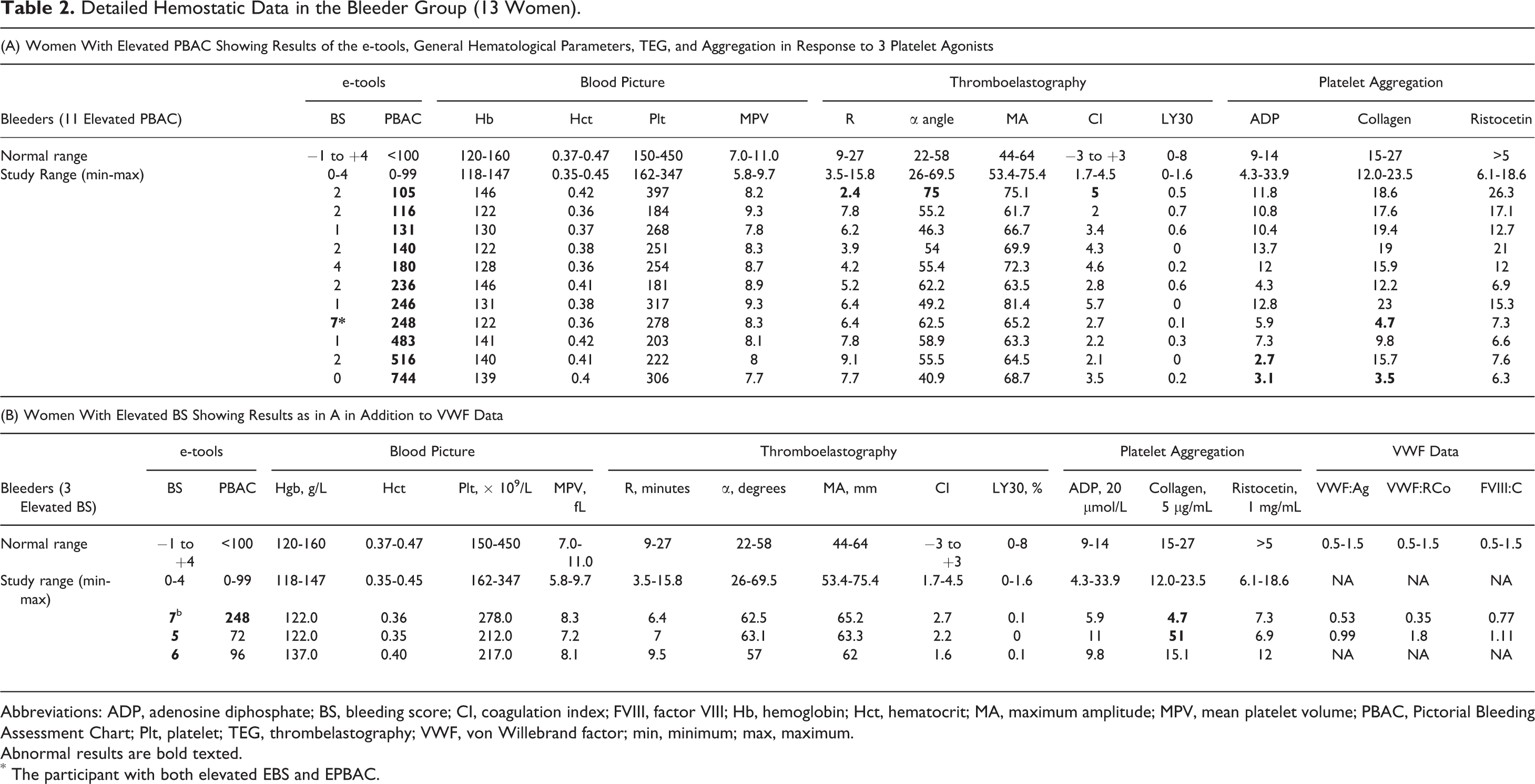
Abbreviations: ADP, adenosine diphosphate; BS, bleeding score; CI, coagulation index; FVIII, factor VIII; Hb, hemoglobin; Hct, hematocrit; MA, maximum amplitude; MPV, mean platelet volume; PBAC, Pictorial Bleeding Assessment Chart; Plt, platelet; TEG, thrombelastography; VWF, von Willebrand factor; min, minimum; max, maximum.
Abnormal results are bold texted.
*The participant with both elevated EBS and EPBAC.
