
Abstract
Early diagnosis is the key point in the management of acute pulmonary thromboembolism (PTE). There are no reports in the literature comparing the serum cystatin C levels in patients with acute PTE and normal volunteers. Therefore, in this study, we analyzed 50 patients with acute PTE and 45 healthy volunteers with normal renal function. The serum cystatin C level was significantly higher in the PTE group than in the non-PTE group (1.08 mg/dL [interquantile range (IQR) 0.79-1.56] and 0.85 mg/dL [IQR 0.77-1.03], respectively, P = .017). When determining the presence of PTE, the highest value of sensitivity and specificity was set at a cutoff value of 1.15 mg/dL with 93.3% specificity, 46.0% sensitivity, 88.5% positive predictive value, and 60.9% negative predictive value. In the multivariate model, cystatin C was significantly associated with the presence of PTE (odds ratio: 12.34, 95% CI 2.64-57.75). In conclusion, cystatin C may be an indicator of acute PTE in patients with normal renal function.
Introduction
Pulmonary thromboembolism (PTE) is the most common cause of vascular death after myocardial infarction and stroke and the leading preventable cause of death in hospital patients.
1
Early diagnosis is the key point in the management of acute PTE, since immediate treatment is highly effective. Failure to diagnose acute PTE is a serious management error since 30% of untreated patients die, while only 8% die with effective therapy.
2
The approach used to diagnose PTE is mainly based on noninvasive diagnostic strategies including clinical probability assessment,
Cystatin C is a protease inhibitor that controls the proteolitic enzymes in the processes of blood coagulation, complement activation, and food digestion. 10 It has been shown that cystatin C is a more sensitive marker of glomerular filtration rate (GFR) changes than serum creatinine (Scr), 11 because its levels are not affected by muscle mass, age, inflammation, fever, or exogenous agents. 12 Recent studies have shown that cystatin C is not only a candidate marker of impaired kidney function but is also associated with coronary artery disease, 13 congestive heart failure, 14 carotid atherosclerosis, 15 and peripheral vascular disease. 16 In a report with relatively normal renal function patients, it was found that the serum level of cystatin C was significantly higher in patients with cardiovascular events than in patients without cardiovascular events. 17
In a recent report, plasma cystatin C levels were evaluated to predict the prognosis of patients with acute PTE.
18
They found that cystatin C elevation was associated with a poor 30-day prognosis in acute PTE. In another report, Brodin et al analyzed 83 incident venous thromboembolic events in 3251 patients during a median of 12.3 years of follow-up.
19
They found that serum cystatin C levels were associated with the risk of venous thromboembolism in patients with normal kidney function. However, to the best of our knowledge, there are no reports in the literature comparing the serum cystatin C levels in patients with acute PTE and non-PTE. Therefore, we aimed to evaluate/compare the serum cystatin C levels in patients with acute PTE and non-PTE who had normal renal function. In addition, we compared the difference in levels of cystatin C in patients with massive, submassive, and nonmassive PTE and the correlation between the levels of cystatin C and
Methods and Materials
The present prospective study was approved by the ethics review board of Erciyes University. All patients were informed about the study, and their written consent was obtained.
Study Population and Definitions
In the present study, we analyzed 50 patients with acute PTE diagnosed by contrast-enhanced spiral computed chest tomography and 45 healthy volunteers. Patients with a history of coronary artery disease, or heart failure, previously diagnosed malignancy, history of previous PTE, apparent kidney failure (estimated GFR [eGFR] ≤60 mL/min/1.73 m2), and patients younger than 20 years and older than 80 years of age were excluded from the study.
History of surgery was accepted as surgery during the past 6 weeks. Chronic respiratory disease was defined as chronic obstructive pulmonary disease, asthma, or interstitial lung disease, which were previously diagnosed.
Massive PTE was defined as acute PTE with sustained hypotension (systolic blood pressure [SBP] 90 mm Hg for at least 15 minutes or requiring inotropic support, not due to a cause other than PE, such as arrhythmia, hypovolemia, sepsis, or left ventricular dysfunction), pulselessness, or persistent profound bradycardia (heart rate 40 bpm with signs or symptoms of shock). Submassive PTE was defined as acute PTE without systemic hypotension (SBP 90 mm Hg) but with right ventricular dysfunction (RVD). Nonmassive PTE was defined as acute PTE and the absence of the clinical markers of adverse prognosis that define massive or submassive PTE. 20
Data Collection and Laboratory Measurements
Sociodemographic characteristics, previous medical history, and details regarding lifestyle behaviors (smoking) were obtained by face to face interview. Height and weight were measured, and body mass index (BMI) was defined as weight in kilograms divided by height in square meters. Systolic blood pressure and diastolic blood pressure (DBP) were recorded at rest.
