
Abstract
Leukocytes are reported as crucial not only for plaque activation but also in thrombus formation in acute coronary syndromes (ACSs). Among the markers of inflammation, in coronary artery disease neutrophil–lymphocyte ratio (NLR) has been reported to have the greatest predictive power of poor outcomes. Our aim was to evaluate the association of NLR with coronary thrombus in patients with non-ST-segment elevated ACSs (NST-ACSs). A total of 251 patients were hospitalized with a diagnosis of NST-ACS including non-ST-segment elevated myocardial infarction and unstable angina pectoris. Coronary angiographies were performed. In 167 patients, coronary thrombus was detected. Between the patient groups with and without coronary thrombus, neutrophil count, platelet count, and NLR are significantly increased, and lymphocyte count is significantly decreased in the group with coronary thrombus as compared to patient group without coronary thrombus. Leukocyte count and NLR may give an indication about the presence of coronary thrombus. In NST-ACS, blood parameters may give valuable information about the status of the coronary arteries.
Introduction
Atherosclerosis represents an active inflammation that leukocytes play major role. 1 Disruption of the vulnerable atherosclerotic plaque exposes blood to subendothelial collagen, tissue factor, and other procoagulant factors that leads to activation of platelets and culminate formation of thrombosis that is the central of acute coronary syndrome (ACS) pathogenesis. The subtypes of white blood cell count have been investigated for their role in atherosclerosis. 2 White blood cells are reported as crucial not only for plaque activation but also in thrombus formation and thrombus growth in ACSs. 3 Mononuclear cells (monocyte/macrophages, T lymphocytes) are studied as pathogenic within unstable coronary artery plaques. 4 Neutrophils are involved with infarct healing and are also pathogenic (eg, as with leukocyte–platelet aggregate formation and as a cause of reperfusion injury in the setting of ACSs). The neutrophil–lymphocyte ratio (NLR) was reported as an independent predictor of mortality and myocardial infarction (MI) in coronary artery disease (CAD). 5 The NLR has also been studied as a prognostic marker in noncardiac disease 6 and in patients who undergo percutaneous coronary intervention (PCI). 7
Within the markers of inflammation in CAD, NLR has been reported to have the greatest predictive power of poor outcomes in patients with CAD. Neutrophil and lymphocyte indicate opposing clinical outcomes in ACSs. 8 Increased neutrophil count has been related to myocardial infract extension, 9 development of postinfarction heart failure, 10 impaired epicardial and microvascular perfusion, 11,12 and postinfarction mortality. 13 Lymphocytes have important role in modifying the inflammatory response in atherosclerosis. 14 –16 In acute setting, lymphopenia is a common finding during stress response, resulting from increased levels of corticosteroids 17 and has good discriminative ability for the diagnosis of acute MI (AMI). 18
The goal of this study was to evaluate the association of subtypes of white blood cells and NLR with coronary thrombus formation in patients with non-ST-segment elevated ACSs (NST-ACSs).
Methods
A total of 251 consecutive patients were hospitalized in our hospital with a diagnosis of NST-ACS. The ACSs were defined as presentation with symptoms of ischemia in association with electrocardiographic changes, positive cardiac enzymes, new documentation of CAD, or the previous CAD diagnosis as defined by similar previous studies. 19 Symptomatic patients were assessed by a standard diagnostic flowchart that included clinical and electrocardiographic monitoring as well as biochemical measurements of myocardial necrosis markers. Patients diagnosed with AMI with non-ST-segment elevation MI (non-STEMI) and unstable angina (UA) were included in this study. The study protocol was approved by the institutional review board in our center, and informed consent was obtained from all patients. Demographic characteristics, medical histories, laboratory studies including leukocyte counts and peripheral differential counts, and a variety of hospital outcome data were collected. Clinical information included data on systemic hypertension (HTN), diabetes mellitus, dyslipidemia, smoking, and previous history of CAD, including coronary angioplasty or myocardial revascularization and early family history of CAD. Diabetes was determined by physician report and was based on a fasting blood sugar level ≥126 mg/dL or use of an antidiabetes medication. Hypertension was physician reported for systolic blood pressure ≥140 mm Hg, diastolic blood pressure ≥90 mm Hg, or use of antihypertensive agents. Hyperlipidemia was physician reported for total cholesterol ≥200 mg/dL, low-density lipoprotein (LDL) level ≥130 mg/dL, or use of cholesterol-lowering medication. Family history was self-reported when a first-order relative had cardiovascular death, MI, or coronary revascularization before 65 years of age. Smoking included active or previous (>10 pack-years) tobacco use. The blood sample for neutrophil count, lymphocyte count, and NLR assessment was collected 1 hour after admission to the hospital. In our hospital, blood samples are collected from the antecubital vein by an atraumatic puncture and are sent to the laboratory for analysis within 1 hour after collection. Venous blood is collected in a tube containing K3 EDTA for measurement of hematologic indices in all patients undergoing the coronary angiography. Hematologic indices are evaluated from complete blood count analysis performed using a Coulter LH 780 Hematology Analyzer (Beckman Coulter Ireland Inc, Mervue, Galway, Ireland). Coronary angiographies were performed in our clinic using the standard Judkins technique, and angiographic assessment of the presence of thrombus was made. 20 Patients with a history of trauma, surgery, neoplasm, or infectious disease in the last 30 days prior to hospitalization as well as current use of immunosuppressant (including corticosteroids) were excluded from the study. We also excluded any patients with history of postadmission complications such as cardiogenic shock, serious arrhythmias with hemodynamic instability, or heart failure.