Establishing the study’s Normal Range for Platelet Aggregation and Assessing the 13 Bleeders
Similar to TEG, the detailed analysis of the 31 nonbleeder participants revealed variation in platelet aggregation parameters compared to the manufacturer’s reference range. Accordingly, we used the normal range obtained from the healthy participants to assess the data retrieved from the 13 bleeders. Again we anticipated this variation to be related to this phase of menstrual cycle. Of the 13 bleeders, 1 had abnormally low aggregation in response to ADP and 1 had abnormally low aggregation in response to collagen, and a third had abnormally low aggregation in response to both ADP and collagen indicating PFDs. Student t test showed no significant difference in the aggregation in response to the 3 different agonists between the healthy group and the bleeders (Figure 3). Although there was no correlation between the BS and platelet aggregation in response to any of ADP, collagen, and ristocetin, Spearmen correlation showed a strong negative association of aggregation in response to each of the 3 agonists with PBAC (r = .3, .4, .4; P = .04, .002, .009, respectively).
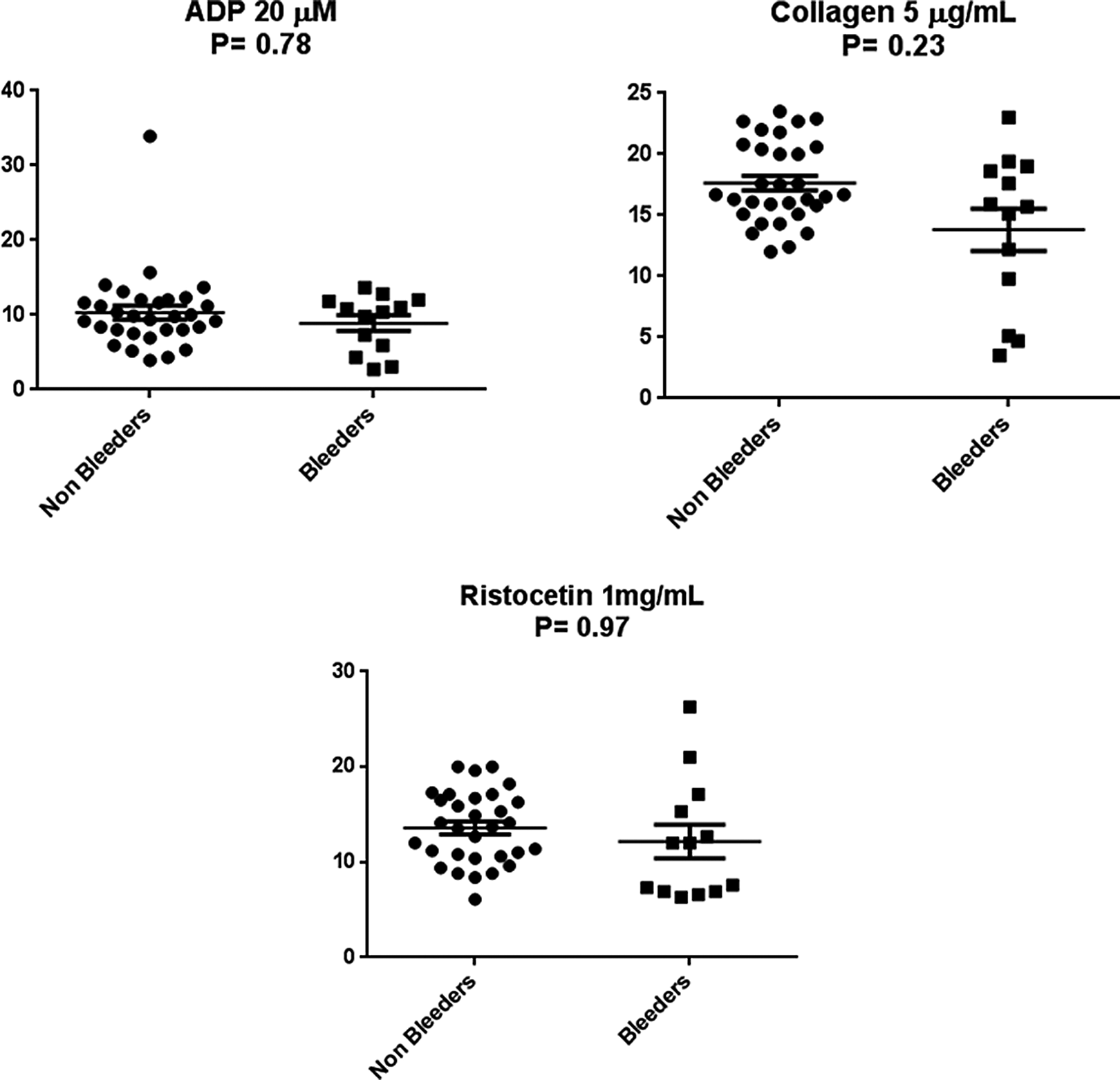
Comparison of platelet aggregation between bleeders and nonbleeders. Student t-test shows there is no significant difference in aggregation in response to any of the 3 platelet agonists between the 2 groups.