Blood samples were taken within 24 hours of hospital administration. Blood samples for cystatin C were obtained and centrifuged, then stored at −80°C. Serum cystatin C levels were analyzed after blood samples were obtained from all study patients, and it was determined with an particle-enhanced turbidimetric immunoassay method (Abbot, Wiesbaden, Germany).
Echocardiography
Transthoracic echocardiography for the assessment of RV dysfunction was performed using a Vivid 7 (GE Medical Systems, Milwaukee, Wisconsin) echocardiographic system. Echocardiography was performed in patients within 48 hours of acute PTE diagnosis. The examinations were digitally recorded by an experienced echocardiographer blinded to the results of biochemical assays. Patients with ≥1 of the following were considered to have acute RV dysfunction: 22 (1) RV dilatation (end-diastolic diameter >30 mm or RV/left ventricular end-diastolic diameter ratio >0.9 in 4-chamber view), (2) paradox septal systolic motion, and (3) pulmonary hypertension (Doppler pulmonary acceleration time <90 ms or the presence of an RV/atrial gradient >30 mm Hg).
Statistical Analysis
SPSS 15.0 software (SPSS, Chicago, Illinois) was used for the basic statistical analysis. The Kolmogorov-Smirnov test was used to determine the normality of distributions of variables. Continuous variables with normal distribution are presented as mean value ± standard deviation (SD). Median values with interquantile ranges (IQR, 25th to 75th percentiles) were used where normal distribution was absent. Statistical analysis of the parametric variables between the 2 groups was performed using Student t test; Mann-Whitney U test was used for nonparametric variables. Categorical variables were analyzed by the chi-square (χ2) test. The correlation analysis was performed by Spearman correlation test for nonparametric results. The Kruskal-Wallis test was used to compare the cystatin C levels between the PTE subgroups. Receiver–operating characteristic (ROC) curves were analyzed to assess the optimal cutoff values of cystatin C for acute PTE. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated for the chosen cutoff value. Multiple logistic regression analysis was used to determine the predictors for acute PTE. Significant univariate variables with P < .1 were included in the multiple logistic regression analysis for the calculation of odds ratios (ORs) and 95% confidence intervals (CIs). All P values are 2 sided, and a P value of <.05 was considered significant.
Results
The mean age was 59.9 ± 16.4 years in the PTE group and 55.1 ± 9.4 years in the non-PTE group (P = .08). The rates of gender, smoking, hypertension, diabetes mellitus (DM), and chronic respiratory disease were similar in the 2 groups. Deep vein thrombosis and a history of surgery in the past 6 weeks were significantly higher in the PTE group, as expected (P < .001). There were no differences in SBP and DBP between the 2 groups. The BMI, Scr level, and eGFR were also statistically not significant between the PTE group and the non-PTE group (P > .05). The demographic characteristics of patients in the 2 groups are shown in Table 1.
Clinical and Biochemical Characteristics of the Study Patients.