Statistical Analysis
Patient demographic characteristics are presented as means and standard deviations for continuous variables and as proportions (percentages) for categorical variables. Simple 2-group comparisons used chi-square for categorical variables and t test statistics for continuous variables. In order to investigate the distribution of data, Shapiro-Wilk test was used. Comparison of the 2 groups for normally distributed data was performed with t test. Mann-Whitney U test was used for the data that were not normally distributed. Relationships between variables were examined by Pearson correlation coefficient. Threshold values of the receiver–operating characteristic curve (ROC) analysis were statistically significant. The level of significance was set at α = .05. Statistical analyses were performed with MedCalc statistical package version 12.4.0 and SPSS 20.0.
Results
A total of 251 consecutive patients were admitted with NST-ACS to our institution during the study period. During coronary angiography, coronary thrombus was not detected in 82 patients (group 1). In the coronary angiography of 169 patients, coronary thrombus was detected at various grades (group 2). Differential leukocyte counts were obtained, and NLR was calculated. The baseline characteristics across the population are listed in Table 1.
The Baseline Characteristics of the Study Groups.
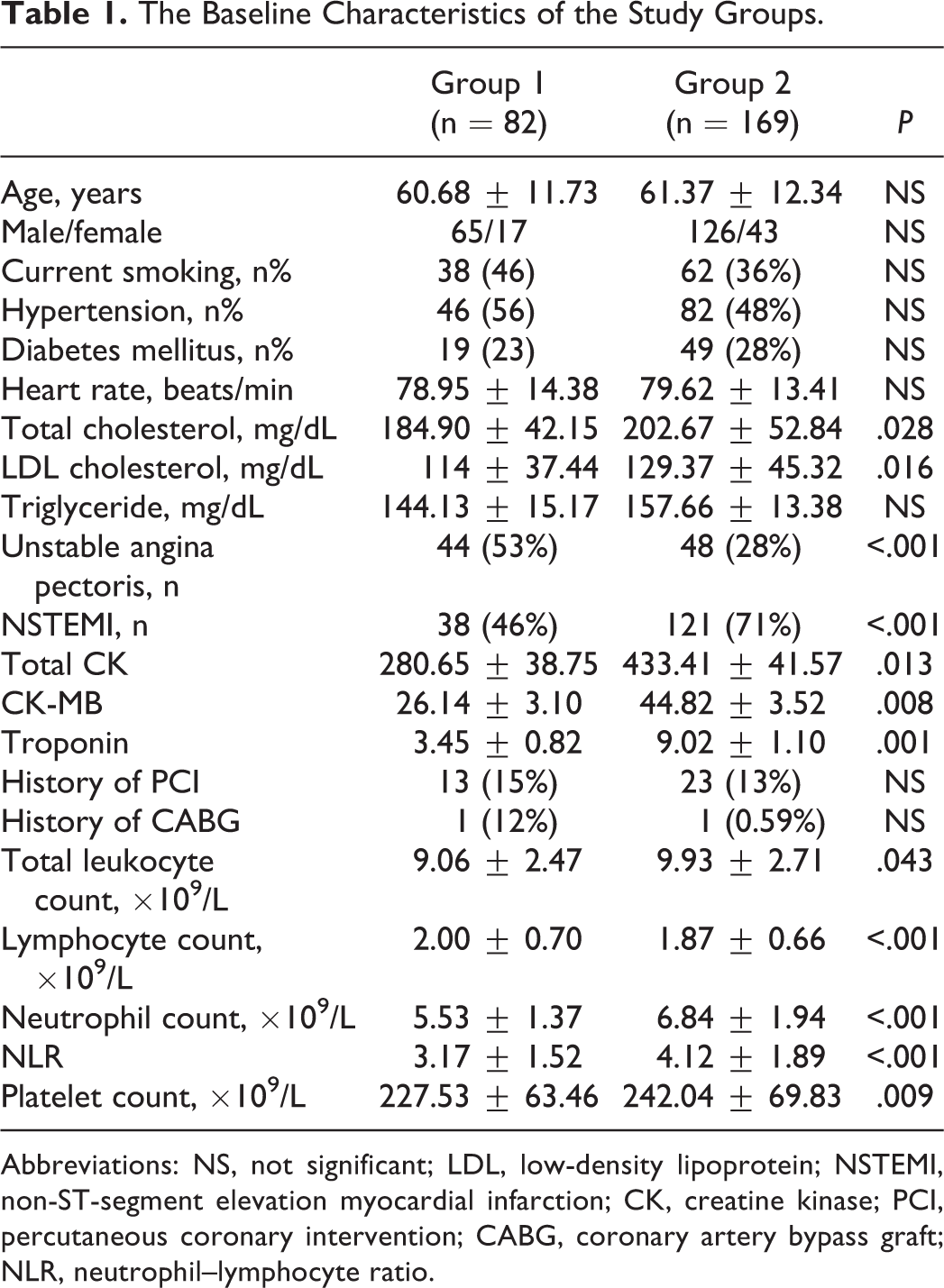
Abbreviations: NS, not significant; LDL, low-density lipoprotein; NSTEMI, non-ST-segment elevation myocardial infarction; CK, creatine kinase; PCI, percutaneous coronary intervention; CABG, coronary artery bypass graft; NLR, neutrophil–lymphocyte ratio.