Further Evaluation of Participants With Elevated BS
Of the 3 participants with elevated BS, 1 declined referral to the hematologist. The laboratory data of the second participant were found consistent with the diagnosis of type 1 VWD (this patient also had elevated ePBAC and low aggregation in response to collagen); the third participant had normal von Willebrand factor (VWF) levels. Unfortunately, we were unable to test all nonbleeders and those who have elevated PBAC for VWF levels, so it is not known whether we would have identified participants with low VWF in the nonbleeders or those with elevated PBAC at the same level to the elevated BS group. This is a limitation in this study. Laboratory data are provided in Table 2, part (B). Descriptive statistics for TEG and platelet aggregation for healthy participants and bleeders are shown in Table 3.
Descriptive Statistics of Thromboelastography and Platelet Aggregation Data Based on Analysis of the 31 Nonbleeding Women During Follicular Phase of Menstrual Cycle.
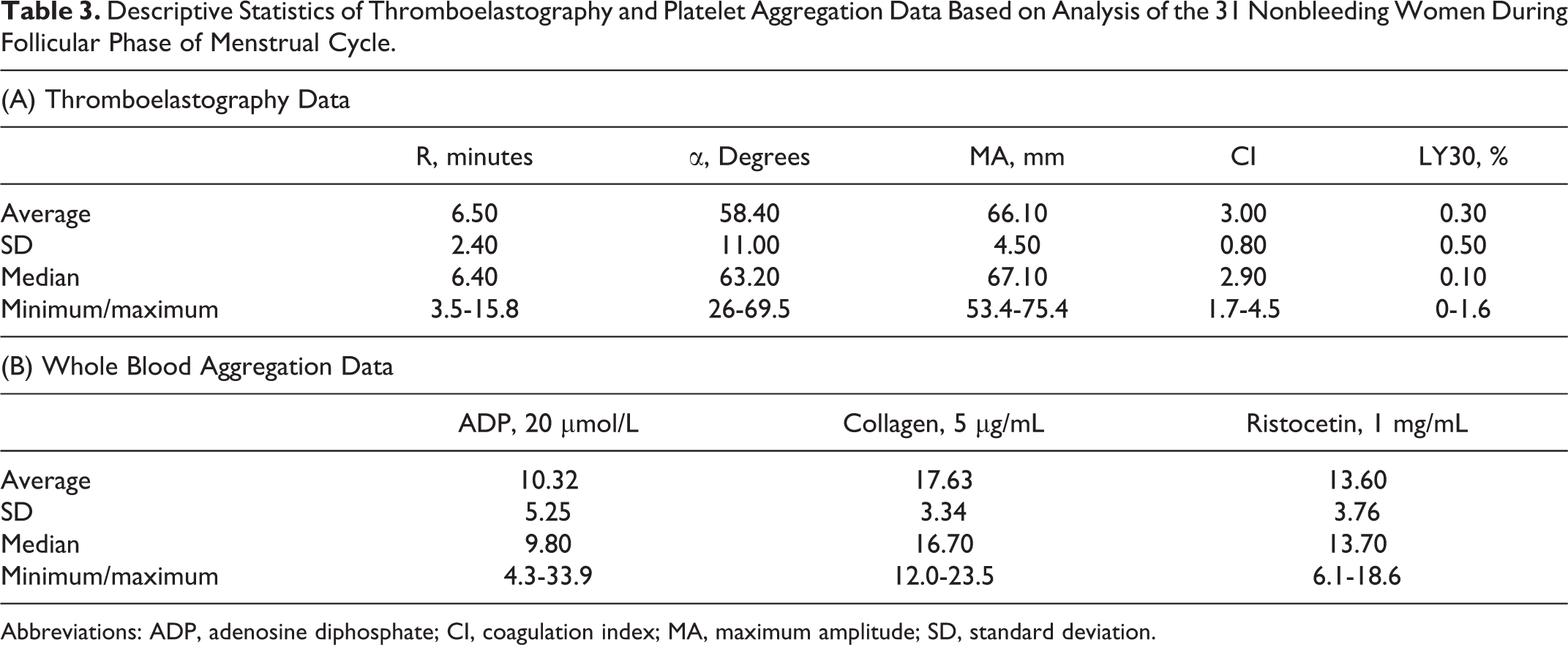
Abbreviations: ADP, adenosine diphosphate; CI, coagulation index; MA, maximum amplitude; SD, standard deviation.
Discussion
In this study, the analysis of 47 normal females using electronic tools showed 23.4% have HMB and 2.1% showed a diagnosis of type 1 VWD and 4.3% showed a PFD (total 6.4 actual MBD). This study also reports data related to the normal range for TEG as well as whole blood platelet aggregation in females in the childbearing period (17-47 years) during the follicular phase of the menstrual cycle. Although TEG and platelet aggregation did not distinguish clearly between the healthy participants and the bleeders, platelet aggregation decreased with the elevation in PBAC and the clot strength/stability (as evidenced by MA) decreased with the increase in BS indicating that these tools may aid in predicting MBD.