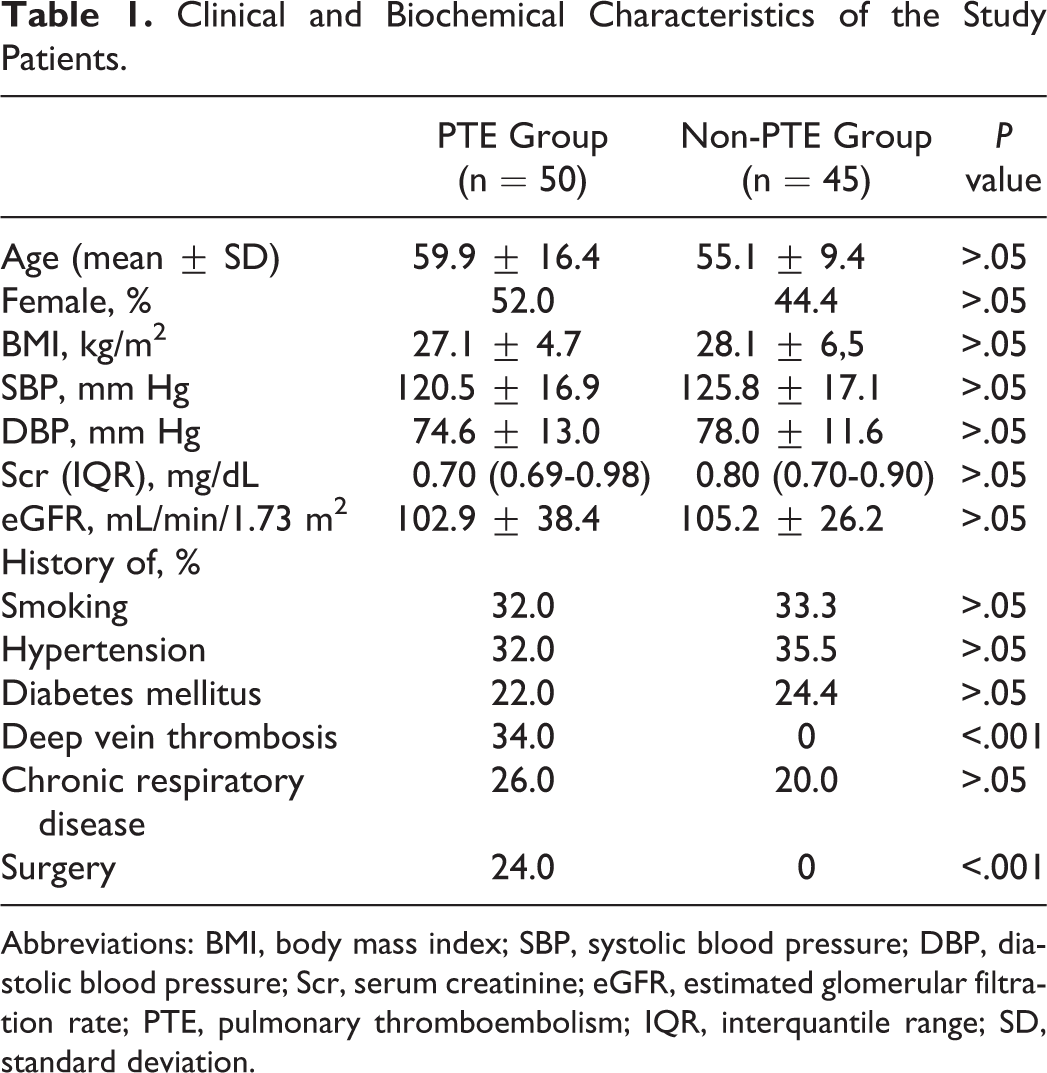
Abbreviations: BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; Scr, serum creatinine; eGFR, estimated glomerular filtration rate; PTE, pulmonary thromboembolism; IQR, interquantile range; SD, standard deviation.
Figure 1 shows the comparison of cystatin C levels in the 2 groups. The cystatin C level was significantly higher in the PTE group than in the non-PTE group (1.08 mg/dL [IQR 0.79-1.56] and 0.85 mg/dL [IQR 0.77-1.03], respectively, P = .017). When determining the presence of acute PTE, the highest value of total sensitivity and specificity was set at a cutoff value of 1.15 mg/dL with 46.0% sensitivity, 93.3% specificity, 88.5% PPV, and 60.9% NPV. The area under the ROC curve was calculated as 0.643 (P = .011; Figure 2). Cystatin C levels were also higher in patients with acute PTE with ≥10 days hospital stay (n = 18, 36%) than in those with <10 days hospital stay (n = 32, 64%). Figure 3 shows the difference in these 2 groups (cystatin C; 1.33 mg/dL [IQR 0.84-2.03] and 1.01 mg/dL [IQR 0.73-1.36], respectively, P = .047).