In the analyses of the study groups, total cholesterol and LDL cholesterol were significantly increased in the patient group with coronary thrombus as compared to the patient group without coronary thrombus. Creatine kinase (CK), CK-MB, and troponin were significantly increased in the group with coronary thrombus. Left ventricular ejection fraction (LVEF) was significantly decreased in the patient group with coronary thrombus. The platelet count was significantly increased in the group with coronary thrombus as compared to the group without coronary thrombus. Although the platelet count was significantly different between the study groups, mean platelet volume (MPV) was not different between the groups with and without coronary thrombus. Although the neutrophil count and the NLR were significantly increased in the group with coronary thrombus, the lymphocyte count was significantly decreased in the group with coronary thrombus as compared to the patient group without coronary thrombus. Also the body mass index of the group with coronary thrombus was found significantly increased as compared to the group without coronary thrombus. Between the study groups with and without coronary thrombus, there was no significant difference in patients’ age, smoking status, HTN prevalence, diabetes prevalence, average heart rate, aspirin use, hemoglobin, and hematocrit levels (Table 1).
It was observed that in patients with a high NLR, there was an increased incidence of non-STEMI. In the subgroup analyzes of the study patients according to the final diagnosis as NSTEMI and UA, there was no significant differences between the patients with NSTEMI and UA for age, body mass index, HTN, diabetes, heart rate, smoking status, coronary artery bypass graft and PCI history, platelet counts, MPV, and lymphocyte count. On the other hand, LDL cholesterol, total CK, CK-MB, troponin value, aspirin use, LVEF, total leukocyte count, neutrophil count, and NLR were significantly different between the groups with NSTEMI and UA (Table 2).
Subgroup Analyzes of the Patients According to the Final Diagnosis.
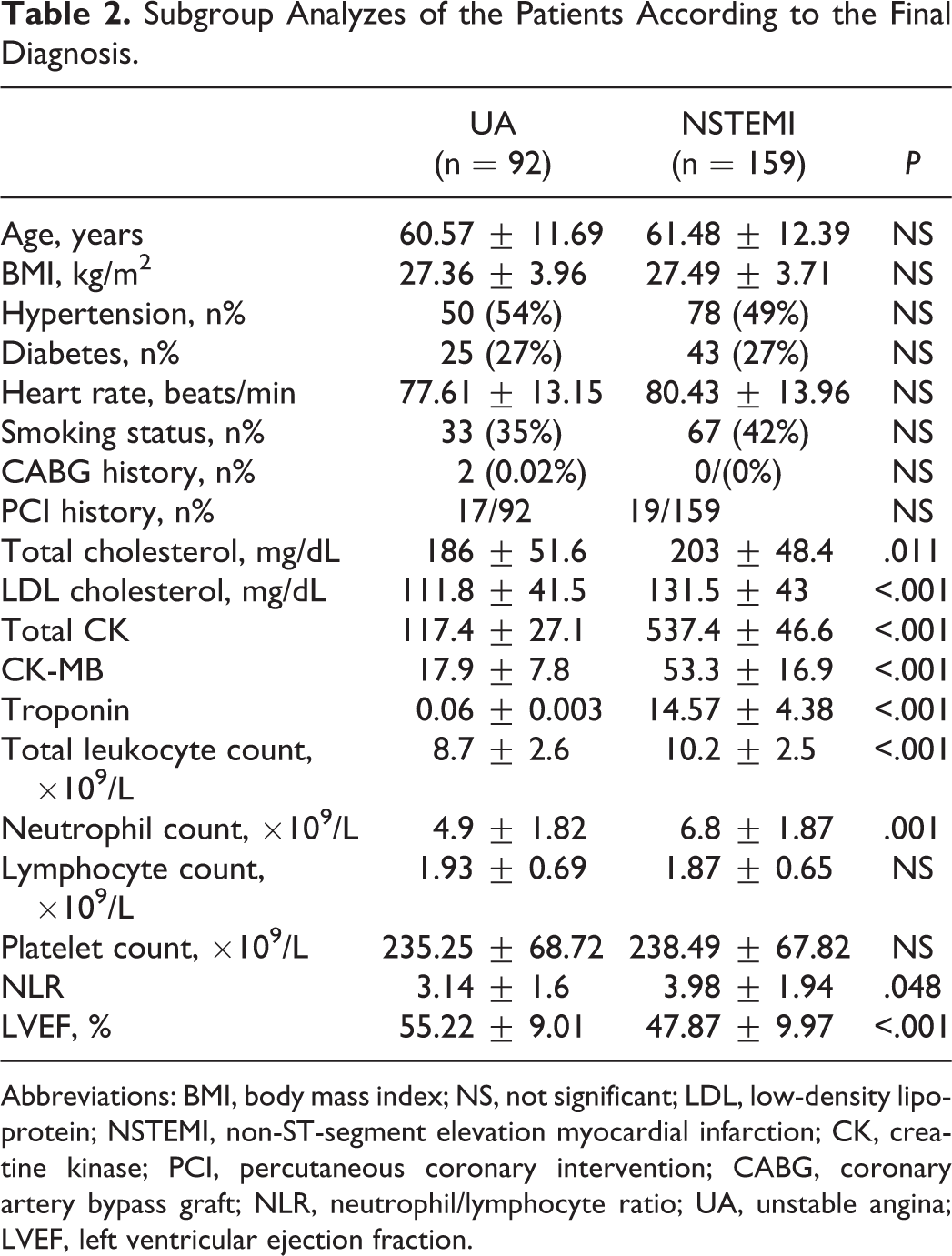
Abbreviations: BMI, body mass index; NS, not significant; LDL, low-density lipoprotein; NSTEMI, non-ST-segment elevation myocardial infarction; CK, creatine kinase; PCI, percutaneous coronary intervention; CABG, coronary artery bypass graft; NLR, neutrophil/lymphocyte ratio; UA, unstable angina; LVEF, left ventricular ejection fraction.
