
Abstract
Diagnosing acute pulmonary embolism (PE) involves clinical suspicion in combination with sequential diagnostic tests including
Introduction
The diagnosis of pulmonary embolism (PE) can be difficult due to variable clinical presentation with symptoms that are often shared with several other disease entities, namely shortness of breath, chest pain, and tachycardia. Laboratory assays are used to help clinicians decide when imaging is required. The
The AADD cutoff value calculated as ([age (years) × 10] ng/mL) was proposed by Douma et al after their analysis of 1721 consecutive outpatients with clinical suspicion for PE. This was then validated using 3 large cohorts of patients with an unlikely Wells score or a non-high probability Geneva score inpatients ≥50 years of age. The researchers concluded that PE could be ruled out in an additional 25% to 30% of patients whom would have had a positive conventional
Multiple previous studies have demonstrated that the novel AADD cutoff has a greater clinical utility compared to the traditional cutoff value without sacrificing sensitivity.
1,4
-7
In light of this evidence, we decided to revisit our institutions
Methods
We retrospectively searched for patients 50 years of age and older at our institution who presented with a chief complaint of either “shortness of breath” or “chest pain” in a 1-year time period that were evaluated with CDD. We accumulated 4000 encounters and then reviewed
Demographics of Study Population.

Abbreviations: DVT, deep vein thrombosis; PE, pulmonary embolism.
In our institution,
Results
Of all, 132 of 4000 patients met criteria for inclusion. With the CDD cutoff value, 124 (94.0%) patients had false positives and 8 (6.1%, Table 2) patients had true positives. In the AADD cutoff cohort 104 patients would have a positive laboratory value to warrant a CT-PE scan for diagnosis. The remaining 28 patients would have initially screened negative and would not have warranted diagnostic imaging resulting in a 21.2% (28 of 132) reduction in CT-PE scans (Table 2). Positive predictive value for the CDD group was 6.1% versus 6.7% for the AADD group. Across all age groupings, there was a relative increase in negative AADD testing. This was appreciated most in the 70 to 79 age-group (27.3%) and least in the 50 to 59 age-group (13.7%) as shown in Figure 1.
Findings Based on Laboratory Assay Cutoff of Conventional

Abbreviations: AADD, age-adjusted
a Values are numbers (percentages) of patients unless otherwise specified.
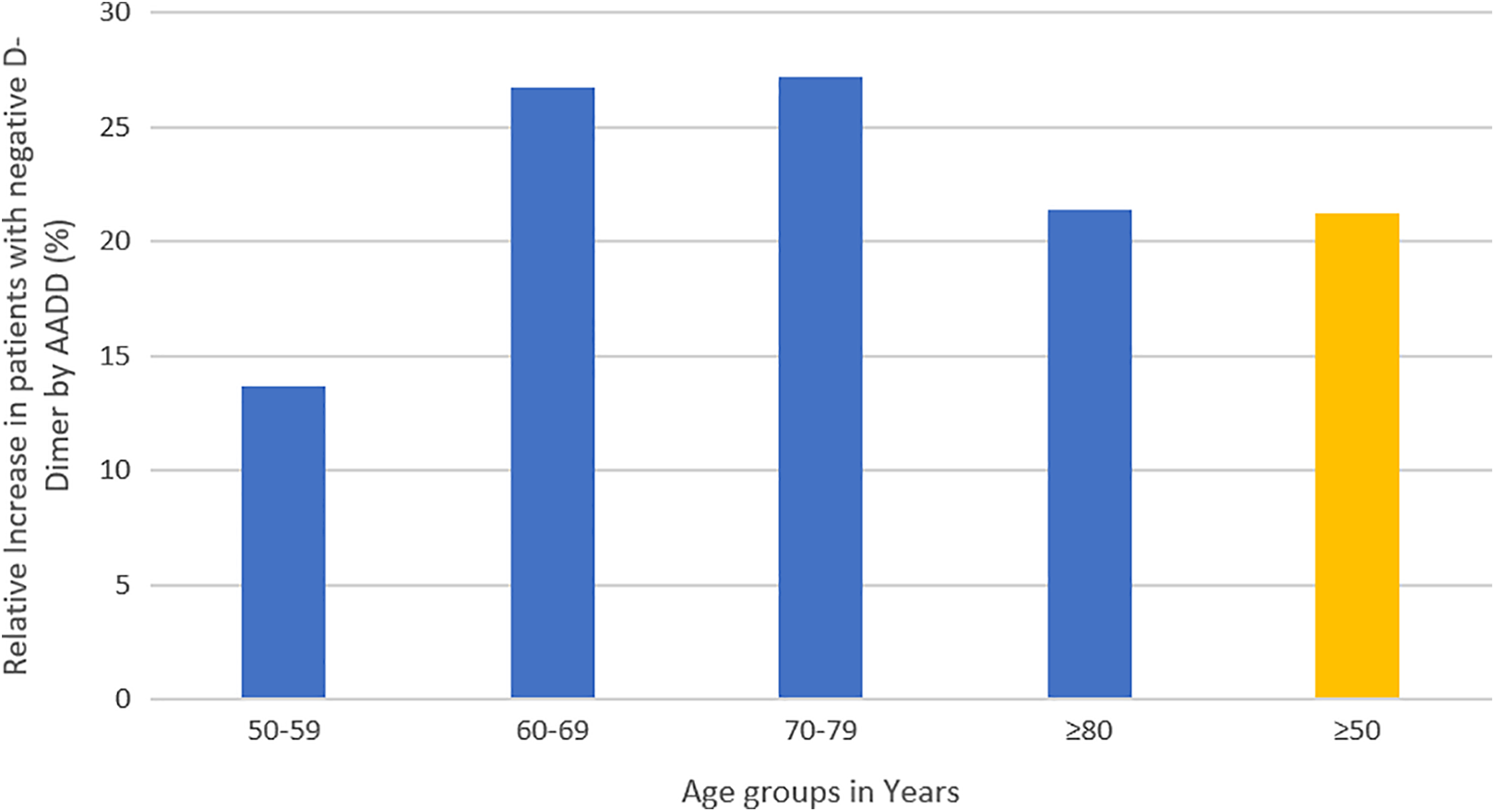
Relative increase in patients with negative AADD results by age-group. AADD indicates age-adjusted
Discussion
In patients with an intermediate or low clinical risk for PE, a highly sensitive screening laboratory test such as
The AADD cutoff has a significant increase in accuracy and specificity compared to our institution’s CDD cutoff. When we initially used the CDD, there were 132 patients that qualified for a CT-PE scan based on their clinical presentation and laboratory assay. Using the AADD cutoff, 104 (78.8%) patients out of those 132 would have continued to have a positive
The ADJUST-PE study was a prospective management validation study of the AADD cutoff.
7
They showed an additional reduction in CT imaging of 23.3% without a significant change in false-negative results when compared to a standard