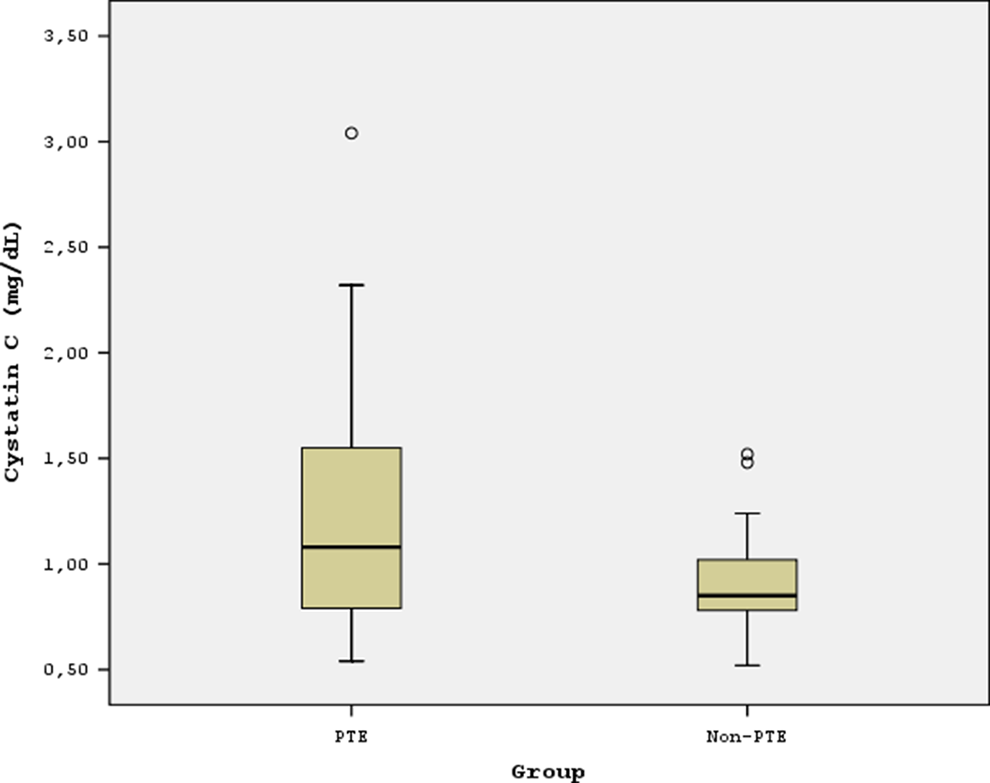
Comparison of cystatin C level in the pulmonary thromboembolism (PTE) group and in the non-PTE group.
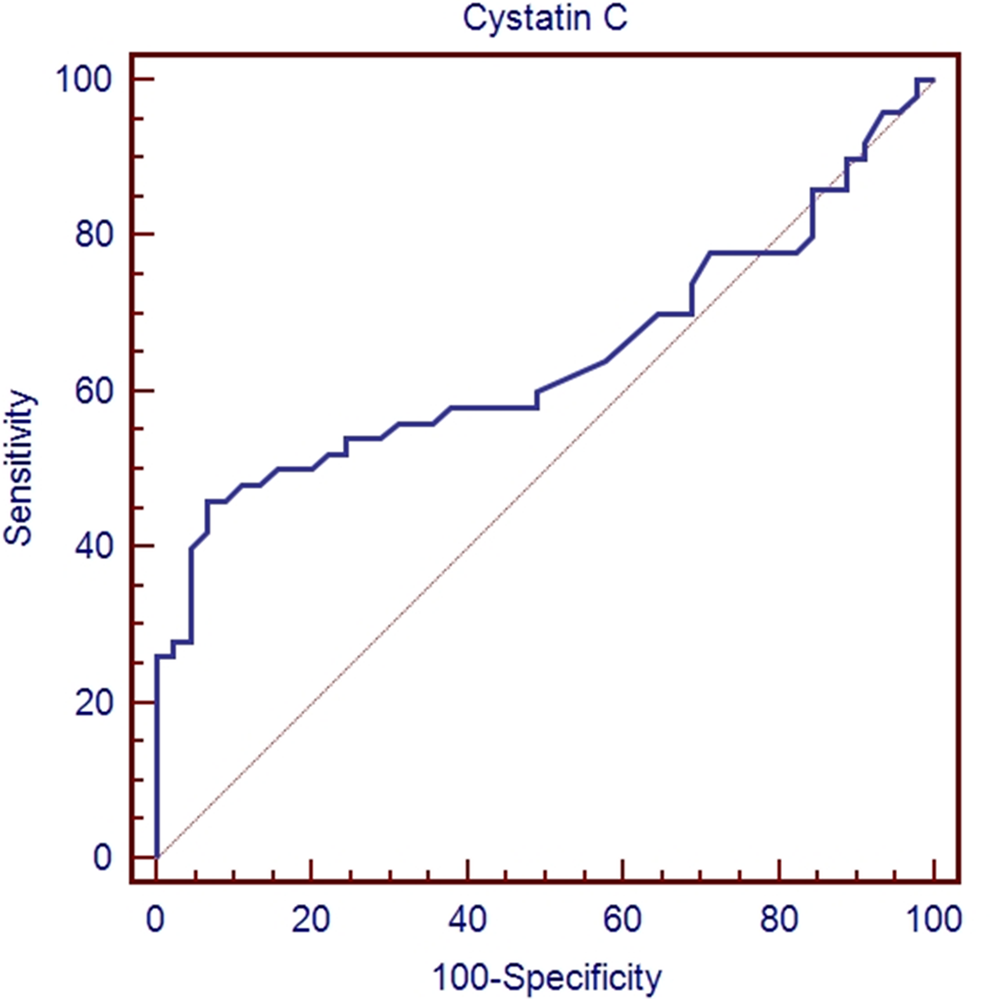
Receiver–operating characteristic (ROC) curve analyses for cystatin C to predict acute pulmonary thromboembolism (PTE).