When the study groups were analyzed together, heart rate is found to be positively correlated with total leukocyte count; total CK is positively correlated with total leukocyte count, NLR, and existence of thrombus in coronaries; CK-MB is correlated with total leukocyte count and existence of thrombus in coronaries; troponin is correlated with total leukocyte count, neutrophil count, NLR, and existence of thrombus in coronaries; total leukocyte count is correlated with platelet count, neutrophil count, lymphocyte count, NLR, and existence of thrombus in coronaries; platelet count is correlated with neutrophil count and existence of thrombus in coronaries; neutrophil count is positively correlated with existence of thrombus in coronaries; lymphocyte count is negatively correlated with NLR and existence of thrombus in coronaries; NLR is positively correlated with existence of thrombus in coronaries (Table 3).
Correlations.
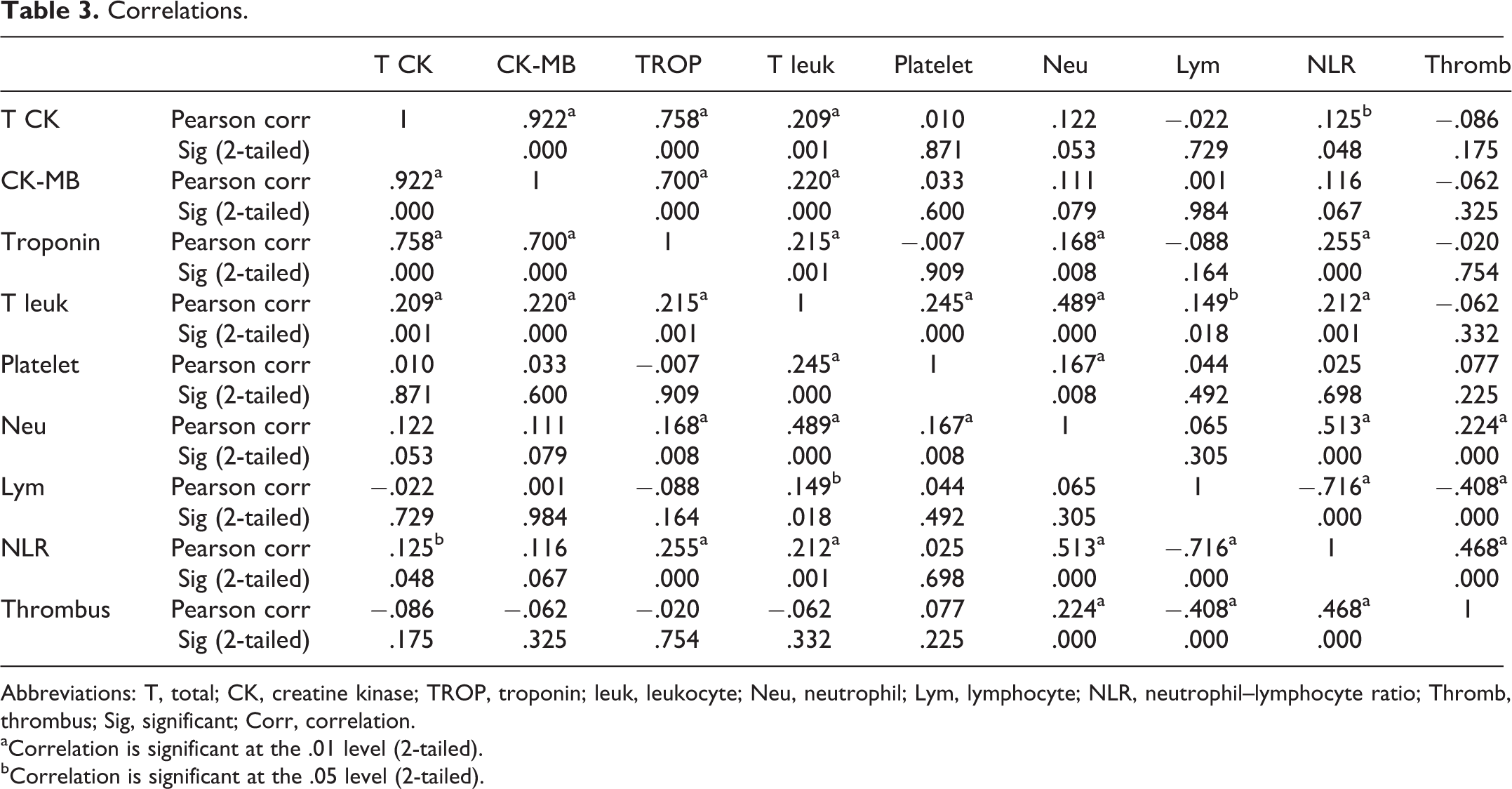
Abbreviations: T, total; CK, creatine kinase; TROP, troponin; leuk, leukocyte; Neu, neutrophil; Lym, lymphocyte; NLR, neutrophil–lymphocyte ratio; Thromb, thrombus; Sig, significant; Corr, correlation.