Health care costs in the United States continue to grow at an exponential level and cause grave concern. With almost daily negative reports about the state and cost of health care in this country, it is important to understand the value of quality care. In a 220 patient study out of South Chicago, an estimated US$200 000 of billed testing was performed due to elevated
In addition to the financial benefit, reducing CT-PE will decrease adverse outcomes related to contrast administration. The elderly individuals (>65 years of age) have lower baseline kidney function due to an increased prevalence of diabetic nephropathy, dehydration, congestive heart failure, and concurrent use of nephrotoxic drugs. 10 These preexisting risk factors lead to an increase in acute kidney injury by way of contrast induced nephropathy (CIN). The prevalence of CIN has been reported as high as 5% for inpatients and up to 14% for patients needing intensive care unitcare. 10 This makes the AADD cutoff especially useful in the elderly population where complications of CIN can be more severe.
The increase in radiation exposure is also a concern, even in the elderly individual. A Retrospective analysis of 5203 patients older than the age of 50 receiving a 10-year cumulative cancer screening radiation dose of 9 to 13 mSv had a 0.05% increased risk of major cancer. 11 Patients with symptoms of “chest pain” or “shortness of breath” often have disease processes that lead to multiple recurrent emergency room presentations and hospital admissions. This produces clinical situations for recurrent need of CT-PE and hence higher doses of radiation. We should strive for As Low As Reasonably Achievable radiation doses for our patients which is better achieved utilizing the AADD cutoff for reduction in CT-PE scans.
Standardization on
There are several limitations to our study including the absence of Wells score in 30 of our patients along with a low risk Wells score (<2) in 13 of our patients. In both these circumstances, there is an override option that allows the ordering physician to bypass the Wells score entirely or proceed with the order despite a low risk Wells score. We also found that in our study population, the CDD carries a true-positive rate of 6.1%. This is quite low and believed to be both from unnecessary CT-PE scans and an over utilization of the
Conclusion
In conclusion, using the CDD to determine the necessity of CT-PE imaging for patients with symptoms such as shortness of breath, chest pain, and tachycardia has a low utility in the absence of useful clinical criteria such as the Wells criteria. The improved accuracy of implementing the AADD cut-off for diagnosing PE in our institution would lead to a decrease in unnecessary testing; however, this is no substitute for astute clinical judgment. In performing this analysis, we have also identified areas of improvement in our process for care of patients with suspected PE. We hope that this study encourages other institutions to revisit utilizing the AADD cutoff and current procedure for diagnosis of PE which ultimately will produce cost savings and higher quality patient care.
Footnotes
Authors’ Note
Ethical approval to report this case was obtained from Ascension Providence Hospital Southfield Campus institutional review board (Project Title: [1240969-1] The Role of Age Adjusted
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.