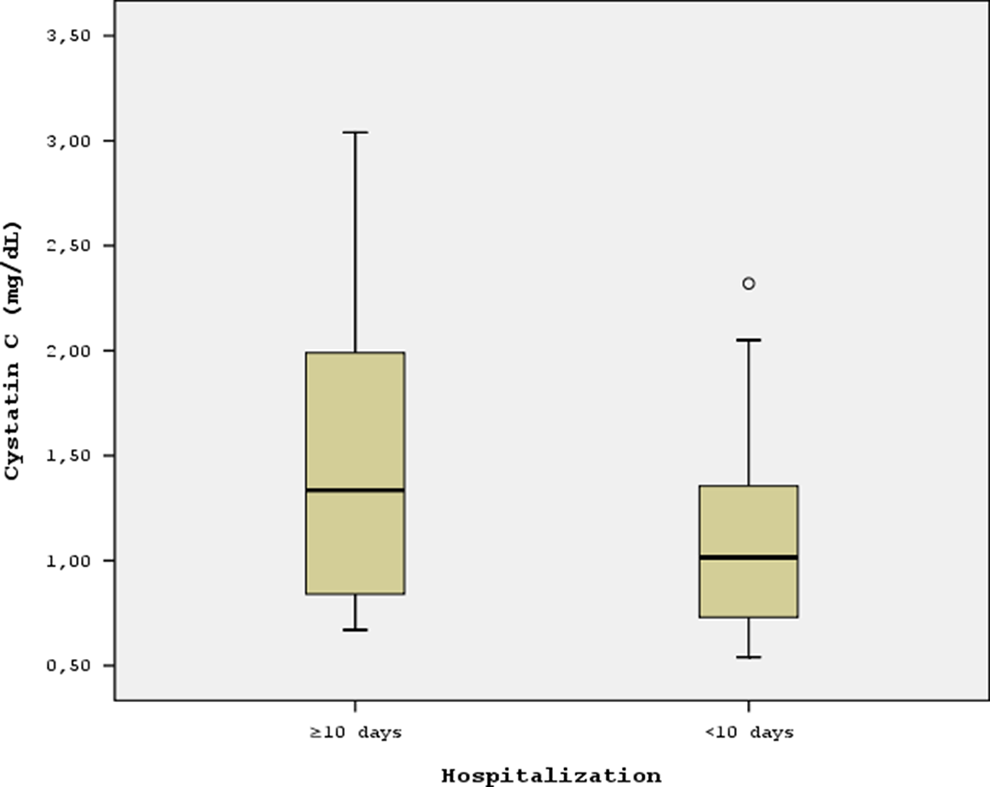
Comparison of cystatin C level in the pulmonary thromboembolism (PTE) patients with ≥10 days hospital stay and in those with <10 days hospital stay.
We next investigated the relationship between serum cystatin C levels and clinical biochemical parameters (Table 2). The Spearman correlation analysis demonstrated that serum cystatin C was highly correlated with age in all participants. It was correlated with Scr, and it was also negatively correlated with eGFR in all participants. In the PTE group, the mean
Correlation of Serum Cystatin C Levels With Clinical and Biological Parameters.