aCorrelation is significant at the .01 level (2-tailed).
bCorrelation is significant at the .05 level (2-tailed).
On multivariate linear regression, total leukocyte count, neutrophil count, lymphocyte count, NLR, and total CK were found to be independent predictors of coronary thrombus in patients with NST-ACS (Table 4).
Coefficients.a
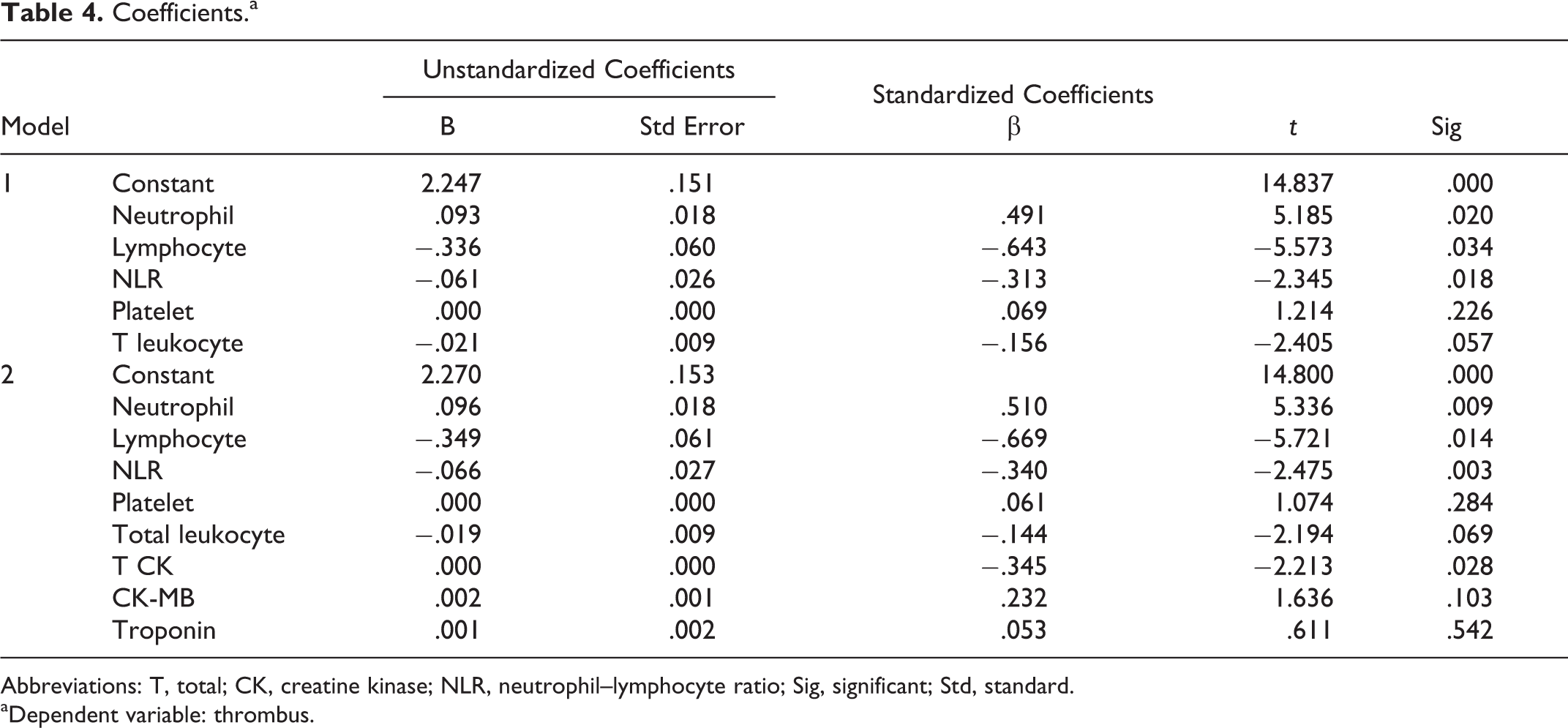
Abbreviations: T, total; CK, creatine kinase; NLR, neutrophil–lymphocyte ratio; Sig, significant; Std, standard.
aDependent variable: thrombus.