Electronic questionnaires are increasingly being used for a number of reasons. They enhance completion of item responses compared to various paper-and-pencil methods. 26,27 Participants generally prefer the electronic method compared to the traditional paper-based version, 28 and the consistency between the electronic format and the paper-based version has been documented. 26 Statistical evidence to support the use of electronic questionnaires has been provided in the literature. In this study, the electronic questionnaire was user friendly, positively contributed to the process of data collection, and also potentially reduced the chances for errors that often results from manual calculation of the BS. The e-PBAC facilitated the collection of menstrual data in a real time and greatly improved participation. Participants were able to record their information in a real-time fashion from home and had a secure unimpeded access to recording data. The feedback received from participants was that this process was easy, straightforward, and allowed them to actually reflect on their bleeding experience during menstruation. In this study, the use of e-BQ and e-PBAC has helped identification of 13 (27.7%) potential bleeders and helped the diagnosis of VWD in 1 (2.1%) and PFD in 2 (4.3%) of the 47 seemingly normal women. Unfortunately, we were unable to test all nonbleeders and those who had elevated PBAC for VWF levels, so it is not known whether we would have identified participants with low VWF in the nonbleeders or those with elevated PBAC at the same level compared to the elevated BS group. This is a limitation in this study.
Heavy menstrual bleeding is a significant problem and many seemingly normal women ignore and/or are unaware of the importance of the objective assessment of menstrual blood loss. In this study, 8 (72.7%) of 11 women with elevated PBAC did not respond to their referral for further gynecological assessment and thus failed to be investigated. This may indicate the poor awareness of the importance of abnormal menstrual blood loss and calls for educational programs among the general female population are important as these may improve the diagnosis of MBDs.
Platelet function defects were highlighted in this study since 1 of the 3 participants who had abnormal BS showed reduced aggregation in response to collagen with normal VWF levels. Although an isolated abnormality, this may indicate PFD. The other 2 showing abnormally low aggregation had normal BS but presented with HMB and had the highest e-BPAC score. All other haemostatic tests including platelet count were normal in these participants. No further investigations were performed.
Although TEG parameters did not show tendency for bleeding in any of those with elevated BS or PBAC, paradoxically, 1 participant with mildly elevated PBAC showed evidence of hypercoagulability as evidenced by R time and CI. Thrombosis has previously been reported in patients with bleeding disorders such as hemophilia and VWD. 29 However, this case was not investigated further.
Recent research showed that the menstrual phase and early follicular phase are the optimal time to conduct hemostatic testing as the variation in hemostatic variables is lowest. 14 In addition to the menstrual cycle phase, variation from the manufacturer’s range in TEG or platelet aggregation in the healthy female population (nonbleeders) may be related to other factors such as smoking and contraception. In this study, the use of oral contraceptives had no significant effect on platelet aggregation mediated by ADP, ristocetin, and collagen. Also, there was no significant difference in TEG parameters between oral contraceptive users and nonusers. Despite variation from manufacturer’s range, the platelet aggregation data were relatively tight. Also, with the exception of α angle, the TEG parameters exhibited similar pattern.
The variation in TEG parameters in the healthy female population from the manufacturer’s was mainly related to shorter R time and increased CI and can be related to gender and menstrual cycle. This is supported by a previous TEG study on 118 healthy participants where healthy women were significantly more hypercoagulable than men, particularly in relation to the R time. 11 Since blood samples were taken from all females at the same phase of menstrual cycle, we speculated that the variation among the healthy women could be related to this phase of menstrual cycle or the timing with respect to menses in oral contraceptive users. Variations in clotting factors including factor VII, fibrinogen, and factor X during menstrual cycle or with the use of oral contraceptives have been reported 30 and variation in TEG toward hypercoagulability in females has also been shown. 31 Oral contraception was shown to affect blood coagulability as well; however, the effect is dependent on the dose, type, and duration of contraception used. 12,15,16,32,33 The TEG as well as whole blood aggregation manufacturers recommend each study site to establish its own reference ranges to facilitate the appropriate comparison. We believe it is critical to also consider the phase of the menstrual cycle when interpreting results for these hemostatic tests.
In conclusion, although we acknowledge the relatively small size of the tested population, the study indicates that the electronic tools, e-BQ and e-PBAC, facilitate data collection and may help screen women with MBD and those in need of gynecological investigations. The study also alerts clinicians the importance of considering the possibility of HMB in apparently normal women and highlights the need to enhance awareness in the general female population. This small study is a prelude to a study to determine the validity of these tools in screening for MBDs in women.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by an internal research grant from St Lawrence College and a “Dream of Cure” grant from Canadian Hemophilia Society.