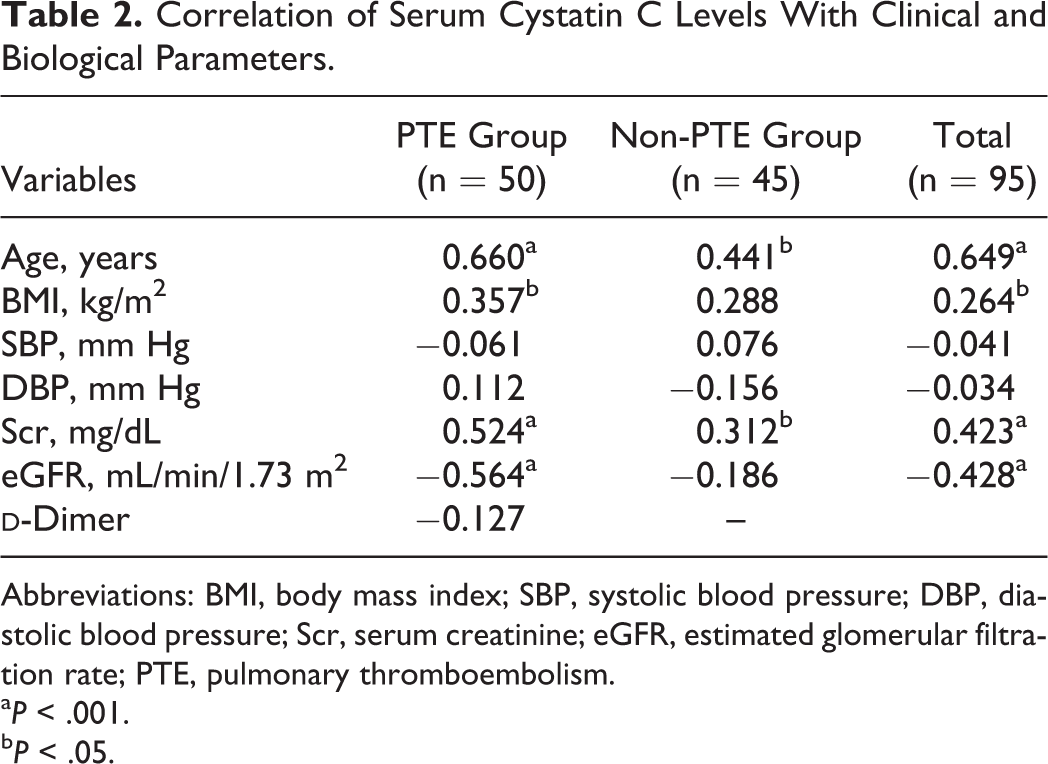
Abbreviations: BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; Scr, serum creatinine; eGFR, estimated glomerular filtration rate; PTE, pulmonary thromboembolism.
a P < .001.
b P < .05.
Univariate analysis of age, BMI, Scr, eGFR, and serum cystatin C revealed that there was a statistically significant association between the presence of PTE and both age and cystatin C (P = .09 for age and P = .001 for cystatin C). In the multivariate binary logistic regression model, cystatin C remained significantly associated with the presence of pulmonary embolism (OR 12.34, 95% CI 2.64-57.75). This implies that for every increase in serum cystatin C of 1 mg/dL, the probability of PTE increases 12-fold.
In the PTE group, 5 (10%) patients had massive PTE, 27 (54%) patients had submassive PTE, and 18 (36%) patients had nonmassive PTE. The cystatin C levels were 1.28 mg/dL (IQR = 0.75-1.77), 1.18 mg/dL (IQR 0.80-1.67), and 0.85 mg/dL (IQR 0.73-1.35) in patients with massive, submassive, and nonmassive acute PTE, respectively, and the difference was not statistically significant (P = .336). The mean RV/LV ratio was 0.81 ± 0.17, and 32 (64%) patients had RVD in the PTE group. Cystatin C levels were higher in patients with RVD than in those without RVD (1.19 mg/dL [IQR 0.81-1.66] and 0.85 mg/dL [IQR 0.73-1.35], respectively), but the difference was also statistically not significant (P > .05).