Since patients who had coronary thrombus had significantly higher NLRs, higher neutrophil counts, and lower lymphocyte counts, we performed an ROC analysis to determine whether the best cutoff value of NLR, neutrophil count, and lymphocyte count predicts thrombus formation in coronaries. For NLR, the area under the curve was 0.86 (95% confidence interval [CI] 0.81-0.91, P < .001), and the best cutoff value was 1.96, with sensitivity and specificity of 93% and 62%, respectively (Figure 1). For neutrophil count, the area under the curve was 0.69 (95% CI 0.61-0.78, P < .001), and the best cutoff value was 4.50, with sensitivity and specificity of 87% and 70%, respectively (Figure 2). For lymphocyte count, the area under the curve was 0.82 (95% CI 0.76-0.89, P < .001) and the best cutoff value was 2.56, with sensitivity and specificity of 88% and 48%, respectively (Figure 3).
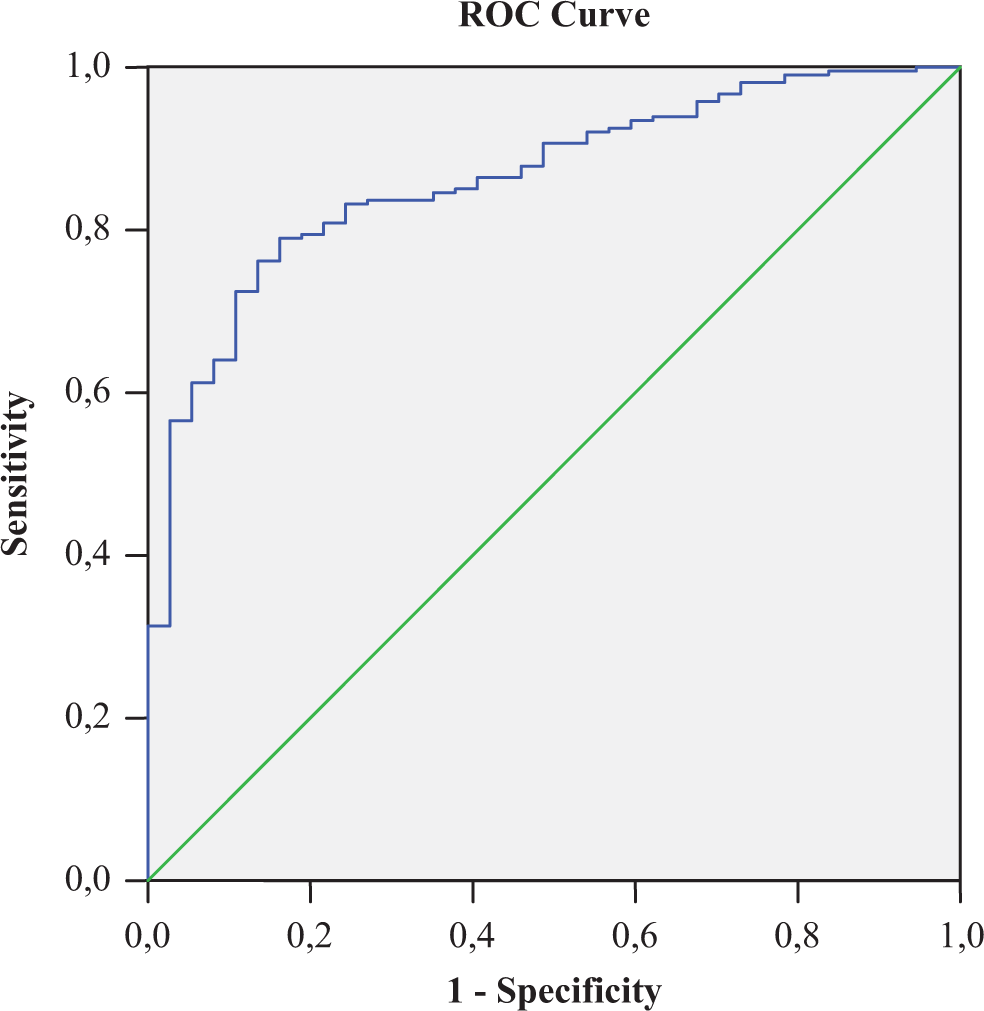
For NLR, the area under the curve was 0.86 (95% CI 0.81-0.91, P < .001), and the best cutoff value was 1.96, with sensitivity and specificity of 93% and 62%, respectively. CI indicates confidence interval; NLR, neutrophil–lymphocyte ratio.
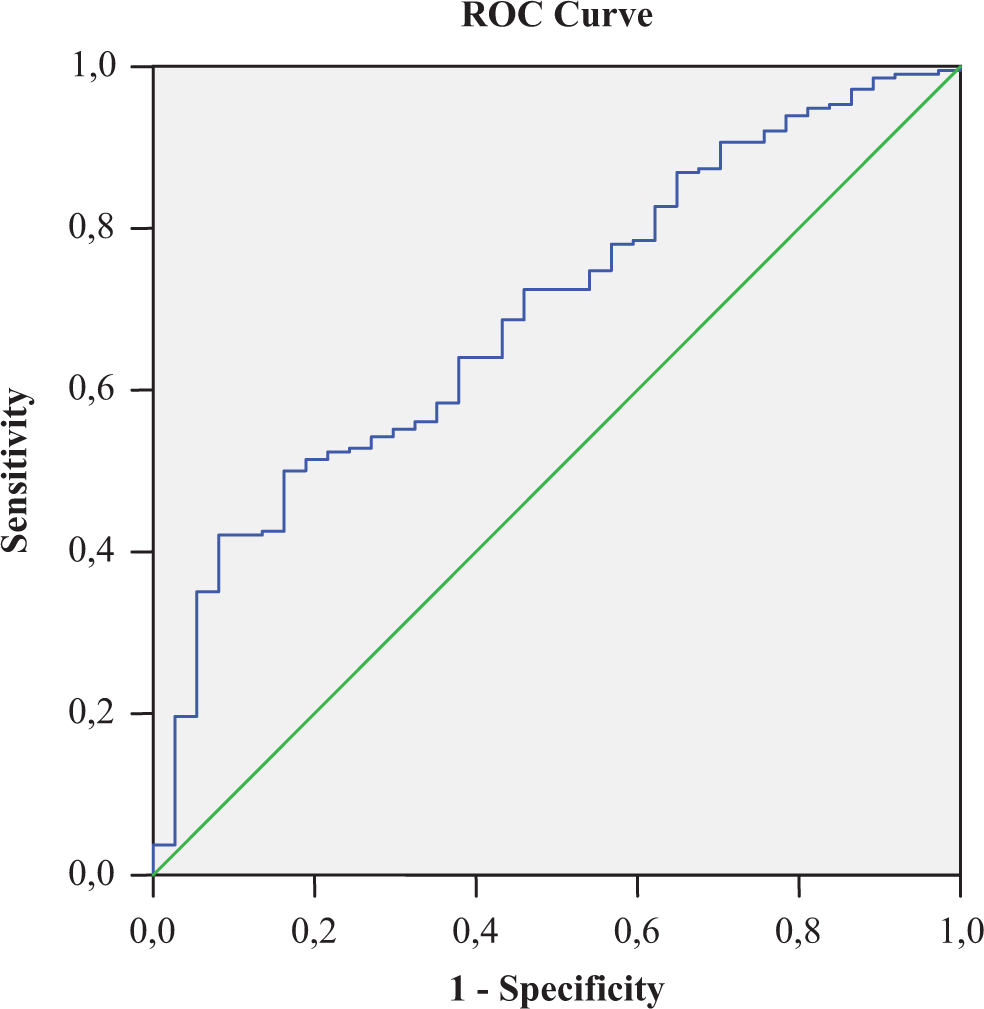
For neutrophil count; the area under the curve was 0.69 (95% CI 0.61-0.78, P < .001), and the best cutoff value was 4.50, with sensitivity and specificity of 87% and 70%, respectively. CI indicates confidence interval.
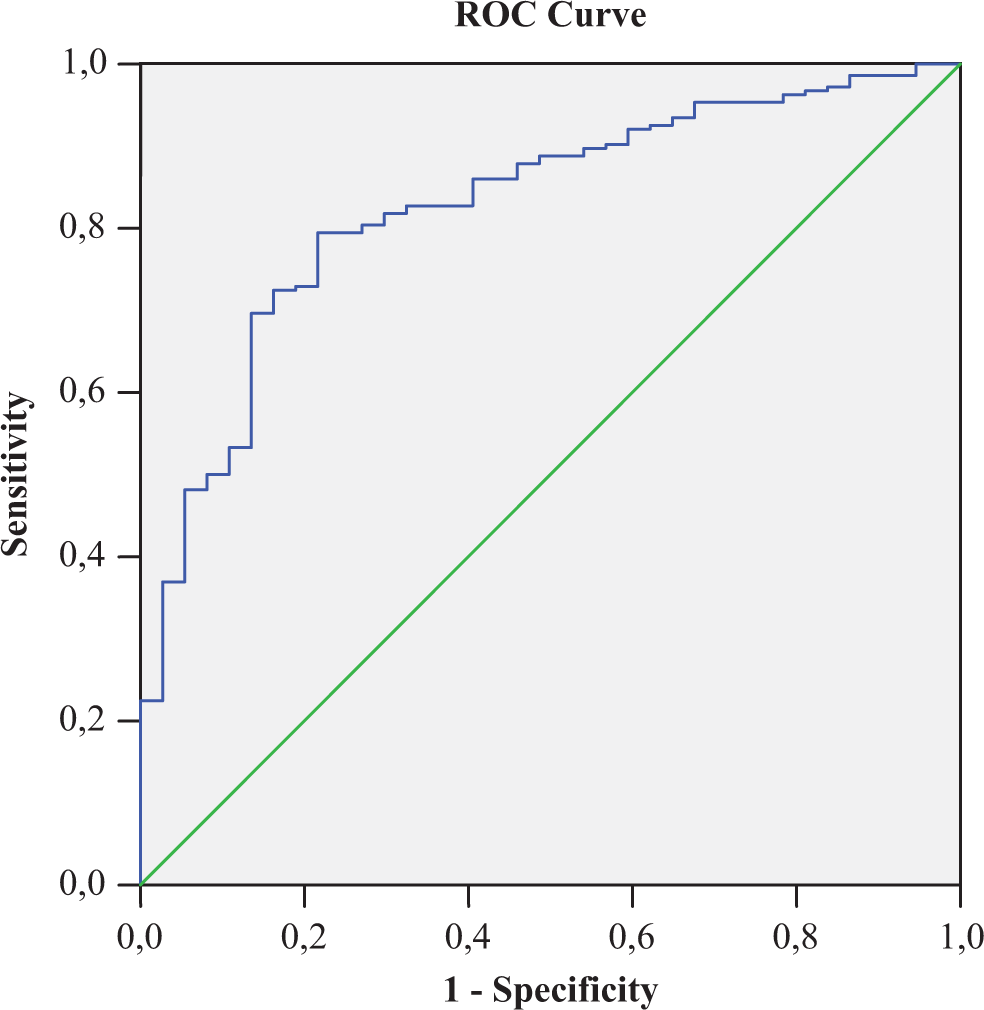
For lymphocyte count, the area under the curve was 0.82 (95% CI 0.76-0.89, P < .001), and the best cutoff value was 2.56, with sensitivity and specificity of 88% and 48%, respectively. CI indicates confidence interval.