All cause 30-day mortality rate was 4% (n = 2) in the PTE group. One of these patients had massive embolism and the other had submassive embolism. Cystatin C levels were 1.28 mg/dL and 0.79 mg/dL, respectively.
Discussion
In the present study, serum cystatin C levels were significantly increased in patients with acute PTE having normal renal function according to the non-PTE patients who had similar age, BMI, eGFR, and comorbidities such as DM, hypertension, and chronic respiratory diseases. This is the first study demonstrating high serum cystatin C levels in patients with acute PTE having normal renal function.
In a recent article, Brodin et al reported that 61.4% of the 83 patients with VTE had deep vein thrombosis and only 38.6% had PTE. 19 The authors showed that patients with serum cystatin C levels in the top quartile (≥0.87 mg/L) had a 2.5-fold increased risk of VTE compared to those with levels in the bottom quartile (≤0.72 mg/L) adjusted for age, sex, BMI, smoking, diabetes, and high sensitivity (hs)-CRP. 19 In addition, when analyzing cystatin C as a continuous variable, they found that an increase of 1 SD (0.11 mg/L) in cystatin C concentration was associated with a 46% increased risk of VTE. In the present report, deep vein thrombosis was detected only in 34% of the patients with acute PTE, and serum cystatin C was the only variable that was significantly associated with the presence of acute PTE in the multivariate model, and with every increase in serum cystatin C of 1 mg/dL, the probability of PTE increases 12-fold.
Venous thromboembolism and atherothrombosis have shared risk factors and a common pathophysiology that includes inflammation, hypercoagulability, and endothelial injury. 25 It was also shown that cystatin C was associated with coronary artery disease and carotid atherosclerosis. 13,15 In one meta-analysis, one marker of inflammation (CRP) was associated with a substantial increase in risk of venous thromboembolism. 26 Although inflammation may be regarded as the underlying mechanism between cystatin C and acute PTE, Brodin et al analyzed patients with VTE having normal renal function, and they found that adjustment for hs-CRP in the statistical models did not affect the risk estimates for VTE by cystatin C. In addition, cystatin C is known to modulate neutrophil chemotactic activity and may inhibit the prothrombotic activity of proteolytic substances secreted by activated neutrophils. 19,27 Although the mechanism that prevents thrombosis formation may also be an explanation for the underlying link between cystatin C and acute PTE, more studies are needed to determine the correct pathway.
It was shown that serum cystatin C level appears to be a good biomarker in the prediction of AKI and to be useful in estimating GFR. 28,29 In addition, increased cystatin C levels were also correlated with BMI and older age. 19,30 –32 The present study also shows that serum cystatin C levels were correlated with age, BMI, Scr, and eGFR in the total population in accordance with other previous reports.
Pulmonary thromboembolism is divided into 3 subgroups as massive, submassive or nonmassive PTE. 20 Right ventricular dysfunction has an important role in the stratification of patients as massive and submassive PTE. 20,34 However, echocardiography is a user-dependent procedure and is not always readily available for a diagnostic workup and risk stratification of PTE. Therefore, the use of more inexpensive and widely available laboratory measurement of biomarkers may also be beneficial. At the same time, various studies examined the role of BNP, NT-pro-BNP, CRP, troponin I or T, CA IX, and tenasin C in the risk stratification of patients with PTE. 3 –9 In the present report, although the serum cystatin C levels were higher in patients with RVD than in patients without RVD, the difference was not statistically significant. The serum cystatin C levels were also high in patients with massive and submassive PTE, although again the difference was not statistically significant. This may be due to the low power of the study that contained only 50 patients with acute PTE. The history of chronic respiratory disease (26% of patients with acute PTE) may be the other reason that can be the cause of RVD.
Our study has some limitations. First of all, we only included a relatively small number of patients and volunteers. The non-PTE group had no echocardiography and
Conclusion
The present study shows that serum cystatin C levels significantly increased in patients with acute PTE having normal renal function in comparison to the non-PTE patients. Elevated serum cystatin C level was also associated with prolonged hospitalization in patients with acute PTE. Serum cystatin C may be an indicator of acute PTE in patients with normal renal function from the point of PTE diagnosis and risk stratification.
Footnotes
Acknowledgments
The authors would like to thank İsmail Koçyiğit for help with the study design, Ferhan Elmalı for data analysis, and S. Kader Köse and Cevat Yazıcı for the biochemical measurement.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.