Discussion
The principal finding of our study is that NLR, neutrophil count, and lymphocyte count are independent predictors of coronary thrombus formation in patients with NST-ACS. Patients with higher NLRs, neutrophil counts, and lower lymphocyte counts showed increased thrombus incidence, thus providing an additional level of risk stratification in patients with NST-ACS.
Neutrophils are involved in ischemic CAD, especially in acute phase. In peripheral blood, increased expression of neutrophil and monocyte adhesion molecules and other markers (eg, CD11b/CD18) of polymorphonuclear and monocyte activation have been reported in patients with ACS and ischemic heart diseases. 21,22 In ACS, increased neutrophils are associated with the formation of platelet–leukocyte aggregates in the vascular lumen, which causes to extend the infarct area. Neutrophils can also regulate platelet function by direct adhesion and by paracrine effects of secreted factors. 23 Neutrophils also induce atherosclerotic plaque rupture with the release of proteolytic enzymes, superoxide radicals, and arachidonic acid derivatives that make atherosclerotic plaque rupture easier. 24 On the other hand, lymphocyte concentrations were reported to be lower in patients with ACS. The reduction in lymphocyte count should be related to physiological stress that leads to increased cortisol production and increased apoptosis of lymphocyte triggered by increased inflammation. 25,26 Low lymphocyte count is associated with adverse outcomes in patients with acute MI 27 and advanced heart failure. 28 Decrease in CD4, which is the main subtype of total lymphocyte count, correlates with low ejection fraction, reinfarction, and mortality in patients after MI. 29 Based on these information, the NLR reflects the balance between neutrophil and lymphocyte levels in the body and is an indicator of systemic inflammation. 5,30 The NLR has been evaluated in numerous studies of CAD and ACSs. 30,31 The NLR combines 2 leukocyte subtypes with opposite actions in terms of vascular inflammation. Various studies previously have found that high NLR is associated with adverse clinical outcomes in patients with CAD. 8,19,32 Also, at the time of hospitalization, NLR was found to be an independent predictor of in-hospital and 6-month mortality in patients with ACS. 19 The NLR is also an independent predictor of 1-month, 6-month, and 4-year mortalities in patients with non-STEMI. 32 Furthermore, NLR is useful to predict mortality in patients with STEMI and has a indicative ability compared to leukocyte counts. 8
The crucial processes accounting for thrombus formation begin when disrupted, and highly thrombogenic subendothelial matrix and plaque are exposed to circulating platelets and white blood cells. Prominent factors accounting for the formation of a high-grade thrombus burden include hyperglycemia and an increased white blood cell count. 33 In our study, in patients with NST-ACS, the NLR is significantly correlated with thrombus formation in coronary arteries. As mentioned before, increased NLR ratio signifies the severity of the inflammation in ACS. Also increased neutrophil count implies increased aggregation of the platelets in vascular lumen, which directly enhances the thrombus size and consequently extents to the infarct area. The thrombus formation in coronaries is essentially important not only for the extension of the infarct area but also for making the management decisions prior to or during the coronary interventional procedures. In our study, we found that NLR has more ability to predict thrombus formation as compared to the neutrophil count and lymphocyte count alone. This finding discloses the importance of using NLR instead of the leukocyte counts alone for prediction of coronary thrombus formation in the patients with NST-ACS.
In subgroup analysis of our study, we found that, at admission to intensive coronary unit, NLR and neutrophil count were significantly increased in the study group in whom the cardiac biomarkers have increased (NSTEMI) as compared to the patient group with UA whose cardiac biomarkers have not increased. Our finding was compatible with previous studies in which increased neutrophil count also might indicate maladaptive processes; circulating leukocyte–platelet aggregates facilitate vascular plugging and consequently infarct extension. 34 The subgroup analysis between the study groups with and without increased cardiac enzymes may enable clinicians to make further arrangements in medical and interventional treatment facilities of these patients in early phase of the disease, especially at admission to coronary care units.
Conclusion
Neutrophil–lymphocyte ratio, neutrophil, and lymphocyte counts are readily available biomarkers that give important information about the inflammatory activity during acute phase of the coronary syndrome. These simple markers, especially NLR, may provide a risk stratification in patients with NST-ACS beyond that provided by conventional risk scores. This readily available marker may be useful during admission to hospital for choosing the treatment strategy in patients with NST-ACS in early phase either medically or interventionally in early stages of the disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.